
Behavioral and Mental Responses towards the COVID-19 Pandemic among Chinese Older Adults: A Cross-Sectional Study

 ,
, 


Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
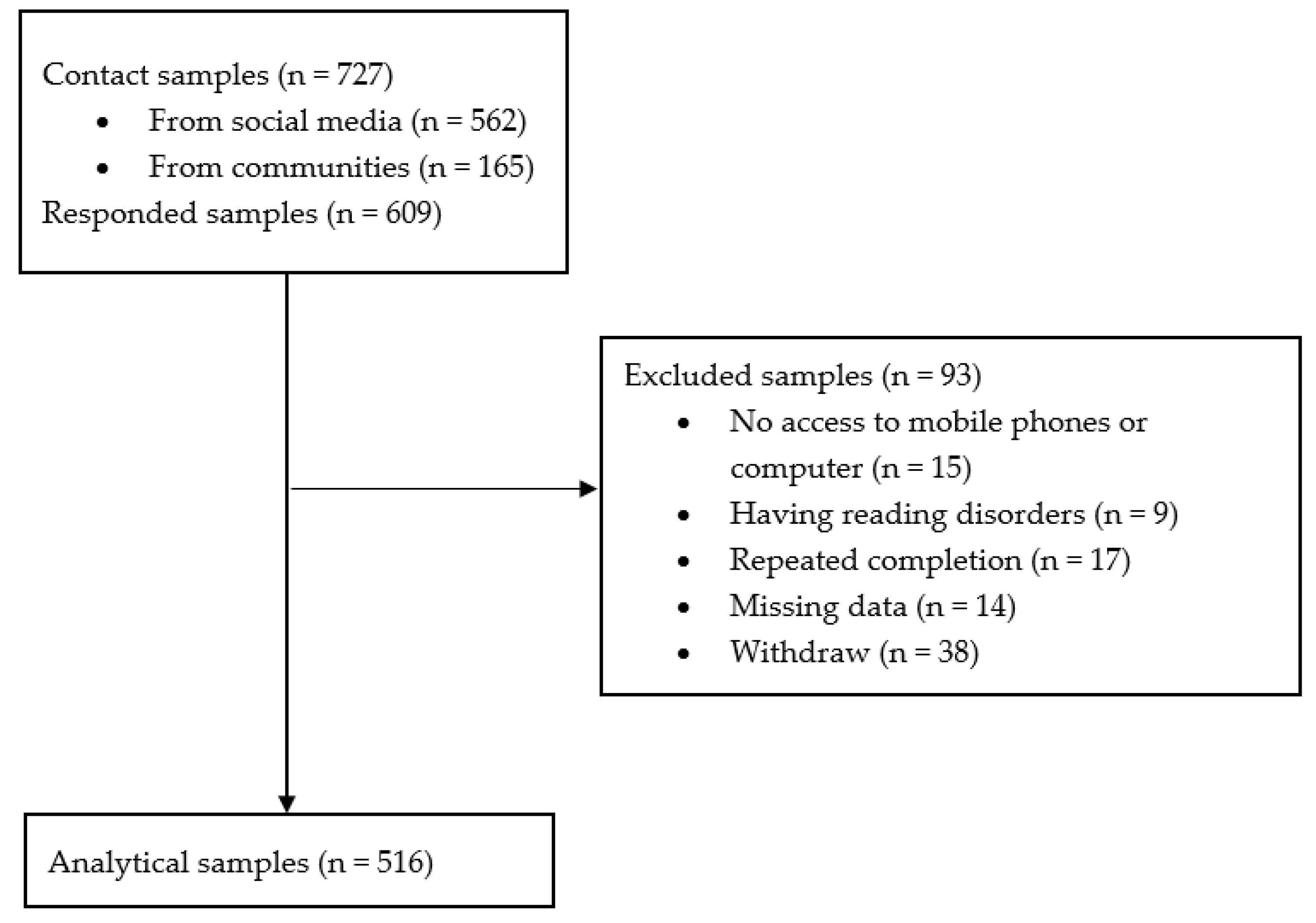
3.1. Study Design and Participants
3.2. Procedure
3.3. Measures
3.3.1. Behavioral Responses
- Preventive behaviors (PB): the adherence to the PB was measured by six items covering the three major PB as recommended by the WHO, including hand washing, facemask wearing, and physical distancing (WHO 2021b). Each behavior was assessed by two items. For example, the items for hand washing were asked with the stem of “during the previous week, I adhered to washing my hands with soap and water or alcohol-based hand rub (for at least 20 s, on all surfaces of the hands) …” followed by two situations including “(a) in a daily life situation, e.g., before eating, and (b) in a disease-related situation, e.g., after caring for the sick.” All responses were indicated on a 4-point Likert scale ranging from “1 = strongly disagree” to “4 = strongly agree” (Liang et al. 2021). Participants who indicated “agree/strongly agree” for all six items were coded as “1 = adhering to PB”, otherwise as “0 = non-adhering to PB”.
