The Prediction Capacity 3-D Software, on a 2-D Analysis, in Planning the Positioning of the Upper Lip After Maxillary Advancement
 ,
,
Abstract
:Introduction
Materials and Methods
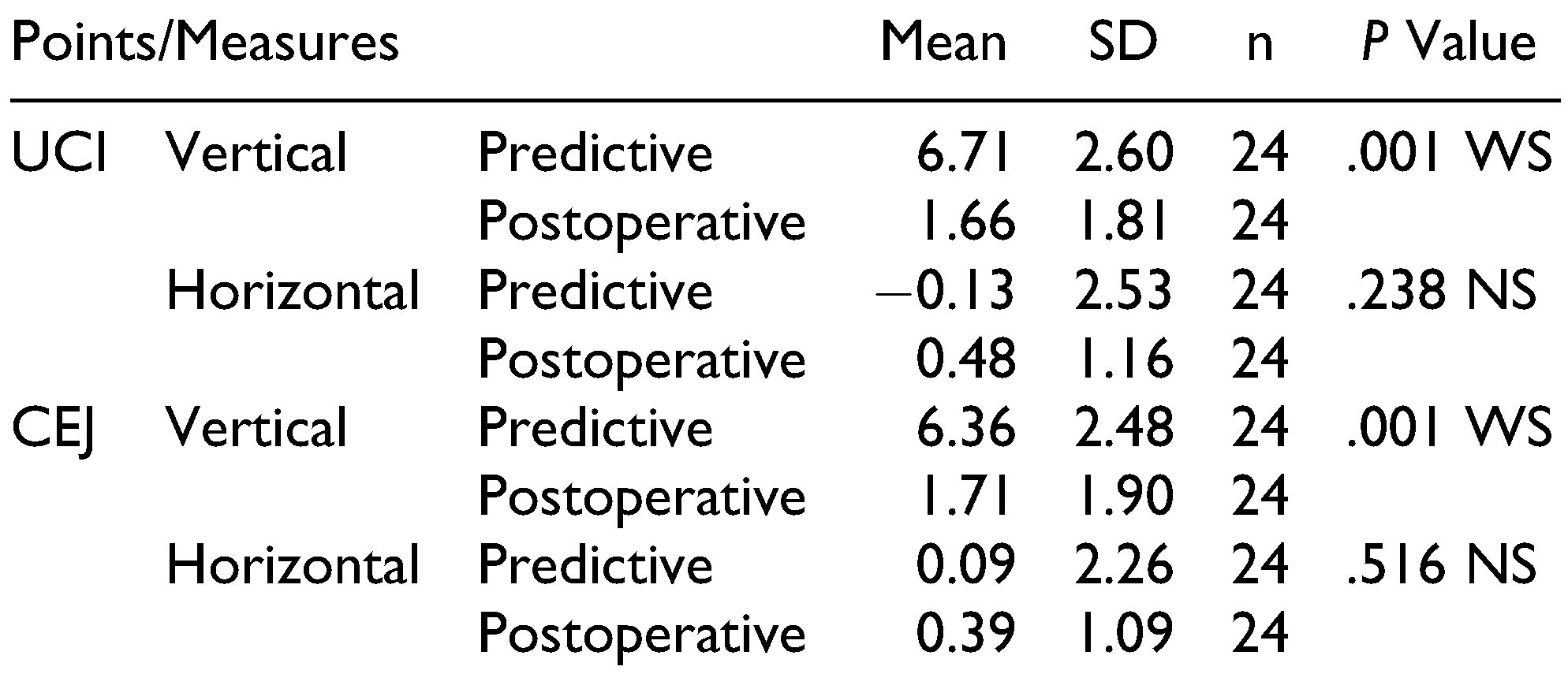
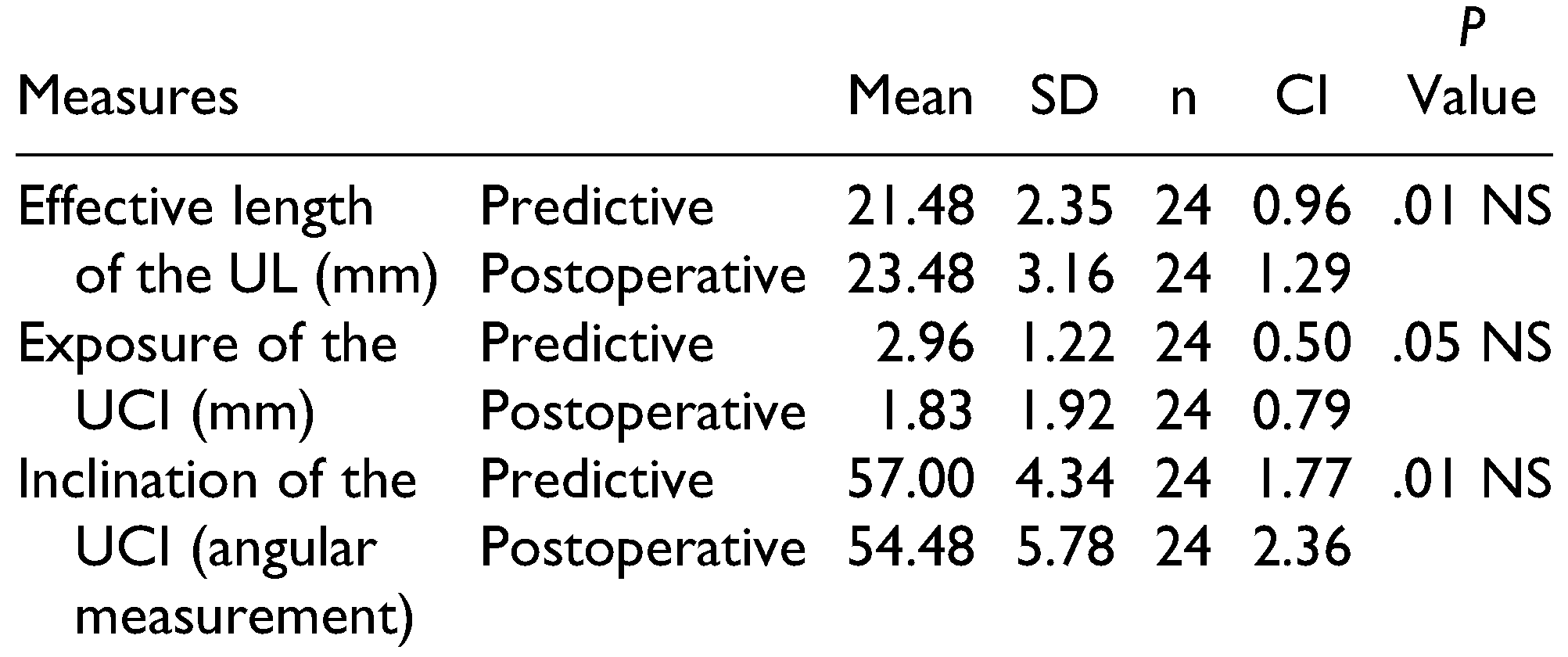
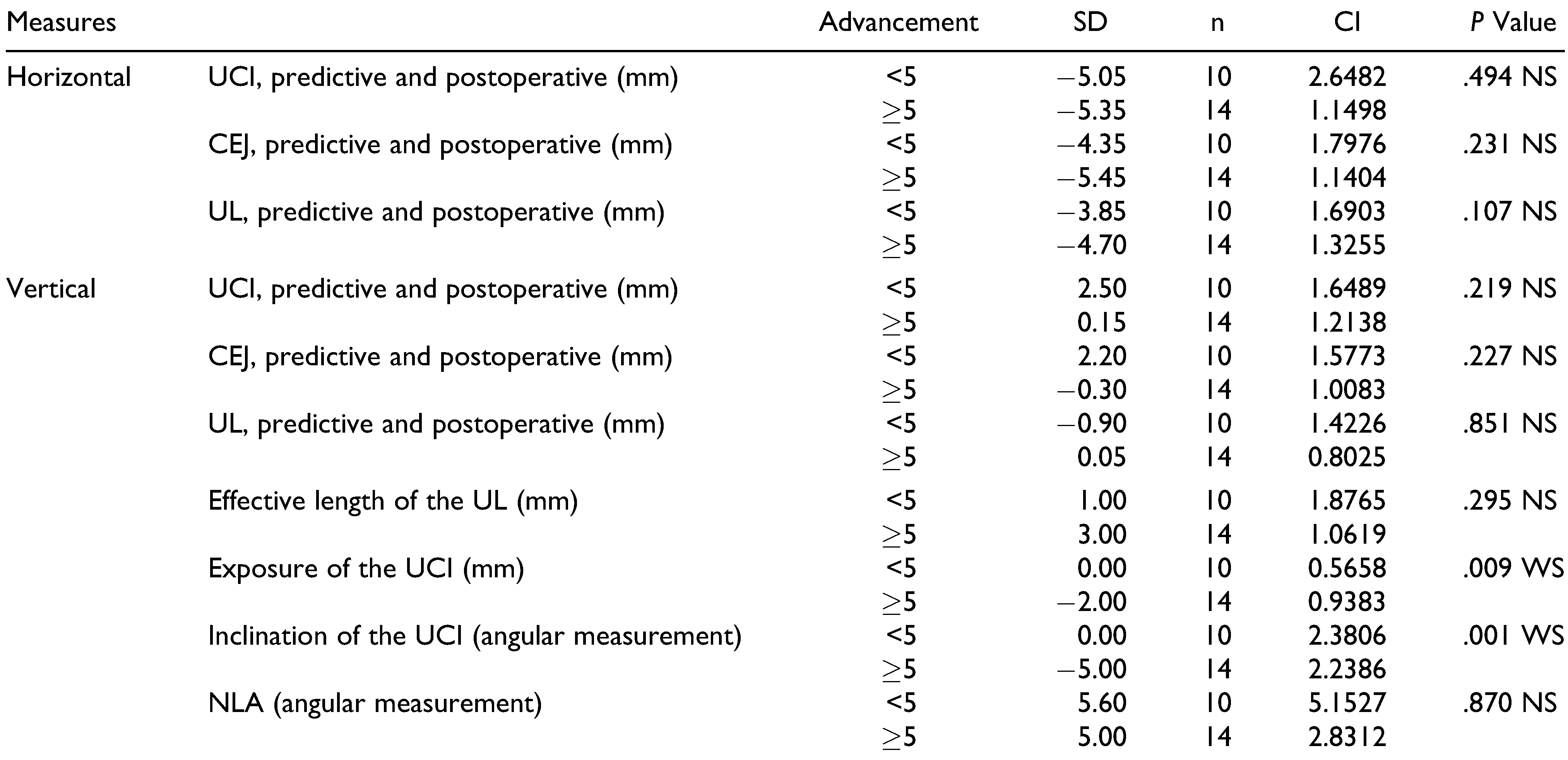
Results
Discussion
Conclusion
Funding
Conflicts of Interest
References
- Shafi, M.I.; Ayoub, A.; Ju, X.; Khambay, B. The accuracy of three-dimensional prediction planning for the surgical correction of facial deformities using Maxilim. Int J Oral Maxillofac Surg. 2013, 42, 801–806. [Google Scholar]
- Rosen, H.M. Lip-nasal aesthetics following Le Fort I osteotomy. Plast Reconstr Surg. 1988, 81, 171–182. [Google Scholar] [PubMed]
- McFarlane, R.B.; Frydman, W.L.; McCabe, S.B.; Mamandras, A.M. Identification of nasal morphologic features that indicate susceptibility to nasal tip deflection with the Le Fort I osteotomy. Am J Orthod Dentofacial Orthop. 1995, 107, 259–267. [Google Scholar] [PubMed]
- Bailey, L.J.; Collie, F.M.; White, R.P., Jr. Long-term soft tissue changes after orthognathic surgery. Int J Adult Orthodon Orthognath Surg. 1996, 11, 7–18. [Google Scholar]
- Stella, J.P.; Streater, M.R.; Epker, B.N.; Sinn, D.P. Predictability of upper lip soft tissue changes with maxillary advancement. J Oral Maxillofac Surg. 1989, 47, 697–703. [Google Scholar] [PubMed]
