Introduction
Traumatic injury is one of the established causes of blindness [
1]. The first documented relationship between facial injury and loss of vision was made by Hippocrates 2641 years ago [
2,
3]. In the last 2 decades, various investigators have reported the incidence of this uncommon but handicapping injury to be between .32% and 20.4% [
3,
4,
5]. Its rarity is attributable to a prominent bony orbit, protective reflexes such as blinking, hand deflection to protect the eyes and globe resilience [
6].
In 2018, Stathopoulos and colleagues [
3] retrospectively reviewed 5708 patients with facial trauma over a 27-year period in Greece. They found 19 (.33%) cases of unilateral blindness, and retrobulbar haemorrhage was the most common cause of blindness. Facial gunshot injury was strongly associated with loss of sight, and zygomatic complex (ZMC) fracture was the most frequent facial injury. Similarly, Beogo et al [
7] in Burkina Faso studied 970 patients who presented with maxillofacial fractures over a 10-year period. They reported 13 eyes of 10 (1.1%) patients (7 unilateral and 3 bilateral) with vision loss. In their series, interpersonal violence was significantly associated with blindness compared with other accidental aetiological factors. Naso–orbito–ethmoid (NOE) complex fracture was the most implicated fracture type, and globe rupture (or perforation) was the most common cause of blindness.
The only study in Nigeria that specifically documented blindness following facial trauma was a single institutional retrospective study of 295 patients with mid-facial injury published in 2006 [
4]. Thirty two (10.8%) of these patients had unilateral visual loss with ruptured globe as the most common cause of blindness and facial gunshot injury as the most frequent mechanism of trauma. The most common fracture type associated with blindness in this series was ZMC fracture. After 15 years, another study to determine the current epidemiology of blindness from facial trauma is necessary. Besides, the incidence of blindness in the report of Ugboko et al [
4] was in a segment of the Nigerian population and may not be representative of the sociogeographical diversity of the entire Nigerian population. We opine that a multi-centre Nigerian study will project a national picture on the current prevalence, mechanism of injury and aetiology of facial trauma related blindness.
The objective of this multi-centre study, therefore, was to determine the prevalence, pattern and mechanism of facial trauma associated with blindness among Nigerians. Findings from this study will be useful in formulating primary and secondary preventive policies with regards to allocating appropriate resources to and planning for the optimal management of these patients. The multi-centre nature of the study will allow for extrapolation of results to different regions of the country.
Materials and Methods
This was a collaborative, retrospective study of all patients with blindness resulting from facial trauma that were managed by maxillofacial surgeons and ophthalmologists in 4 Nigerian public tertiary health facilities between January 2010 and December 2019. The study was approved by the Ethics and Research Committee of Obafemi Awolowo University Teaching Hospital Complex (OAUTHC), Ile-Ife (Protocol number: ERC/2020/07/13).
All cases of major facial injury comprising facial bone fractures and soft tissue injuries that required in-patient maxillofacial surgical care were identified. Only patients with facial bony and/or soft tissue injuries with blindness in at least one eye were included in the study. These patients were examined by ophthalmologists at presentation and managed in each collaborating centre. At presentation, visual acuity and intraocular pressure were assessed and recorded, as well as other ophthalmic examination findings. Requested radiological investigations were ocular ultrasound scan, craniofacial or facial computed tomography scan and plain radiographs. Blindness was defined as presenting visual acuity worse than 3/60 (or 20/200) [
8]. Information retrieved from individual patients’ records included age, sex, ethnic group, mechanism of facial trauma, interval before presentation, visual acuity, clinical diagnosis, aetiology of blindness and ophthalmic treatments. Patients with preexisting blindness and blindness secondary to surgical intervention or blind eye(s) at presentation due to causes other than the current facial trauma were excluded from the study. Data analysis was done using IBM SPSS Statistics (version 21.0 for windows, IBM© Inc, Chicago, IL, USA). Descriptive statistics were applied for prevalence, categorical and continuous data. Categorical data was reported as frequencies and percentages. The Kolmogorov– Smirnov test was done to assess the normality of distribution of continuous data. Continuous variables were reported as means with standard deviations. Chi-square test was used to compare mechanisms of facial trauma with respect to aetiology of blindness. The mechanisms of facial trauma were categorised into 2 groups (traffic accident facial trauma and non-traffic accident facial trauma) to facilitate inferential statistical analysis.