- Physical activity (PA) and fruit–vegetable consumption (FVC): each behavior response was measured by one item. Participants were asked about their changes in weekly amount of PA and daily portion of FVC since the outbreak of the COVID-19 pandemic. Responses included “0 = less” and “1 = same or more”.
3.3.2. Mental Responses
- Depression: the 10-item Chinese version of the Epidemiologic Studies Short Depression Scale (CESD-10) was used to measure the depressive symptoms (Rankin et al. 1993). The questions were asked with the stem: “In the past week, how often I feel...”, followed by 10 items such as “I was bothered by things that usually don’t bother me”. The responses were indicated on a 4-point Likert scale, ranging from “0 = rarely (less than 1 day)” to “3 = for most of the time (5–7 days)” (Cronbach’s alpha = 0.82) (Rankin et al. 1993; Liang et al. 2019). The total score of the 10 items was calculated, where the score of 0–9 was coded as “0 = no significant depressive symptoms”, and ≥10 was coded as “1 = significant depressive symptoms” (Andresen et al. 1994).
- Loneliness: the 6-item Chinese version of the De Jong Grieveld Loneliness Scale was used to measure loneliness (Leung et al. 2008). The scale consisted of two dimensions (social lonely and emotional lonely), with three items for each dimension. Participants were asked with the stem “Please see if the statements are describing your situations or feelings now…” followed by six items, such as “I experience a general sense of emptiness” (emotional) and “There are plenty of people I can rely on when I have problems” (social) (Cronbach’s alpha = 0.76) (Leung et al. 2008). The total score of the 6 items was calculated, where the score of 0–3 was coded as “0 = light loneliness” and ≥4 was coded as “1 = severe loneliness” (De Jong Gierveld and Theo Van Tilburg 1999).
3.3.3. Demographics
3.4. Statistical Analysis
4. Results
4.1. Characteristics of the Study Sample
4.2. Characteristics of Behavioral and Mental Responses
4.3. Associations of Demographic Correlates, Behavioral Responses, and Mental Responses
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | 1.000 | ||||||||||||
| 2. Gender | −0.035 | ||||||||||||
| 3. Living situation | −0.140 ** | −0.124 ** | |||||||||||
| 4. Marital status | 0.143 ** | 0.123 ** | −0.370 ** | ||||||||||
| 5. Education level | −0.150 ** | −0.139 ** | 0.064 | −0.175 ** | |||||||||
| 6. Occupation | 0.151 ** | 0.079 | −0.060 | 0.155 ** | −0.241 ** | ||||||||
| 7. Household Income | 0.011 | −0.022 | 0.115 ** | −0.133 ** | 0.295 ** | −0.153 ** | |||||||
| 8. Health status | −0.190 ** | 0.010 | 0.012 | −0.009 | 0.040 | −0.138 ** | 0.172 ** | ||||||
| 9. Medical condition | 0.170 ** | −0.046 | −0.022 | −0.003 | 0.052 | −0.030 | −0.063 | −0.418 ** | |||||
| 10. PB adherence | 0.023 | −0.037 | −0.170** | 0.069 | −0.174 ** | 0.032 | −0.136 ** | −0.049 | −0.012 | ||||
| 11. PA change | 0.076 | 0.037 | −0.027 | 0.054 | 0.029 | 0.025 | 0.021 | −0.104 * | 0.100 * | 0.043 | |||
| 12. FVC change | 0.110 * | −0.013 | −0.072 | 0.061 | −0.046 | 0.065 | −0.003 | −0.052 | 0.072 | 0.032 | 0.287 ** | ||
| 13. Depression | 0.038 | −0.018 | −0.090 * | 0.130 ** | −0.104 * | 0.049 | −0.151 ** | −0.212 ** | 0.103 * | 0.191 ** | 0.132 ** | 0.163 ** | |
| 14. Loneliness | −0.079 | 0.045 | 0.020 | −0.036 | −0.013 | −0.027 | 0.023 | 0.095 * | −0.049 | −0.024 | 0.117 ** | −0.033 | −0.015 |
References
- Amatriain-Fernández, Sandra, Eric Simón Murillo-Rodríguez, Thomas Gronwald, Sergio Machado, and Henning Budde. 2020. Benefits of physical activity and physical exercise in the time of pandemic. Psychological Trauma: Theory, Research, Practice, and Policy 12: S264. [Google Scholar] [CrossRef] [PubMed]
