
Factor V Leiden (R506Q), Prothrombin G20210A, and MTHFR C677T Variants and Thrombophilia in Qatar Biobank Participants: A Case Control Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approvals and Study Participants
2.2. Definition of Thrombosis
2.3. Genotyping Techniques
2.4. Statistical Analysis
3. Results
3.1. Cohort Characteristics
3.2. Distribution of FV Leiden Variant
3.3. Distribution of the MTHFR Variant
3.4. Distribution of the F2 (Prothrombin) Variant
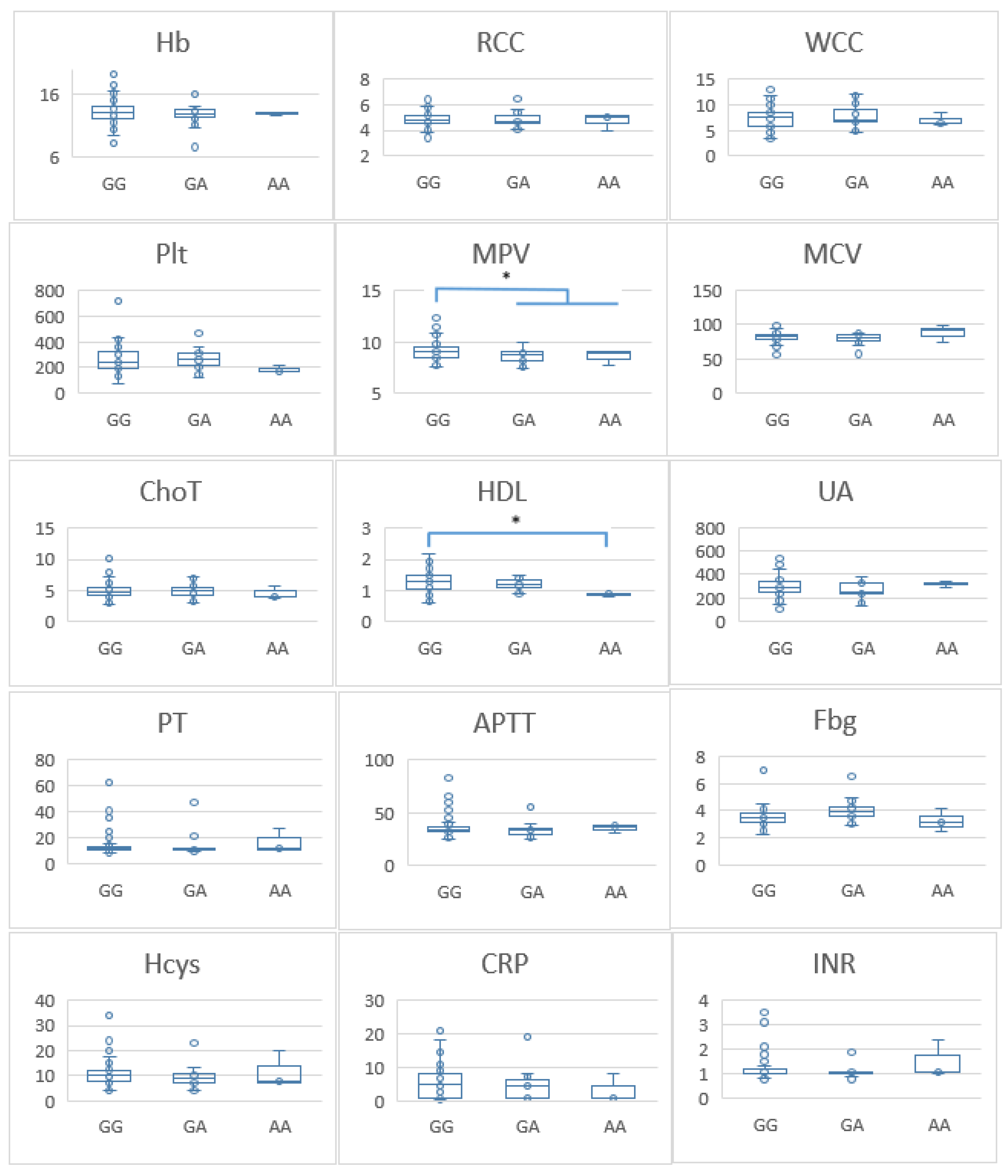
3.5. FV Leiden Variant and Laboratory Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yamashita, A.; Asada, Y. Underlying Mechanisms of Thrombus Formation/Growth in Atherothrombosis and Deep Vein Thrombosis. Pathol. Int. 2023, 73, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Alkarithi, G.; Duval, C.; Shi, Y.; Macrae, F.L.; Ariëns, R.A.S. Thrombus Structural Composition in Cardiovascular Disease. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 2370–2383. [Google Scholar] [CrossRef] [PubMed]
- Lowe, G.D.O. Venous and Arterial Thrombosis: Epidemiology and Risk Factors at Various Ages. Maturitas 2004, 47, 259–263. [Google Scholar] [CrossRef]
- Wendelboe, A.M.; Raskob, G.E. Global Burden of Thrombosis: Epidemiologic Aspects. Circ. Res. 2016, 118, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and Regional Mortality from 235 Causes of Death for 20 Age Groups in 1990 and 2010: A Systematic Analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef] [PubMed]
- Wendelboe, A.M.; McCumber, M.; Hylek, E.M.; Buller, H.; Weitz, J.I.; Raskob, G.; Angchaisuksiri, P.; Blanco, A.N.; Hunt, B.J.; Kakkar, A.; et al. Global Public Awareness of Venous Thromboembolism. J. Thromb. Haemost. 2015, 13, 1365–1371. [Google Scholar] [CrossRef]
- Elkhadir, A.M.; Wazzan, M.A.; Abduljabbar, A.H.; Badwi, N.M.; Hendi, F.M.; Al-Shomrani, K.M.; Al-Malawi, A.A. Prevalence of Deep Venous Thrombosis (DVT) in Jeddah. Int. J. Med. Sci. Clin. Invent. 2018, 5, 4089–4091. [Google Scholar] [CrossRef]
- Eldomiaty, M.; Alanazi, S.; Alhejaili, R.; Fallatah, R. Prevalence, Risk Factors, and Therapeutic Strategies of DVT Cases in Al-Madinah Province. IJMDC 2022, 6, 52–57. [Google Scholar] [CrossRef]
- Ambra, N.; Mohammad, O.H.; Naushad, V.A.; Purayil, N.K.; Mohamedali, M.G.; Elzouki, A.N.; Khalid, M.K.; Illahi, M.N.; Palol, A.; Barman, M.; et al. Venous Thromboembolism among Hospitalized Patients: Incidence and Adequacy of Thromboprophylaxis—A Retrospective Study. VHRM 2022, 18, 575–587. [Google Scholar] [CrossRef]
