Abstract
The traumatic bone cyst (TBC) is an uncommon and poorly understood lesion. First described in 1929, TBCs lack an epithelial lining, typically occur during the second decade of life, and are most frequently located in the jaw. Although the majority of TBCs are asymptomatic, rarely a TBC can cause a pathologic fracture of the mandible. We present a case of an adolescent suffering a sports-related pathologic mandible fracture secondary to a traumatic bone cyst.
The traumatic bone cyst (TBC) is an uncommon and poorly understood entity. First described in 1929, by definition, TBCs lack an epithelial lining. These lesions most frequently occur in the jaw [1]. Although most often asymptomatic, rarely a TBC can lead to a pathologic fracture of the mandible [2,3]. Only a few such cases appear in the literature. In this report, we present a case of an adolescent suffering a sports-related pathologic mandible fracture secondary to a TBC.
Facial fractures in the pediatric population are uncommon. Less than 15% of all facial fractures occur in the pediatric population [4]. The most common site for a mandible fracture in children is the condyle, accounting for ~45% of fractures [4,5].
Motor vehicle accidents account for nearly 60% of mandible fractures [5]. Only 2% of mandible fractures in children are caused by sports injury.5
1. Case Report
A 13-year-old adolescent boy presented to our Emergency Department (ED) with persistent facial pain following a collision while playing football. During practice, the patient was struck in the chin with a teammate’s knee. He was wearing a helmet, mouth guard, and football pads at the time. He was initially evaluated at an outside hospital, where a computed tomography (CT) scan was performed and iden- tified a significantly displaced left-sided parasymphyseal mandible fracture. He was referred initially to a local surgeon as an outpatient, but presented to our ED the following day.
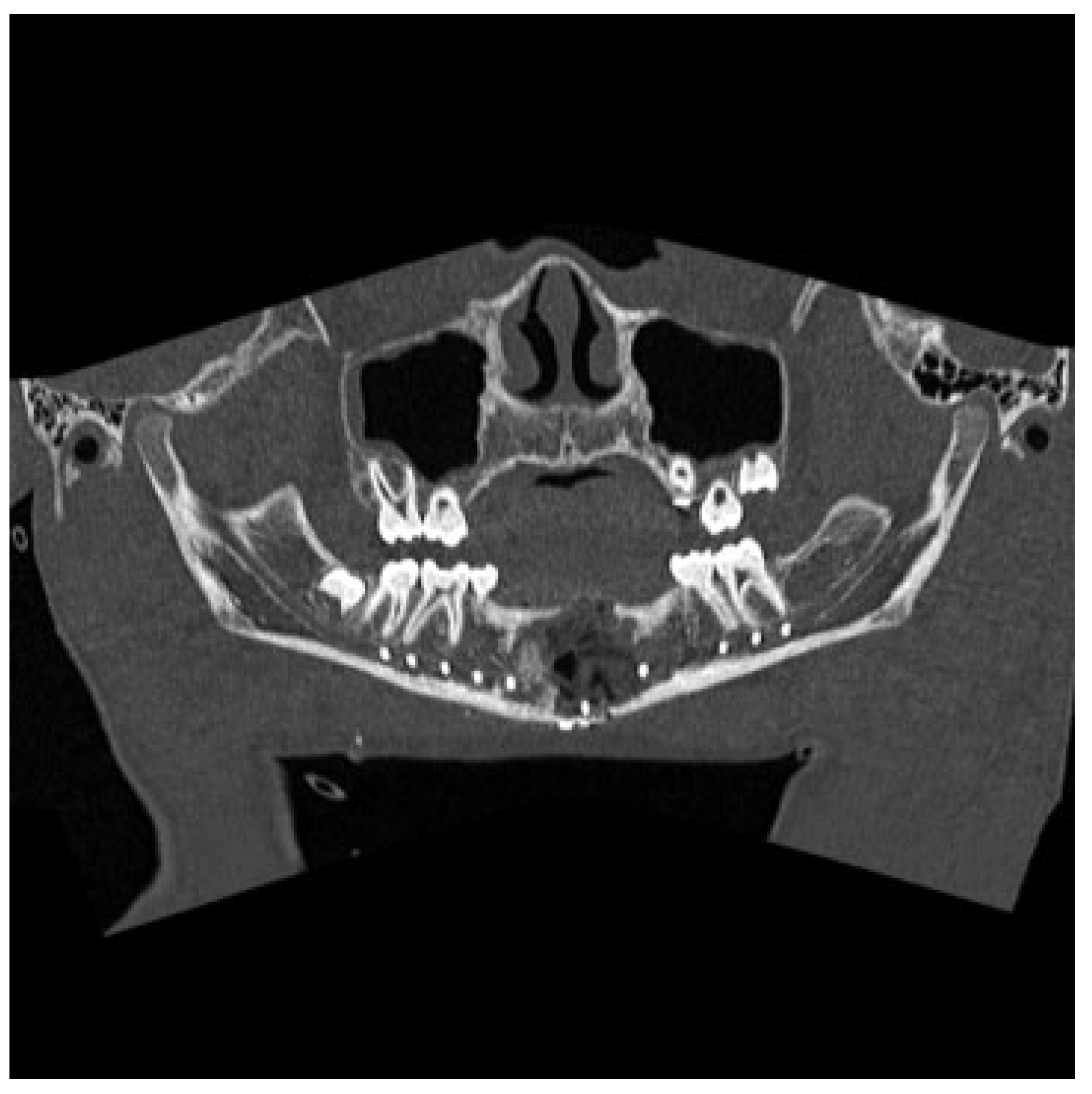
The Otolaryngology-Head and Neck Surgery department was consulted upon arrival to our ED. Physical examination revealed tenderness of the left side of the mandible and a visible intraoral step-off between the left mandibular lateral incisor and canine tooth. The CT was reviewed and demon- strated a significantly displaced fracture of the left para- symphysis. The fracture was deemed pathologic secondary to an apparent preexistent cystic lesion of the mandibular symphysis measuring 2.5 × 1.5 × 1.5 cm, with evidence of bony expansion (Figure 1).