- Anderson, Eileen S., Richard A. Winett, and Janet R. Wojcik. 2007. Self-regulation, self-efficacy, outcome expectations, and social support: Social cognitive theory and nutrition behavior. Annals of Behavioral Medicine 34: 304–12. [Google Scholar] [CrossRef] [PubMed]
- Andresen, Elena M., Judith A. Malmgren, William B. Carter, and Donald L. Patrick. 1994. Screening for depression in well older adults: Evaluation of a short form of the CES-D. The American Journal of Preventive Medicine 10: 77–84. [Google Scholar] [CrossRef]
- Arora, Teresa, and Ian Grey. 2020. Health behaviour changes during COVID-19 and the potential consequences: A mini-review. Journal of Health Psychology 25: 1155–63. [Google Scholar] [CrossRef]
- Balkhi, Fizra, Aamna Nasir, Arhama Zehra, and Ramsha Riaz. 2020. Psychological and behavioral response to the coronavirus (COVID-19) pandemic. Cureus 12: e7923. [Google Scholar] [CrossRef]
- Caputo, Eduardo L., and Felipe F. Reichert. 2020. Studies of physical activity and COVID-19 during the pandemic: A scoping review. Journal of Physical Activity and Health 17: 1275–84. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Cindy, Joan Barceló, Allison Spencer Hartnett, Robert Kubinec, and Luca Messerschmidt. 2020. COVID-19 government response event dataset (CoronaNet v. 1.0). Nature Human Behaviour 4: 756–68. [Google Scholar] [CrossRef]
- Codagnone, Cristiano, Francesco Bogliacino, Camilo Gómez, Rafael Charris, Felipe Montealegre, Giovanni Liva, Francisco Lupiáñez-Villanueva, Frans Folkvord, and Giuseppe A. Veltri. 2020. Assessing concerns for the economic consequence of the COVID-19 response and mental health problems associated with economic vulnerability and negative economic shock in Italy, Spain, and the United Kingdom. PLoS ONE 15: e0240876. [Google Scholar] [CrossRef]
- Center for Systems Science and Engineering (CSSE) at Johns Hopkins University, USA. 2021. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 26 September 2021).
- Cunningham, Conor, Roger O’Sullivan, Paolo Caserotti, and Mark A. Tully. 2020. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. The Scandinavian Journal of Medicine & Science in Sports 30: 816–27. [Google Scholar] [CrossRef]
- De Jong Gierveld, Jenny, and Theo Van Tilburg. 1999. Manual of the loneliness scale 1999. Department of Social Research Methodology, Vrije Universiteit Amsterdam, Amsterdam (Updated Version 1801 02). Available online: https://home.fsw.vu.nl/TG.van.Tilburg/manual_loneliness_scale_1999.html (accessed on 26 September 2021).
- Duan, Yanping, Sonia Lippke, Wei Liang, Borui Shang, Wagner Petra, Julien Steven Baker, Jiali He, and Franziska Marie Keller. 2021. Association of social-cognitive factors with individual preventive behaviors of Covid-19 among a mixed-sample of older adults from China and Germany. Res-Square. Available online: https://www.researchsquare.com/article/rs-503762/v1 (accessed on 26 September 2021). [CrossRef]
- Dwyer, Michael John, Margherita Pasini, Stefano De Dominicis, and Elda Righi. 2020. Physical activity: Benefits and challenges during the COVID-19 pandemic. The Scandinavian Journal of Medicine & Science in Sports 30: 1291. [Google Scholar] [CrossRef]
- Gehlich, Kerstin H., Johannes Beller, Bernhard Lange-Asschenfeldt, Wolfgang Köcher, Martina C. Meinke, and Jürgen Lademann. 2019. Fruit and vegetable consumption is associated with improved mental and cognitive health in older adults from non-Western developing countries. Public Health Nutrition 22: 689–96. [Google Scholar] [CrossRef] [PubMed]
- Hu, Zhao, Xuhui Lin, Atipatsa Chiwanda Kaminga, and Huilan Xu. 2020. Impact of the COVID-19 epidemic on lifestyle behaviors and their association with subjective well-being among the general population in mainland China: Cross-sectional study. The Journal of Medical Internet Research 22: e21176. [Google Scholar] [CrossRef]
