Cost-Effectiveness Analysis of Contemporary Advanced Prostate Cancer Treatment Sequences †



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design Overview
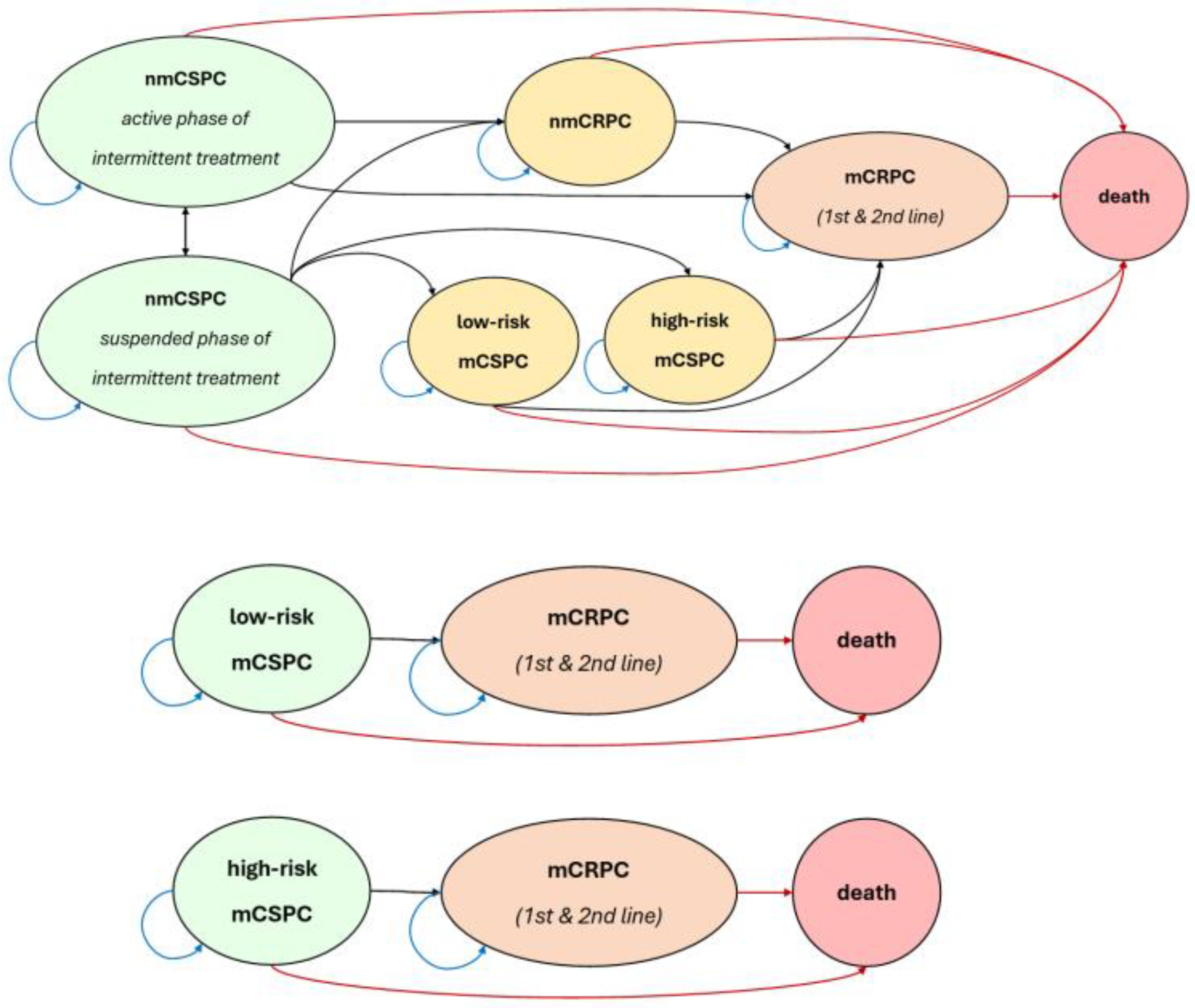
2.2. Model Structure
2.3. Novel Parameter Estimation Algorithm
2.4. Utility Values
2.5. Treatment Costs
2.6. Results Description
2.7. Sequence Description
3. Results
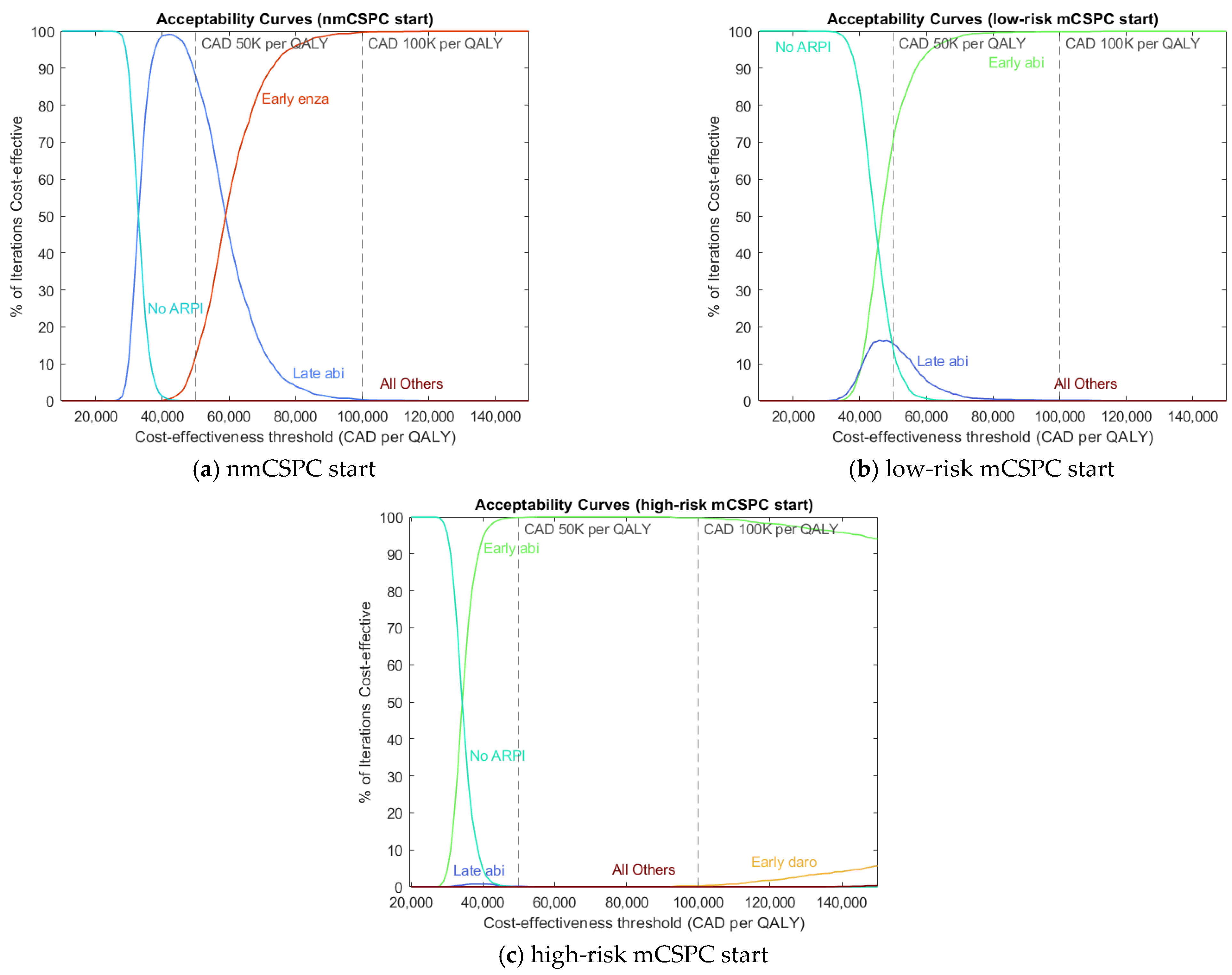
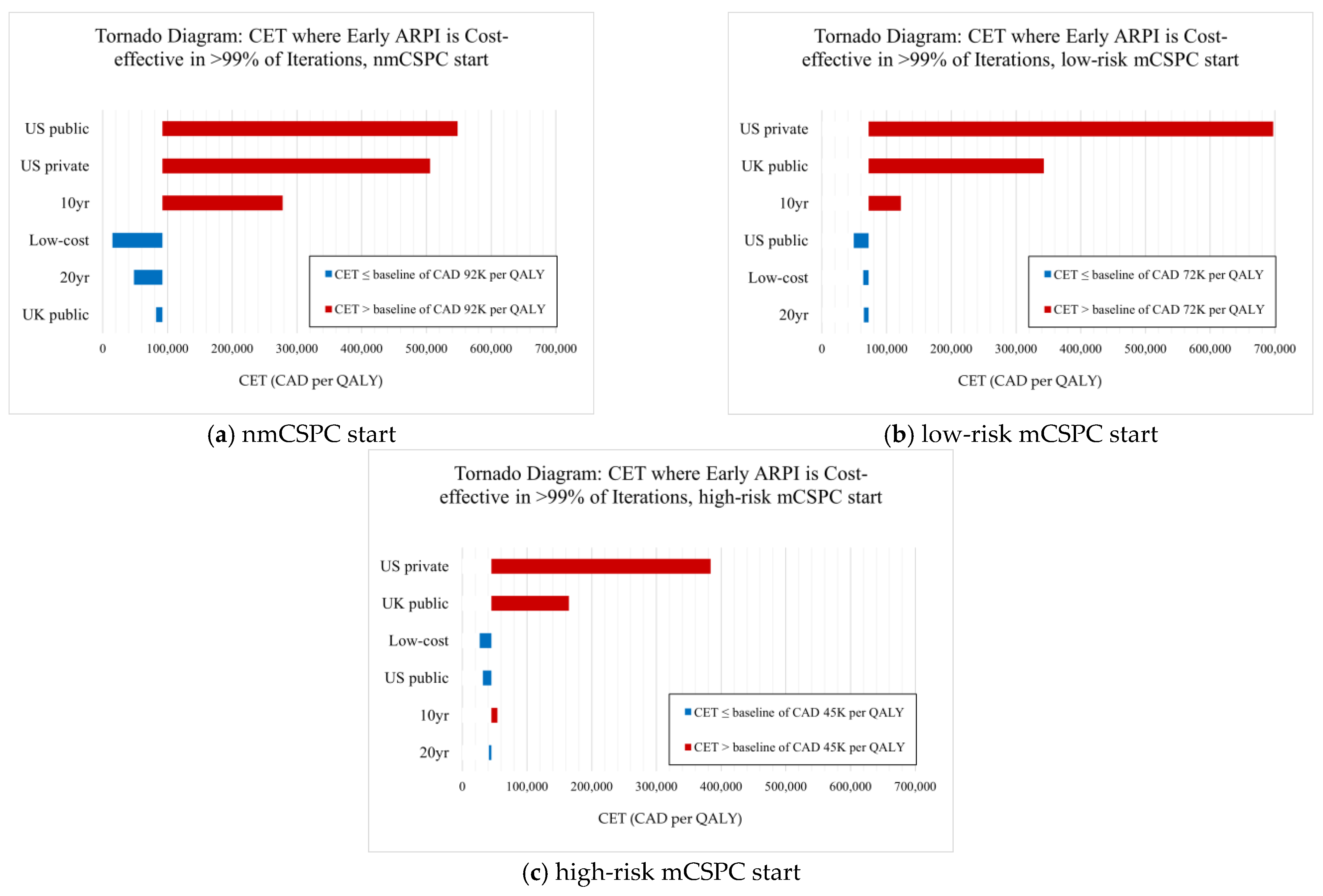
Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PCa | Prostate cancer |
| ARPI | Androgen receptor pathway inhibitor |
| ADT | Androgen deprivation therapy |
| nmCSPC | Nonmetastatic castration-sensitive prostate cancer |
| mCSPC | Metastatic castration-sensitive prostate cancer |
| nmCRPC | Nonmetastatic castration-resistant prostate cancer |
| mCRPC | Metastatic castration-resistant prostate cancer |
| NCCN | National Comprehensive Cancer Network |
| CUA | Canadian Urological Association |
| CDA | Canada’s Drug Agency |
| PFS | Progression-free survival |
| OS | Overall survival |
| KM | Kaplan–Meier |
| NHB | Net health benefit |
| CET | Cost-effectiveness threshold |
| ICER | Incremental cost-effectiveness ratio |
| AC | Acceptability curve |
| abi | Abiraterone |
| apa | Apalutamide |
| caba | Cabazitaxel |
| daro | Daroluatmide |
| doce | Docetaxel |
| enza | Enzalutamide |
References
- Wang, L.; Lu, B.; He, M.; Wang, Y.; Wang, Z.; Du, L. Prostate Cancer Incidence and Mortality: Global Status and Temporal Trends in 89 Countries From 2000 to 2019. Front. Public Health 2022, 10, 811044. [Google Scholar] [CrossRef]
- Freedland, S.J.; Luz, M.d.A.; De Giorgi, U.; Gleave, M.; Gotto, G.T.; Pieczonka, C.M.; Haas, G.P.; Kim, C.-S.; Ramirez-Backhaus, M.; Rannikko, A.; et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N. Engl. J. Med. 2023, 389, 1453–1465. [Google Scholar] [CrossRef] [PubMed]