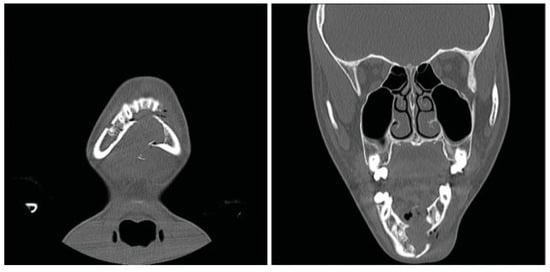
Figure 1.
Coronal computed tomography (CT) scan revealing a parasymphyseal fracture in line with a cystic cavity.
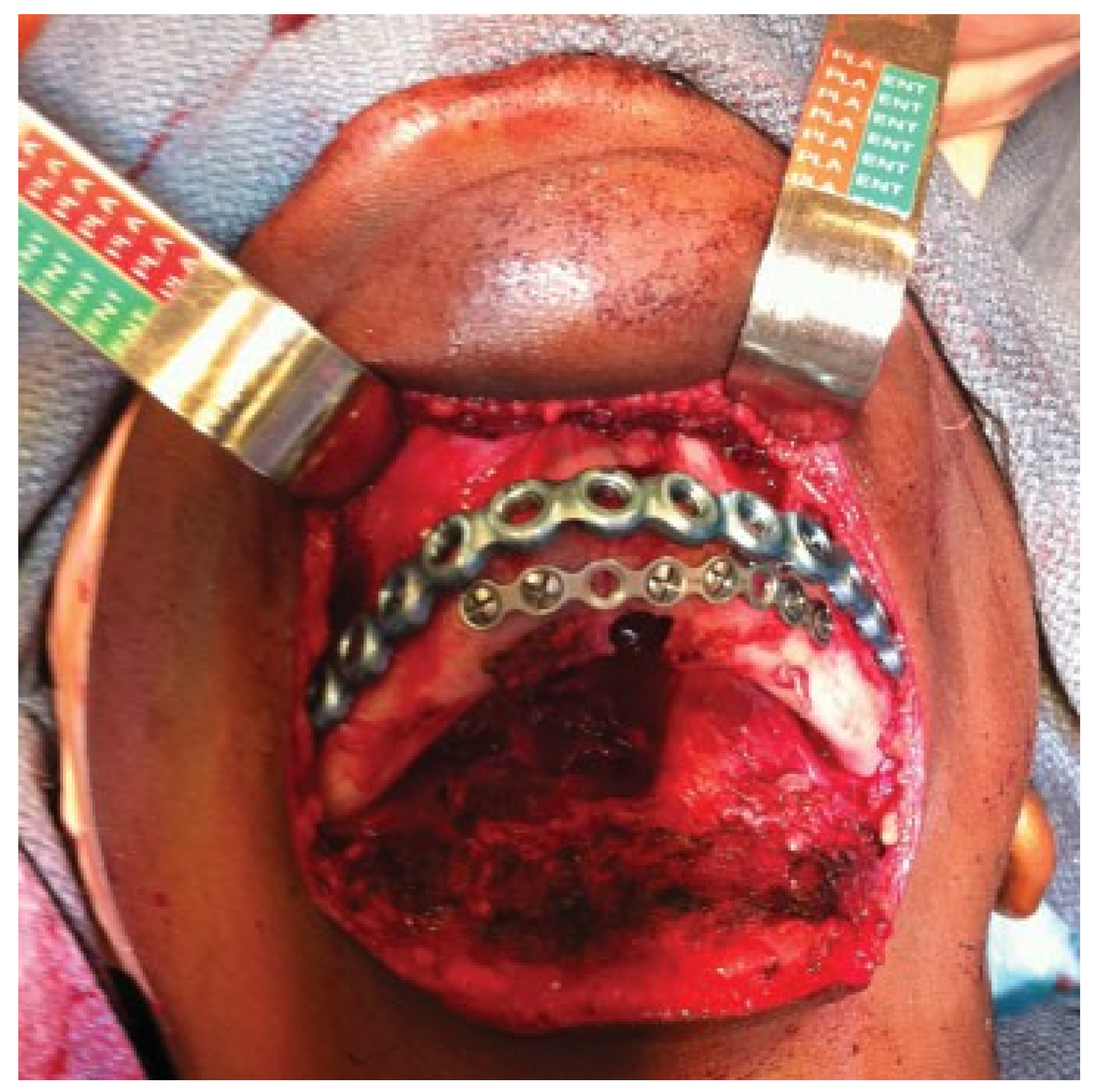
The patient was taken to the operating room the next day. With evidence of a lesion in the mandible of unknown pathology, the decision was made to proceed with a trans- cervical approach to provide broader access that would allow for adequate curettage and resection if needed. The fracture line and cystic cavity were identified. A cystic lumen was filled with organized blood clotlike material. No definitive solid tissue was identified (Figure 2). The clot and the cortex of the cavity were curetted and sent for histologic interpreta- tion. Occlusion had been established previously with max-illomandibular fixation. The mandibular fracture was reduced and repaired with a lower-border Synthes Matrix mandibular locking bar with bicortical screws (Synthes CMF, West Chester, PA, USA). An additional 2.0 Synthes Matrix mono- cortical plate was used to