P value of <.05 was set as significant level.
Results
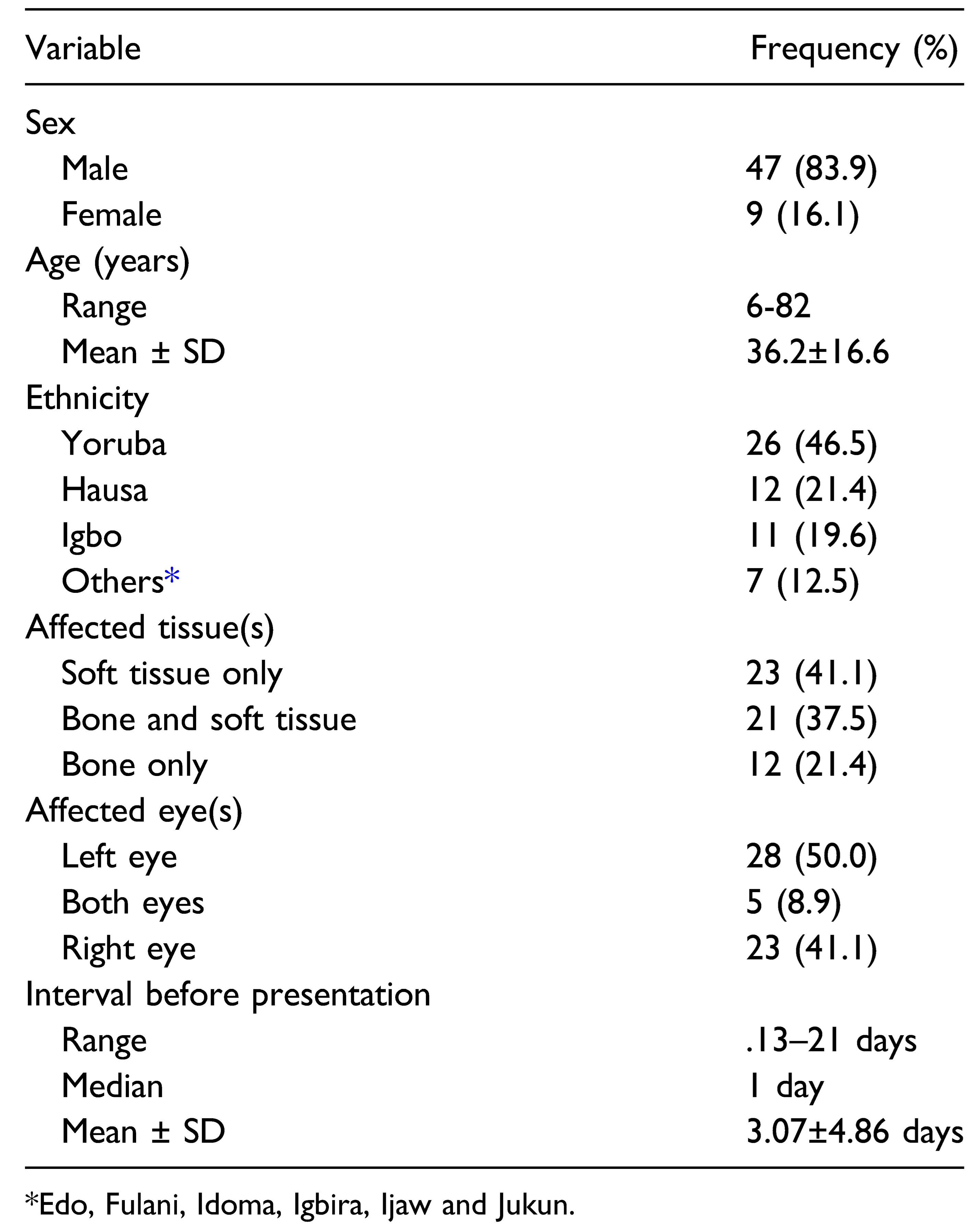
The participating centres were OAUTHC, Ile-Ife and University of Nigeria Teaching Hospital, Nsukka (UNTH) from southern Nigeria; and Ahmadu Bello University Teaching Hospital, Zaria (ABUTH) and National Hospital Abuja (NHA) from northern Nigeria. From these hospitals, a total of 2070 patients presented with facial trauma requiring in-patient surgical care during the study period. Of these, 56 (2.7%) patients presented with associated blindness in at least one eye. There were 51 (91.1%) unilateral cases and 5 (8.9%) bilateral cases of patients presenting at initial visits with visual acuity worse than 3/60. Forty-seven (83.9%) of these patients were males with female-to-male ratio of 1:5.2. The mean age (SD) at presentation was 36.2 (16.6) years (
Table 1).