- Chi, K.N.; Chowdhury, S.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, A.; Juárez, A.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide in patients with metastatic castration-sensitive prostate cancer: Final survival analysis of the randomized, double-blind, phase III TITAN study. J. Clin. Oncol. 2021, 39, 2294–2303. [Google Scholar] [CrossRef]
- Fizazi, K.; Foulon, S.; Carles, J.; Roubaud, G.; McDermott, R.; Fléchon, A.; Tombal, B.; Supiot, S.; Berthold, D.; Ronchin, P.; et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomised, phase 3 study with a 2×2 factorial design. Lancet 2022, 399, 1695–1707. [Google Scholar] [CrossRef] [PubMed]
- Hoyle, A.P.; Ali, A.; James, N.D.; Cook, A.; Parker, C.C.; de Bono, J.S.; Attard, G.; Chowdhury, S.; Cross, W.R.; Dearnaley, D.P.; et al. Abiraterone in “high-” and “low-risk” metastatic hormone-sensitive prostate cancer. Eur. Urol. 2019, 76, 719–728. [Google Scholar] [CrossRef]
- Saad, F.; Vjaters, E.; Shore, N.; Olmos, D.; Xing, N.; Pereira de Santana Gomes, A.J.; Cesar de Andrade Mota, A.; Salman, P.; Jievaltas, M.; Ulys, A.; et al. Darolutamide in Combination with Androgen-Deprivation Therapy in Patients with Metastatic Hormone-Sensitive Prostate Cancer from the Phase III ARANOTE Trial. J. Clin. Oncol. 2022, 42, 4271–4281. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Hussain, M.; Saad, F.; Fizazi, K.; Sternberg, C.N.; Crawford, D.; Manarite, J.; Muslin, D.; Farrington, T.; Tombal, B. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N. Engl. J. Med. 2022, 386, 1132–1142. [Google Scholar] [CrossRef]