- Mitchell, C.; Oeltjen, J.; Panthaki, Z.; Thaller, S.R. Nasolabial aesthetics. J Craniofac Surg. 2007, 18, 756–765. [Google Scholar]
- Uribe, F.; Janakiraman, N.; Shafer, D.; Nanda, R. Three-dimensional cone-beam computed tomography-based virtual treatment planning and fabrication of a surgical splint for asymmetric patients: Surgery first approach. Am J Orthod Dentofacial Orthop. 2013, 144, 748–758. [Google Scholar]
- Adolphs, N.; Liu, W.; Keeve, E.; Hoffmeister, B. Rapid splint: Virtual splint generation for orthognathic surgery—Results of a pilot series. Comput Aided Surg. 2014, 19, 20–28. [Google Scholar]
- Olate, S.; Zaror, C.; Mommaerts, M.Y. A systematic review of soft-to-hard tissue ratios in orthognathic surgery. Part IV: 3D analysis—Is there evidence? J Craniomaxillofac Surg. 2017, 45, 1278–1286. [Google Scholar]
- Nkenke, E.; Vairaktaris, E.; Kramer, M.; et al. Three-dimensional analysis of changes of the malar-midfacial region after Le Fort I osteotomy and maxillary advancement. Oral Maxillofac Surg. 2008, 12, 5–12. [Google Scholar]
- Nadjmi, N.; Tehranchi, A.; Azami, N.; Saedi, B.; Mollemans, W. Comparison of soft-tissue profiles in Le Fort I osteotomy patients with Dolphin and Maxilim softwares. Am J Orthod Dentofacial Orthop. 2013, 144, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Sant’Ana, E.; Souza, D.P.E.; Temprano, A.B.; Shinohara, E.H.; Faria, P.E.P. Lingual short split: A bilateral sagittal split osteotomy technique modification. J Craniofac Surg. 2017, 28, 1852–1854. [Google Scholar] [CrossRef]