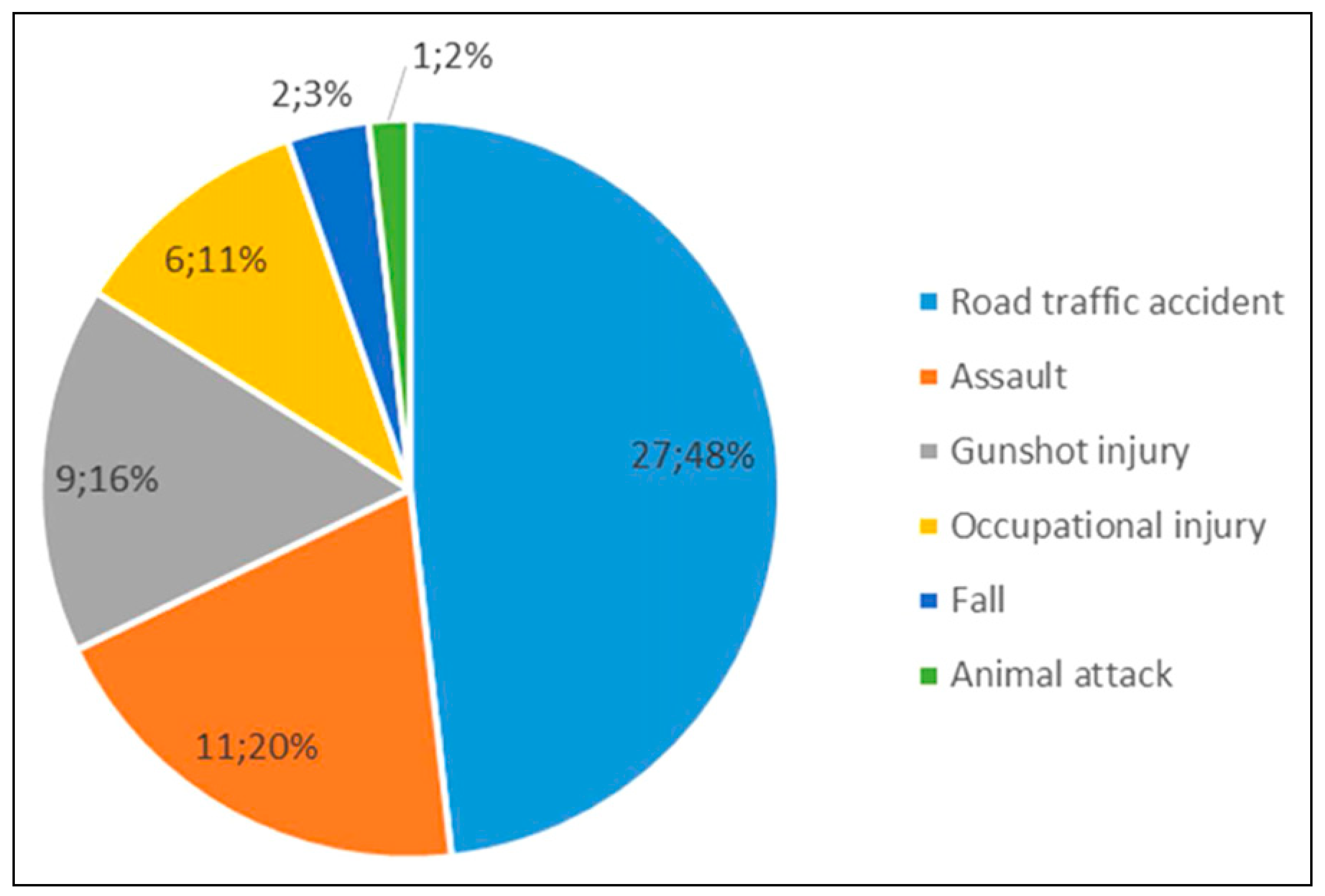
Road traffic accident (n = 27; 48%) was the leading mechanism of injury while assault and gunshot injury were responsible for 20% (n = 11) and 16% (n = 9) of facial bone fractures and soft tissue injuries, respectively, in these patients (
Figure 1).
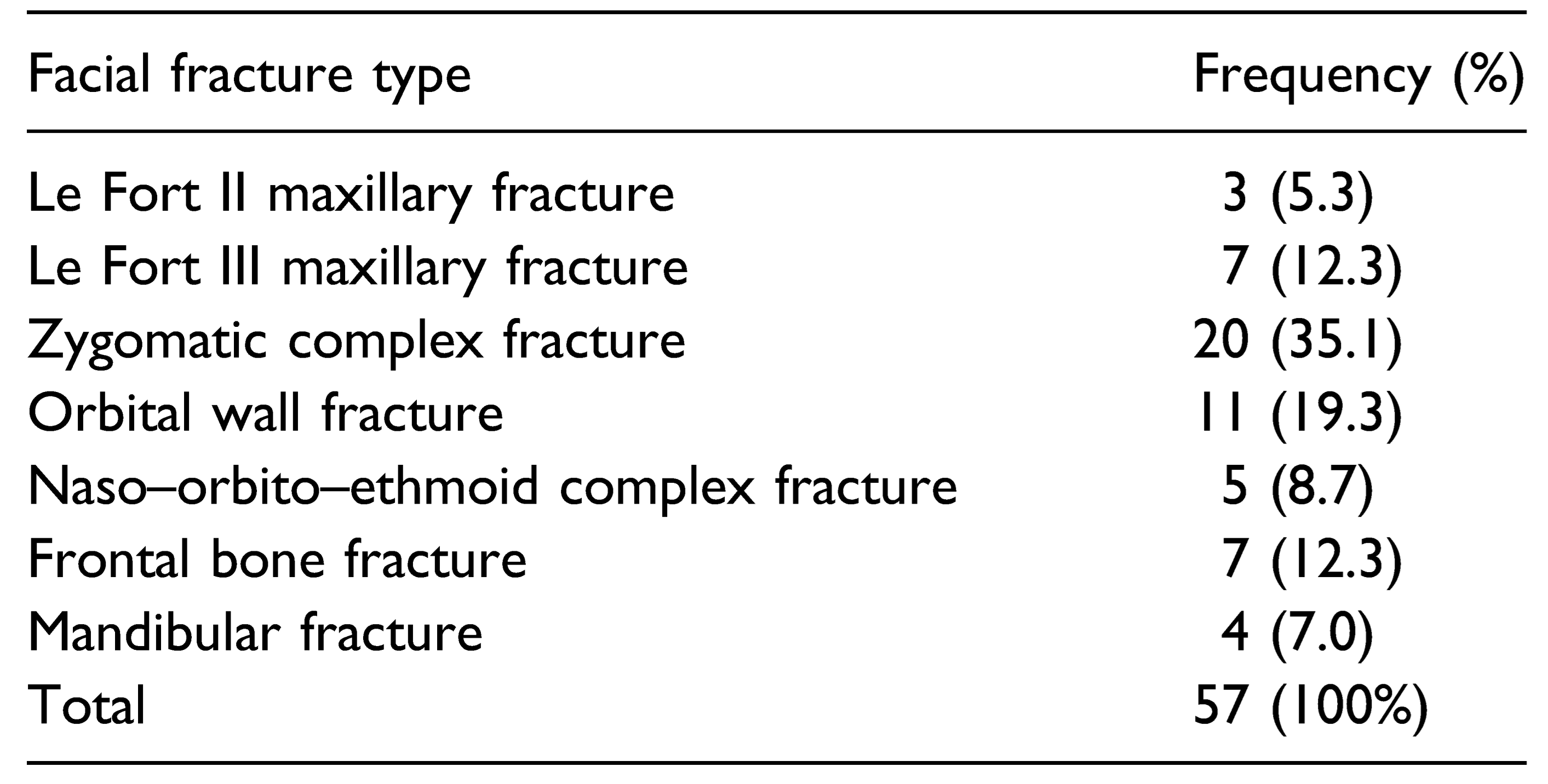
A total of 57 facial bone fractures (16 single, 20 double and 7 triple fractures) were recorded in 33 patients. Of the 33 patients, 12 patients had only bone injury, while 21 patients had a combination of bone and soft tissue injuries. The commonest facial bone fracture associated with blindness was zygomatic complex fracture (
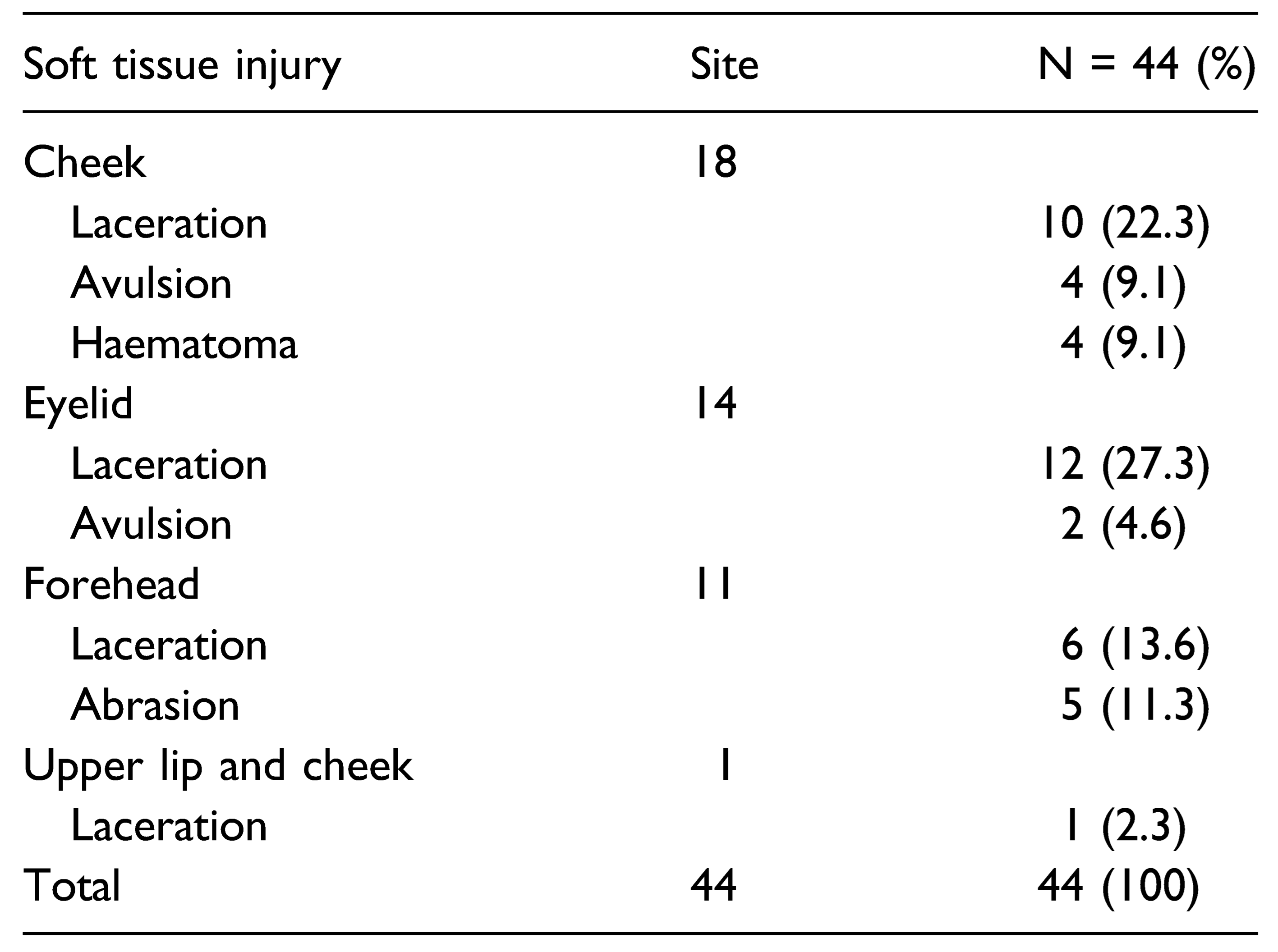
Table 2). Altogether, 44 (78.6%) patients sustained facial soft tissue injuries with/ without facial fractures (23 patients had soft tissue injuries only and 21 patients had both bone and soft tissue injuries).
