1. Current Research
Suicide prevention is an urgent public health problem in the U.S. [
1]. In comparison with years prior, past-year prevalence rates of suicide ideation (4.3%) and attempts (0.6%) remain elevated [
1]). Suicide prevention and intervention efforts depend on individuals at risk communicating to others their ideation or intent. Even suicide prevention efforts that rely on passive detection (e.g., machine learning) ultimately require that an individual at risk for suicide communicates with health care professionals or social networks for any form of intervention to take place. Despite the importance of understanding, facilitating and appropriately responding to suicidal communications, this area of research remains relatively untapped [
2].
The largest body of literature on this topic focuses on prevalence rates. A recent meta-analysis indicated that 44.5% of decedents were known to have communicated about their intent before death [
3]). Across studies using large samples, there is high variability in rates. Between 33% and 61% of individuals with a past suicide attempt reported communicating about their intent [
4,
5,
6]. Although suicidal communications are not homogenous [
3,
6], communication is often assumed to be direct and verbal and serve a help-seeking function. Prior research suggests [
6,
7] that there are various forms and functions of suicidal communications. However, current research largely neglects the potential for a range of forms and functions of suicidal communications, which may explain the high variability in prevalence across samples.
This neglect of the complex, multifaceted nature of suicidal communications is directly related to the gap in measurement. To date, suicidal communication measurement primarily consists of single-item and unvalidated interviews [
8,
9]. Only two published multi-item measures exist related to suicidal communications. The validated Self-Harm and Suicide Disclosure Scale (SHSDS) [
10] assesses the level of detail attempt survivors provide (e.g., method used and severity). Hypothesized to be related to suicide stigma, this unidimensional measure assesses how much information survivors share with others about their suicide ideation and attempt histories. The Family Quality Reaction Scale (FQRS) [
11] assesses the helpfulness of communication recipients’ reactions. The scale is unidimensional and captures increased comfort and perceived helpfulness following disclosure. These measures are a promising initial attempt at comprehensive measurement of suicidal communications. Frey and colleagues [
7,
10,
11] have provided the most significant contribution thus far to this area of research. Two limitations necessitate creating additional measures: these measures do not exist within a theoretical model, and do not completely address the need for a comprehensive examination of suicidal communications. While it is helpful to understand the amount of detail provided in suicide disclosure and in the helpfulness of reactions, these measures do not work together to describe the process of suicidal communications. A comprehensive and theoretically based battery of validated instruments would fill this critical gap.