- Arnett, G.W.; Jelic, J.S.; Kim, J.; et al. Soft tissue cephalometric analysis: Diagnosis and treatment planning of dentofacial deformity. Am J Orthod Dentofacial Orthop. 1999, 116, 239–253. [Google Scholar] [CrossRef] [PubMed]
- Araujo, A.; Schendel, S.A.; Wolford, L.M.; Epker, B.N. Total maxillary advancement with and without bone grafting. J Oral Surg. 1978, 36, 849–858. [Google Scholar] [PubMed]
- Louis, P.J.; Waite, P.D.; Austin, R.B. Long-term skeletal stability after rigid fixation of Le Fort I osteotomies with advancements. Int J Oral Maxillofac Surg. 1993, 22, 82–86. [Google Scholar] [CrossRef]
- Costa, F.; Robiony, M.; Sembronio, S.; Polini, F.; Politi, M. Stability of skeletal Class III malocclusion after combined maxillary and mandibular procedures. Int J Adult Orthodon Orthognath Surg. 2001, 16, 179–192. [Google Scholar]
- Dahlberg, G. Statistical methods for medical and biological students. Br Med J. 1940, 2, 358–359. [Google Scholar]
- Sun, Y.; Luebbers, H.T.; Agbaje, J.O.; et al. Accuracy of upper jaw positioning with intermediate splint fabrication after virtual planning in bimaxillary orthognathic surgery. J Craniofac Surg. 2013, 24, 1871–1876. [Google Scholar] [CrossRef]