Soft tissue injuries were mostly to the cheek (n = 18; 40.9%) and eyelid (n = 14; 31.9%) with eyelid laceration as the commonest soft tissue wound (
Table 3).
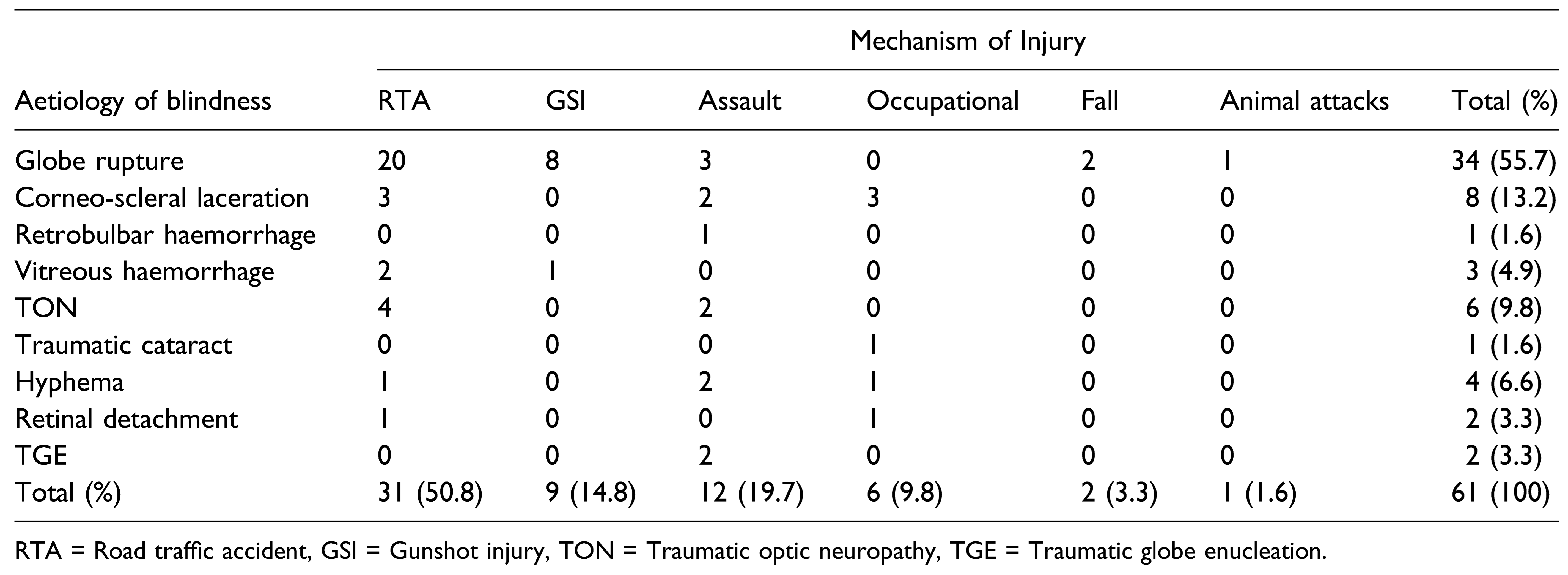
Sixty-one eyes of 56 (61/112; 54.5%) patients were blind following facial trauma. Twenty-eight (28/56; 50%) patients were blind in their left eye only, 23 (23/56; 41.1%) in their right eye only and 5 (5/56; 8.9%) in both eyes. Of the 61 blind eyes, 39 (63.9%) were caused by open globe injuries, 18 (29.5%) were caused by closed globe injuries and 4 (6.6%) were from atypical injury types (2 eyes [3.3%] each traumatized by intraocular foreign body and traumatic globe enucleation was observed in an assaulted patient).
Globe rupture (n = 34) was the commonest cause of blindness accounting for 55.7% of the affected eyes (
Table 4). There was no statistically significant difference (
