The etiology of facial fractures has been the subject of numerous studies. The etiology of this group of fractures has changed over the years and it is related to several factors such as gender, age, geographic region, and socioeconomic status. This makes both the incidence and the etiology different between countries, and even within the same country. The aim of this study is to assess the incidence, epidemiology, type, and cause of all facial fractures receiving a surgical treatment by the Department of Oral and Maxillofacial Surgery, A Corun˜a University Hospital, from 2001 to 2008.
Patients and Methods
A retrospective study was conducted, including all patients treated by the Department of Oral and Maxillofacial Surgery, A Corun˜a University Hospital (Spain), for facial fracture, from January 2001 to December 2008. Isolated nasal and dento-alveolar fractures, as well as nonsurgical ones, were excluded. The following variables were studied in this descriptive and analytic report: age, gender, year of the trauma, fracture type, and etiology. Data were collected from the patient’s medical history and completed if necessary by phone interview.
The fracture type was classified into orbit, zygomatic complex, nasoethmoidal (NE) complex, frontal, panfacial (those concerning all the three facial thirds), and Le Fort fractures. The cause of injury was classified into traffic accidents (including vehicle-pedestrian collisions), accidental traumas, sports-related accidents, industrial accidents, assaults, syncopes, rural accidents, and suicide attempts. Among traffic accidents, we differentiated between motorcycle and non-motorcycle accidents. Traumas for syncope included strokes, epileptic crisis, falls involving alcohol, and vaso-vagal syncopes. It was impossible to verify the etiology in seven patients because of an incomplete medical history and being unable to contact them.
Six hundred and forty-three patients with 793 fractures were included; of these, 83.2% were males and 16.8% were females. Their age ranged from 18 months to 89 years and they were classified into the following age groups (in years): younger than 16, 16 to 30, 31 to 45, 46 to 60, 60 to 65, and older than 75.
The database was created using Microsoft Excel software. The results were analyzed and tested for statistical significance with SPSS 15.0, and we used the x2 test for bivariate associations.
Results
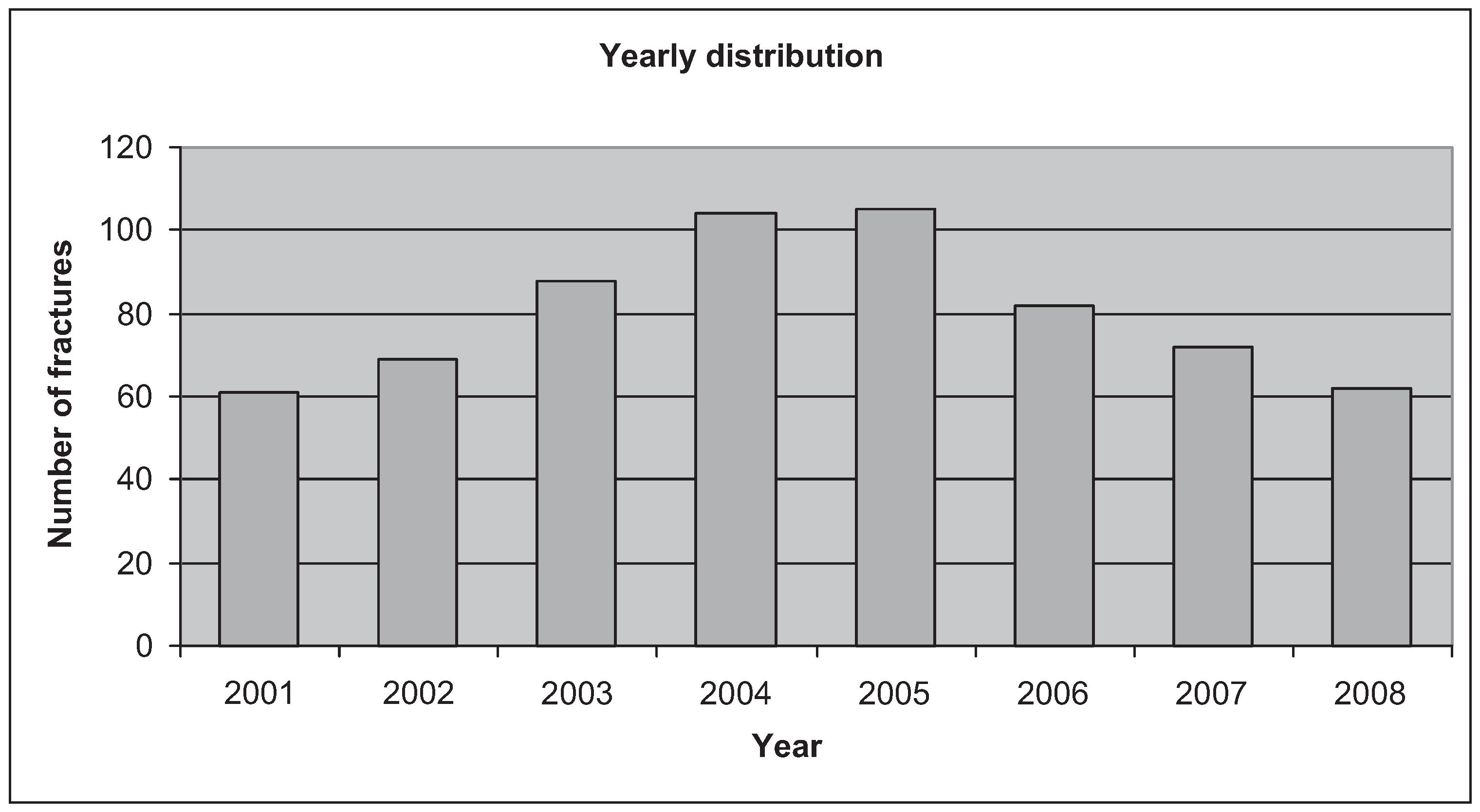