- Hu, Xinyi, Antoine Flahault, Alexander Temerev, and Liudmila Rozanova. 2021. The Progression of COVID-19 and the Government Response in China. International Journal of Environmental Research and Public Health 18: 3002. [Google Scholar] [CrossRef] [PubMed]
- Jin, Huajie, Haiyin Wang, Xiao Li, Weiwei Zheng, Shanke Ye, Sheng Zhang, Jiahui Zhou, and Mark Pennington. 2021. Economic burden of COVID-19, China, January–March, 2020: A cost-of-illness study. Bulletin of the World Health Organization 99: 112. [Google Scholar] [CrossRef]
- Khan, Kiran Shafiq, Mohammed A. Mamun, Mark D. Griffiths, and Irfan Ullah. 2020. The mental health impact of the COVID-19 pandemic across different cohorts. International Journal of Mental Health and Addiction 9: 1–7. [Google Scholar] [CrossRef]
- Kingsbury, Mila, Gabrielle Dupuis, Felice Jacka, Marie-Hélène Roy-Gagnon, Seanna E. McMartin, and Ian Colman. 2016. Associations between fruit and vegetable consumption and depressive symptoms: Evidence from a national Canadian longitudinal survey. Journal of Epidemiology and Community Health 70: 155–61. [Google Scholar] [CrossRef] [PubMed]
- Leung, Grace Tak Yu, Jenny de Jong Gierveld, and Linda Chiu Wa Lam. 2008. Validation of the Chinese translation of the 6-item De Jong Gierveld Loneliness Scale in elderly Chinese. International Psychogeriatrics 20: 1262–72. [Google Scholar] [CrossRef]
- Li, Xiaojing, and Qinliang Liu. 2020. Social media use, eHealth literacy, disease knowledge, and preventive behaviors in the COVID-19 pandemic: Cross-sectional study on Chinese netizens. Journal of Medical Internet Research 22: e19684. [Google Scholar] [CrossRef]
- Li, Siyue, Bo Feng, Wang Liao, and Wenjing Pan. 2020. Internet use, risk awareness, and demographic characteristics associated with engagement in preventive behaviors and testing: Cross-sectional survey on COVID-19 in the United States. The Journal of Medical Internet Research 22: e19782. [Google Scholar] [CrossRef] [PubMed]
- Liang, Wei, Yan Ping Duan, Bo Rui Shang, Yan Ping Wang, Chun Hu, and Sonia Lippke. 2019. A web-based lifestyle intervention program for Chinese college students: Study protocol and baseline characteristics of a randomized placebo-controlled trial. BMC Public Health 19: 1. [Google Scholar] [CrossRef] [Green Version]
- Liang, Wei, Yanping Duan, Borui Shang, Chun Hu, Julien Steven Baker, Zhihua Lin, Jiali He, and Yanping Wang. 2021. Precautionary behavior and depression in older adults during the COVID-19 pandemic: An online cross-sectional study in Hubei, China. International Journal of Environmental Research and Public Health 18: 1853. [Google Scholar] [CrossRef]
- Litton, Michelle M., and Alyssa W. Beavers. 2020. The Relationship between Food Security Status and Fruit and Vegetable Intake during the COVID-19 Pandemic. Nutrients 13: 712. [Google Scholar] [CrossRef] [PubMed]
- Liu, Hua-Xuan, Bik-Chu Chow, Wei Liang, Holger Hassel, and YaJun Wendy Huang. 2021. Measuring a broad spectrum of eHealth skills in the Web 3.0 context using an eHealth Literacy Scale: Development and validation study. The Journal of Medical Internet Research 23: e31627. [Google Scholar] [CrossRef]
- López-Bueno, Rubén, Guillermo F. López-Sánchez, José A. Casajús, Joaquín Calatayud, Alejandro Gil-Salmerón, Igor Grabovac, Mark A. Tully, and Lee Smith. 2020. Health-related behaviors among school-aged children and adolescents during the Spanish Covid-19 confinement. Frontiers in Pediatrics 8: 573. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission of China. 2021. Update on the New Coronavirus Cases. Available online: http://health.people.com.cn/GB/26466/431463/431576/index.html (accessed on 26 September 2021).