- Sweeney, C.J.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Cheung, L.; Chi, K.N.; Chowdhury, S.; Frydenberg, M.; Horvath, L.G.; Joshua, A.M.; et al. Testosterone suppression plus enzalutamide versus testosterone suppression plus standard antiandrogen therapy for metastatic hormone- sensitive prostate cancer (ENZAMET): An international, open-label, randomised, phase 3 trial. Lancet Oncol. 2023, 24, 323–334. [Google Scholar] [CrossRef]
- De Bono, J.S.; Logothetis, C.J.; Molina, A.; Fizazi, K.; North, S.; Chu, L.; Chi, K.N.; Jones, R.J.; Goodman, O.B., Jr.; Saad, F.; et al. Abiraterone and increased survival in metastatic prostate cancer. N. Engl. J. Med. 2011, 364, 1995–2005. [Google Scholar] [CrossRef]
- Ryan, C.J.; Smith, M.R.; Fizazi, K.; Saad, F.; Mulders, P.F.A.; Sternberg, C.N.; Miller, K.; Logothetis, C.J.; Shore, N.D.; Small, E.J.; et al. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): Final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2015, 16, 152–160. [Google Scholar] [CrossRef]
- Scher, H.I.; Fizazi, K.; Saad, F.; Taplin, M.-E.; Sternberg, C.N.; Miller, K.; de Wit, R.; Mulders, P.; Chi, K.N.; Shore, N.D.; et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N. Engl. J. Med. 2012, 367, 1187–1197. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Shore, N.; Tammela, T.L.; Ulys, A.; Vjaters, E.; Polyakov, S.; Jievaltas, M.; Luz, M.; Alekseev, B.; Kuss, I.; et al. Darolutamide in nonmetastatic, castration-resistant prostate cancer. N. Engl. J. Med. 2019, 380, 1235–1246. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.; Fizazi, K.; Saad, F.; Rathenborg, P.; Shore, N.; Ferreira, U.; Ivaschenko, P.; Demirhan, E.; Modelska, K.; Phung, D.; et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N. Engl. J. Med. 2018, 378, 2465–2474. [Google Scholar] [CrossRef]
- Smith, M.R.; Saad, F.; Chowdhury, S.; Oudard, S.; Hadaschik, B.A.; Graff, J.N.; Olmos, D.; Mainwaring, P.N.; Lee, J.Y.; Uemura, H.; et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N. Engl. J. Med. 2018, 378, 1408–1418. [Google Scholar] [CrossRef]