In this study, 793 fractures in 643 patients were included. The total number of patients receiving a surgical treatment has annually increased until 2005, beginning to decrease since then (
Figure 1). Of the patients, 83.2% were males and 16.8% were females. The global ratio of male:female was 4.95, taking its maximum value in patients between 16 and 30 years, and the minimum in patients older than 75 years.
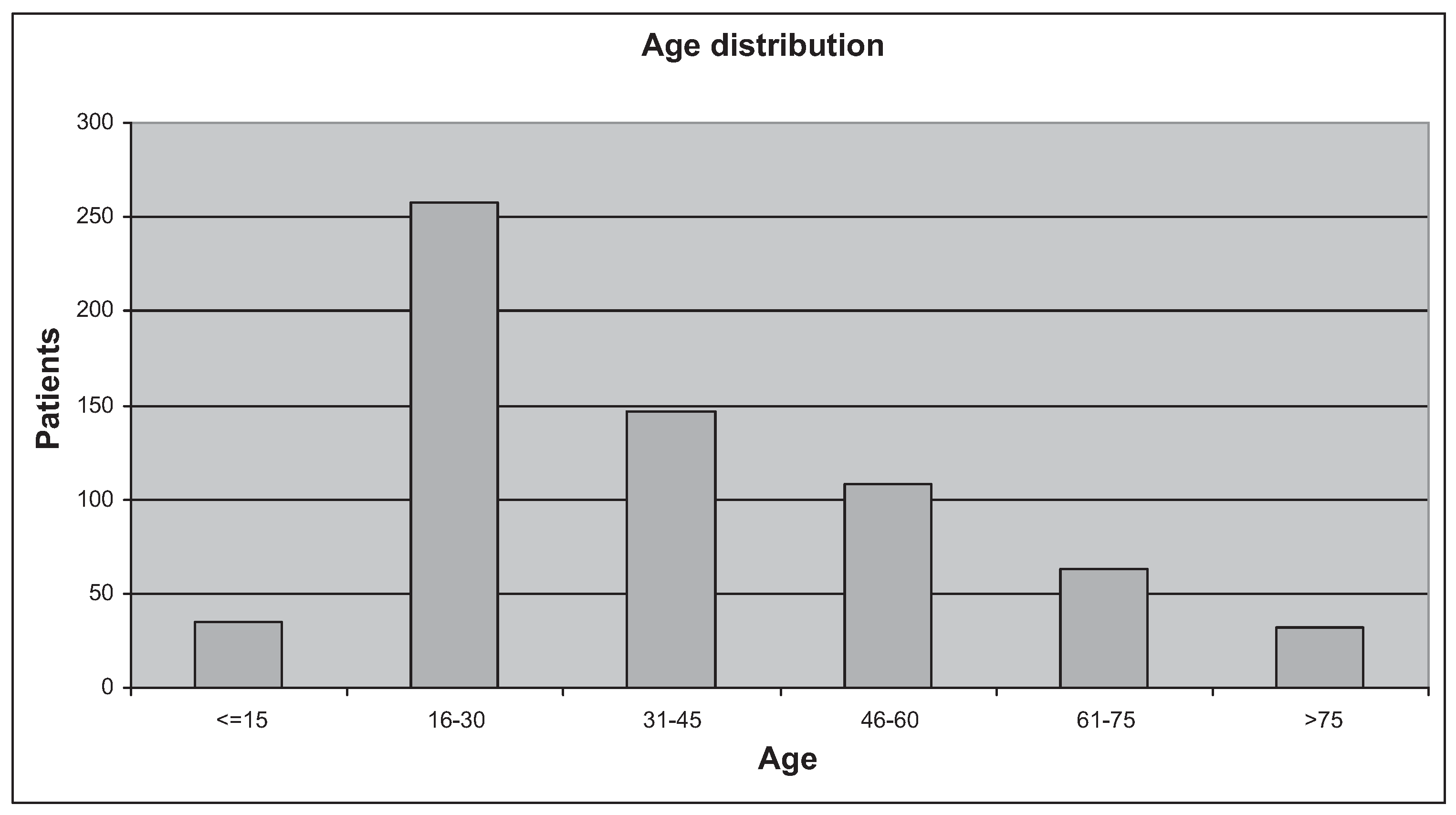
The patients’ age ranged between 1 and 89 years, with a mean of 37.6 and a median of 33 (
Figure 2). Among the patients 40.2% were between 16 and 30 years. The mean and the median were, respectively, 35.9 and 31 in males and 45.9 and 45.5 in females. The median was 13.5 years higher in females (statistically significant difference,
p < 0.001). The facial fracture incidence peak was different in males and females: the majority of fractures in males occurred between 16 and 30 years, the frequency decreasing with age after that; females, nevertheless, suffered more fractures between 31 and 45 years, the risk being inversely related to age, but maintaining higher relative risks than males older than 45 years. In males, 71.2% of all fractures occurred in those younger than 46 years, whereas in females 50% of fractured occurred in those older than 45.