- Abdelwahab, R.; Hamad, A.; Negm, R.; Tarawneh, N.A.; Elazzazy, S. Assessment of Deep Vein Thrombosis (DVT) Incidence among Ambulatory Cancer Patients in Qatar: A Retrospective Cohort Study. GSC Biol. Pharm. Sci. 2021, 16, 049–058. [Google Scholar] [CrossRef]
- Minet, C.; Potton, L.; Bonadona, A.; Hamidfar-Roy, R.; Somohano, C.A.; Lugosi, M.; Cartier, J.-C.; Ferretti, G.; Schwebel, C.; Timsit, J.-F. Venous Thromboembolism in the ICU: Main Characteristics, Diagnosis and Thromboprophylaxis. Crit. Care 2015, 19, 287. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.Y.; Habas, E.; Sulaiman, T.O.; Hamid, O.A.; Abdalhadi, A.; Khalaf, A.; Afana, M.S.; Ali, M.Y.; Baniamer, Y.Z.; Kanjo, W.; et al. Risk Factors, Clinical Presentation, Diagnosis, and Treatment Outcomes of Portal Vein Thrombosis: A Five-Year Hospital-Based Study From Qatar. J. Clin. Med. Res. 2022, 14, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Pastori, D.; Cormaci, V.M.; Marucci, S.; Franchino, G.; Del Sole, F.; Capozza, A.; Fallarino, A.; Corso, C.; Valeriani, E.; Menichelli, D.; et al. A Comprehensive Review of Risk Factors for Venous Thromboembolism: From Epidemiology to Pathophysiology. Int. J. Mol. Sci. 2023, 24, 3169. [Google Scholar] [CrossRef] [PubMed]
- Cushman, M. Epidemiology and Risk Factors for Venous Thrombosis. Semin. Hematol. 2007, 44, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Hotoleanu, C. Association between Obesity and Venous Thromboembolism. Med. Pharm. Rep. 2020, 93, 162–168. [Google Scholar] [CrossRef]
- Yuan, S.; Bruzelius, M.; Håkansson, N.; Åkesson, A.; Larsson, S.C. Lifestyle Factors and Venous Thromboembolism in Two Cohort Studies. Thromb. Res. 2021, 202, 119–124. [Google Scholar] [CrossRef]
- Goldhaber, S.Z. Race and Venous Thromboembolism: Nature or Nurture? Circulation 2014, 129, 1463–1465. [Google Scholar] [CrossRef]
- Zöller, B.; Ohlsson, H.; Sundquist, J.; Sundquist, K. A Sibling Based Design to Quantify Genetic and Shared Environmental Effects of Venous Thromboembolism in Sweden. Thromb. Res. 2017, 149, 82–87. [Google Scholar] [CrossRef]
- Souto, J.C.; Almasy, L.; Borrell, M.; Blanco-Vaca, F.; Mateo, J.; Soria, J.M.; Coll, I.; Felices, R.; Stone, W.; Fontcuberta, J.; et al. Genetic Susceptibility to Thrombosis and Its Relationship to Physiological Risk Factors: The GAIT Study. Genetic Analysis of Idiopathic Thrombophilia. Am. J. Hum. Genet. 2000, 67, 1452–1459. [Google Scholar] [CrossRef]
- Fautrad, P.; Thomas, G.M.; Morange, P.E. The Missing Heritability of Venous Thrombosis: What about Factor V Leiden Heterogeneity? J. Thromb. Haemost. 2018, 16, 2125–2127. [Google Scholar] [CrossRef]