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; Ahmed, B.; An, Y.; Bitting, R.; Chapin, B.; Cheng, H.H.; Cho, S.Y.; D’Amico, A.V.; et al. NCCN Clinical Practice Guidelines in Oncology: Prostate Cancer. Version 1.2025. Available online: https://www.NCCN.org (accessed on 10 February 2025).
- So, A.I.; Chi, K.; Danielson, B.; Fleshner, N.E.; Kinnaird, A.; Kapoor, A.; Niazi, T.; Pouliot, F.; Rendon, R.A.; Shayegan, B.; et al. 2022 UPDATE: Canadian Urological Association-Canadian Urologic Oncology Group guideline: Metastatic castration-naive and castration-sensitive prostate cancer (Summary of changes). Can. Urol. Assoc. J. 2022, 16, 389–391. [Google Scholar] [CrossRef]
- Saad, F.; Aprikian, A.; Finelli, A.; Fleshner, N.E.; Gleave, M.; Kapoor, A.; Niazi, T.; North, S.A.; Pouliot, F.; Rendon, R.A.; et al. 2022 Canadian Urological Association (CUA)-Canadian Uro Oncology Group (CUOG) guideline: Management of castration-resistant prostate cancer (CRPC). Can. Urol. Assoc. J. 2022, 16, E506–E515. [Google Scholar] [CrossRef] [PubMed]
- Binder, L.; Ghadban, M.; Sit, C.; Barnard, K. Health Technology Assessment Process for Oncology Drugs: Impact of CADTH Changes on Public Payer Reimbursement Recommendations. Curr. Oncol. 2022, 29, 1514–1526. [Google Scholar] [CrossRef]
- Oudard, S.; Fizazi, K.; Sengeløv, L.; Daugaard, G.; Saad, F.; Hansen, S.; Hjälm-Eriksson, M.; Jassem, J.; Thiery-Vuillemin, A.; Caffo, O.; et al. Cabazitaxel Versus Docetaxel as First-Line Therapy for Patients with Metastatic Castration-Resistant Prostate Cancer: A Randomized Phase III Trial—FIRSTANA. J. Clin. Oncol. 2017, 35, 3189–3197. [Google Scholar] [CrossRef]