- Zhang, N.; Liu, S.; Hu, Z.; Hu, J.; Zhu, S.; Li, Y. Accuracy of virtual surgical planning in two-jaw orthognathic surgery: Comparison of planned and actual results. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016, 122, 143–151. [Google Scholar] [CrossRef]
- Tweed, C.H. A philosophy of orthodontic treatment. Am J Orthod. 1945, 31, 74–103. [Google Scholar] [CrossRef]
- Chew, M.T. Soft and hard tissue changes after bimaxillary surgery in Chinese Class III patients. Angle Orthod. 2005, 75, 959–963. [Google Scholar] [PubMed]
- Muradin, M.S.; Seubring, K.; Stoelinga, P.J.; vd Bilt, A.; Koole, R.; Rosenberg, A.J. A prospective study on the effect of modified alar cinch sutures and V-Y closure versus simple closing sutures on nasolabial changes after Le Fort I intrusion and advancement osteotomies. J Oral Maxillofac Surg. 2011, 69, 870–876. [Google Scholar] [PubMed]
- Khamashta-Ledezma, L.; Naini, F.B. Systematic review of changes in maxillary incisor exposure and upper lip position with Le Fort I type osteotomies with or without cinch sutures and/or VY closures. Int J Oral Maxillofac Surg. 2014, 43, 46–61. [Google Scholar] [PubMed]
- Jeon, J.H. Timing of orthognathic surgery: Paradigm shift by surgery-first approach? J Korean Assoc Oral Maxillofac Surg. 2017, 43, 61–62. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
 |
 |
 |
 |
 |
© 2020 by the author. The Author(s) 2020.
Share and Cite