- Pels, Fabian, and Jens Kleinert. 2016. Loneliness and physical activity: A systematic review. International Review of Sport and Exercise Psychology 9: 231–60. [Google Scholar] [CrossRef]
- Pinquart, Martin. 2001. Correlates of subjective health in older adults: A meta-analysis. Psychology and Aging 16: 414. [Google Scholar] [CrossRef] [PubMed]
- Probst, Tahira M., Hyun Jung Lee, and Andrea Bazzoli. 2020. Economic stressors and the enactment of CDC-recommended COVID-19 prevention behaviors: The impact of state-level context. The Journal of Applied Psychology 105: 1397–407. [Google Scholar] [CrossRef]
- Puspitasari, Irma Melyani, Lutfiah Yusuf, Rano K. Sinuraya, Rizky Abdulah, and Hiroshi Koyama. 2020. Knowledge, attitude, and practice during the COVID-19 pandemic: A review. The Journal of Multidisciplinary Healthcare 13: 727. [Google Scholar] [CrossRef]
- Qin, Fei, Yiqing Song, George P. Nassis, Lina Zhao, Yanan Dong, Cuicui Zhao, Yiwei Feng, and Jiexiu Zhao. 2020. Physical activity, screen time, and emotional well-being during the 2019 novel coronavirus outbreak in China. International Journal of Environmental Research and Public Health 17: 5170. [Google Scholar] [CrossRef]
- Rankin, Sally H., Michael E. Galbraith, and Sharon Johnson. 1993. Reliability and validity data for a Chinese translation of the Center for Epidemiological Studies-Depression. Psychological Reports 73: 1291–98. [Google Scholar] [CrossRef]
- Schrack, Jennifer A., Amal A. Wanigatunga, and Stephen P. Juraschek. 2020. After the COVID-19 pandemic: The next wave of health challenges for older adults. The Journals of Gerontology 75: e121–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selya, Arielle S., Jennifer S. Rose, Lisa C. Dierker, Donald Hedeker, and Robin J. Mermelstein. 2012. A practical guide to calculating Cohen’s f2, a measure of local effect size, from PROC MIXED. Frontiers in Psychology 3: 111. [Google Scholar] [CrossRef] [Green Version]
- Shahid, Zainab, Ricci Kalayanamitra, Brendan McClafferty, Douglas Kepko, Devyani Ramgobin, Ravi Patel, Chander Shekher Aggarwal, Ramarao Vunnam, Nitasa Sahu, Dhirisha Bhatt, and et al. 2020. COVID-19 and older adults: What we know. Journal of the American Geriatrics Society 68: 926–29. [Google Scholar] [CrossRef] [Green Version]
- Shankar, Aparna, Anne McMunn, and Andrew Steptoe. 2010. Health-related behaviors in older adults: Relationships with socioeconomic status. The American Journal of Preventive Medicine 38: 39–46. [Google Scholar] [CrossRef]
- Singh, Jaspreet, and Jagandeep Singh. 2020. COVID-19 and its impact on society. Electronic Research Journal of Social Sciences and Humanities 2. Available online: https://ssrn.com/abstract=3567837 (accessed on 26 September 2021).
- Stickley, Andrew, Tetsuya Matsubayashi, Hajime Sueki, and Michiko Ueda. 2020. COVID-19 preventive behaviours among people with anxiety and depressive symptoms: Findings from Japan. Public Health 189: 91–3. [Google Scholar] [CrossRef]
- Usher, Kim, Debra Jackson, Joanne Durkin, Naomi Gyamfi, and Navjot Bhullar. 2020. Pandemic-related behaviours and psychological outcomes; A rapid literature review to explain COVID-19 behaviours. International Journal of Mental Health Nursing 29: 1018–34. [Google Scholar] [CrossRef]
- Vahia, Ipsit V., Dilip V. Jeste, and Charles F. Reynolds. 2020. Older adults and the mental health effects of COVID-19. JAMA 324: 2253–4. [Google Scholar] [CrossRef]
- Wang, Cuiyan, Riyu Pan, Xiaoyang Wan, Yilin Tan, Linkang Xu, Cyrus S. Ho, and Roger C. Ho. 2020. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health 17: 1729. [Google Scholar] [CrossRef] [Green Version]
- Wang, Cuiyan, Riyu Pan, Xiaoyang Wan, Yilin Tan, Linkang Xu, Roger S. McIntyre, Faith N. Choo, B. Tran, R. Ho, Vijay K. Sharma, and et al. 2020. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain, Behavior, and Immunity 87: 40–48. [Google Scholar] [CrossRef] [PubMed]
- Weaver, Raven H., Alexandra Jackson, Jane Lanigan, Thomas G. Power, Alana Anderson, Anne E. Cox, Linda Eddy, Louise Parker, Yoshie Sano, and Elizabeth Weybright. 2021. Health Behaviors at the Onset of the COVID-19 Pandemic. The American Journal of Health Behavior 45: 44–61. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. 2020. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 15 October 2020).
- WHO. 2021a. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 26 September 2021).
- WHO. 2021b. World Health Organization. Coronavirus Disease (COVID-19) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 30 August 2021).
- Wilczyńska, Dominika, Jianye Li, Yin Yang, Hongying Fan, Taofeng Liu, and Mariusz Lipowski. 2021. Fear of COVID-19 changes the motivation for physical activity participation: Polish-Chinese comparisons. Health Psychology Report 2: 138–48. Available online: https://czasopisma.bg.ug.edu.pl/index.php/HPR/article/view/5754 (accessed on 26 September 2021).