- Gravis, G.; Fizazi, K.; Joly, F.; Oudard, S.; Priou, F.; Esterni, B.; Latorzeff, I.; Delva, R.; Krakowski, I.; Laguerre, B.; et al. Androgen-deprivation therapy alone or with docetaxel in non-castrate metastatic prostate cancer (GETUG-AFU 15): A randomised, open-label, phase 3 trial. Lancet Oncol. 2013, 14, 149–158. [Google Scholar] [CrossRef]
- Merseburger, A.S.; Attard, G.; Åström, L.; Matveev, V.B.; Bracarda, S.; Esen, A.; Feyerabend, S.; Senkus, E.; López-Brea Piqueras, M.; Boysen, G.; et al. Continuous enzalutamide after progression of metastatic castration-resistant prostate cancer treated with docetaxel (PRESIDE): An international, randomised, phase 3b study. Lancet Oncol. 2022, 23, 1398–1408. [Google Scholar] [CrossRef]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Evans, C.P.; Kim, C.-S.; Kimura, G.; et al. Enzalutamide in men with chemotherapy-naïve metastatic castration-resistant prostate cancer: Extended analysis of the phase 3 PREVAIL study. Eur. Urol. 2017, 71, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Eisenberger, M.; Hardy-Bessard, A.C.; Kim, C.S.; Géczi, L.; Ford, D.; Mourey, L.; Carles, J.; Parente, P.; Font, A.; Kacso, G.; et al. Phase III study comparing a reduced dose of cabazitaxel (20 mg/m2) and the currently approved dose (25 mg/m2) in postdocetaxel patients with metastatic castration-resistant prostate cancer-PROSELICA. J. Clin. Oncol. 2017, 35, 3198–3206. [Google Scholar] [CrossRef]
- Attard, G.; Murphy, L.; Clarke, N.W.; Cross, W.; Jones, R.J.; Parker, C.C.; Gillessen, S.; Cook, A.; Brawley, C.; Amos, C.L.; et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet 2022, 399, 447–460. [Google Scholar] [CrossRef]
- De Bono, J.S.; Oudard, S.; Ozguroglu, M.; Hansen, S.; Machiels, J.-P.; Kocak, I.; Gravis, G.; Bodrogi, I.; Mackenzie, M.J.; Shen, L.; et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 2010, 376, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada, Health Canada. Patent Register-Drug Products. 2024. Available online: https://www.canada.ca (accessed on 10 February 2025).
