
Development, Validity, and Reliability of the Perceived Telemedicine Importance, Disadvantages, and Barriers (PTIDB) Questionnaire for Egyptian Healthcare Professionals

 ,
,  ,
,
Abstract
1. Introduction
Purpose
2. Development and Pre-Testing of the PTIDB Questionnaire
2.1. Phase-I: Development of the Questionnaire
2.2. Phase-2: Preliminary Testing of the Questionnaire (Cognitive Interview)
2.3. Phase-3: Investigating the Validity and Reliability of the Questionnaire Using a Large Survey
3. Materials and Methods
3.1. Design and Setting
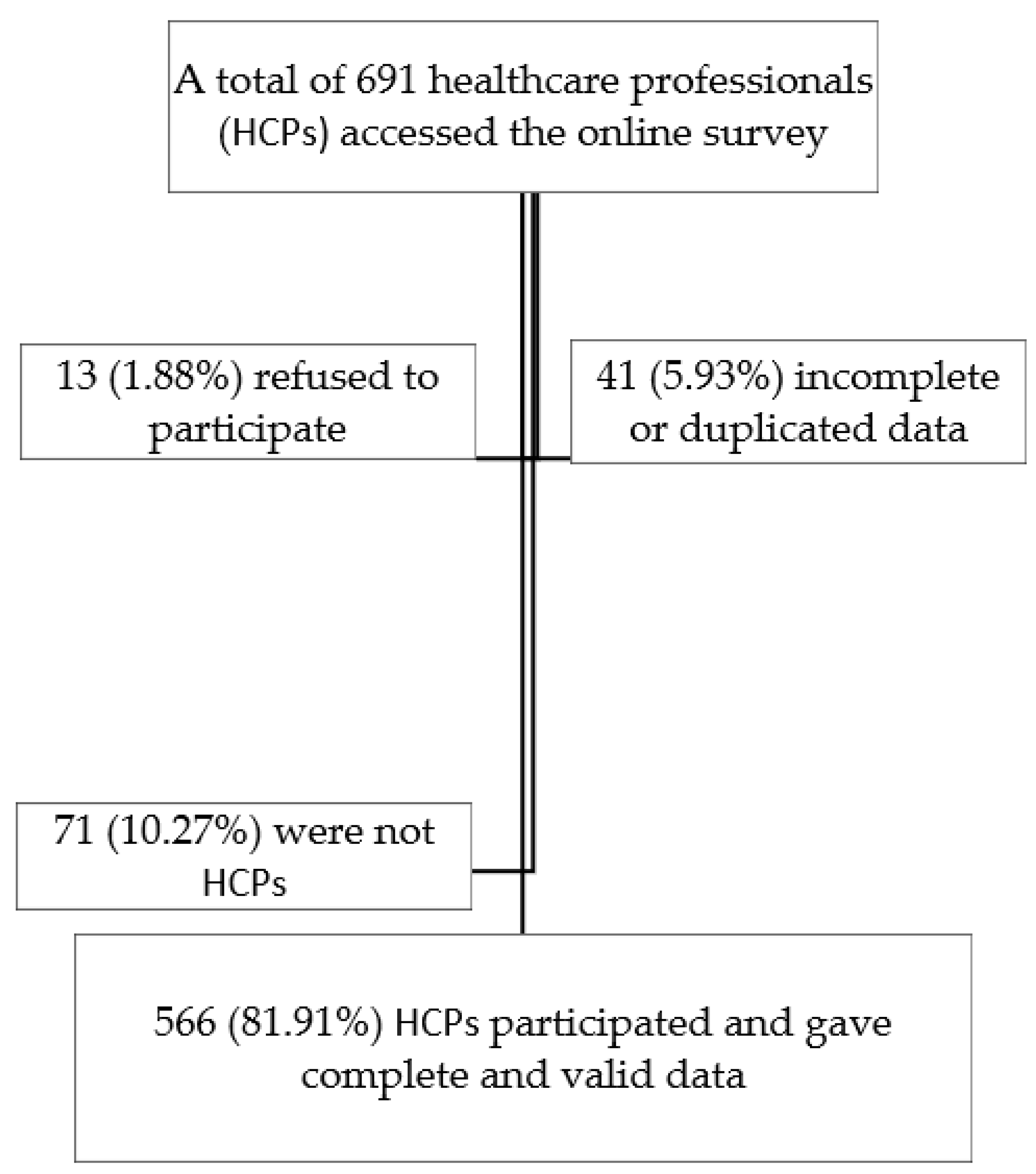
3.2. Population, Criteria, and Sample Size