secure a sizable secondary fragment of the cystic wall (Figure 3). The cystic space was packed with Gelfoam (Pfizer, Pharmacia and Upjohn Company, Kalamazoo, MI, USA), as a means of filling the cystic dead space with a nonpermanent material that would not interfere with later osteogenesis. The remainder of surgery was uncomplicated and a small suction drain was placed at closing. A postoperative image revealed satisfactory alignment (Figure 4). The drain was removed on postoperative day 2, and the patient was dis-charged home 3 days later, tolerating a soft diet. Fifteen days after discharge, the patient returned to our ED with worsening pain and swelling at the surgical site. He was diagnosed with a small submental abscess. The patient was admitted and treated successfully with bedside incision and drainage and a short course of intravenous antibiotics. The remainder of his recovery was uneventful, with good occlusion and function. Follow-up CT imaging at 6 weeks showed good fracture healing and some early osteogenesis within the cystic cavity (Figure 5). One year after surgery, he had normal occlusion and no evidence of hardware complications. Additionally, CT imaging demonstrated ossification of the majority of the cystic space, with only a few small lateral areas of persistent cyst (Figure 6).
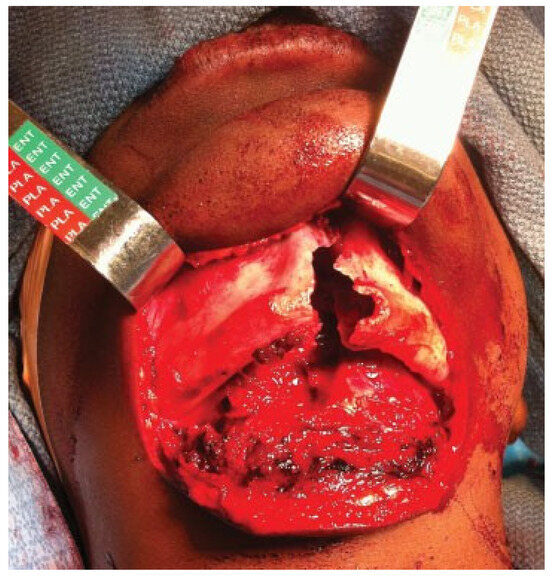
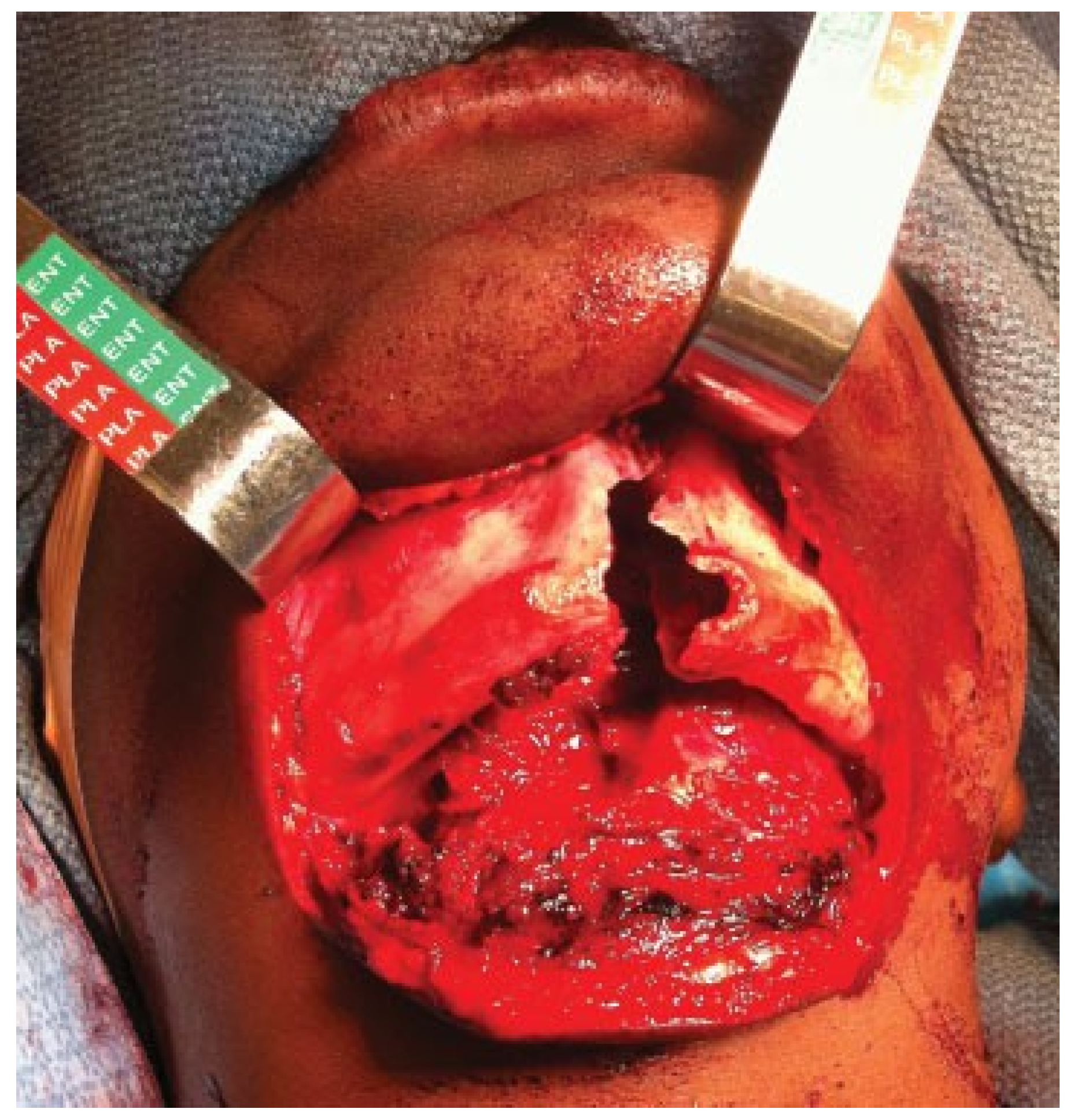
Figure 2.
Intraoperative photograph demonstrating a parasymphyseal mandibular fracture through the cavity of a preexisting mandibular cyst.
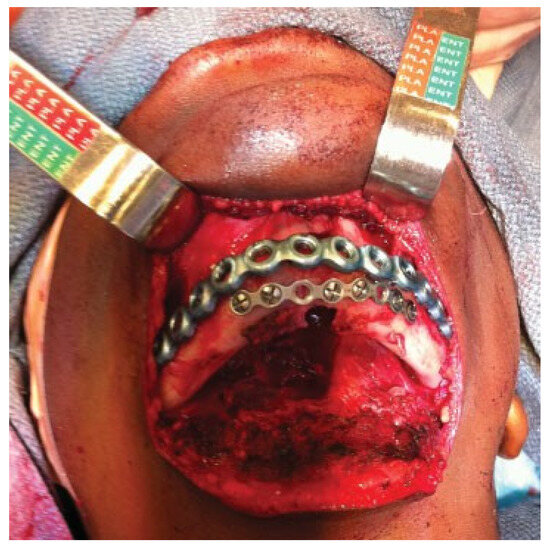
Figure 3.
Intraoperative photograph after further stabilization of the parasymphyseal mandibular fracture with the use of a second, smaller profile plate.
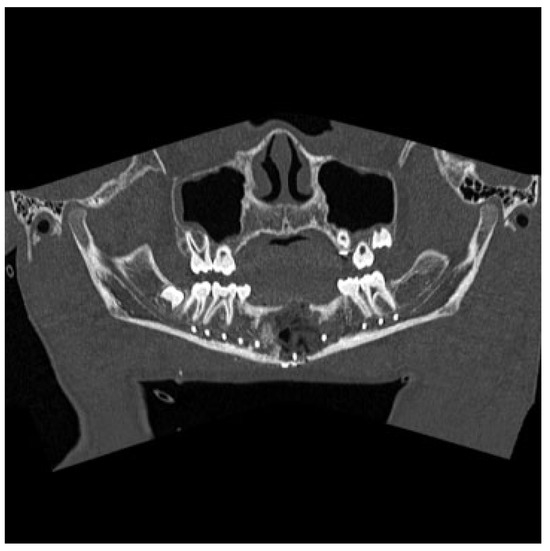
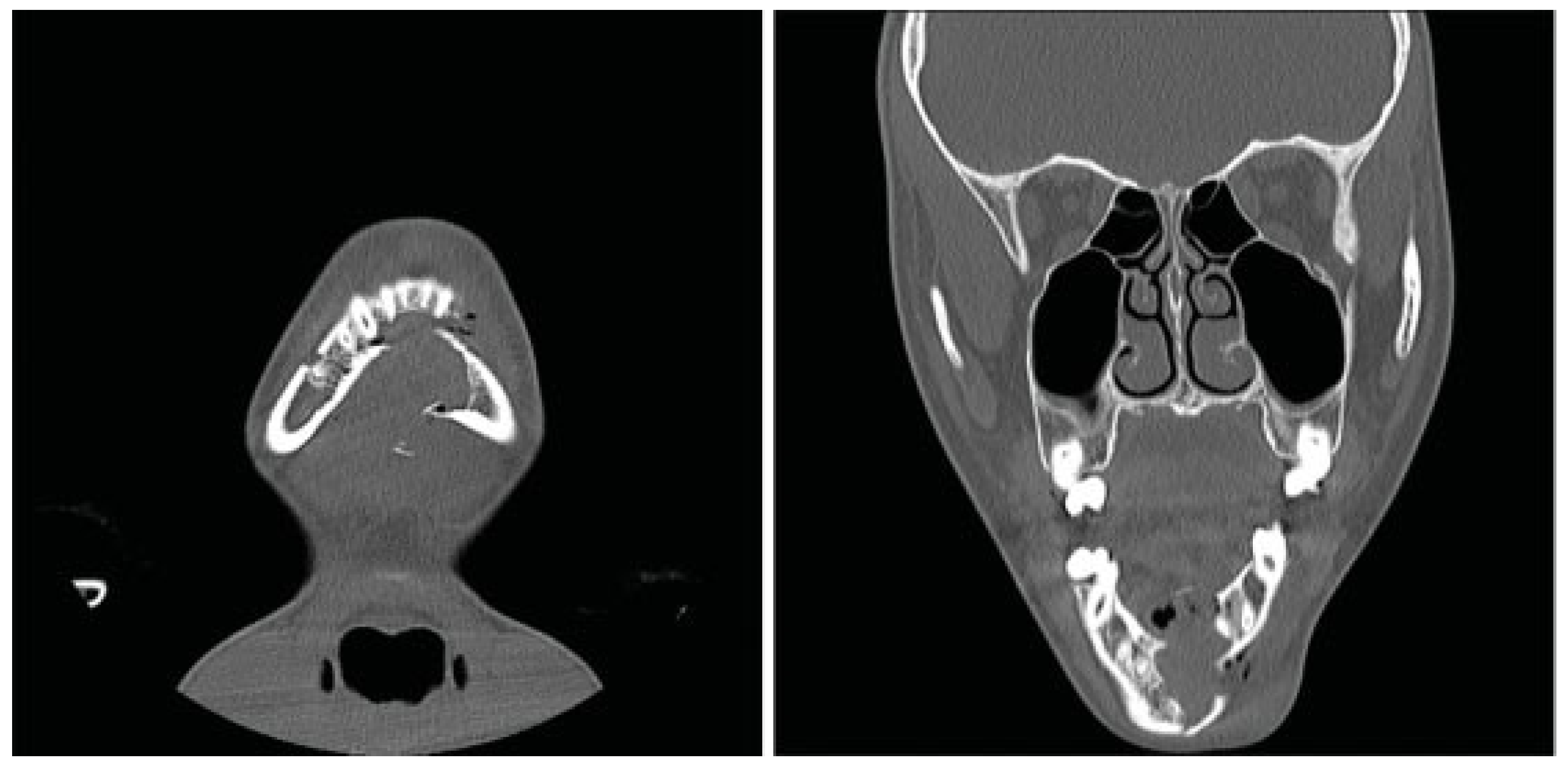
Figure 4.
Panorex computed tomography scan obtained in the immediate postoperative period showing improved anatomic alignment.
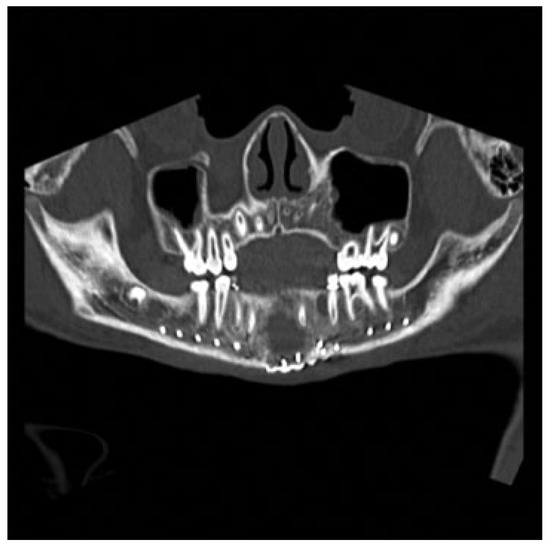
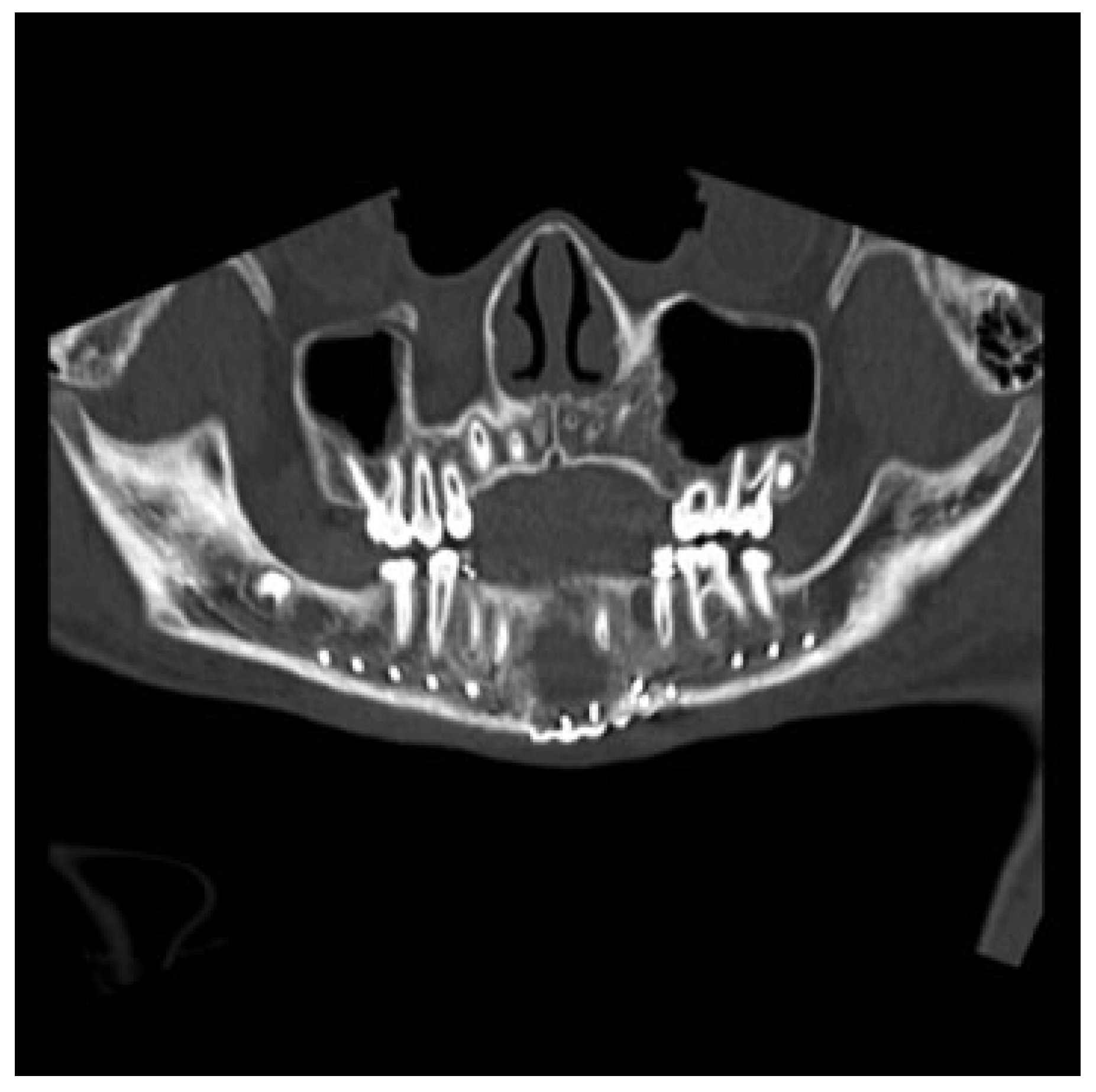
Figure 5.