- De Stefano, V.; Chiusolo, P.; Paciaroni, K.; Leone, G. Epidemiology of Factor V Leiden: Clinical Implications. Semin. Thromb. Hemost. 1998, 24, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Poort, S.R.; Rosendaal, F.R.; Reitsma, P.H.; Bertina, R.M. A Common Genetic Variation in the 3′-Untranslated Region of the Prothrombin Gene Is Associated with Elevated Plasma Prothrombin Levels and an Increase in Venous Thrombosis. Blood 1996, 88, 3698–3703. [Google Scholar] [CrossRef] [PubMed]
- Bafunno, V.; Margaglione, M. Genetic Basis of Thrombosis. Clin. Chem. Lab. Med. 2010, 48 (Suppl. S1), S41–S51. [Google Scholar] [CrossRef] [PubMed]
- Eppenberger, D.; Nilius, H.; Anagnostelis, B.; Huber, C.A.; Nagler, M. Current Knowledge on Factor V Leiden Mutation as a Risk Factor for Recurrent Venous Thromboembolism: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 883986. [Google Scholar] [CrossRef]
- Brugge, J.M.; Simioni, P.; Bernardi, F.; Tormene, D.; Lunghi, B.; Tans, G.; Pagnan, A.; Rosing, J.; Castoldi, E. Expression of the Normal Factor V Allele Modulates the APC Resistance Phenotype in Heterozygous Carriers of the Factor V Leiden Mutation. J. Thromb. Haemost. 2005, 3, 2695–2702. [Google Scholar] [CrossRef]
- Jarjour, R.A.; Ammar, S.; Majdalawi, R. Frequency of Three Prothrombotic Polymorphisms among Syrian Population: Factor V G1691A, Prothrombin G20210A and Methylenetetrahydrofolate Reductase C677T. Ann. Hum. Biol. 2017, 44, 70–73. [Google Scholar] [CrossRef]
- Middeldorp, S. Inherited Thrombophilia: A Double-Edged Sword. Hematol. Am. Soc. Hematol. Educ. Program 2016, 2016, 1–9. [Google Scholar] [CrossRef]
- Lim, M.Y.; Moll, S. Thrombophilia. Vasc. Med. 2015, 20, 193–196. [Google Scholar] [CrossRef]
- Magavern, E.F.; Smedley, D.; Caulfield, M.J. Factor V Leiden, Estrogen, and Multimorbidity Association with Venous Thromboembolism in a British-South Asian Cohort. iScience 2023, 26, 107795. [Google Scholar] [CrossRef]
- Eslami, M.M.; Khalili, M.; Soufizomorrod, M.; Abroun, S.; Razi, B. Factor V Leiden 1691G > A Mutation and the Risk of Recurrent Pregnancy Loss (RPL): Systematic Review and Meta-Analysis. Thromb. J. 2020, 18, 11. [Google Scholar] [CrossRef]
- Tsalta-Mladenov, M.; Levkova, M.; Andonova, S. Factor V Leiden, Factor II, Protein C, Protein S, and Antithrombin and Ischemic Strokes in Young Adults: A Meta-Analysis. Genes 2022, 13, 2081. [Google Scholar] [CrossRef] [PubMed]