3.3. Instruments
3.4. Statistical Analysis
3.5. Ethical Considerations
4. Results
4.1. Participants’ Sociodemographic Characteristics
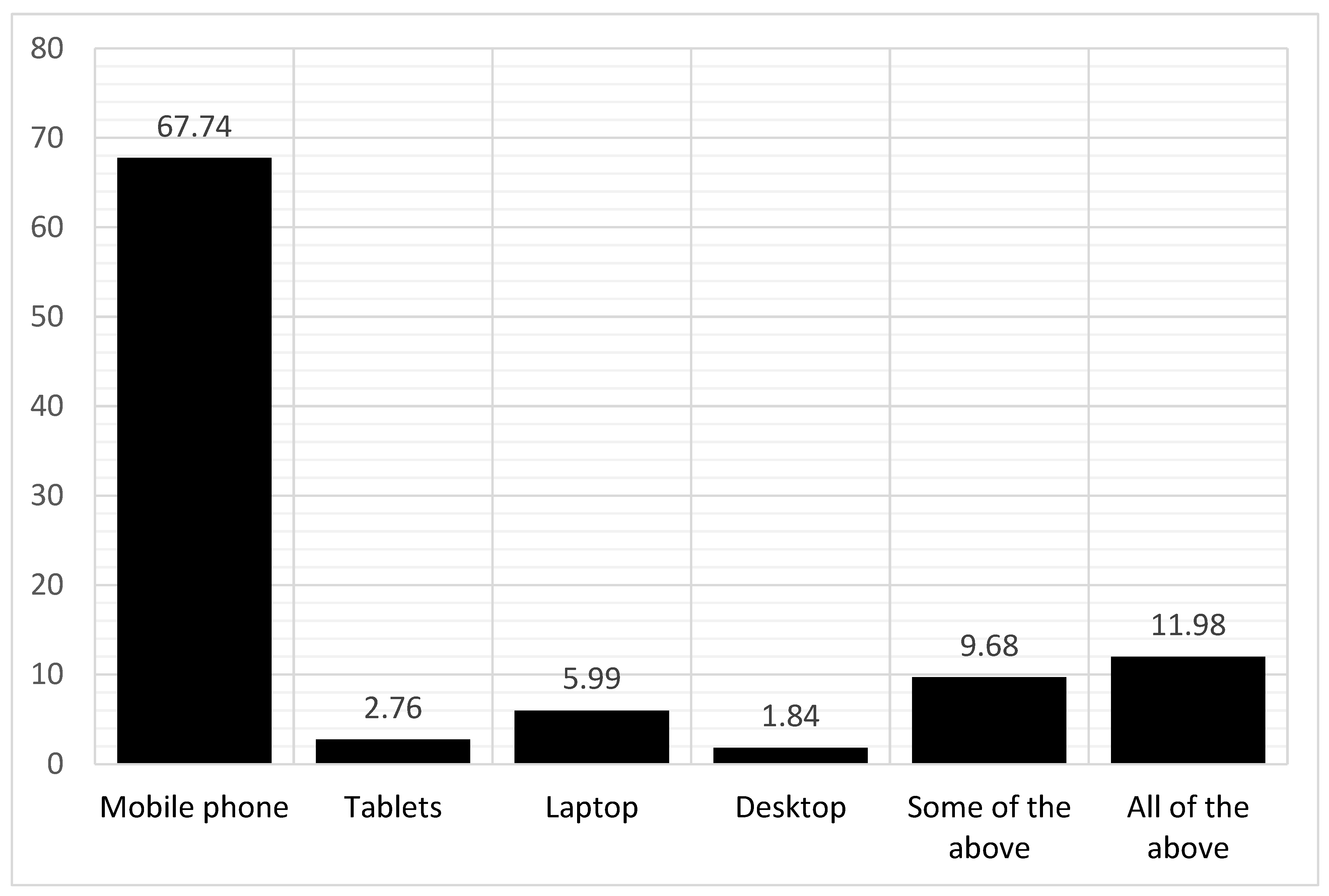
4.2. Utilization of Telemedicine among the Study Participants
4.3. Association between Sociodemographic Variables and Using Telemedicine
4.4. Exploratory Factor Analysis (EFA)
4.5. Divergent Validity
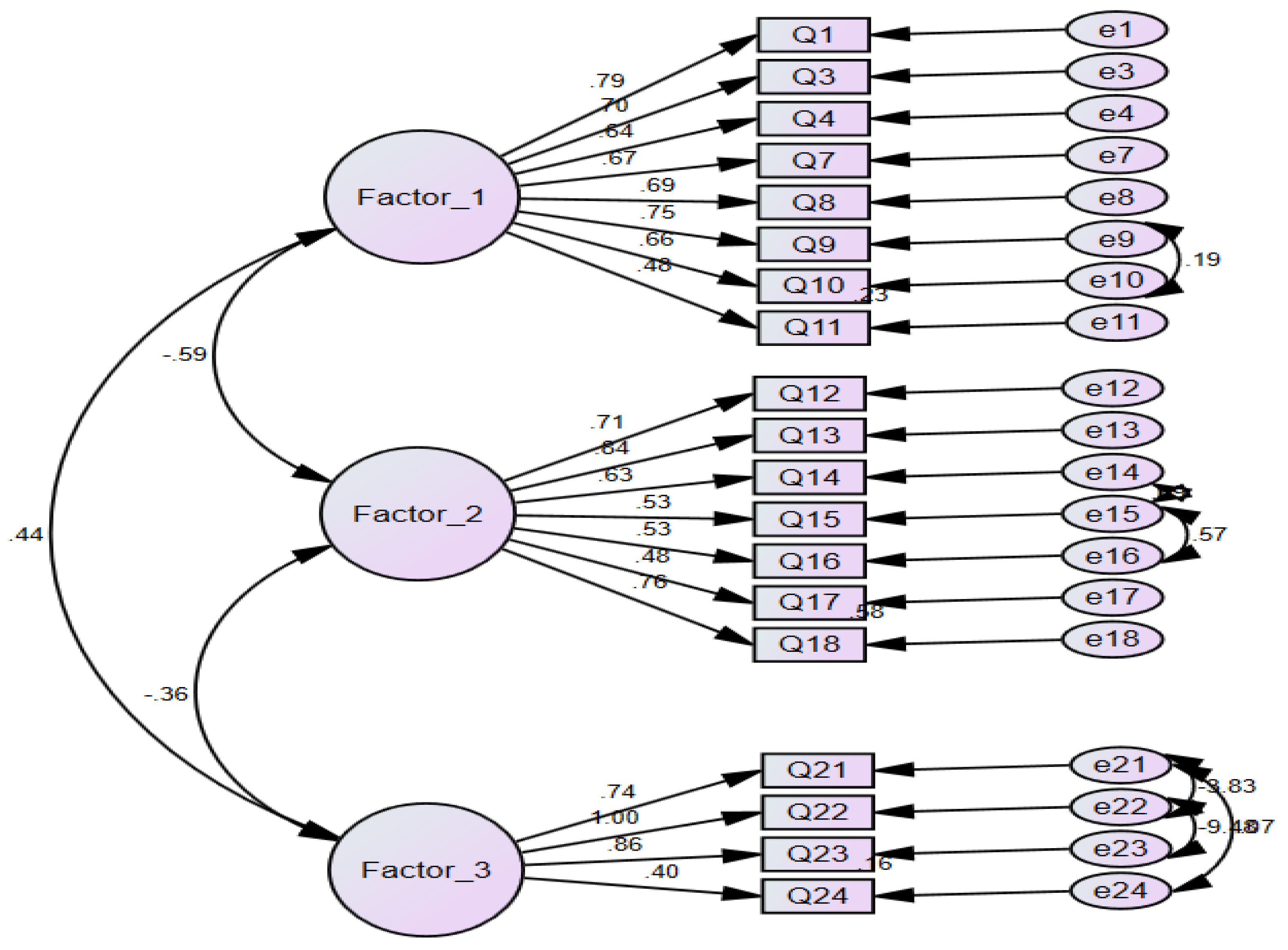
4.6. Confirmatory Factor Analysis (CFA)
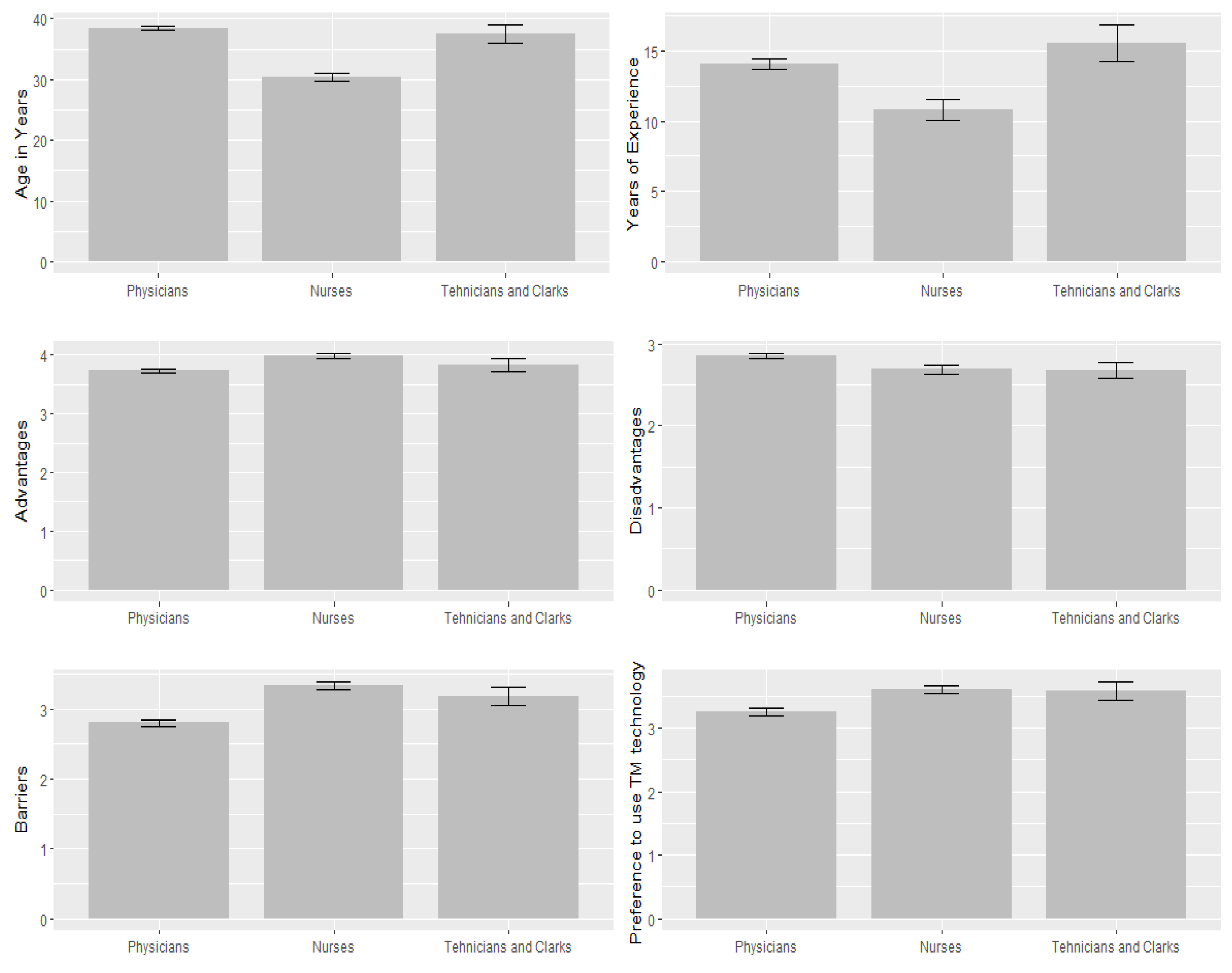
4.7. Discriminant Validity
4.8. Reliability Analysis and Convergent Validity
5. Discussion
5.1. Utilization of Telemedicine and Associated Factors
5.2. Construct Validity of the PTIDB
5.3. Divergent Validity of the PTIDB
5.4. Discriminant (Known Group) Validity
5.5. Reliability of the PTIDB
5.6. Strengths, Limitations, and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19–11 March 2020. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 12 May 2022).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard | WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. 2022. Available online: https://covid19.who.int (accessed on 21 September 2022).
- El Kassas, M.; Asem, N.; Abdelazeem, A.; Madkour, A.; Sayed, H.; Tawheed, A.; Al Shafie, A.; Gamal, M.; Elsayed, H.; Badr, M.; et al. Clinical features and laboratory characteristics of patients hospitalized with COVID-19: Single centre report from Egypt. J. Infect. Dev. Ctries 2020, 14, 1352–1360. [Google Scholar] [CrossRef]
- World Health Organization WHO Health Emergency Dashboard. WHO (COVID-19) Homepage. Egypt Situation. 2022. Available online: https://covid19.who.int/region/emro/country/eg (accessed on 11 August 2022).
- World Health Organization. Egypt WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. 2022. Available online: https://covid19.who.int/?mapFilter=vaccinations (accessed on 21 September 2022).