- Wu, Bei. 2020. Social isolation and loneliness among older adults in the context of COVID-19: A global challenge. Global Health Res and Policy 5: 1–3. [Google Scholar] [CrossRef] [PubMed]
- Yahia, Elhadi M., María Elena Maldonado Celis, and Mette Svendsen. 2017. The contribution of fruit and vegetable consumption to human health. In Fruit and vegetable Phytochemicals. Edited by E. M. Yahia. Hoboken: John Wiley & Sons, vol. 29, pp. 3–52. [Google Scholar]
- Yang, Yuan, Wen Li, Qinge Zhang, Ling Zhang, Teris Cheung, and Yu-Tao Xiang. 2020. Mental health services for older adults in China during the COVID-19 outbreak. The Lancet Psychiatry 7: e19. [Google Scholar] [CrossRef]
- Ye, Yisheng, Ruoxi Wang, Da Feng, Ruijun Wu, Zhifei Li, Chengxu Long, Zhanchun Feng, and Shangfeng Tang. 2020. The recommended and excessive preventive behaviors during the COVID-19 pandemic: A community-based online survey in China. International Journal of Environmental Research and Public Health 17: 6953. [Google Scholar] [CrossRef]

| PB | PA | FVC | Depression | Loneliness | |
|---|---|---|---|---|---|
| Non-Adherence: n (%) | Decreased: n (%) | Decreased: n (%) | Yes: n (%) | High: n (%) | |
| Total (n = 516) | |||||
| Age (n, %) | |||||
| 60–69 yrs. (354, 68.60%) | 36 (10.2%) | 125 (35.3%) | 23 (6.5%) * | 105 (29.7%) | 233 (65.8%) |
| 70–79 yrs. (128, 24.80%) | 128 (11.7%) | 52 (40.6%) | 13 (10.2%) * | 42 (32.8%) | 76 (59.4%) |
| ≥80 yrs. (34, 6.60%) | 34 (11.8%) | 17 (50.0%) | 7 (20.6%) * | 12 (35.3%) | 18 (52.9%) |
| Gender (n, %) | |||||
| Male (217, 42.10%) | 26 (12.0%) | 77 (35.5%) | 19 (8.8%) | 69 (31.8%) | 132 (60.8%) |
| Female (299, 57.90%) | 29 (9.7%) | 171 (39.1%) | 24 (8.0%) | 90 (30.1%) | 195 (65.2%) |
| Living situation (n, %) | |||||
| Alone (48, 9.30%) | 13 (27.1%) *** | 20 (41.7%) | 7 (14.6%) | 21 (43.80%) * | 29 (60.4%) |
| Not alone (468, 90.70%) | 42 (9.0%) *** | 174 (37.2%) | 36 (7.7%) | 138 (29.5%) * | 298 (73.7%) |
| Marital status (n, %) | |||||
| Single (14, 2.70%) | 3 (21.4%) * | 7 (50.0%) | 1 (7.1%) | 5 (35.7%) ** | 10 (71.4%) |
| Married (432, 83.70%) | 39 (9.0%) * | 154 (35.6%) | 33 (7.6%) | 120 (27.8%) ** | 275 (63.7%) |
| Divorced/widowed (70, 13.60%) | 13 (18.6%) * | 33 (41.7%) | 9 (12.9%) | 34 (48.6%) ** | 42 (60.0%) |
| Educational level (n, %) | |||||
| Primary school or below (45, 8.70%) | 12 (26.7%) *** | 18 (40.0%) | 5 (11.1%) | 21 (46.7%) * | 28 (62.2%) |
| Middle or High school (231, 44.80%) | 29 (12.6%) *** | 81 (35.1%) | 21 (9.1%) | 74 (32.0%) * | 149 (64.5%) |
| College or above (240, 46.50%) | 14 (5.8%) *** | 95 (39.6%) | 17 (7.1%) | 64 (26.7%) * | 150 (62.5%) |
| Occupational status (n, %) | |||||
| Employed (16, 3.10%) | 3 (18.8%) | 2 (12.5%) | 0 (0.00%)) | 4 (20.5%) | 11 (68.8%) |
| Pensioner or retired (478, 92.60%) | 47 (9.8%) | 186 (38.9%) | 40 (8.4%) | 146 (30.5%) | 303 (63.4%) |
| Unemployed (22, 4.30%) | 5 (9.10%) | 6 (27.3%) | 3 (13.6%) | 9 (40.9%) | 13 (59.1%) |
| Household income (n, %) | |||||
| Below average (113, 21.90%) | 21 (18.6%) ** | 43 (38.1%) | 10 (8.8%) | 48 (42.5%) ** | 69 (61.1%) |