Chihara, L.L.; Segantin, J.d.F.; Faria, P.E.P.; Sant’Ana, E.; Dias-Ribeiro, E.; Nogueira, R.L.M.; Ferreira-Júnior, O. The Prediction Capacity 3-D Software, on a 2-D Analysis, in Planning the Positioning of the Upper Lip After Maxillary Advancement. Craniomaxillofac. Trauma Reconstr. 2020, 13, 93-98. https://doi.org/10.1177/1943387520906670
Chihara LL, Segantin JdF, Faria PEP, Sant’Ana E, Dias-Ribeiro E, Nogueira RLM, Ferreira-Júnior O. The Prediction Capacity 3-D Software, on a 2-D Analysis, in Planning the Positioning of the Upper Lip After Maxillary Advancement. Craniomaxillofacial Trauma & Reconstruction. 2020; 13(2):93-98. https://doi.org/10.1177/1943387520906670
Chicago/Turabian StyleChihara, Letícia Liana, Jéssica de Fátima Segantin, Paulo Esteves Pinto Faria, Eduardo Sant’Ana, Eduardo Dias-Ribeiro, Renato Luiz Maia Nogueira, and Osny Ferreira-Júnior. 2020. "The Prediction Capacity 3-D Software, on a 2-D Analysis, in Planning the Positioning of the Upper Lip After Maxillary Advancement" Craniomaxillofacial Trauma & Reconstruction 13, no. 2: 93-98. https://doi.org/10.1177/1943387520906670
APA StyleChihara, L. L., Segantin, J. d. F., Faria, P. E. P., Sant’Ana, E., Dias-Ribeiro, E., Nogueira, R. L. M., & Ferreira-Júnior, O. (2020). The Prediction Capacity 3-D Software, on a 2-D Analysis, in Planning the Positioning of the Upper Lip After Maxillary Advancement. Craniomaxillofacial Trauma & Reconstruction, 13(2), 93-98. https://doi.org/10.1177/1943387520906670