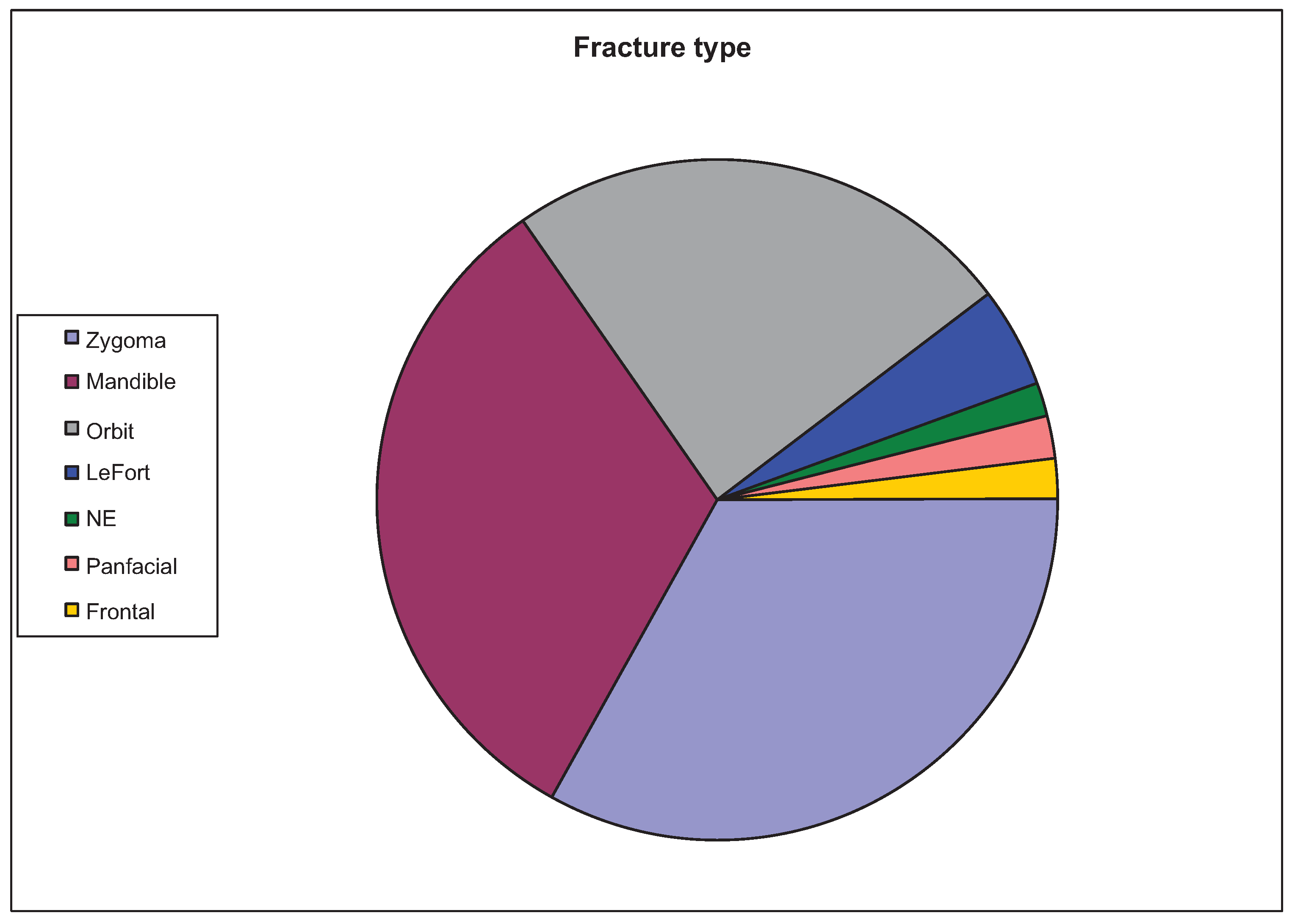
Regarding fracture type, zygomatic complex fractures accounted for 33.2%, mandible fractures for 32%, and orbit fractures for 24.5%; 4.8% were Le Fort fractures; 2%, panfacial fractures; 1.9% frontal fractures; and 1.6% NE complex fractures (
Figure 3). Of the total number of patients, 25% had at least two associated fractures: the most common association were orbit and malar (18.9% of all patients), followed by malar and mandible (6%).
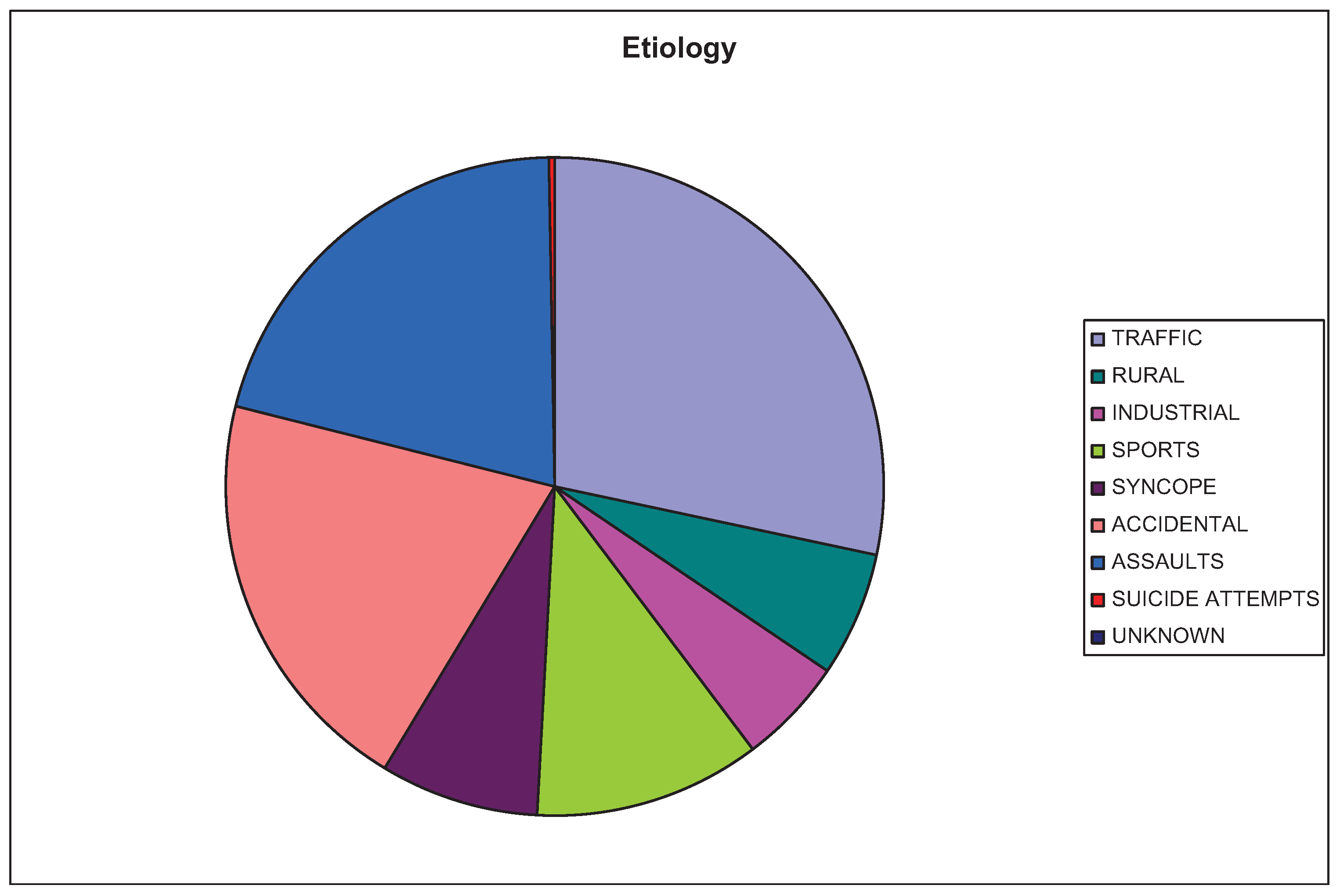
In this study, the major cause of injury was traffic accidents (27%, 6.7% of them were motorcycle accidents), which was followed by other causes such as assaults (20.5%), accidental traumas (20.1%), sportsrelated accidents (11%), syncopes (7.8%), rural accidents (6.1%, of which 3.3% were machinery-related and 2.8% related to domestic animals), industrial accidents (5.1%), suicide attempts (0.3%); in 1.1% of the patients, it was impossible to ascertain the etiology, due to an incomplete medical history and to the inability to contact the patient (
Figure 4).
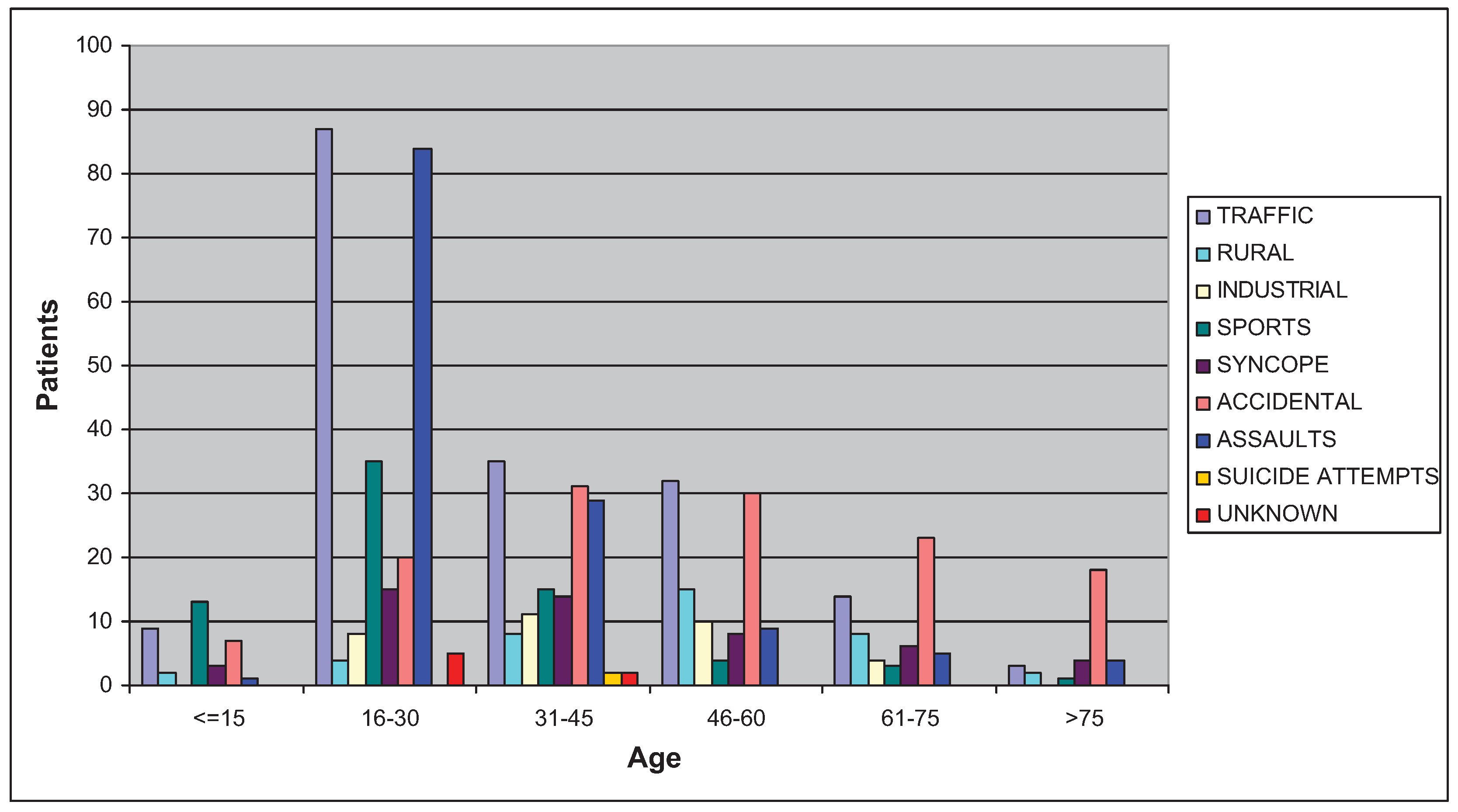
