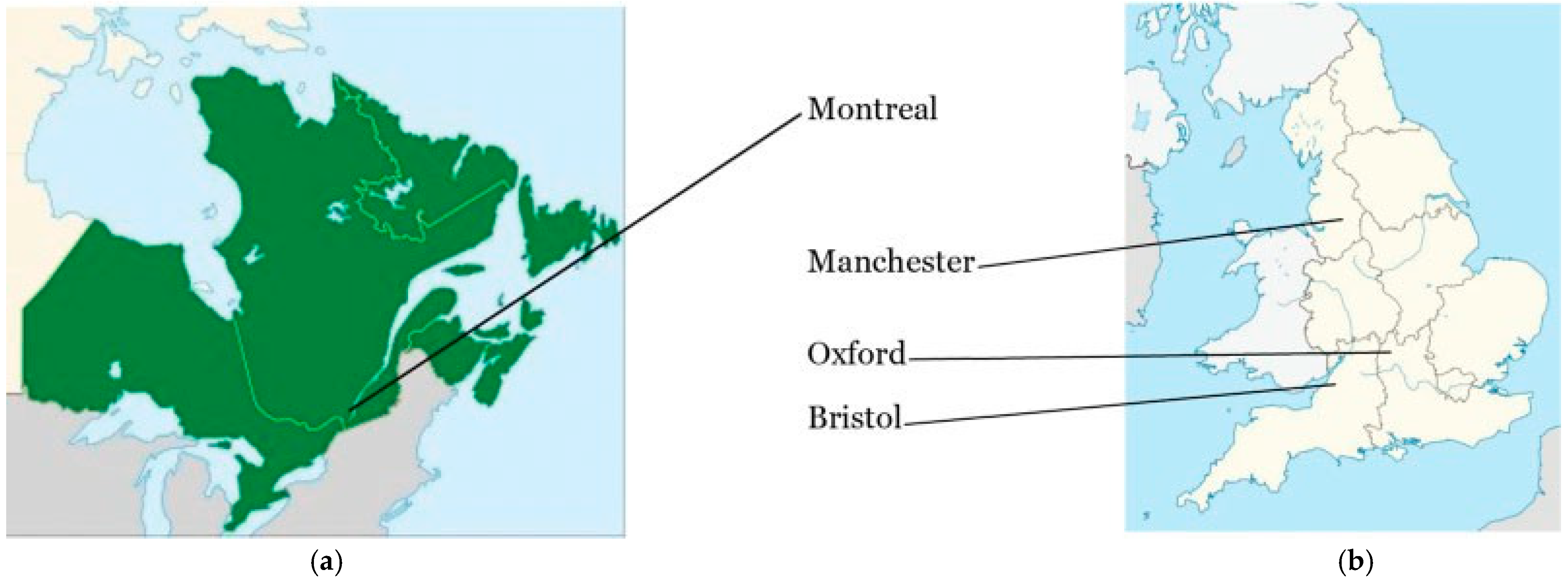
Anatomical Revelations in 1921 Kindled Operative Repair of the Orbit, Eyelids, and Periorbit over the Ensuing 100 Years: The Diuturnity of Ernest Whitnall (1876–1950) of Oxford, Montreal, and Bristol
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