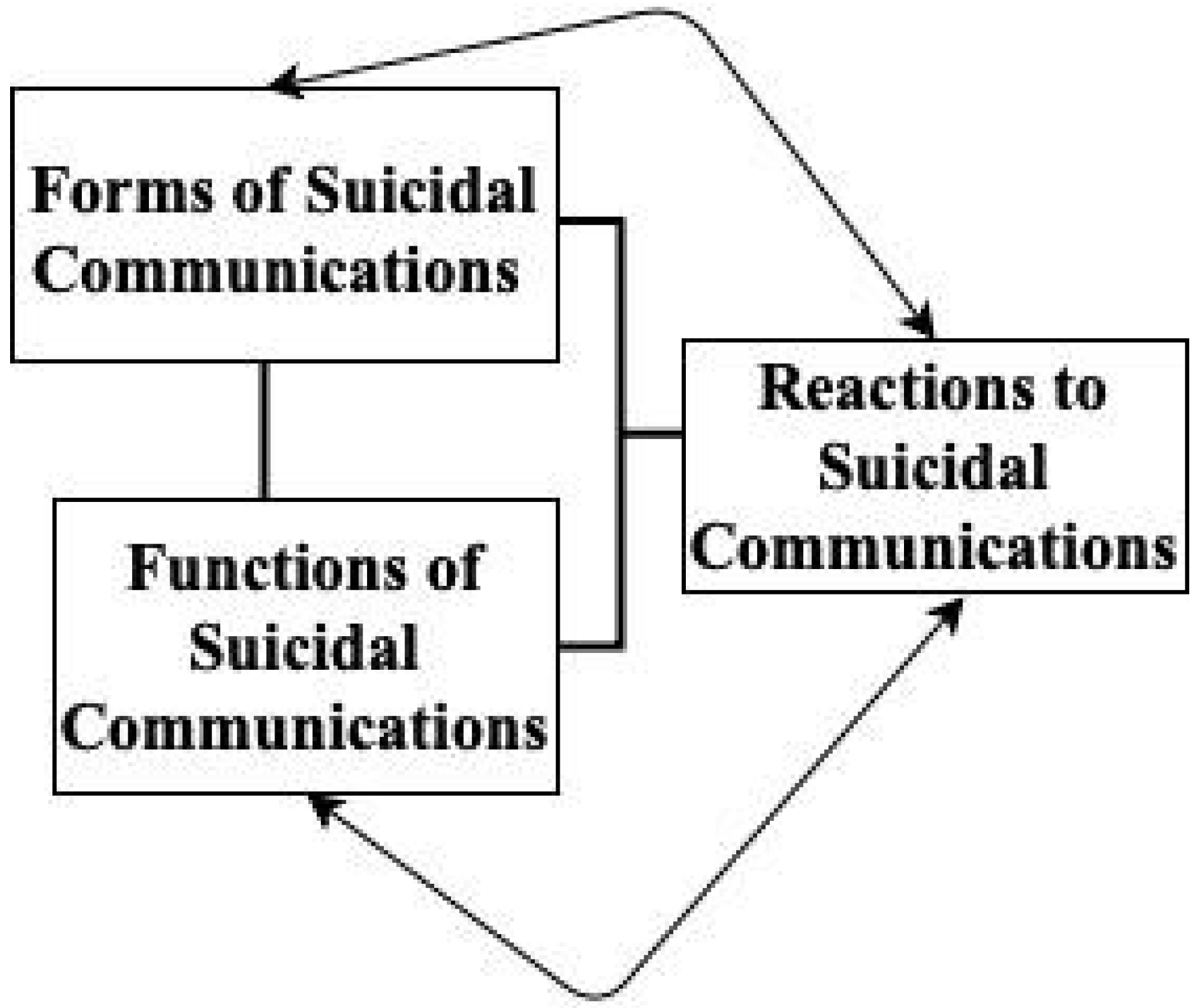
The current article presents a measure of the functions of suicidal communications grounded in a preliminary empirical framework (see
Figure 1. This theory states that suicidal communications are an interpersonal construct that must be defined in terms of their form, function, and perceived reactions as suggested by prior research [
6,
7]. The current article aims to fill a gap in measurement of the functions construct. Prior theoretical work exists to hypothesize multiple functions of suicidal communications [
7]). However, this hypothesis has not been tested empirically through factor analytic methods. First, such communications may serve a help-seeking function (e.g., treatment seeking and support seeking). For instance, in a series of qualitative interviews about suicide communication with a small sample of 40 individuals with a history of suicide attempts, the majority endorsed getting help as the primary reason to communicate [
12]. Although the term ‘getting help’ was broadly used, examples consisted of seeking care from any health care provider or paraprofessional and obtaining support or help from friends or family to get connected with care. Similarly, in an undergraduate sample with past suicidal ideation who reported being directly asked by others if they were considering suicide, 40.6% reported communicating to get support in seeking treatment, 36.3% reported communicating to receive medication, 33.8% to receive therapy, and 11.9% to seek hospitalization [
9]. These studies suggest that help seeking is likely a commonly endorsed function of suicidal communications.
Individuals may also communicate about suicide to plan and prepare for suicide, such as directly soliciting another’s assistance to attempt suicide, obtaining another person’s assistance to prepare for death, or communicating as a way of obtaining closure on a relationship before death (e.g., saying goodbye to loved ones and resolving interpersonal disputes). Direct solicitation of others’ assistance to die by suicide has most frequently been examined on pro-suicide message boards and chatrooms, and other discussion-based mechanisms [
13]. This form of communication may include a person requesting and receiving detailed information about suicide methods or general self-injury techniques [
14,
15], or receiving encouragement after communicating intent [
16,
17,
18,
19] In one study, 14.5% of internet forum users reported using forums specifically for these reasons [
20]. Although no literature on tying up loose ends before death [
21] directly speaks to others’ involvement, some preparations for death (e.g., arranging care for dependents) are highly likely to involve a trusted person. Finally, given high percentages of saying goodbye to loved ones found in other modes of death (physician-assisted death; 87%) [
22], some individuals may similarly say goodbye before suicide. For instance, 38% of a male sample who had attempted suicide reported saying goodbye to loved ones before the attempt [
23]. Suicidal communications may therefore be motivated by plans and preparations for suicide.
