Introduction
Standing electric scooters (e-scooters) provide a cheap and environmentally friendly transport alternative, but also elicit substantial concern regarding their volume of associated injuries. The rapid uptake of e-scooters in the developed world since their 2017 ride-sharing launch corresponds with increasing reports of associated injuries from Australia, [
1] Denmark, [
2] England, [
3] Finland, [
4] France, [
5] Germany, [
6] New Zealand, [
7] Singapore, [
8] South Korea, [
9] Sweden [
10] and the United States. [
11]
Previous retrospective analyses have described a wide range of craniofacial injuries associated with e-scooters, including bony fractures, dental injuries, soft tissue injuries and traumatic brain injuries. [
4,
12] Injury to the craniofacial region is especially concerning as involvement of adjacent vital intracranial structures may be life-threatening, [
13] injury to local sensory or motor structures can impair function, [
13] and the visibility of facial defects can have important psychological impacts. [
14]
This will be the first systematic review exploring this emerging area of concern. It aims to investigate the demographics, risk factors, types of injury and surgical management of craniofacial trauma associated with e-scooters. Better understanding of this area will aid preventive strategies and surgical planning, resulting in improved patient care and resource allocation.
Discussion
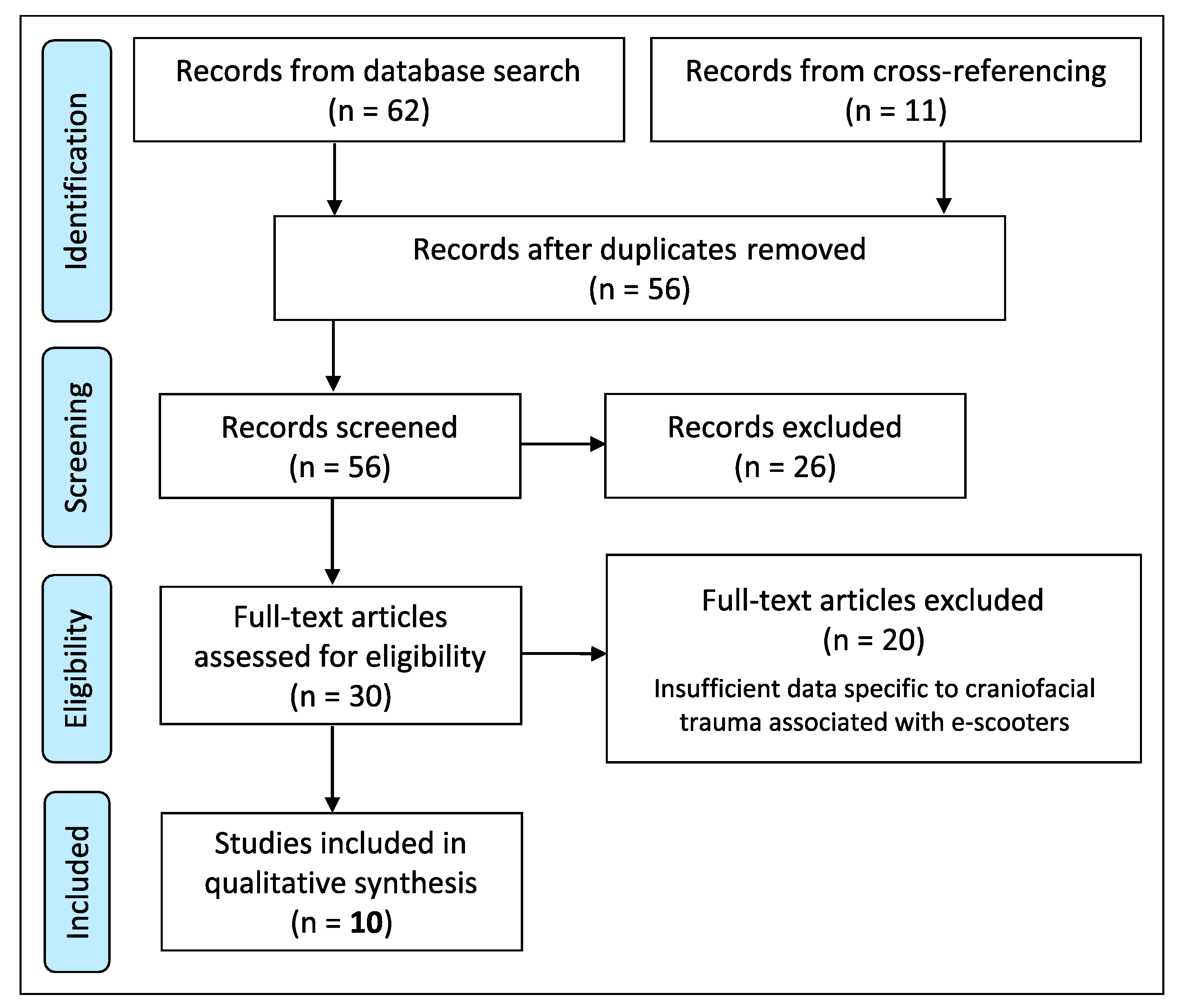
This is the first PRISMA-guided systematic review exploring the demographics, risk factors, types of injury and surgical management of craniofacial trauma associated with e-scooters.
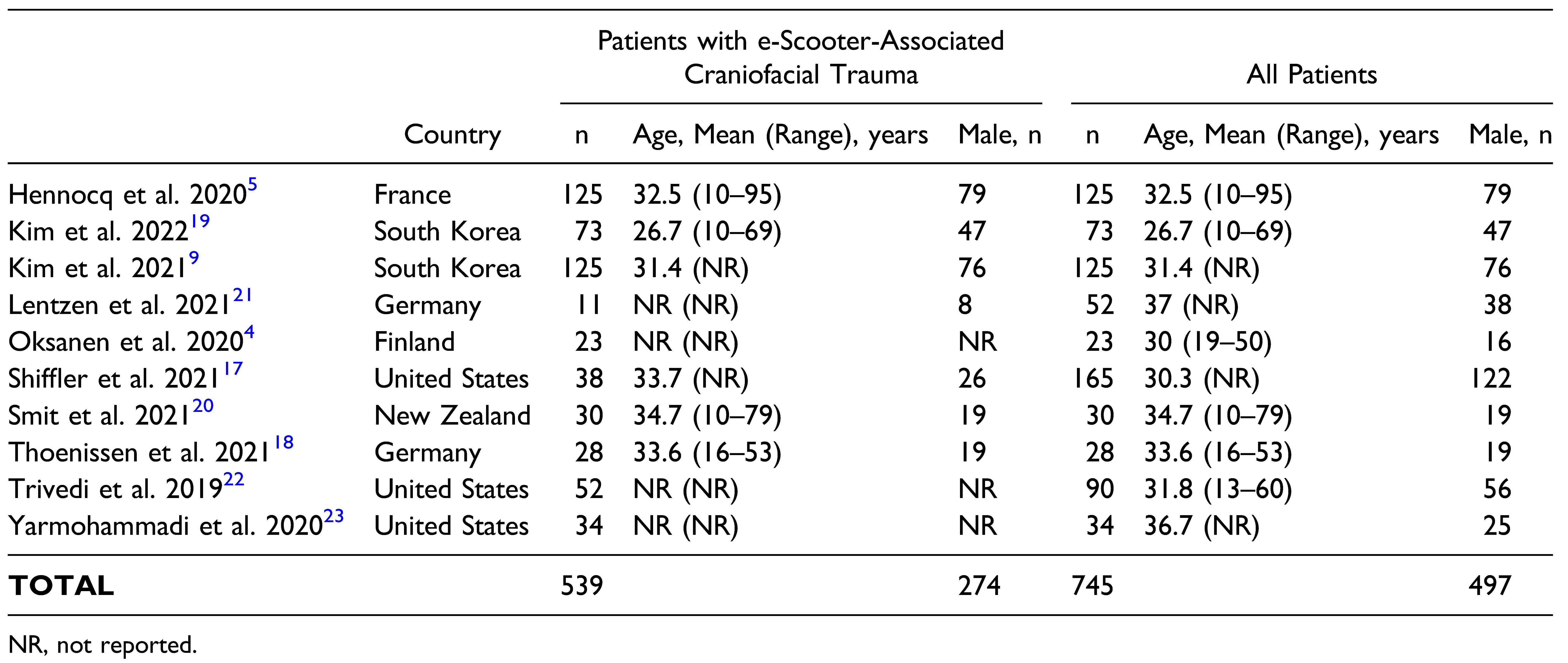
E-scooter use demographics favour a younger adult population with an approximate 2:1 male-to-female ratio, [
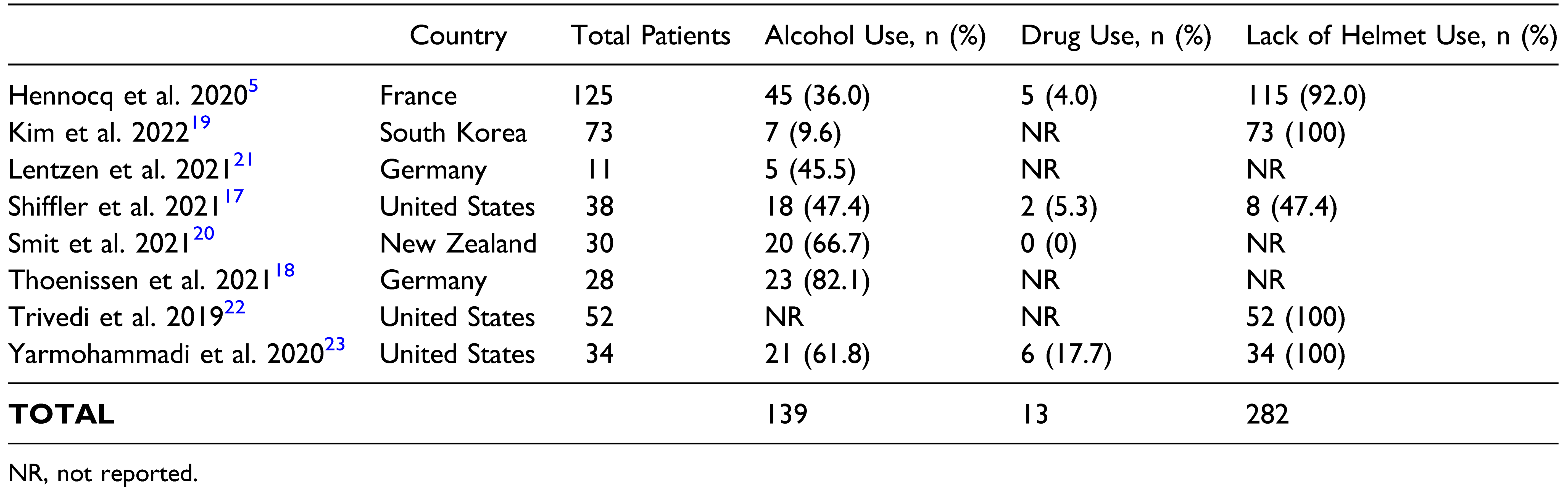
24] which is reflected in this review with patients having a mean age of 31.5 years and 63.7% being male. Significant risk factors for these injuries were alcohol/drug intoxication (
P < .01) and the absence of distal extremity injuries (
P ≤ .03). Lack of helmet use was also a common risk factor, with helmet use reported in less than 1 in thirty patients. These risk factors are similar to those reported for bicycle and electronic bicycle (e-bike) accidents, where traumatic brain injury (TBI) is significantly more likely in the setting of alcohol intoxication. [
25] Helmet use is also an established significant protective factor in bicycle accidents against head injuries [
26] and facial fractures. [
27] Alcohol causes impaired judgement, as well as compromised neuromuscular reflexes for head protection such as an outstretched limb to brace against a fall, which was the most common mechanism of injury reported in this review. The latter corresponds with the absence of distal extremity injuries as a significant risk factor. Additionally, intoxicated patients have been found to be significantly less likely to wear helmets. [
28] Awareness of these risk factors contributes to prevention strategies and improved screening for such injuries in e-scooter accidents, with the aim of improving patient outcomes.