Panorex computed tomography scan obtained 7 weeks postoperatively demonstrating improved anatomic alignment with some neo-osteogenesis and persistent cystic defect of the mandible.
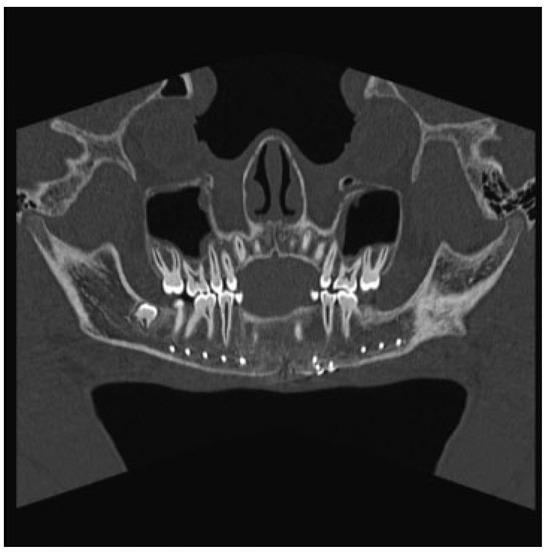
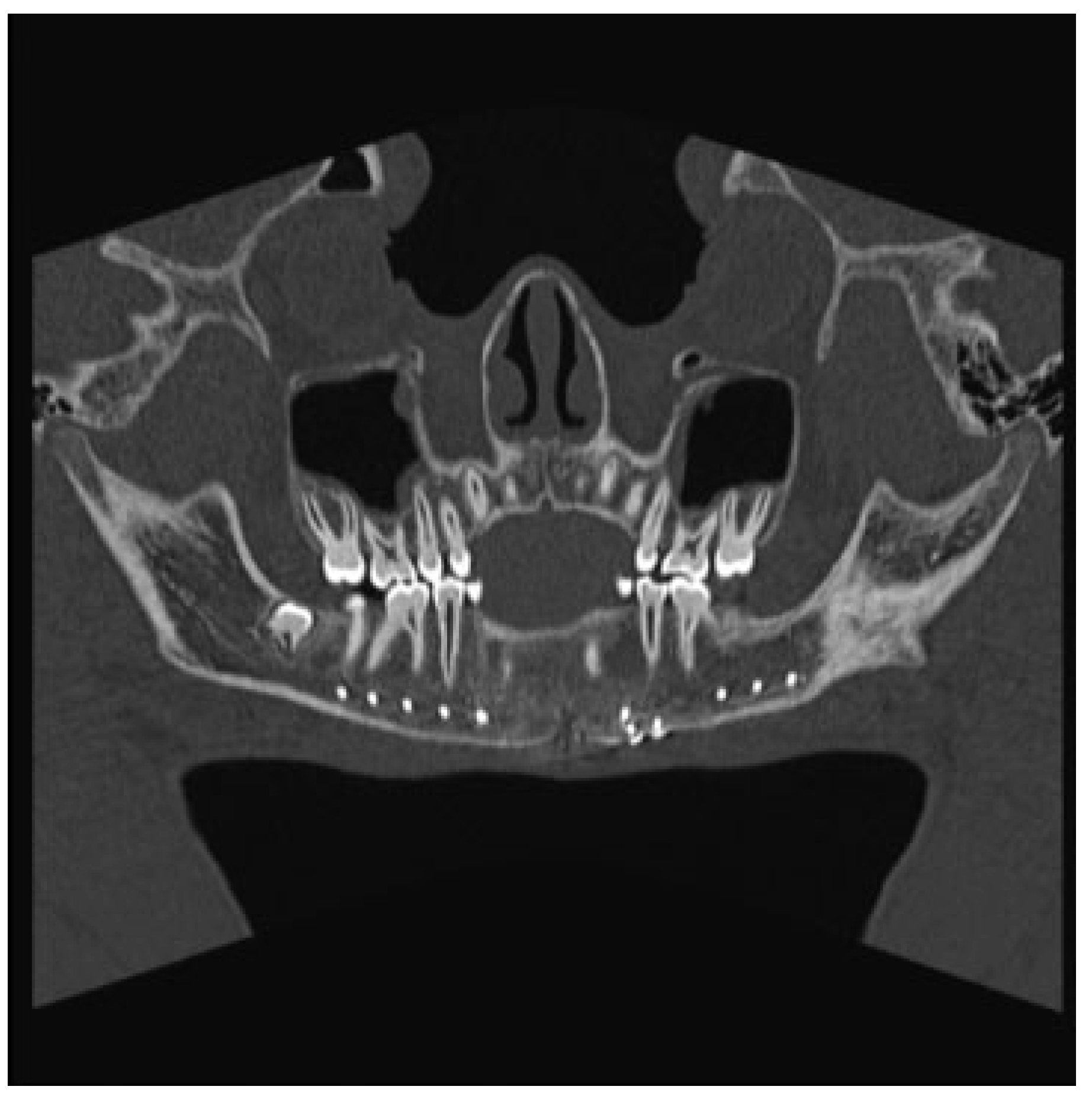
Figure 6.
Panorex computed tomography scan obtained 1 year postoperatively demonstrating near-complete ossification of the cys- tic defect of the mandible.
Histopathology of the curetted material from the mandible confirmed the diagnosis of a TBC, revealing granulation tissue, old hemorrhage, and reactive woven bone. No epithe- lial or other cystic elements were identified. Apart from the patient’s current injury, he denied any history of previous mandibular trauma.
2. Discussion
Lucas and Blum first described the TBC in 1929. Somewhat of a misnomer, TBCs lack an epithelial lining and thus are not true cysts [1]. TBCs are also referred to by various other names in the literature, including extravasation cyst, hemorrhagic bone cyst, progressive bone cavity, simple bone cyst, solitary bone cyst, and unicameral bone cyst [6]. Traumatic