Suicidal communications may also serve an intrinsic interpersonal emotion regulation function. Broadly, intrinsic interpersonal emotion regulation occurs when individuals seek and engage in specific interpersonal interactions (e.g., venting, reassurance seeking, and communicating emotions) to regulate their emotions [
24,
25]. Specifically, as thoughts of suicide may be highly distressing, negative affect may be alleviated by communicating with others. Research highlighting reported positive feelings from individuals after communicating about or discussing suicide during a research study e.g., [
26,
27,
28] and crisis line call [
29] supports this hypothesis. Indeed, in an undergraduate sample who had been directly asked by others if they had thoughts of suicide, 69% endorsed disclosing to obtain emotional support [
9]. In the qualitative interview study previously mentioned, participants endorsed both the above—sharing their suicidal ideation/experiences to process with others and strengthening their relationship with that person [
12]. Ample evidence exists to support a potential interpersonal emotion regulation function of suicidal communications.
Finally, suicidal communications may be motivated by a desire to resolve ambivalence about suicide. Research on the decision-making process involved in suicide attempts highlights a period of “mulling over” [
30] that may encompass last attempts at seeking help, conflict resolution, and steps to relieve psychological pain. Approximately half of a psychiatric sample reported a consideration period (from first current thought to attempt) of less than 10 minutes and those who took longer reported elevated suicidal intent [
31]. Indeed, increased time for consideration may indicate greater chronic suicide risk. Attempts at ambivalence resolution through suicidal communications may, therefore, also represent heightened chronic risk.
5. Discussion