- Kujovich, J.L. Factor V Leiden Thrombophilia. Genet. Med. 2011, 13, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Asmis, L.; Hellstern, P. Thrombophilia Testing—A Systematic Review. Clin. Lab. 2023, 69, 670–691. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Taylor, A.K.; Lozano, R.; Grody, W.W.; Griffin, J.H.; ACMG Professional Practice and Guidelines Committee. Addendum: American College of Medical Genetics Consensus Statement on Factor V Leiden Mutation Testing. Genet. Med. 2021, 23, 2463. [Google Scholar] [CrossRef]
- Perez Botero, J.; Majerus, J.A.; Strege, A.K.; Johnson, R.D.; Chen, D.; Pruthi, R.K. Diagnostic Testing Approaches for Activated Protein C Resistance and Factor V Leiden: A Comparison of Institutional and National Provider Practices. Am. J. Clin. Pathol. 2017, 147, 604–610. [Google Scholar] [CrossRef]
- Favaloro, E.J.; McDonald, D. Futility of Testing for Factor V Leiden. Blood Transfus. 2012, 10, 260. [Google Scholar] [CrossRef]
- Li, J.; Liang, Y. Associations Between Mean Platelet Volume and Risk of Deep Vein Thrombosis: A Mendelian Randomization Study and a Retrospective Study. Int. J. Gen. Med. 2023, 16, 515–524. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Ayvazyan, L.; Mikhailidis, D.P.; Kitas, G.D. Mean Platelet Volume: A Link between Thrombosis and Inflammation? Curr. Pharm. Des. 2011, 17, 47–58. [Google Scholar] [CrossRef]
- Liew, S.-C.; Gupta, E.D. Methylenetetrahydrofolate Reductase (MTHFR) C677T Polymorphism: Epidemiology, Metabolism and the Associated Diseases. Eur. J. Med. Genet. 2015, 58, 1–10. [Google Scholar] [CrossRef]
- Raina, J.K.; Panjaliya, R.K.; Dogra, V.; Sharma, S.; Anupriya; Kumar, P. Association of MTHFR and MS/MTR Gene Polymorphisms with Congenital Heart Defects in North Indian Population (Jammu and Kashmir): A Case-Control Study Encompassing Meta-Analysis and Trial Sequential Analysis. BMC Pediatr. 2022, 22, 223. [Google Scholar] [CrossRef]
- El Alami, H.; Ouenzar, F.; Errafii, K.; Alidrissi, N.; Belyamani, L.; Ghazal, H.; Wakrim, L.; Abidi, O.; Naamane, A.; Daoud, R.; et al. Meta-Analysis of MTHFR C677T Polymorphism and Type 2 Diabetes Mellitus in MENA Region. Diabetes Metab. Syndr. 2024, 18, 102965. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.-J.; Li, J.-C.; Yin, Y.-W.; Li, B.-H.; Liu, Y.; Liao, S.-Q.; Gao, C.-Y.; Zhang, L.-L. Association of MTHFR C677T Polymorphism and Risk of Cerebrovascular Disease in Chinese Population: An Updated Meta-Analysis. J. Neurol. 2014, 261, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Gohil, R.; Peck, G.; Sharma, P. The Genetics of Venous Thromboembolism. A Meta-Analysis Involving Approximately 120,000 Cases and 180,000 Controls. Thromb. Haemost. 