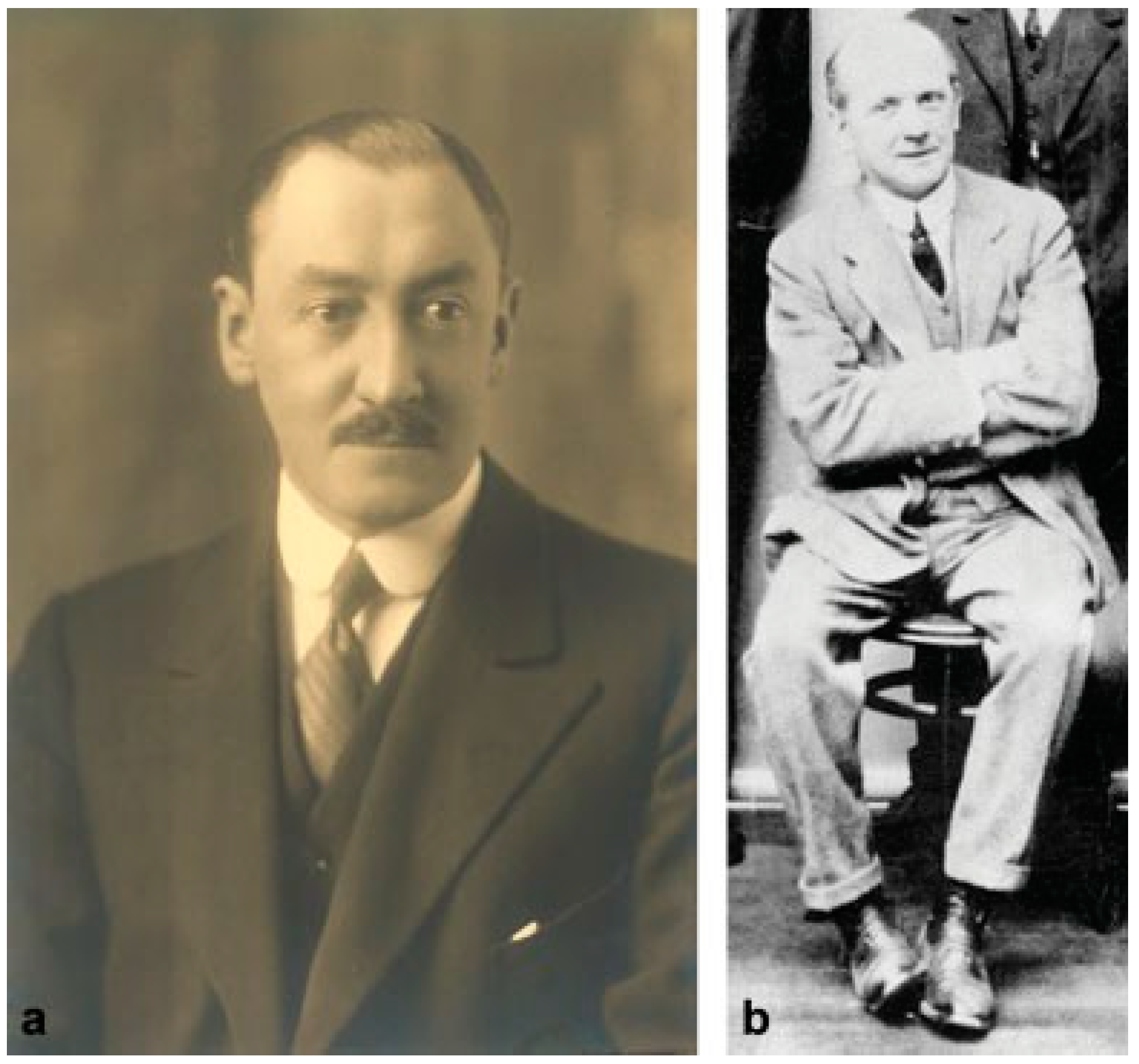
:Samuel Ernest Whitnall (1876–1950)
- “On a tubercle on the malar bone … [for] lateral attachment of the tarsal plate” [8].
- “On a ligament acting as a check to the action of the levator palpebral superioris muscle” [9].