The current study was a psychometric pilot of a novel measure written to assess four potential functions of suicidal communications. Developed to fit within a theory [
53] that synthesizes existing empirical work on suicidal communication, the original set of items examined the potential for multiple functions of suicidal communications. Specifically, we posited four motivations: help-seeking, preparatory behavior, interpersonal emotion regulation, and ambivalence resolution. Results did not confirm the multiple functions of suicidal communications hypothesis. They revealed a unidimensional structure, capturing ambivalence resolution motivations. As the first measure to assess this construct, the current study represents a first step towards a comprehensive and theory-based measurement of suicidal communications. Results illuminate the next steps required for rigorous assessment of suicidal communication functions.
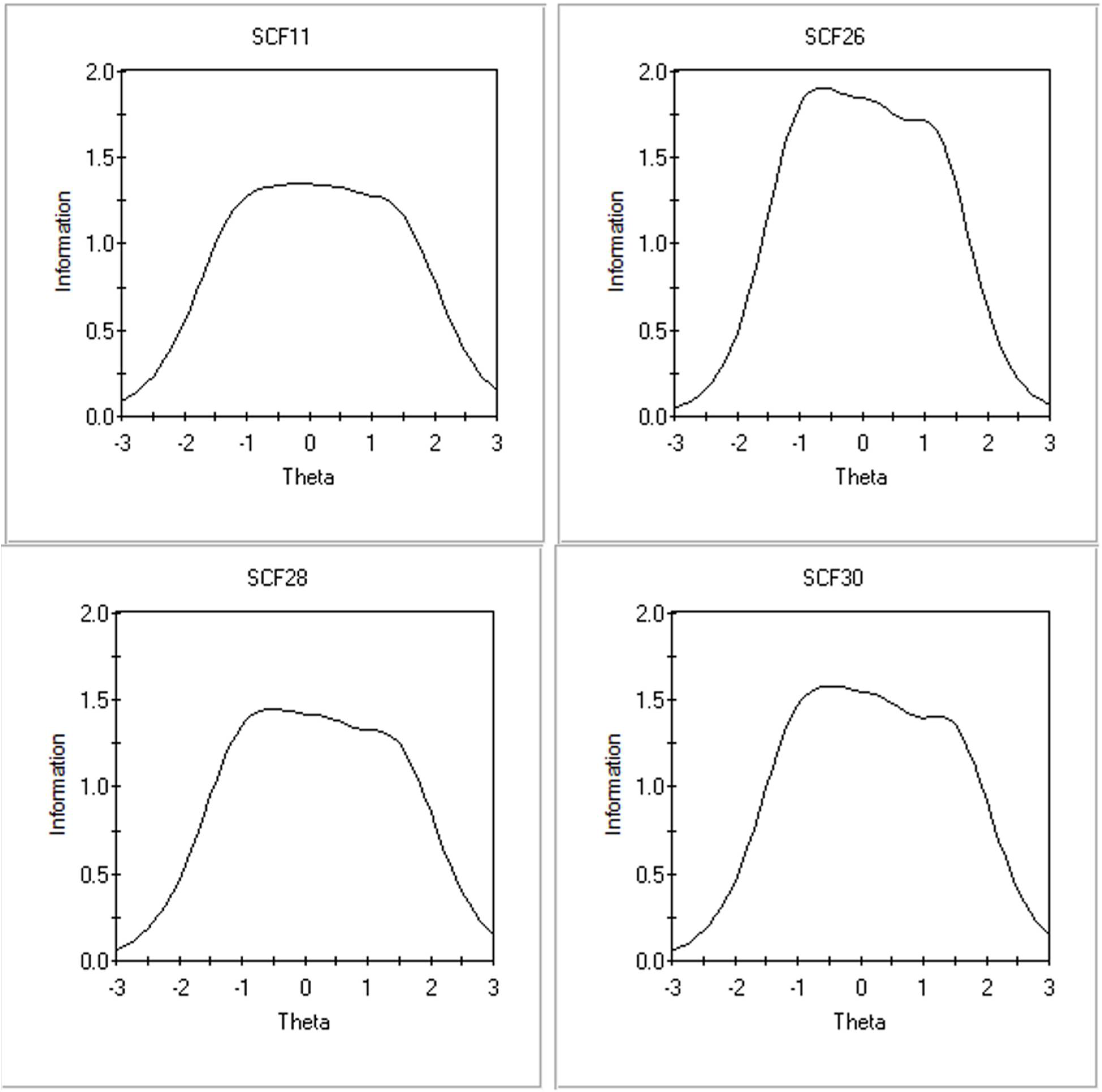
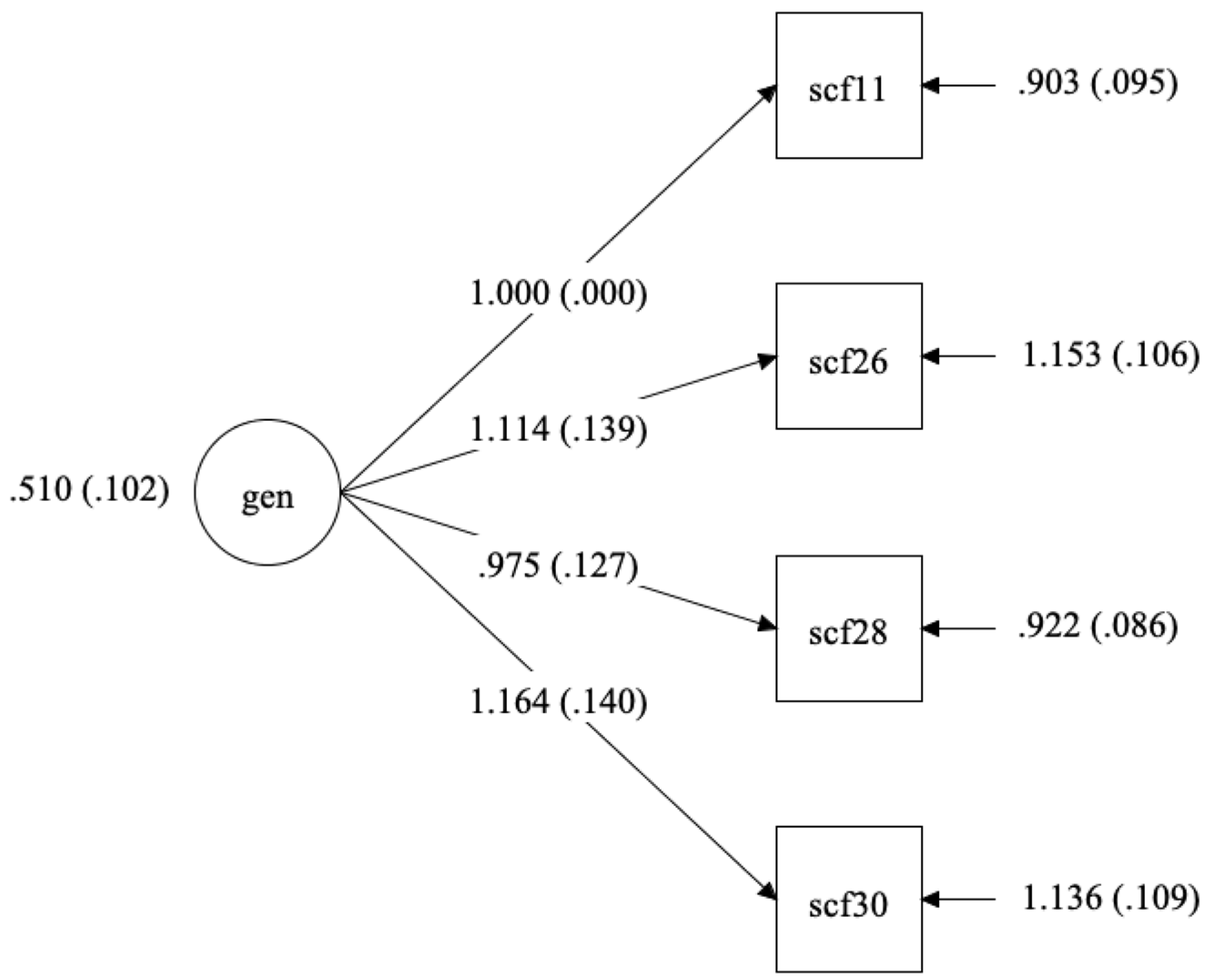
Given limited theoretical and empirical work [
6,
7], the current study relied on quantitative indices over theory-based measure development strategies to test the multiple functions of suicidal communications hypothesis. Item response theory methods were used following exploratory and confirmatory factor analysis to assess the measure’s structure. Initial signs (e.g., parallel analysis and EFA) pointed to a two-factor solution describing preparatory behavior and interpersonal conflict-related motivations, and IER motivations. Due to high correlations between both factors and the small percent of variance explained by the second factor, bifactor modeling was an appropriate next step in the analytic plan. Although the model converged, ancillary indices of fit and reliability indicated that the measure was primarily unidimensional.
The resulting scale comprised items related to final attempts to get help, indirect or avoidant communication, seeking connection, and suicide decision making. Given that people may communicate about suicide to strengthen relationships, get help or support [