P = .189) between aetiology of blindness in traffic accident facial trauma (n = 31; 50.8%) and non-traffic accident facial trauma (n = 30; 49.2%). In addition, globe rupture was the leading aetiology of blindness for both groups.
Facial soft tissue lacerations and avulsion were repaired by primary closure (n = 29; 65.9%) and local flaps (n = 4; 9.1%). Four cheek haematomas were evacuated (n = 4; 9.1%). Facial bone fractures were reduced and fixed using standard fixation techniques. Ophthalmic treatments included surgical intervention for 53 (67.2%) eyes and nonsurgical treatment for 12 (19.7%) eyes. Six (9.8%) eyes could not be treated because the patients declined surgery, and for 2 (3.3%) eyes, the patients died from other injuries prior to receiving treatment. The commonest ophthalmic surgical procedure performed was evisceration (
Figure 2). Twelve (12/29; 41.4%) patients had ocular prosthesis postenucleation and evisceration.
Discussion
Facial trauma is a subject of sustained interest in maxillofacial surgery and ophthalmology because of the muchdreaded loss of vision as well as its associated aesthetic and psychological complications. In this study, we reviewed patients with uniocular and binocular blindness in at least one eye following facial injuries at four public tertiary hospitals in Nigeria. The interval before presentation in this series suggests a relatively earlier pattern compared with maxillofacial trauma and road traffic accident cases in Nigeria and other developing countries [
9]. This pattern lends credence to the respect accorded the eye and the dread of visual impairment in the Nigerian setting.
We found the prevalence of blindness arising from facial injury at collaborating centres located in northern and southern Nigeria to be 2.7%. This indicates that blindness from facial injuries is fairly common among Nigerians. This is similar to a prevalence of 2.9% reported by Ioannides et al [
10] at a University hospital in the Netherlands, but higher than .33% and 1.52% documented by Stathopoulos et al [
3] and Ansari, [
6] respectively. This being the first national, multi-centre study on blindness from traumatic facial injuries in Nigeria, it can only be related with previous single institution studies. Other authors like Ugboko et al [
4] in Nigeria and Ashar and colleagues [
5] in the United Arab Emirates have reported much higher incidences of blindness (10.8% and 20%, respectively). In our opinion, the discrepancies in the literature stem from a combination of methodology which includes visual impairments as blindness [
4,
11] and other selection bias like focusing on patients with midfacial and orbital fractures and exclusion of patients with other facial injuries [
5,
10,
12,
13].