Discussion
An Afterword
Acknowledgments
Conflicts of Interest
References
- Shin, E.K.; Meals, R.A. The historical importance of the hand in advancing the study of human anatomy. J Hand Surg Am 2005, 30, 209–221. [Google Scholar] [PubMed]
- Le Fort, R. Etude experimental sur les fractures de la machoire superieure. Rev Chir Paris 1901, 23, 208–227. [Google Scholar]
- Testut, J.L. Traite d’Anatomie Humaine, 2nd ed.; Doin: Paris, France, 1911. [Google Scholar]
- Testut, J.L. Anatomica Humanica, 3rd ed.; Doin: Torino, Italy, 1943. [Google Scholar]
- Cryer, M.H. Internal Anatomy of the Face; Lea & Febiger: Philadelphia, PA, USA, 1916. [Google Scholar]
- Pollock, R.A. (Ed.) Buttresses of the craniomaxillofacial skeleton. In Craniomaxillofacial Buttresses: Anatomy and Operative Repair; Thieme: New York, NY, USA, 2012. [Google Scholar]
- Whitnall, S.E. The Anatomy of the Human Orbit and Accessory Organs of Vision; Henry Frowde and Hodder & Stoughton: London, UK, 1921. [Google Scholar]
- Whitnall, S.E. On a tubercle on the malar bone, and on the lateral attachments of the tarsal plates. J Anat Physiol 1911, 45 Pt 4, 426–432. [Google Scholar]
- Whitnall, S.E. A ligament acting as a check to the action of the levator palpebral superioris muscle. J Anat Physiol 1911, 45 Pt 2, 131–139. [Google Scholar]
- In memoriam: Samuel Ernest Whitnall, M.A., M.D., B.Ch. (Oxon), M.R.C.S., L.R.C.P. (Lond.). J Anat 1950, 84, 395–396.
- Hanaway, J.; Cruess, R.L. McGill Medicine: The Second Half-Century, 1885–1936; McGill-Queen’s University Press: Montreal, QC, Canada, 2008; Volume 2. [Google Scholar]
- Bourguet, J. Les hernies graisseuses de l’orbite: Notre traitement chirurgical. Bull Acad Natl Med 1924, 92, 1227–1232. [Google Scholar]
- Bourguet, M.D.J. The pioneer in aesthetic surgery of the neck. Clin Plast Surg 1983, 10, 363–365. [Google Scholar]
- Converse, J.M.; Smith, B. Reconstruction of the floor of the orbit by bone grafts. Arch Ophthalmol 1950, 44, 1–21. [Google Scholar] [CrossRef]
- McCoy, F.J. Management of the orbit in facial fractures. Plast Reconstr Surg 1957, 19, 236–245. [Google Scholar]
- Smith, B.; Converse, J.M. Early treatment of orbital floor fractures. Trans Am Acad Ophthalmol Otolaryngol 1957, 61, 602–608. [Google Scholar]
- Smith, B.; Regan, W.F., Jr. Blow-out fracture of the orbit; mechanism and correction of internal orbital fracture. Am J Ophthalmol 1957, 44, 733–739. [Google Scholar] [CrossRef]
- Dingman, R.O.; Natvig, P. Surgery of Facial Fractures; WB Saunders: Philadelphia, PA, USA, 1964. [Google Scholar]
- Dingman, R.O.; Grabb, W.C.; Oneal, R.M. Management of injuries of the naso-orbital complex. Arch Surg 1969, 98, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Stranc, M.F. Primary treatment of naso-ethmoid injuries with increased intercanthal distance. Br J Plast Surg 1970, 23, 8–25. [Google Scholar] [PubMed]
- Tenzel, R.R.; Miller, G.R. Orbital blow-out fracture repair, conjunctival approach. Am J Ophthalmol 1971, 71, 1141–1142. [Google Scholar]
- Tessier, P. The conjunctival approach to the orbital floor and maxilla in congenital malformation and trauma. J Maxillofac Surg 1973, 1, 3–8. [Google Scholar] [PubMed]
- Rowe, N.L. Fractures of the orbit. Acta Stomatol Belg 1975, 72, 681–685. [Google Scholar]
- Stranc, M.F.; Robertson, G.A. A classification of injuries of the nasal skeleton. Ann Plast Surg 1979, 2, 468–474. [Google Scholar]