12], or say goodbye [
23], these items primarily reflect an ambivalence resolution function that may encapsulate the undecided nature of most suicide decision making. While considering unsolidified suicide plans and preparations, the same individual may also be seeking help and relationship improvement. Given that people at risk of suicide experience low connectedness [
54], seeking conflict resolution or relationship repair may be a form of ambivalence resolution and reflect a critical part of the suicide decision-making process [
30].
Results suggest that there may not be categorically different functions of suicidal communications. Instead, ambivalence may underscore these seemingly disparate functions (help-seeking, preparation, interpersonal emotion regulation), characterized by conflicting desires to seek help or increase one’s connection to the world, while at the same time, considering preparation for death. Given the evidence that ambivalence about living and dying (as opposed to certainty about a desire to die) characterizes the suicidal state [
55,
56], communication during this period is likely to reflect this internal struggle. Further, since ambivalence about suicide comprises the simultaneous wish to live and the wish to die [
57], we might expect measure items such as those retained for the current study to reflect both dimensions. Finally, the role of ambivalence in suicidal communication is consistent with the non-linear change processes of suicide risk and desire (in addition to stable constructs) proposed by the fluid vulnerability theory of suicide [
58]. As suicidal desire and risk dynamically fluctuate in response to external and internal processes throughout periods of acute and baseline risk, communication about suicide may express this fluctuation by simultaneously serving life-oriented and death-oriented purposes.