bone cyst is currently the most commonly used name [6,7]. TBCs occur most frequently during the second decade of life [8,9,10]. The gender predilection is reported to be roughly equal in most literature [9,11], although a recent study has suggested women may be affected more than men [12]. The body of the mandible and mandibular symphysis are predominant locations for TBCs to form [9,10,13]. The exact pathogenesis of TBCs is unknown, but a multitude of theories have been suggested. Most believe that trauma, including tooth extraction, causes intraosseous bleeding. The blood eventually clots and osteoclasts destroy the surrounding bone, resulting in formation of the cyst cavity [14]. The role of trauma in the formation of TBCs remains unknown. Kaugars and Cale reported that incidence of trau-ma in TBC to be equal to the general population,11 but others reported a clear history of trauma in less than 29% of cases [12,15].
TBCs are asymptomatic in the majority of cases. They are frequently discovered incidentally during routine radiologic examination. If symptomatic, pain is the most common symptom but is present in less than 20% of cases [8,9,10]. Other symptoms are far less common and include tooth sensitivity, paresthesia, and pathologic fracture of the mandible [2,7,9]. A pathologic fracture as the presenting sign of a TBC is rare, and is mentioned in the literature sparsely [2,3].
Radiographically and histopathologically, traumatic bones cysts are bland. On X-ray or CT, TBCs are unilocular lesions with well-defined and irregular borders. The classic descrip- tion of “scalloping” can be seen with cystic involvement of the interdental space [16]. At biopsy, fibrous connective tissue and normal bone are the most common histologic findings. As TBC is not a true cyst, there is never evidence of epithelial lining to the cavity [9]. Uncommonly, bony expansion or erosion may be noted [9]. Because tissue for histologic examination is frequently inadequate, observation during surgery of an empty bone cavity lacking an epithelial lining is often the predominant finding [9].