- Guyot, P.; Ades, A.; Ouwens, M.J.; Welton, N.J. Enhanced secondary analysis of survival data: Re- constructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Qiu, T.; Aballéa, S.; Pochopień, M.; Toumi, M.; Dussart, C.; Yan, D. A systematic review on the appropriate discounting rates for the economic evaluation of gene therapies: Whether a specific approach is justified to tackle the challenges? Int. J. Technol. Assess. Health Care 2024, 40, e23. [Google Scholar] [CrossRef]
- Majer, I.; Kroep, S.; Maroun, R.; Williams, C.; Klijn, S.; Palmer, S. Estimating and Extrapolating Survival Using a State-Transition Modeling Approach: A Practical Application in Multiple Myeloma. Value Health 2022, 25, 595–604. [Google Scholar] [CrossRef]
- Pahuta, M.A.; Werier, J.; Wai, E.K.; Patchell, R.A.; Coyle, D. A technique for approximating transition rates from published survival analyses. Cost Eff. Resour. Alloc. 2019, 17, 12. [Google Scholar] [CrossRef]
- Jansen, J.P.; Incerti, D.; Trikalinos, T.A. Multi-state network meta-analysis of progression and survival data. Stat. Med. 2023, 42, 3371–3391. [Google Scholar] [CrossRef]
- Li, S.; Litvin, V.; Manski, C.F. Partial Identification of Personalized Treatment Response with Trial-reported Analyses of Binary Subgroups. Epidemiology 2023, 34, 319. [Google Scholar] [CrossRef]
- Spackman, E.; Weaver, C.; Danthurebandara, V.; Faria, R.; Soares, M. Estimating Markov State Transition Probabilities from Published Kaplan-Meier Survival Curves. Available online: https://www.cda-amc.ca/sites/default/files/symp-2018/presentations/april16-2018/Concurrent-Session-B8-Eldon-Spackman.pdf (accessed on 8 March 2025).