- Tessier, P.; Rougier, R.; Hervouet, F.; et al. Plastic Surgery of the Orbit and Eyelids (Translated by Wolfe SA); Masson USA: New York, NY, USA, 1981. [Google Scholar]
- Merville, L.C.; Real, J.P. Fronto-orbito nasal dislocations. Initial total reconstruction. Scand J Plast Reconstr Surg 1981, 15, 287–297. [Google Scholar]
- Morgan, R.F.; Manson, P.N.; Shack, R.B.; Hoopes, J.E. Management of naso-ethmoid-orbital fractures. Am Surg 1982, 48, 447–450. [Google Scholar]
- Gruss, J.S. Naso-ethmoid-orbital fractures: Classification and role of primary bone grafting. Plast Reconstr Surg 1985, 75, 303–317. [Google Scholar]
- Gruss, J.S. Complex nasoethmoid-orbital and midfacial fractures: Role of craniofacial surgical techniques and immediate bone grafting. Ann Plast Surg 1986, 17, 377–390. [Google Scholar] [PubMed]
- Paskert, J.P.; Manson, P.N.; Iliff, N.T. Nasoethmoidal and orbital fractures. Clin Plast Surg 1988, 15, 209–223. [Google Scholar] [CrossRef]
- Jackson, I.T. Classification and treatment of orbitozygomatic and orbitoethmoid fractures. The place of bone grafting and plate fixation. Clin Plast Surg 1989, 16, 77–91. [Google Scholar]
- Jackson, I.T. Orbital wall trauma. In Repair and Reconstruction in the Orbital Region; Mustarde, J.C., Ed.; Churchill Livingstone: Edinburgh, UK, 1991; pp. 361–375. [Google Scholar]
- Gossman, M.D.; Pollock, R.A. Acute orbital trauma: Diagnosis and treatment. In Oculoplastic Surgery, 3rd ed.; McCord, C.D., Jr., Tanenbaum, M., Nunery, W.R., Eds.; Raven Press: New York, NY, USA, 1994; pp. 515–552. [Google Scholar]
- Manson, P.N. Orbital fractures. In Manual of Internal Fixation in the Cranio-Facial Skeleton; Prein, J., Ed.; Springer: Berlin, Germany, 1998; pp. 139–147. [Google Scholar]
- Pollock, R.A.; Gossman, M.D. The canthofornix incision (lower eyelid “bypass”) in the management of orbital and zygomatic fractures. Craniomaxillofac Trauma 2001, 7, 13–22. [Google Scholar]
- Hollier, L.H.; Thornton, J.; Pazmino, P.; Stal, S. The management of orbitozygomatic fractures. Plast Reconstr Surg 2003, 111, 2386–2392. [Google Scholar] [CrossRef]
- Manson, P.N. The orbit after Converse: Seeing what is not there. J Craniofac Surg 2004, 15, 363–367. [Google Scholar] [CrossRef]
- Martin, M.; Rodriguez, E.; Grant, M.; Vanderkolk, C.; Manson, P. Three-point fixation of orbitozygomatic fractures: The lateral orbit. Plast Reconstr Surg 2005, 116, 605–612. [Google Scholar] [CrossRef]
- Wolfe, S.A.; Ghurani, R.; Podda, S.; Ward, J. An examination of post-traumatic, postsurgical orbital deformities: Conclusions drawn for improvement of primary treatment. Plast Reconstr Surg 2008, 122, 1870–1881. [Google Scholar] [CrossRef] [PubMed]
- Pollock, R.A.; Gossman, M.D. The lateral orbit. In Craniomaxillofacial Buttresses: Anatomy and Operative Repair; Pollock, R.A., Ed.; Thieme: New York, NY, USA, 2012; pp. 150–193. [Google Scholar]
- Stanwix, M.G.; Rodriguez, E.D. Naso-orbital-ethmoid fractures. In Essentials of Craniomaxillofacial Trauma; Marcus, J.R., Erdmann, D., Rodriguez, E.D., Eds.; Quality Medical: St. Louis, MO, USA, 2012. [Google Scholar]
- Pollock, R.A. Current principles of repair. In Craniomaxillofacial Buttresses: Anatomy and Operative Repair; Pollock, R.A., Ed.; Thieme: New York, NY, USA, 2012; pp. 29–46. [Google Scholar]