If future research supports the ambivalence resolution function of suicidal communications, then communication may serve a key role in suicide decision making. They may bridge the “mulling over” and preparations steps on the path to suicide attempts [
30]. People may communicate thoughts of suicide to prepare for death and determine if they want to go through with an attempt. The outcome of suicidal communications may provide information relevant to a person’s decision-making process (e.g., improving a relationship and obtaining needed help after several attempts). Contrary to communication motivations for suicide attempts [
59], ambivalence resolution motivations for suicidal communications may, therefore, be associated with greater risk. Lengthier decision-making periods are associated with increased risk [
31,
60], and suicidal communications occurring during these periods may indicate a potentially critical point of transition from ideation to action.
Notably, the function of ambivalence resolution, as measured by the current scale, was positively and significantly correlated with history of suicide ideation and behavior, though the correlation was low. There was alternatively no significant association between past-year suicide ideation severity/frequency and ambivalence functions. Prior research indicates an association between reduced or non-communication (versus communication) and elevated suicide risk [
4,
61,
62]. In some respects, this non-significant correlation confirms prior work by finding a non-significant negative correlation with past-year ideation severity. However, the positive and significant correlation with lifetime suicide ideation and behavior suggests that people endorsing ambivalence motivations may have a history of heightened risk. These findings do not necessary suggest that those who communicate are at more or less risk of suicide, but only that people who endorse ambivalence resolution motivations are more likely to have experienced more of the suicide ideation and behavior spectrum to warrant a need for ambivalence resolution. Endorsement of ambivalence resolution motivations, therefore, suggests at least having deeply considered suicide as an option. Finally, as expected, the ambivalence resolution function was highly correlated with interpersonal motivations for suicide attempts in comparison with intrapersonal motivations. However, this correlation was not high enough to suggest that the two scales measured identical constructs. People engaging in suicidal behavior who report help-seeking and interpersonal motivations may also be more likely to communicate their intentions to resolve ambivalence.
6. Limitations
The present study is a first attempt at operationalizing the functions of suicidal communications. Given that the FSC-C is the first measure on the construct, the current study is also the first to test the multiple functions hypothesis. However, several limitations must be considered when interpreting our results. First, participants were recruited from Amazon Mechanical Turk (MTurk), eliciting potential data quality concerns. We took several steps to address this risk, such as the 95% approval rating eligibility criterion [