| Average (299, 57.90%) | 28 (9.4%) ** | 108 (36.1%) | 24 (8.0%) | 89 (29.8%) ** | 191 (63.9%) |
| Above average (104, 20.20%) | 6 (5.8%) ** | 43 (41.3%) | 9 (8.7%) | 22 (21.2%) ** | 67 (64.4%) |
| Health status (n, %) | |||||
| Poor (48, 9.30%) | 6 (12.5%) | 21 (43.80%) | 5 (10.4%) | 28 (58.3%) *** | 25 (52.1%) |
| Satisfactory (196, 38.00%) | 24 (12.20%) | 84 (42.90%) | 19 (9.7%) | 69 (35.2%) *** | 119 (60.7%) |
| Excellent (272, 52.70%) | 25 (9.2%) | 89 (32.7%) | 19 (7.0%) | 62 (22.8%) *** | 183 (67.3%) |
| Medical condition (n, %) | |||||
| No (254, 49.20%) | 28 (11.0%) | 83 (32.7%) * | 16 (6.3%) | 66 (26.0%) * | 167 (65.7%) |
| Yes (262, 50.80%) | 27 (10.3%) | 111 (42.4%) * | 27 (10.3%) | 93 (35.5%) * | 160 (61.1%) |
| Variable | PB Non-Adherence | PA Decrease | FVC Decrease | |||
|---|---|---|---|---|---|---|
| OR | 95%CI | OR | 95%CI | OR | 95%CI | |
| Age group (60–69 yrs. as ref.) | ||||||
| 70–79 yrs. | 0.82 | (0.40, 1.71) | 1.08 | (0.69, 1.67) | 1.30 | (0.62, 2.75) |
| ≥80 yrs. | 0.74 | (0.22, 2.55) | 1.55 | (0.73, 3.31) | 2.85 * | (1.02, 7.95) |
| Gender (male as ref.) | ||||||
| Female | 0.58 | (0.31, 1.09) | 1.10 | (0.75, 1.63) | 0.84 | (0.43, 1.64) |
| Living situation (alone as ref.) | ||||||
| Not alone | 0.31 | (0.12, 0.79) | 1.19 | (0.58, 2.42) | 0.58 | (0.20, 1.68) |
| Marital status (single as ref.) | ||||||
| Married | 0.36 | (0.08, 1.64) | 0.56 | (0.18, 1.72) | 0.97 | (0.11, 8.34) |
| Divorced/widowed | 0.38 | (0.08, 1.96) | 0.91 | (0.27, 3.05) | 1.25 | (0.13, 11.68) |
| Educational level (primary school or below as ref.) | ||||||
| Middle or high school | 0.49 | (0.19, 1.26) | 0.84 | (0.39, 1.80) | 1.29 | (0.38, 4.39) |
| College or above | 0.20 ** | (0.07, 0.59) | 1.00 | (0.46, 2.19) | 0.98 | (0.27, 3.64) |
| Occupational status (employed as ref.) | ||||||
| Unemployed | 0.47 | (0.11, 2.08) | 3.62 | (0.79, 16.57) | N/A | N/A |
| Pensioner or retired | 0.45 | (0.07, 3.07) | 1.96 | (0.31, 12.53) | N/A | N/A |
| Household income (below above as ref.) | ||||||
| Average | 0.62 | (0.31, 1.24) | 0.99 | (0.61, 1.60) | 1.12 | (0.49, 2.58) |
| Above average | 0.43 | (0.15, 1.28) | 1.21 | (0.66, 2.24) | 1.25 | (0.43, 3.66) |
| Health status (poor as ref.) | ||||||
| Satisfactory | 1.40 | (0.47, 4.21) | 1.05 | (0.53, 2.06) | 1.21 | (0.40, 3.66) |
| Excellent | 0.89 | (0.28, 2.86) | 0.77 | (0.38, 1.56) | 1.09 | (0.34, 3.47) |
| Medical condition (no chronic diseases as ref.) | ||||||
| Yes | 0.80 | (0.41, 1.56) | 1.29 | (0.86, 1.94) | 1.56 | (0.76, 3.19) |
| Depression | Loneliness | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Model 1 | Model 2 | Model 1 | Model 2 | ||||
| OR | 95%CI | OR | 95%CI | OR | 95%CI | OR | 95%CI | |
| Age group (60–69 yrs. as ref.) | ||||||||
| 70–79 yrs. | 0.83 | (0.52, 1.35) | 0.82 | (0.50, 1.35) | 0.81 | (0.52, 1.26) | 0.81 | (0.52, 1.26) |
| ≥80 yrs. | 0.74 | (0.32, 1.75) | 0.64 | (0.26, 1.47) | 0.65 | (0.30, 1.38) | 0.63 | (0.29, 1.36) |
| Gender (male as ref.) | ||||||||
| Female | 0.79 | (0.52, 1.21) | 0.84 | (0.54, 1.29) | 1.18 | (0.80, 1.73) | 1.15 | (0.78, 1.70) |
| Living situation (alone as ref.) | ||||||||