Most of the patients with traumatic blindness in the present study were males and younger than 40 years of age. This finding is similar to reports of previous studies on this subject [
3,
4,
5,
6,
7]. It is of great concern that most patients with blind eyes were adult males in the productive age group which could have negative economic consequences. This finding implies that individuals younger than 40 years could serve as the target population for instituting preventive measures for blindness from facial injuries. The trend in the mechanisms of injury in this study implicated road traffic accidents, assault and gunshot injury as the leading causes of traumatic blindness. This is similar to the reports of Beogo et al [
7] and Ansari [
6]. Facial injuries resulting in blindness were caused by road traffic accidents in about half of reviewed patient population. This is not unexpected as road traffic accidents are known to inflict high energy impacts on the facial skeletons with attendant ocular morbidity [
3,
6,
7].
With respect to facial injuries that resulted in blindness, more than half of the patients with blind eyes also sustained facial skeletal and soft tissue injuries. Eyelid laceration and zygomatic complex fractures were the commonest facial soft tissue and bone injuries associated with blindness in this study. We attribute this pattern to the protective effect and proximity of these structures to the eyeball, and consequently, any damage to them render the eye more vulnerable to blindness from facial trauma. Expectedly, almost all previous studies of blindness associated with facial injury reported zygomatic complex fractures as the predominant facial fractures [
3,
4,
6,
7]. Also, eyelid laceration as a common presentation in both open and closed globe injuries may be suggestive of severe ocular injury that requires thorough evaluation [
1].
Globe rupture was the commonest cause of unilateral and bilateral blindness from facial trauma in this series. And it was mainly caused by blunt force trauma, this finding could be related to the fact that road traffic accidents (which is a cause of blunt trauma) was the predominant mechanism for facial trauma in this study. This finding is consistent with reports from Ugboko et al [
4] and Beogo et al [
7] who found globe rupture to be the commonest ophthalmic injury leading to blindness. This is, however, in contrast to the findings of Ansari [
6] in Iran and Stathopoulos et al [
3] in Greece where retrobulbar haemorrhage was the leading cause of blindness after facial injury. The difference in aetiology of blindness may probably be attributable to the difference in mechanism of facial injury and accuracy of ophthalmic diagnosis [
11].
While the surgical management of ocular injuries typically occurs at the earliest time upon presentation (as emergency sight saving procedure), an interval before presentation in the hospital (3.07 ± 4.86 days) is often built into the time frame in our settings (
Table 1). Although this study did not capture timing of the management of ocular and facial injuries, a team approach (ophthalmologists and maxillofacial surgeons) aimed at achieving the maximum possible repair at a single operating room session is often adopted. The exceptions would however be where this is not feasible or when intervention is adjudged to be detrimental to an excellent outcome. In this situation, surgical management of ocular trauma was done before the repair of facial fractures.
More than two-thirds of the blind eyes required surgical treatments of which more than half were eye enucleations or eviscerations. Trauma is the main indication of eye removal surgeries in both northern [
14] and southern [
15] Nigeria. However, in developed countries, the indication for most surgical eye removal procedure was unsalvageable eyes with orbito-ocular tumours [
16]. The psychological complication of blindness attributable to changes in lifestyles and habits necessitates psychosocial care along with ophthalmic treatments [
17]. Although there were reported cases of sight recovery after treatment in some patients with blindness from facial trauma, eyesight was not recovered in any of the patients in our study as evidenced by the post-treatment visual acuity [
18].
Limitation and Future Perspective
This is a hospital-based epidemiologic study of blindness resulting from facial injury. Aside from the nonparticipating hospitals, we acknowledge that a number of cases may not have presented in the hospital at all. As such, it is likely that prevalence of blindness from facial trauma in Nigeria is even higher than our finding. This is because some patients may not present at any of the collaborating centres for management.
Future research should focus on prospective, multicentre studies to determine the correlation between traumatic blindness and/or visual impairment and specific facial injuries.
 ,
, 


{kind=link}
{kind=link}