These risk factors can also have important legal implications, in terms of local regulation and commercial promotion. Of the ten studies included, 7 were conducted after the local launch of ride-sharing e-scooters, which was 2017 in the United States, [
17,
22,
23] 2018 in New Zealand [
20] and 2019 in Finland [
4] and Germany [
18,
21]; while 3 studies included data before and after the transition, which was 2018 in France [
5] and South Korea. [
9,
19] This reflects growing interest in the relatively recent phenomenon of e-scooter injuries. Accordingly, there are still significant and evolving variations in national legislations relating to categorical definition of e-scooters as a micro-vehicle and allowed areas of use, helmet use and insurance laws, as well as speed and age limits. [
24] From a commercial viewpoint, the degree of emphasis that e-scooter companies place on safety for their products and campaigns is an important consideration. Content analyses of e-scooter market leader Bird’s Instagram account in 2017–2019 revealed minimal photographic or textual feature of protective gear, with concerns that this may normalise unsafe riding behaviours in e-scooter users. [
29,
30] This is also an evolving space, with Bird’s current website displaying numerous prominent photographic and textual mention of helmet use. [
31]
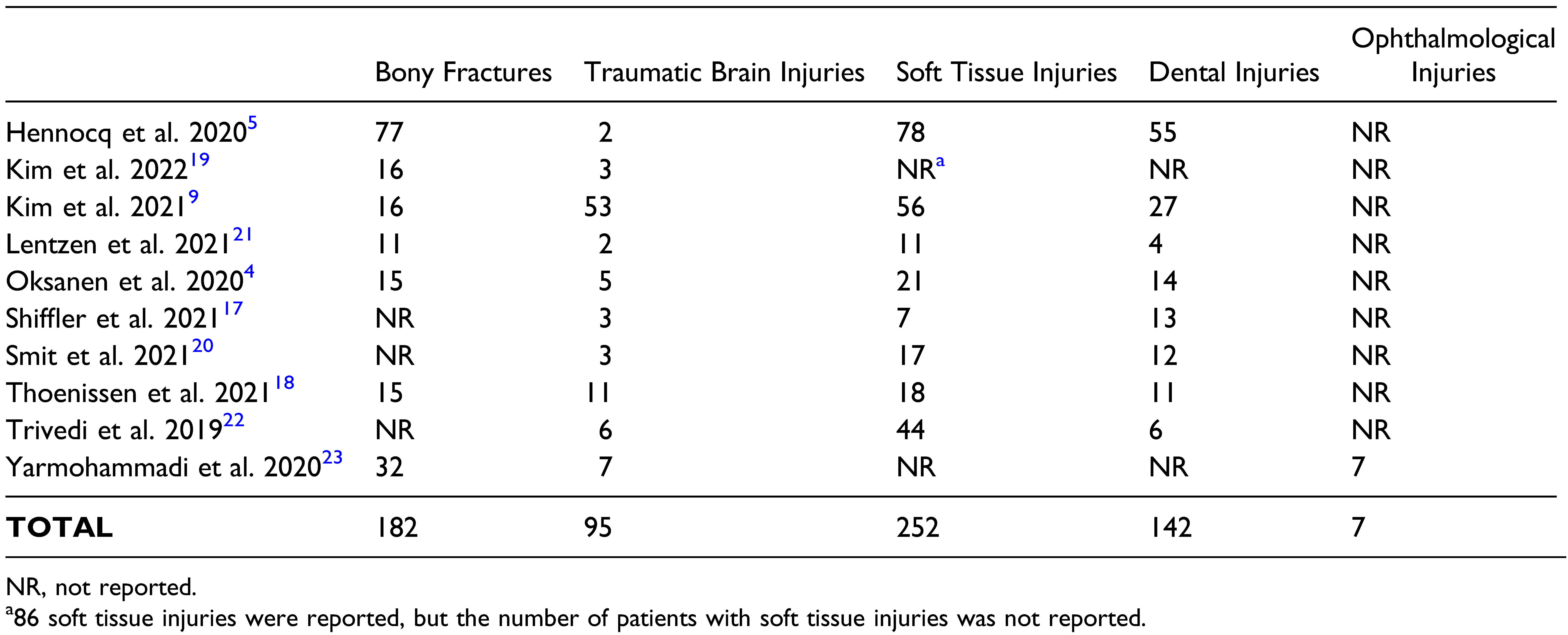
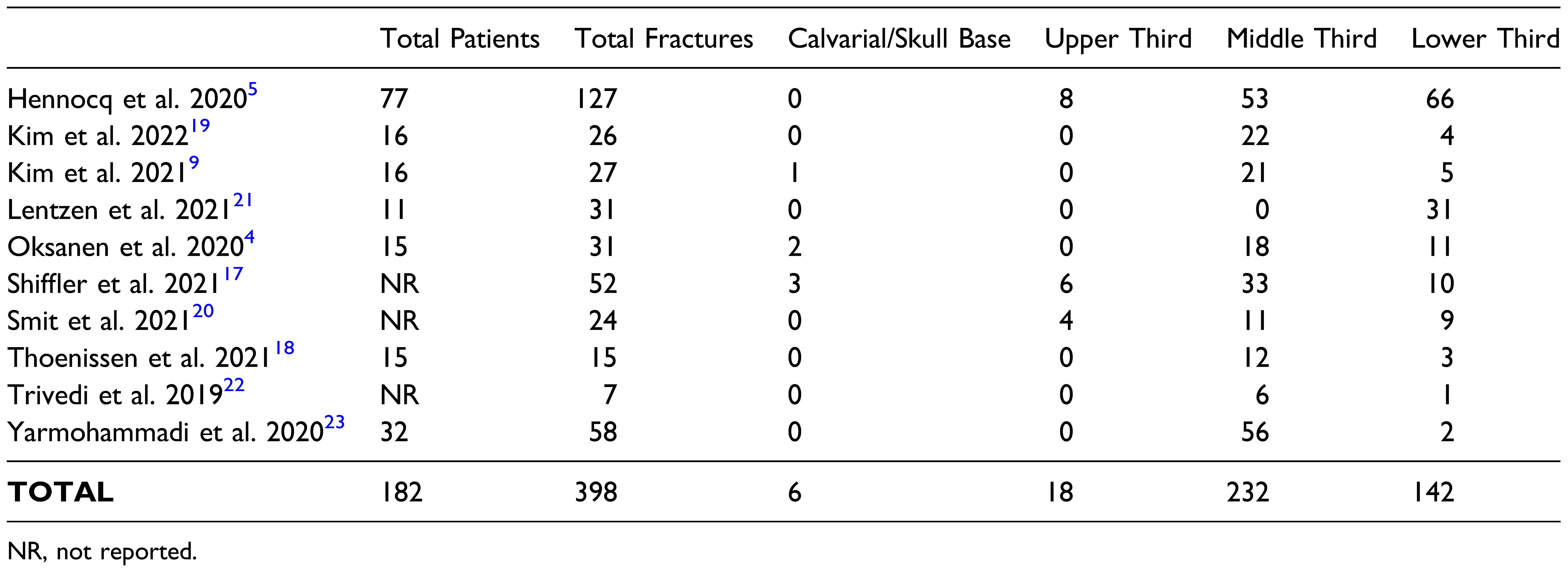
The types of injuries described in this review consisted of bony fractures and TBI, as well as soft tissue, dental and ophthalmological injuries. Almost 1 in 5 patients had a TBI (n = 95 of 539) but only 2 patients were explicitly reported to have had concomitant TBI and facial fractures. This is an important distinction due to the significant potential for morbidity and mortality in these combined injuries, with common patient factors being males in their thirties, traffic accidents and middle third fractures. [
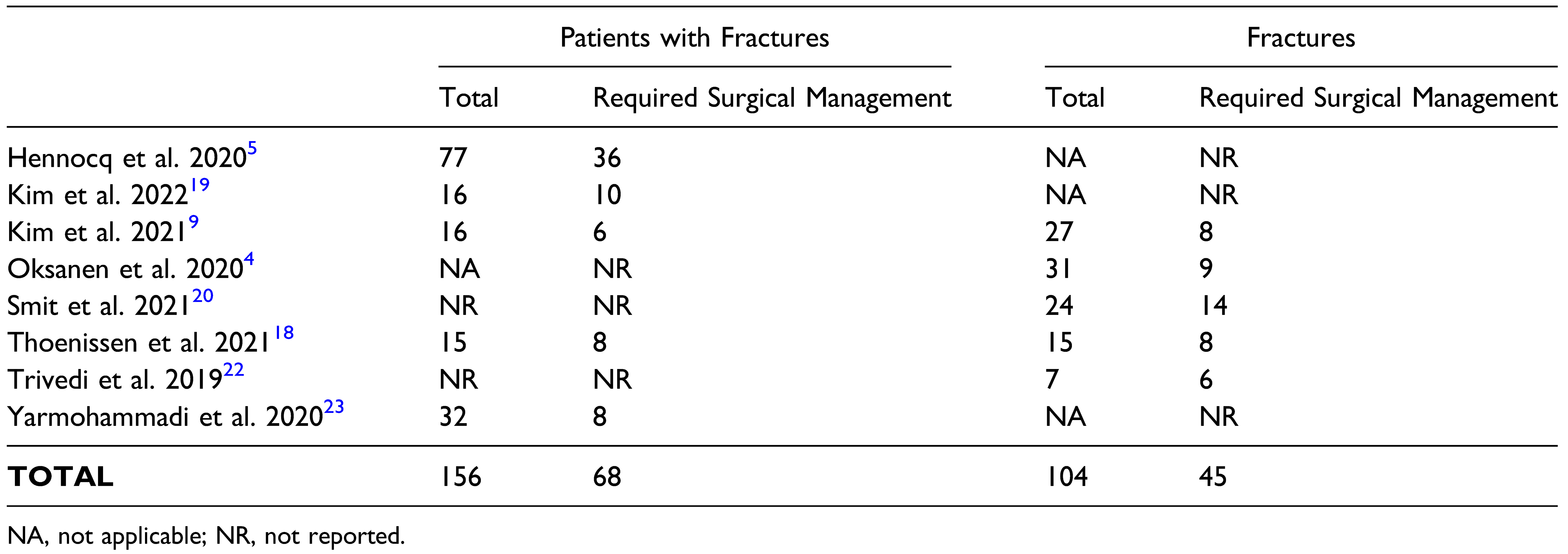
32] These were also commonly reported demographics in this review, with a 63.7% male proportion and an average age of 31.5 years, all mechanisms of injury being e-scooter accidents, and the most common fracture pattern being middle third fractures. Surgical delay is a significant risk factor for complications in patients with combined TBI and facial fractures, so increased awareness is important for prophylactic management of post-operative sequelae. [
32] In this review, surgical management was required for approximately 4 in ten patients for facial fractures; however, there were minimal data reported for risk factors predisposing surgical management, and none for post-operative complications. Soft tissue and dental injuries were common, and represent important subsets of craniofacial trauma due to associated functional and aesthetic implications. Ophthalmological sequelae of e-scooter accidents have been understudied and should be an important area of future research in considering the potential for substantial visual morbidity.