| Not alone | 0.86 | (0.41, 1.80) | 1.07 | (0.49, 2.35) | 1.08 | (0.53, 2.20) | 1.00 | (0.48, 2.07) |
| Marital status (single as ref.) | ||||||||
| Married | 0.73 | (0.22, 2.51) | 0.87 | (0.24, 3.20) | 0.67 | (0.20, 2.27) | 0.72 | (0.21, 2.48) |
| Divorced/widowed | 1.68 | (0.45, 6.18) | 1.98 | (0.50, 7.89) | 0.60 | (0.17, 2.19) | 0.59 | (0.16, 2.21) |
| Educational level (primary school or below as ref.) | ||||||||
| Middle or high school | 0.70 | (0.32, 1.52) | 0.75 | (0.33, 1.69) | 0.91 | (0.43, 1.94) | 0.94 | (0.44, 2.00) |
| College or above | 0.55 | (0.25, 1.24) | 0.64 | (0.27, 1.50) | 0.81 | (0.37, 1.77) | 0.79 | (0.36, 1.73) |
| Occupational status (employed as ref.) | ||||||||
| Unemployed | 0.89 | (0.27, 2.97) | 0.84 | (0.24, 2.91) | 0.93 | (0.31, 2.81) | 0.82 | (0.27, 2.50) |
| Pensioner or retired | 0.65 | (0.13, 3.18) | 0.59 | (0.11, 3.06) | 0.85 | (0.20, 3.69) | 0.84 | (0.19, 3.70) |
| Household income (below above as ref.) | ||||||||
| Average | 0.81 | (0.50, 1.33) | 0.83 | (0.50, 1.39) | 1.03 | (0.64, 1.65) | 1.02 | (0.63, 1.66) |
| Above average | 0.58 | (0.30, 1.14) | 0.59 | (0.29, 1.17) | 1.10 | (0.60, 2.20) | 1.07 | (0.58, 1.97) |
| Health status (poor as ref.) | ||||||||
| Satisfactory | 0.42 * | (0.21, 0.84) | 0.37 ** | (0.18, 0.76) | 1.33 | (0.68, 2.60) | 1.35 | (0.69, 2.66) |
| Excellent | 0.23 *** | (0.11, 0.48) | 0.21 *** | (0.10, 0.46) | 1.71 | (0.85, 3.44) | 1.81 | (0.89, 3.69) |
| Medical condition (no chronic diseases as ref.) | ||||||||
| Yes | 1.10 | (0.70, 1.72) | 1.04 | (0.65, 1.64) | 1.00 | (0.66, 1.50) | 0.97 | (0.64, 1.47) |
| PA (same and more as ref.) | ||||||||
| Decrease | N/A | N/A | 1.39 | (0.90, 2.15) | N/A | N/A | 2.01 ** | (1.32, 3.05) |
| FVC (same and more as ref.) | ||||||||
| Decrease | N/A | N/A | 2.77 ** | (1.35, 5.69) | N/A | N/A | 0.62 | (0.31, 1.23) |
| PB (adherence as ref.) | ||||||||
| Non-adherence | N/A | N/A | 2.84 ** | (1.51, 5.33) | N/A | N/A | 0.82 | (0.45, 1.52) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, W.; Duan, Y.; Yang, M.; Shang, B.; Hu, C.; Wang, Y.; Baker, J.S. Behavioral and Mental Responses towards the COVID-19 Pandemic among Chinese Older Adults: A Cross-Sectional Study. J. Risk Financial Manag. 2021, 14, 568. https://doi.org/10.3390/jrfm14120568
Liang W, Duan Y, Yang M, Shang B, Hu C, Wang Y, Baker JS. Behavioral and Mental Responses towards the COVID-19 Pandemic among Chinese Older Adults: A Cross-Sectional Study. Journal of Risk and Financial Management. 2021; 14(12):568. https://doi.org/10.3390/jrfm14120568
Chicago/Turabian StyleLiang, Wei, Yanping Duan, Min Yang, Borui Shang, Chun Hu, Yanping Wang, and Julien Steven Baker. 2021. "Behavioral and Mental Responses towards the COVID-19 Pandemic among Chinese Older Adults: A Cross-Sectional Study" Journal of Risk and Financial Management 14, no. 12: 568. https://doi.org/10.3390/jrfm14120568
APA StyleLiang, W., Duan, Y., Yang, M., Shang, B., Hu, C., Wang, Y., & Baker, J. S. (2021). Behavioral and Mental Responses towards the COVID-19 Pandemic among Chinese Older Adults: A Cross-Sectional Study. Journal of Risk and Financial Management, 14(12), 568. https://doi.org/10.3390/jrfm14120568