- Medhat, M.A.; El Kassas, M. COVID-19 in Egypt: Uncovered figures or a different situation? J. Glob. Health 2020, 10, 010368. [Google Scholar] [CrossRef]
- Zhao, Z.; Li, X.; Liu, F.; Zhu, G.; Ma, C.; Wang, L. Prediction of the COVID-19 spread in African countries and implications for prevention and control: A case study in South Africa, Egypt, Algeria, Nigeria, Senegal and Kenya. Sci. Total Environ. 2020, 729, 138959. [Google Scholar] [CrossRef]
- Mahmoud, K.; Jaramillo, C.; Barteit, S. Telemedicine in low-and middle-income countries during the COVID-19 pandemic: A scoping review. Front. Public Health 2022, 10, 914423. [Google Scholar] [CrossRef] [PubMed]
- Perrone, G.; Zerbo, S.; Bilotta, C.; Malta, G.; Argo, A. Telemedicine during Covid-19 pandemic: Advantage or critical issue? Med.-Leg. J. 2020, 88, 76–77. [Google Scholar] [CrossRef]
- Doraiswamy, S.; Abraham, A.; Mamtani, R.; Cheema, S. Use of telehealth during the COVID-19 pandemic: Scoping review. J. Med. Internet Res. 2020, 22, e24087. [Google Scholar] [CrossRef] [PubMed]
- Hong, Z.; Li, N.; Li, D.; Li, J.; Li, B.; Xiong, W.; Lu, L.; Li, W.; Zhou, D. Telemedicine during the COVID19 pandemic: Experiences from western China. J. Med. Internet Res. 2020, 22, e19577. [Google Scholar] [CrossRef]
- WHO Group Consultation on Health Telematics (1997: Geneva, Switzerland). (1998). A Health Telematics Policy in Support of WHO’s Health-for-All Strategy for Global Health Development: Report of the WHO Group Consultation on Health Telematics, 11–16 December, Geneva. World Health Organization. 1997. Available online: https://apps.who.int/iris/handle/10665/63857 (accessed on 3 June 2022).
- World Health Organization. Fifty-eighth World Health Assembly, Geneva: Resolutions and decisions, annex. In Proceedings of the Fifty-Eighth World Health Assembly, Geneva, Switzerland, 16–25 May 2005. [Google Scholar]
- Craig, J.; Patterson, V. Introduction to the practice of telemedicine. J. Telemed. Telecare 2005, 11, 3–9. [Google Scholar] [CrossRef]
- Vidal-Alaball, J.; Garcia Domingo, J.L.; Garcia Cuyàs, F.; Mendioroz Peña, J.; Flores Mateo, G.; Deniel Rosanas, J.; Sauch Valmaña, G. A cost savings analysis of asynchronous teledermatology compared to face-to-face dermatology in Catalonia. BMC Health Serv. Res. 2018, 18, 650. [Google Scholar] [CrossRef]
- Langabeer, J.R.; Champagne-Langabeer, T.; Alqusairi, D.; Kim, J.; Jackson, A.; Persse, D.; Gonzalez, M. Cost–benefit analysis of telehealth in pre-hospital care. J. Telemed. Telecare 2017, 23, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Sayani, S.; Muzammil, M.; Saleh, K.; Muqeet, A.; Zaidi, F.; Shaikh, T. Addressing cost and time barriers in chronic disease management through telemedicine: An exploratory research in select low-and middle-income countries. Ther. Adv. Chronic Dis. 2019, 10, 2040622319891587. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Chen, Y. Telemedicine in the cloud era: Prospects and challenges. IEEE Pervasive Comput. 2015, 14, 54–61. [Google Scholar] [CrossRef]
- Amudha, R.; Nalini, R.; Alamelu, R.; Badrinath, V.; Sharma, M.N. Telehealth and Telenursing-Progression in healthcare practice. Res. J. Pharm. Technol. 2017, 10, 2797–2800. [Google Scholar] [CrossRef]