The male:female ratio for each cause was always higher than 1, ranging from 43 in assaults, 9.7 in motorcycle accidents, and 7.9 in sports, to 2.3 in syncopes and 2.1 in accidental traumas. There was no fracture due to industrial accidents in females. Comparing the most common causes in each age interval, we observe that under 16 years, the main causes were sports (37.1%) and traffic accidents (25.7%); between 16 and 60 years, traffic accidents; and over 60 years the cause was predominantly accidental traumas (
Figure 5). We have found statistically significant differences in the following
aspects: sports-related fractures decreased with age and the frequency of accidental traumas increased in a direct proportion with the age of the patient (p < 0.001 for both significances); industrial accidents and assaults were more common in males (
p < 0.016 and 0.000, respectively), whereas accidental traumas and syncopes were more common in females (
p < 0.017 and 0.000, respectively). The percentage of fractures due to traffic accidents in the first five years of the study was lower than that in the three last ones (
p < 0.004), the inflexion point being 2006, after the implementation of driving license points system in Spain.
Discussion
The etiology of facial fractures varies with time and the geographic region. The main described causes have been traffic accidents, altercations, sports, falls, and wars. In recent decades, a change has taken place in the etiology of these fractures [
1,
2], parallel to a change in the habits and to society development. The different results observed in the literature are due to differences in the way of life, economic development, and other factors related to the studied population [
3,
4]. An important factor is the legislation in terms of road safety and alcohol consumption in each country. Thus, for example, in Iran, where traffic rules are less strict and too much stress is not made in the use of the seatbelt, traffic accidents account for a very important percentage of all facial fractures [
5]. In the United States, the enforcement of traffic rules has decreased the number of traffic accidents [
6] and in Zimbabwe, where very few people have a motor vehicle, a very small percentage of all fractures are due to this cause [
7]. The traffic accidents mortality in Spain has decreased by 14.5% due to the implementation of the driving license points system [
8].