2009, 102, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Ames, P.R.; D’Andrea, G.; Arcaro, A.; Marottoli, V.; Iannaccone, L.; Margaglione, M.; Gentile, F. Homozygous MTHFR C677T Carriers Develop Idiopathic Portal Vein Thrombosis 20 Years Earlier than Wild Type. Blood Coagul. Fibrinolysis 2024, 35, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Ekim, M.; Ekim, H.; Yılmaz, Y.K. The Prevalence of Factor V Leiden, Prothrombin G20210A, MTHFR C677T and MTHFR A1298C Mutations in Healthy Turkish Population. Hippokratia 2015, 19, 309–313. [Google Scholar]
- Rady, P.L.; Tyring, S.K.; Hudnall, S.D.; Vargas, T.; Kellner, L.H.; Nitowsky, H.; Matalon, R.K. Methylenetetrahydrofolate Reductase (MTHFR): The Incidence of Mutations C677T and A1298C in the Ashkenazi Jewish Population. Am. J. Med. Genet. 1999, 86, 380–384. [Google Scholar] [CrossRef]
- Shibeeb, S.; Abdallah, A.; Shi, Z. Blood Homocysteine Levels Mediate the Association Between Blood Lead Levels and Cardiovascular Mortality. Cardiovasc. Toxicol. 2024, 24, 62–70. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | Total (n = 408) * | Cases (n = 104) * | Controls (n = 304) * | p-Value † |
|---|---|---|---|---|
| Sex | ||||
| Male (n%) | 201 (49.3%) | 34 (32.7%) | 167 (54.9%) | <0.0001 |
| Female (n%) | 207 (50.7%) | 70 (67.3%) | 137 (45.1%) | |
| Age (years) | 36.6 ± 11.9 | 46.6 ± 12.6 | 33.2 ± 9.5 | <0.0001 |
| Hb (g/dL) | 13.7 ± 1.8 | 13.1 ± 1.8 | 13.8 ± 1.8 | 0.007 |
| RCC (×106/µL) | 4.98 ± 0.56 | 4.90 ± 0.63 | 5.00 ± 0.56 | 0.13 |
| WCC (×103/µL) | 6.71 ± 1.95 | 7.47 ± 2.18 | 6.49 ± 1.71 | <0.0001 |
| PLT (×103/µL) | 248 ± 69 | 257 ± 93 | 246 ± 61 | 0.17 |
| MPV (Fl) | 9.05 ± 0.94 | 9.02 ± 0.87 | 9.05 ± 0.96 | 0.8 |
| MCV (fl) | 81.6 ± 7.06 | 81.6 ± 7.9 | 81.8 ± 6.74 | 0.8 |
| Total cholesterol (mmol/L) | 4.92 ± 1.0 | 4.9 ± 1.17 | 4.9 ± 0.94 | 1 |
| HDL (mmol/L) | 1.27 ± 0.35 | 1.29 ± 0.35 | 1.26 ± 0.34 | 0.4 |
| Uric acid (µmol/L) | 300.7 ± 81.3 | 289.3 ± 77 | 304.6 ± 82.4 | 0.01 |
| PT (s) | 12.8 ± 4.2 | 14.7 ± 8.3 | 12.1 ± 1.1 | <0.0001 |
| INR | 1.1 ± 0.39 | 1.22 ± 0.51 | 1.04 ± 0.095 | <0.0001 |
| APTT (s) | 33.9 ± 5.7 | 35.8 ± 9.1 | 33.9 ± 4.1 | 0.004 |
| Fib (g/L) | 3.27 ± 0.68 | 3.61 ± 0.72 | 3.15 ± 0.63 | <0.0001 |
| Homocysteine (µmol/L) | 9.7 ± 3.12 | 10.47.3 ± 4.52 | 9.45 ± 2.76 | 0.007 |
| CRP (mg/L) | 3.6 ± 4.9 | 5.3 ± 5.2 | 2.9 ± 4.65 | <0.0001 |
| FV G1691A (rs6025) | Control (N = 304) | Cases (N = 104) | X2 | p-Value | OR (95%CI) | ||
|---|---|---|---|---|---|---|---|
| Count | Frequency | Count | Frequency | ||||
| GG | 285 | 0.937 | 84 | 0.81 | 15.9 | 0.0004 | |
| GA | 18 | 0.06 | 17 | 0.16 | |||