- Manson, P.N. Fronto-basilar fractures. Plast Surg Forum 1981, 4, 14. [Google Scholar]
- Pollock, R.A. The cranial vault and cranial base (frontal, sphenoid, temporal, and occipital bones). In Craniomaxillofacial Buttresses: Anatomy and Operative Repair; Pollock, R.A., Ed.; Thieme: New York, NY, USA, 2012; pp. 106–125. [Google Scholar]
- Gruss, J.S.; Pollock, R.A.; Phillips, J.H.; Antonyshyn, O. Combined injuries of the cranium and face. Br J Plast Surg 1989, 42, 385–398. [Google Scholar]
- Stanley, R.B., Jr. Management of severe frontobasilar skull fractures. Otolaryngol Clin North Am 1991, 24, 139–150. [Google Scholar] [PubMed]
- Burstein, F.; Cohen, S.; Hudgins, R.; Boydston, W. Frontal basilar trauma: Classification and treatment. Plast Reconstr Surg 1997, 99, 1314–1321. [Google Scholar] [PubMed]
- Manson, P.N.; Stanwix, M.G.; Yaremchuk, M.J.; Nam, A.J.; Hui-Chou, H.; Rodriguez, E.D. Frontobasal fractures: Anatomical classification and clinical significance. Plast Reconstr Surg 2009, 124, 2096–2106. [Google Scholar] [PubMed]
- Rudderman, R.H.; Mullen, R.L.; Phillips, J.H. Implications of finite analysis. In Craniomaxillofacial Buttresses: Anatomy and Operative Repair; Pollock, R.A., Ed.; Thieme: New York, NY, USA, 2012; pp. 19–21. [Google Scholar]
- Pollock, R.A. (Ed.) Pancraniomaxillofacial injury. In Craniomaxillofacial Buttresses: Anatomy and Operative Repair; Thieme: New York, NY, USA, 2012; pp. 194–207. [Google Scholar]
- Whitnall, S.E. Astonishing Anatomy; Isaac Pittman & Sons: London, UK, 1913. [Google Scholar]
- Skandalakis, J.E. The rape of anatomy. Am Surg 1980, 46, 197–200. [Google Scholar] [PubMed]
- Brander, B. A Touch of Medical Humor. Becker Briefs, Bernard Becker Medical Library, Washington University School of Medicine. 2016. Available online: https://becker.wustl.edu/about/news/touch-medicalhumor (accessed on 26 September 2017).










© 2019 by the author. The Author(s) 2019.
Share and Cite
Pollock, R.A.; Gossman, M.D. Anatomical Revelations in 1921 Kindled Operative Repair of the Orbit, Eyelids, and Periorbit over the Ensuing 100 Years: The Diuturnity of Ernest Whitnall (1876–1950) of Oxford, Montreal, and Bristol. Craniomaxillofac. Trauma Reconstr. 2019, 12, 95-107. https://doi.org/10.1055/s-0039-1677696
Pollock RA, Gossman MD. Anatomical Revelations in 1921 Kindled Operative Repair of the Orbit, Eyelids, and Periorbit over the Ensuing 100 Years: The Diuturnity of Ernest Whitnall (1876–1950) of Oxford, Montreal, and Bristol. Craniomaxillofacial Trauma & Reconstruction. 2019; 12(2):95-107. https://doi.org/10.1055/s-0039-1677696
Chicago/Turabian StylePollock, Richard A., and M. Douglas Gossman. 2019. "Anatomical Revelations in 1921 Kindled Operative Repair of the Orbit, Eyelids, and Periorbit over the Ensuing 100 Years: The Diuturnity of Ernest Whitnall (1876–1950) of Oxford, Montreal, and Bristol" Craniomaxillofacial Trauma & Reconstruction 12, no. 2: 95-107. https://doi.org/10.1055/s-0039-1677696
APA StylePollock, R. A., & Gossman, M. D. (2019). Anatomical Revelations in 1921 Kindled Operative Repair of the Orbit, Eyelids, and Periorbit over the Ensuing 100 Years: The Diuturnity of Ernest Whitnall (1876–1950) of Oxford, Montreal, and Bristol. Craniomaxillofacial Trauma & Reconstruction, 12(2), 95-107. https://doi.org/10.1055/s-0039-1677696