Traditionally, the main cause of facial fractures has been traffic accidents [
9,
10], and it remains so in many developing countries, followed in second place by assaults. Nevertheless, in some developed countries, altercations are emerging as the most common etiology, followed by traffic accidents. In different series published in the United Kingdom [
11], France [
2], United States [
12], Denmark [
13], Japan [
14], Middle East [
15], and New Zealand [
16], traffic accidents are still the main cause, whereas in other series from Zimbabwe [
7], Sweden [
17], and Finland [
18], altercations predominate over any other etiology.
In our study, traffic accidents represent the most frequent cause, closely followed by assaults, coinciding with the results of other published series [
2,
11] More studies have already reflected the high percentage of traffic accident deaths in our region, Galicia, compared with the rest in our country. In one study [
19], the number of deaths due to traffic accidents per 100 million vehiclekilometers traveled was higher than the Spanish mean in three of the four Galician provinces, and one of these was the Spanish province with the highest rate (Lugo). Some factors that influence this are our climatology, geography, and highway infrastructure (the low proportion of high capacity roads).
Though a statistically significant increase has not been observed in the percentage of fractures due to assaults during the period from 2001 to 2008, there has been a decrease in the percentage of fractures arising due to traffic accidents, from 2006, after the implementation of driving license points system in Spain; this suggests that the enforcement of traffic rules might bring about a decrease in the percentage of fractures due to this etiology.
The third most frequent cause was accidental traumas, with a percentage very close to that of altercations. Though fractures due to accidental traumas were always more frequent than those due to altercations, except in the age group of 16 to 30 years, the latter included 40.1% of the total number of patients.
In the literature, we find sports-related accidents accounting for between 6 and 33% of facial fractures [
10,
20]; our results coincided with the literature (11%). Almost one-half of the fractures for sports involved patients between 16 and 30 years of age.
Fractures due to syncope represented 7.8%; of these, 58% involved patients from 16 to 45 years of age, especially those related to epileptic crisis from 16 to 30 years and for episodes involving alcohol in both the age groups. Nevertheless, those older than 75 years are at the highest risk of fracture due to syncope (12.5% of all fractures in this group).
A distinctive aspect in our series was the relatively high percentage of fractures due to rural accidents (6.1%). Among this 6.1%, 3.3% of the fractures were related to domestic animals, mainly cows and horses, and the other 2.8% to tractors and working tools such as agricultural machinery, tools to cut wood, and others similar to them. Most of these fractures are located in the midface, mainly in the zygomatic complex. This etiology is not reflected as a single category in a majority of the series in the literature because of the very low percentage they account for. This is due to socioeconomic characteristics of the population our center covers, with an important weight of agricultural and livestock sectors. Although the medical assistance for our patients’ trauma used the latest advances in facial surgery such as endoscopy for condylar fractures or resorbable osteosynthesis plates [
21], the low industrial development in our region led to this characteristic pattern. No other series in the reviewed literature of Western countries showed this kind of distribution.
Industrial accidents accounted for only 5.1% of all the observed fractures, probably because they are remitted to private hospitals contracted by insurance companies.
Alcohol consumption is an aspect to be taken into account in the etiology of facial fractures. It may be involved in traffic accidents, accidental falls, syncopes, and, very often, in altercations. In many cases, the patients attribute the fracture to an accidental fall, hiding alcohol consumption by them or by a potential aggressor if an assault. On the other hand, we do not routinely realize toxin analyzes and many of our patients come to us from other centers days or even weeks after having suffered the trauma. Therefore, it is difficult to verify in how many fractures is alcohol consumption involved. But there is no doubt that it is a factor playing an important role in facial trauma and, despite its involvement in traffic accidents is decreasing because of the enforcement of traffic rules, it continues having a close relation.
With regard to age and sex, the higher incidence in young males is a repeated result in the majority of the series, and also in ours. The male:female ratio in our series (4.9:1) coincided with that in other studies from countries culturally similar, such as United Kingdom and France (5:1) [
2]. In other countries, this relation can reach even 11:1, as in Arabic countries [
22], due to social differences between men and women (e.g., very few women drive).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}