Although there have been reported cases of spontaneous resolution [17,18], curettage is the definitive treatment, serving as both a diagnostic and therapeutic procedure. Curettage causes bleeding within the cystic cavity [6]. This forms a clot and ultimately reossifies with complete healing within 17 months [19]. Although initially believed to be rare [10], a recent review of the literature suggests the recurrence rate following treatment is ~26% [19]. Packing the cavity appears to increase healing and reduce the rate of recurrence [19]. Although in our case the patient’s recovery was complicated by development of a submental abscess, the cyst appears to be healing well with significant neo-osteogenesis on follow-up imaging. The abscess was likely attributable to the partially open cystic cavity, providing a location for bacteria to colonize. Follow-up at 1 year reveals continued good clinical and radiographic result, with viable dentition and normal function.
References
- Lucas, C.; Blum, T. Do all cysts of the jaws originate from the dental system. J Am Dent Assoc 1929, 16, 659–661. [Google Scholar]
- Hughes, C.L. Hemorrhagic bone cyst and pathologic fracture of mandible: Report of case. J Oral Surg 1969, 27, 345–346. [Google Scholar] [PubMed]
- Baird, W.O.; Askew, P.A. Traumatic mandibular bone cyst involved in line of fracture. Oral Surg Oral Med Oral Pathol 1958, 11, 1351–1356. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, C.E.; Troulis, M.J.; Kaban, L.B. Pediatric facial fractures: Recent advances in prevention, diagnosis and management. Int J Oral Maxillofac Surg 2005, 34, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Glazer, M.; Joshua, B.Z.; Woldenberg, Y.; Bodner, L. Mandibular frac- tures in children: Analysis of 61 cases and review of the literature. Int J Pediatr Otorhinolaryngol 2011, 75, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Xanthinaki, A.A.; Choupis, K.I.; Tosios, K.; Pagkalos, V.A.; Papanikolaou, S.I. Traumatic bone cyst of the mandible of possible iatrogenic origin: A case report and brief review of the literature. Head Face Med 2006, 2, 40. [Google Scholar] [CrossRef] [PubMed]
- MacDonald-Jankowski, D.S. Traumatic bone cysts in the jaws of a Hong Kong Chinese population. Clin Radiol 1995, 50, 787–791. [Google Scholar] [CrossRef] [PubMed]
- Howe, G.L. “Haemorrhagic cysts” of the mandible. I. Br J Oral Surg 1965, 3, 55–76. [Google Scholar] [CrossRef] [PubMed]
- Hansen, L.S.; Sapone, J.; Sproat, R.C. Traumatic bone cysts of jaws. Oral Surg Oral Med Oral Pathol 1974, 37, 899–910. [Google Scholar] [CrossRef] [PubMed]
- Huebner, G.R.; Turlington, E.G. So-called traumatic (hemorrhagic) bone cysts of the jaws. Review of the literature and report of two unusual cases. Oral Surg Oral Med Oral Pathol 1971, 31, 354–365. [Google Scholar] [CrossRef] [PubMed]
- Kaugars, G.E.; Cale, A.E. Traumatic bone cyst. Oral Surg Oral Med Oral. 1987, 63, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Cortell-Ballester, I.; Figueiredo, R.; Berini-Aytés, L.; Gay-Escoda, C. Traumatic bone cyst: A retrospective study of 21 cases. Med Oral Patol Oral Cir Bucal 2009, 14, E239–E243. [Google Scholar] [PubMed]
- Beasley, J.D., III. Traumatic cyst of the jaws: Report of 30 cases. J Am Dent Assoc 1976, 92, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Olech, E.; Sicher, H.; Weinmann, J.P. Traumatic mandibular bone cysts. Oral Surg Oral Med Oral Pathol 1951, 4, 1160–1172. [Google Scholar] [CrossRef] [PubMed]
- Peñarrocha-Diago, M.; Sanchis-Bielsa, J.M.; Bonet-Marco, J.; Minguez-Sanz, J.M. Surgical treatment and follow-up of solitary bone cyst of the mandible: A report of seven cases. Br J Oral Maxillofac Surg 2001, 39, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Devenney-Cakir, B.; Subramaniam, R.M.; Reddy, S.M.; Imsande, H.; Gohel, A.; Sakai, O. Cystic and cystic-appearing lesions of the mandible: Review. AJR Am J Roentgenol 2011, 196 (Suppl. 6), WS66–WS77. [Google Scholar] [CrossRef] [PubMed]
- Szerlip, L. Traumatic bone cysts. Resolution without surgery. Oral Surg Oral Med Oral Pathol 1966, 21, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Sapp, J.P.; Stark, M.L. Self-healing traumatic bone cysts. Oral Surg Oral Med Oral Pathol 1990, 69, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Suei, Y.; Taguchi, A.; Tanimoto, K. Simple bone cyst of the jaws: Evaluation of treatment outcome by review of 132 cases. J Oral Maxillofac Surg 2007, 65, 918–923. [Google Scholar] [CrossRef] [PubMed]
© 2013 by the author. The Author(s) 2013.