- Stroetmann, K.A.; Kubitschke, L.; Robinson, S.; Stroetmann, V.; Cullen, K.; McDaid, D. How Can Telehealth Help in the Provision of Integrated Care? World Health Organization: Geneva, Switzerland, 2010; pp. 1–39. [Google Scholar]
- Mostafa, P.I.N.; Hegazy, A.A. Dermatological consultations in the COVID-19 era: Is teledermatology the key to social distancing? An Egyptian experience. J. Dermatolog. Treat. 2020, 33, 910–915. [Google Scholar] [CrossRef]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best practices for developing and validating scales for health, social, and behavioral research: A primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef]
- Boparai, J.K.; Singh, S.; Kathuria, P. How to design and validate a questionnaire: A guide. Curr. Clin. Pharmacol. 2018, 13, 210–215. [Google Scholar] [CrossRef]
- Parmanto, B.; Lewis, A.N., Jr.; Graham, K.M.; Bertolet, M.H. Development of the telehealth usability questionnaire (TUQ). Int. J. Telerehabil. 2016, 8, 3. [Google Scholar] [CrossRef]
- Lund, A.M. Measuring usability with the USE questionnaire. Usability Interface 2001, 8, 3–6. [Google Scholar]
- Hirani, S.P.; Rixon, L.; Beynon, M.; Cartwright, M.; Cleanthous, S.; Selva, A.; Sanders, C.; Newman, S.P. Quantifying beliefs regarding telehealth: Development of the whole systems demonstrator service user technology acceptability questionnaire. J. Telemed. Telecare 2017, 23, 460–469. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Ayatollahi, H.; Sarabi, F.Z.P.; Langarizadeh, M. Clinicians’ knowledge and perception of telemedicine technology. Perspect. Health Inf. Manag. 2015, 12, 1c. [Google Scholar]
- Kyriazos, T.A. Applied psychometrics: Sample size and sample power considerations in factor analysis (EFA, CFA) and SEM in general. J. Psychol. 2018, 9, 2207. [Google Scholar] [CrossRef]
- Nunnally, J.C. Psychometric Theory, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Bonett, D.G. Sample size requirements for testing and estimating coefficient alpha. J. Educ. Behav. Stat. 2002, 27, 335–340. [Google Scholar] [CrossRef]
- Bujang, M.A.; Omar, E.D.; Baharum, N.A. A review on sample size determination for Cronbach’s alpha test: A simple guide for researchers. Malays. J. Med. Sci. 2018, 25, 85. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.E.; Babin, B.J.; Black, W.C. Multivariate Data Analysis: A Global Perspective, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Gulledge, C.M.; Smith, D.G.; Ziedas, A.; Muh, S.J.; Moutzouros, V.; Makhni, E.C. Floor and ceiling effects, time to completion, and question burden of PROMIS CAT domains among shoulder and knee patients undergoing nonoperative and operative treatment. JBJS Open Access 2019, 4, e0015. [Google Scholar] [CrossRef] [PubMed]
- Pillai, N.V.; Rjumohan, A. Reliability, Validity and Uni-Dimensionality: A Primer. 2020. Available online: https://mpra.ub.uni-muenchen.de/id/eprint/101714 (accessed on 26 September 2022).
- MacNeill, V.; Sanders, C.; Fitzpatrick, R.; Hendy, J.; Barlow, J.; Knapp, M.; Rogers, A.; Bardsley, M.; Newman, S.P. Experiences of front-line health professionals in the delivery of telehealth: A qualitative study. Br. J. Gen. Pract. 2014, 64, e401–e407. [Google Scholar] [CrossRef]
- Gaggioli, A.; Di Carlo, S.; Mantovani, F.; Castelnuovo, G.; Riva, G. A telemedicine survey among Milan doctors. J. Telemed. Telecare 2005, 11, 29–34. [Google Scholar] [CrossRef]