63], removal of duplicate respondents, free response and Likert scale attention checks, and a captcha to enter the survey. Further, we adhered to published pay recommendations available at the time the data were collected [
35]. However, these measures only reduced rather than eliminated the risk of collecting inattentive or fake respondents.
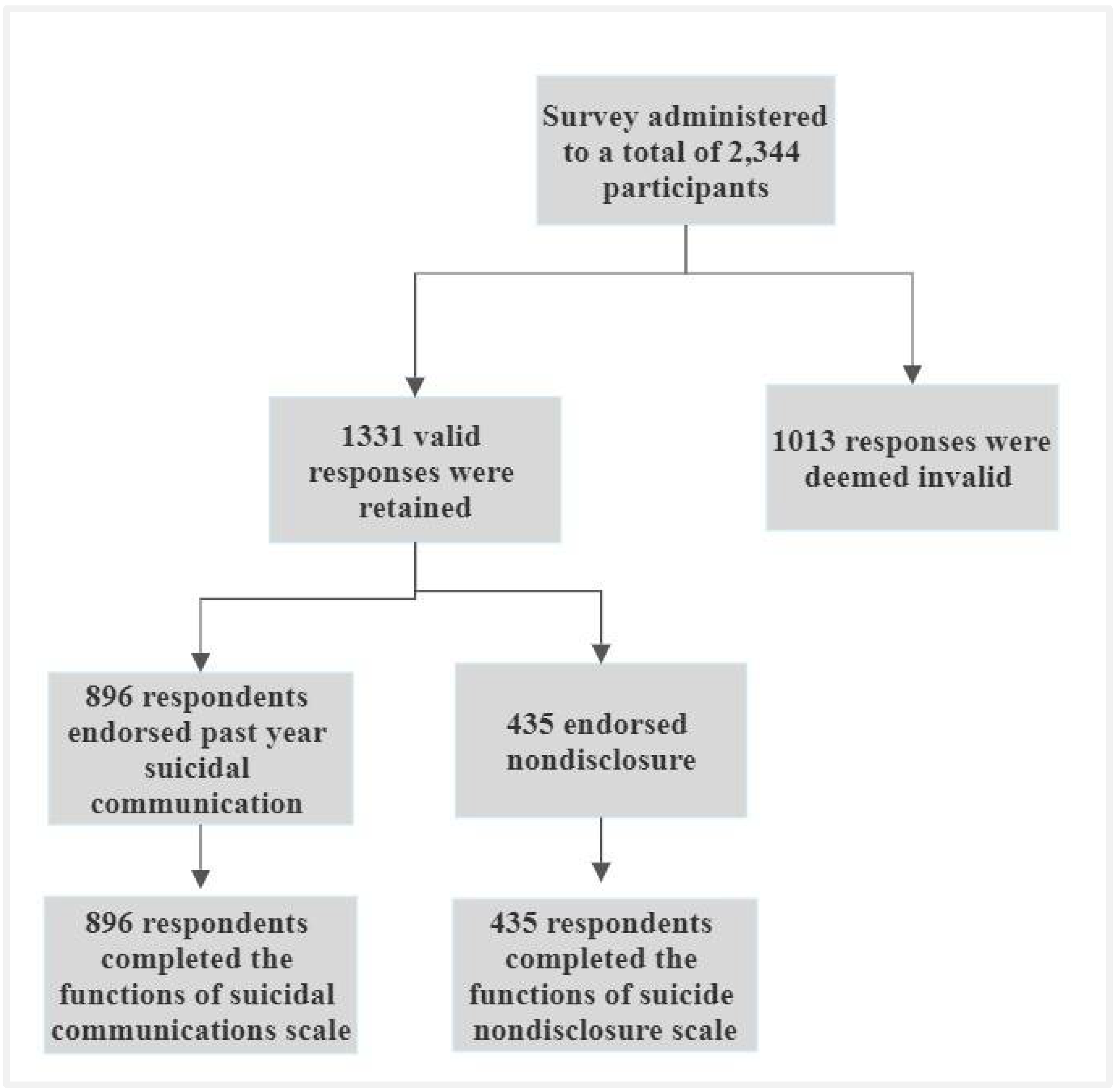
In total, over 50% of the data were removed due to low quality based on a series of attention checks and not utilized in the current study. However, recent research suggests that MTurk data quality may have declined in recent years [
64] and researcher perception of fair compensation may not match participant expectations [
65]. MTurk best practices research must stay abreast of the changing pay expectations and data quality assurance practices. As a result, low-quality responses may have eluded our careful review though all best practices available by the data collection start date were implemented.
Additionally, MTurk participants may not have represented the spectrum of suicidality as well as a clinical sample. Despite this limitation, several studies indicate that MTurk workers may yield a sample with less bias and more diversity than laboratory samples [
36,
66]. Further, MTurk workers report higher depression rates than other types of convenience samples, such as undergraduate college students [
67]. Compared with other convenience samples, MTurk may have advantages for recruiting participants with suicide ideation and behavior but may not yield the advantages of a clinical sample.
Most importantly, although the original item pool was developed based on prior empirical and theoretical work, existing research in this area is limited. The current study is a preliminary step towards formally operationalizing the functions of suicidal communications. Therefore, the resulting unidimensional measure may indicate the limited prior research on which to base item generation than the latent structure of suicidal communications. Relatedly, since there was no measure on the topic (i.e., the functions of suicidal communications) with which to compare psychometric properties, validity indices were limited to suicide ideation and behavior, and motivations for suicide attempts. Prior scales on suicidal communications focus on the helpfulness of family reactions and the amount of detail included in disclosures, neither of which assess functions of communications. While these scales are focused on suicidal communications, they are entirely different constructs than the one we aimed to capture. The scale focused on depth of disclosure [
10], which is the only validated measure on suicidal communications, was, unfortunately, not included in the survey due to system error.



{kind=link}
{kind=link}
{kind=link}
{kind=link}