| AA | 1 | 0.003 | 3 | 0.03 | |||
| G | 588 | 0.97 | 185 | 0.89 | 16.5 | 0.0001 | 3.6 (1.9–6.8) |
| A | 20 | 0.03 | 23 | 0.11 | |||
| GG + GA | 303 | 0.997 | 101 | 0.97 | 5.5 | 0.053 | |
| AA | 1 | 0.003 | 3 | 0.03 | |||
| GA + AA | 19 | 0.063 | 20 | 0.19 | 14.3 | 0.0002 | 3.6 (1.8–7.0) |
| GG | 285 | 0.937 | 84 | 0.81 | |||
| MTHFR C677T (rs1801133) | Control (N = 304) | Cases (N = 104) | ||||
|---|---|---|---|---|---|---|
| Count | Frequency | Count | Frequency | X2 | p-Value | |
| CC | 195 | 0.64 | 63 | 0.61 | 2.97 | 0.23 |
| CT | 100 | 0.33 | 34 | 0.33 | ||
| TT | 9 | 0.03 | 7 | 0.07 | ||
| C | 490 | 0.81 | 160 | 0.77 | 1.07 | 0.3 |
| T | 118 | 0.19 | 48 | 0.23 | ||
| CC + CT | 295 | 0.97 | 97 | 0.93 | 2.01 | 0.15 |
| TT | 9 | 0.03 | 7 | 0.07 | ||
| CT + TT | 109 | 0.36 | 41 | 0.39 | 0.28 | 0.59 |
| CC | 195 | 0.64 | 63 | 0.61 | ||
| F2 (Prothrombin) G20210A (rs1799963) | Control (N = 318) | Cases (N = 104) | ||
|---|---|---|---|---|
| Count | Frequency | Count | Frequency | |
| GG | 300 | 0.99 | 104 | 1 |
| GA | 4 | 0.01 | 0 | 0 |
| AA | 0 | 0 | 0 | 0 |
| G | 604 | 0.99 | 208 | 1 |
| A | 4 | 0.01 | 0 | 0 |
| GG + GA | 304 | 1 | 104 | 1 |
| AA | 0 | 0 | 0 | 0 |
| GA + AA | 4 | 0.01 | 0 | 0 |
| GG | 300 | 0.99 | 104 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shibeeb, S.; Al-Rayashi, N.; Shams, N.; Hadvan, T.; Agbani, E.O.; Abdallah, A.M. Factor V Leiden (R506Q), Prothrombin G20210A, and MTHFR C677T Variants and Thrombophilia in Qatar Biobank Participants: A Case Control Study. Pathophysiology 2024, 31, 608-620. https://doi.org/10.3390/pathophysiology31040044
Shibeeb S, Al-Rayashi N, Shams N, Hadvan T, Agbani EO, Abdallah AM. Factor V Leiden (R506Q), Prothrombin G20210A, and MTHFR C677T Variants and Thrombophilia in Qatar Biobank Participants: A Case Control Study. Pathophysiology. 2024; 31(4):608-620. https://doi.org/10.3390/pathophysiology31040044
Chicago/Turabian StyleShibeeb, Sapha, Nada Al-Rayashi, Nehal Shams, Tameem Hadvan, Ejaife O. Agbani, and Atiyeh M. Abdallah. 2024. "Factor V Leiden (R506Q), Prothrombin G20210A, and MTHFR C677T Variants and Thrombophilia in Qatar Biobank Participants: A Case Control Study" Pathophysiology 31, no. 4: 608-620. https://doi.org/10.3390/pathophysiology31040044
APA StyleShibeeb, S., Al-Rayashi, N., Shams, N., Hadvan, T., Agbani, E. O., & Abdallah, A. M. (2024). Factor V Leiden (R506Q), Prothrombin G20210A, and MTHFR C677T Variants and Thrombophilia in Qatar Biobank Participants: A Case Control Study. Pathophysiology, 31(4), 608-620. https://doi.org/10.3390/pathophysiology31040044