- Gagnon, M.P.; Orruño, E.; Asua, J.; Abdeljelil, A.B.; Emparanza, J. Using a modified technology acceptance model to evaluate healthcare professionals’ adoption of a new telemonitoring system. Telemed. e-Health 2012, 18, 54–59. [Google Scholar] [CrossRef]
- DeVellis, R.F.; Thorpe, C.T. Scale Development: Theory and Applications; Sage Publications: New York, NY, USA, 2021. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Frequency | Percent |
|---|---|---|---|
| Age (mean ± SD) | 36.18 ± 8.93 | ||
| Sex | Male | 308 | 54.42 |
| Female | 258 | 45.58 | |
| Residence | Cairo/Giza | 133 | 23.50 |
| Other | 433 | 76.50 | |
| Occupation | Physicians | 371 | 65.50 |
| Nurses | 155 | 27.40 | |
| Technician and Clarks | 40 | 7.10 | |
| Place of work | Academic Centre/university hospital | 259 | 45.80 |
| General Hospital | 153 | 27.00 | |
| Private hospital/clinic/centers | 112 | 19.80 | |
| Police hospital | 5 | 0.90 | |
| Other | 37 | 6.50 | |
| Variables | Did Not Use Telemedicine 349 (61.7) | Used Telemedicine 217(38.3) | T-Test/Chi-Square | p-Value | |
|---|---|---|---|---|---|
| N (%) | |||||
| Gender | Male | 184 (59.7) | 124 (40.3) | 1.05 | 0.305 |
| Female | 165 (64.0) | 93 (36.0) | |||
| Residence | Cairo/Giza | 75 (56.40) | 58 (43.60) | 2.04 | 0.153 |
| Other | 274 (63.3) | 159 (36.7) | |||
| Job | Physicians | 204 (55.00) | 167 (45.00) | 28.26 | <0.001 |
| Nurses | 123 (79.4) | 32 (20.6) | |||
| Technician and Clarks | 22 (55.00) | 18 (45.00) | |||
| Place of work | Academic Centre/university hospital | 156 (62.20) | 103 (30.80) | 3.85 | 0.426 |
| General Hospital | 104 (68.00) | 49 (32.00) | |||
| Private hospital/clinic/centres | 64 (51.70) | 48 (42.90) | |||
| Police hospital | 3 (60.00) | 2 (40.0) | |||
| Other | 22 (59.50) | 15 (40.50) | |||
| Age | (mean ± Std. Deviation) | 35.40 ± 8.92 | 7.42 ± 8.82 | −2.01 | 0.009 |
| Year of experience | 12.79 ± 8.23 | 14.02 ± 8.36 | −0.171 | 0.087 | |
| Questionnaire’s Items | Factor 1 | Factor 2 | Factor 3 | Communalities |
|---|---|---|---|---|
| Q1 | 0.77 | −0.03 | −0.08 | 0.67 |
| Q3 | 0.78 | 0.04 | 0.01 | 0.57 |
| Q4 | 0.76 | 0.11 | 0.00 | 0.52 |
| Q7 | 0.72 | −0.06 | 0.06 | 0.53 |
| Q8 | 0.66 | −0.07 | −0.07 | 0.52 |
| Q9 | 0.58 | −0.25 | −0.15 | 0.62 |
| Q10 | 0.64 | −0.11 | −0.05 | 0.51 |
| Q11 | 0.61 | 0.06 | 0.04 | 0.34 |
| Q12 | −0.12 | 0.70 | −0.08 | 0.54 |
| Q13 | −0.08 | 0.71 | 0.14 | 0.63 |
| Q14 | −0.08 | 0.68 | −0.07 | 0.49 |
| Q15 | 0.14 | 0.78 | 0.05 | 0.56 |
| Q16 | 0.16 | 0.79 | 0.06 | 0.56 |
| Q17 | −0.11 | 0.60 | −0.18 | 0.39 |
| Q18 | −0.03 | 0.69 | 0.16 | 0.58 |
| Q21 | −0.08 | 0.02 | −0.86 | 0.70 |
| Q22 | 0.22 | −0.11 | −0.60 | 0.55 |
| Q23 | −0.06 | −0.01 | −0.83 | 0.67 |
| Q24 | 0.06 | 0.06 | −0.64 | 0.42 |
| Factors | Correlations Test | Factor-1 | Factor-2 | Factor-3 |
|---|---|---|---|---|
| Importance of TM | r (p-value) | 1 | −0.49 (<0.001) | 0.41(<0.001) |
| Disadvantages of TM | 1 | −0.32(<0.001) | ||
| Barriers to TM utilization | 1 |
| Variables | N | Mean | Std. Deviation | F | Sig. | |
|---|---|---|---|---|---|---|
| Age | Physicians | 371 | 38.46 | 7.70 | 43.02 | <0.001 |
| Nurses | 155 | 30.39 | 8.97 | |||
| Technician and Clarks | 40 | 37.50 | 9.44 | |||
| Year of experience | Physicians | 371 | 14.05 | 7.59 | 2.77 | 0.096 |
| Nurses | 155 | 10.80 | 9.37 | |||
| Technician and Clarks | 40 | 15.53 | 8.28 | |||