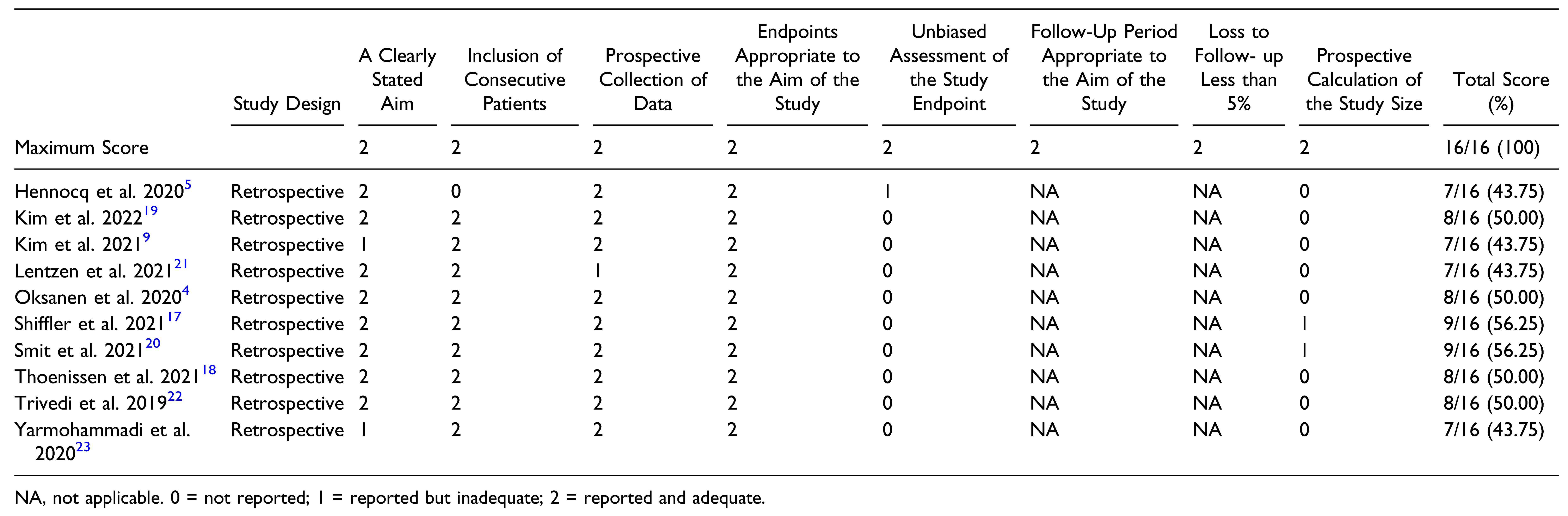
This study has several limitations. At the review level, the small number of included studies makes it difficult to draw firm conclusions from the findings, although they can contribute to future research direction. This is particularly relevant to the lack of studies investigating risk factors for surgical management or post-operative complications, as well as variation in reporting in relation to the review’s parameters of interest. However, this is unsurprising considering the recent nature of e-scooter use, and more comprehensive longitudinal studies relevant to this area may be anticipated in the near future. At the study level, quality assessment with MINORS found a moderate level of evidence overall. Areas for future improvement include prospective data collection, prospective sample size calculation and unbiased endpoint assessment.
In conclusion, the findings of this review suggest common presentations for craniofacial trauma associated with e-scooters. Important risk factors are alcohol/drug intoxication, absence of distal extremity injuries and lack of helmet use. Further investigations utilising robust longitudinal designs with standardised descriptions of types of injuries are required. Gaps in knowledge relate to surgical management, post-operative complications and associated risk factors.


{kind=link}