| Importance | Physicians | 371 | 3.76 | 0.63 | 11.49 | <0.001 |
| Nurses | 155 | 4.00 | 0.51 | |||
| Technician and Clarks | 40 | 3.89 | 0.63 | |||
| Disadvantages | Physicians | 371 | 2.94 | 0.68 | 8.32 | 0.004 |
| Nurses | 155 | 2.74 | 0.70 | |||
| Technician and Clarks | 40 | 2.76 | 0.64 | |||
| Barriers | Physicians | 371 | 2.84 | 0.79 | 27.19 | <0.001 |
| Nurses | 155 | 3.29 | 0.72 | |||
| Technician and Clarks | 40 | 3.16 | 0.87 | |||
| Preference to use TM technology | Physicians | 371 | 4.41 | 3.02 | 19.45 | <0.001 |
| Nurses | 155 | 5.83 | 3.01 | |||
| Technician and Clarks | 40 | 5.50 | 3.26 | |||
| Factors/Items | Mean ± SD | Item to Mean Score Correlation | Cronbach’s Alpha | ||
|---|---|---|---|---|---|
| r | p | ||||
| Importance | 3.84 ± 0.61 | - | - | - | 0.87 |
| Q1 | 3.72 ± 0.82 | 0.80 | 0.001 | 0.74 | |
| Q3 | 3.91 ± 0.85 | 0.74 | 0.001 | 0.65 | |
| Q4 | 3.99 ± 0.74 | 0.69 | 0.001 | 0.59 | |
| Q7 | 4.10 ± 0.74 | 0.70 | 0.001 | 0.62 | |
| Q8 | 3.88 ± 0.84 | 0.73 | 0.001 | 0.64 | |
| Q9 | 3.37 ± 1.05 | 0.79 | 0.001 | 0.68 | |
| Q10 | 3.70 ± 0.90 | 0.74 | 0.001 | 0.61 | |
| Q11 | 4.04 ± 0.83 | 0.60 | 0.001 | ||
| Disadvantages | 2.79 ± 0.69 | - | - | - | 0.82 |
| Q12 | 2.83 ± 0.97 | 0.74 | 0.001 | 0.61 | |
| Q13 | 3.23 ± 1.03 | 0.79 | 0.001 | 0.62 | |
| Q14 | 2.58 ± 0.89 | 0.71 | 0.001 | 0.60 | |
| Q15 | 2.75 ± 0.98 | 0.72 | 0.001 | 0.61 | |
| Q16 | 2.99 ± 0.99 | 0.72 | 0.001 | 0.59 | |
| Q17 | 2.38 ± 0.84 | 0.63 | 0.001 | 0.49 | |
| Q18 | 3.40 ± 1.02 | 0.60 | 0.001 | ||
| Barriers | 2.99 ± 0.81 | - | - | - | 0.79 |
| Q21 | 2.96 ± 1.14 | 0.83 | 0.001 | 0.63 | |
| Q22 | 3.29 ± 0.96 | 0.73 | 0.001 | 0.54 | |
| Q23 | 2.61 ± 1.11 | 0.81 | 0.001 | 0.62 | |
| Q24 | 3.10 ± 1.01 | 0.69 | 0.001 | 0.55 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Youssef, N.; Ghazy, R.M.; Mahdy, R.E.; Abdalgabar, M.; Elshaarawy, O.; Alboraie, M. Development, Validity, and Reliability of the Perceived Telemedicine Importance, Disadvantages, and Barriers (PTIDB) Questionnaire for Egyptian Healthcare Professionals. Int. J. Environ. Res. Public Health 2022, 19, 12678. https://doi.org/10.3390/ijerph191912678
Youssef N, Ghazy RM, Mahdy RE, Abdalgabar M, Elshaarawy O, Alboraie M. Development, Validity, and Reliability of the Perceived Telemedicine Importance, Disadvantages, and Barriers (PTIDB) Questionnaire for Egyptian Healthcare Professionals. International Journal of Environmental Research and Public Health. 2022; 19(19):12678. https://doi.org/10.3390/ijerph191912678
Chicago/Turabian StyleYoussef, Naglaa, Ramy Mohamed Ghazy, Reem Ezzat Mahdy, Mohammad Abdalgabar, Omar Elshaarawy, and Mohamed Alboraie. 2022. "Development, Validity, and Reliability of the Perceived Telemedicine Importance, Disadvantages, and Barriers (PTIDB) Questionnaire for Egyptian Healthcare Professionals" International Journal of Environmental Research and Public Health 19, no. 19: 12678. https://doi.org/10.3390/ijerph191912678
APA StyleYoussef, N., Ghazy, R. M., Mahdy, R. E., Abdalgabar, M., Elshaarawy, O., & Alboraie, M. (2022). Development, Validity, and Reliability of the Perceived Telemedicine Importance, Disadvantages, and Barriers (PTIDB) Questionnaire for Egyptian Healthcare Professionals. International Journal of Environmental Research and Public Health, 19(19), 12678. https://doi.org/10.3390/ijerph191912678