- Krahn, M.D.; Bremner, K.E.; Tomlinson, G.; Naglie, G. Utility and health-related quality of life in prostate cancer patients 12 months after radical prostatectomy or radiation therapy. Prostate Cancer Prostatic Dis. 2009, 12, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, A.J.; Kerr, C.; Penton, J.; Knerer, G. Health-Related Quality of Life and Health Utilities in Metastatic Castrate-Resistant Prostate Cancer: A Survey Capturing Experiences from a Diverse Sample of UK Patients. Value Health 2015, 18, 1152–1157. [Google Scholar] [CrossRef]
- Kretschmer, A.; van den Bergh, R.C.N.; Martini, A.; Marra, G.; Valerio, M.; Tsaur, I.; Heidegger, I.; Kasivisvanathan, V.; Kesch, C.; Preisser, F.; et al. Assessment of Health-Related Quality of Life in Patients with Advanced Prostate Cancer—Current State and Future Perspectives. Cancers 2022, 14, 147. [Google Scholar] [CrossRef]
- Torvinen, S.; Färkkilä, N.; Sintonen, H.; Saarto, T.; Roine, R.P.; Taari, K. Health-related quality of life in prostate cancer. Acta Oncol. 2013, 52, 1094–1101. [Google Scholar] [CrossRef] [PubMed]
- Sathianathen, N.J.; Lawrentschuk, N.; Konety, B.; Azad, A.A.; Corcoran, N.M.; Bolton, D.M.; Murphy, D.G. Cost Effectiveness of Systemic Treatment Intensification for Metastatic Hormone-sensitive Prostate Cancer: Is Triplet Therapy Cost Effective? Eur. Urol. Oncol. 2024, 7, 870–876. [Google Scholar] [CrossRef]
- Baciarello, G.; Delva, R.; Gravis, G.; Tazi, Y.; Beuzeboc, P.; Gross-Goupil, M.; Bompas, E.; Joly, F.; Greilsamer, C.; Hon, T.N.T.; et al. Patient Preference Between Cabazitaxel and Docetaxel for First-line Chemotherapy in Metastatic Castration-resistant Prostate Cancer: The CABADOC Trial. Eur. Urol. 2022, 81, 234–240. [Google Scholar] [CrossRef]
- Beca, J.; Majeed, H.; Chan, K.K.W.; Hotte, S.J.; Loblaw, A.; Hoch, J.S. Cost-effectiveness of docetaxel in high-volume hormone-sensitive metastatic prostate cancer. Can. Urol. Assoc. J. 2019, 13, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Régie de l’Assurance Maladie du Québec (RAMQ). List of Medications, 14 August 2024. Available online: www.ramq.gouv.qc.ca/en/about-us/list-medications (accessed on 10 February 2025).
- Jiang, D.M.; Fallah-Rad, N.; Lee, R.; Ng, P.; Smith, A.D.; Hansen, A.R.; Joshua, A.M.; Beca, J.; Sridhar, S.S. Significantly minimizing drug wastage and the cost of cabazitaxel used to treat metastatic castration-resistant prostate cancer. Eur. Urol. 2021, 79, 177–179. [Google Scholar] [CrossRef]
- De Oliveira, C.; Pataky, R.; Bremner, K.E.; Rangrej, J.; Chan, K.K.W.; Cheung, W.Y.; Hoch, J.S.; Peacock, S.; Krahn, M.D. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer 2016, 16, 809. [Google Scholar] [CrossRef]
- Tannock, I.F.; de Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Théodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N. Engl. J. Med. 2004, 351, 1502–1512. [Google Scholar] [CrossRef]
- Francini, E.; Gray, K.P.; Xie, W.; Shaw, G.K.; Valença, L.; Bernard, B.; Albiges, L.; Harshman, L.C.; Kantoff, P.W.; Taplin, M.-E.; et al. Time of metastatic disease presentation and volume of disease are prognostic for metastatic hormone sensitive prostate cancer (mHSPC). Prostate 2018, 78, 889–895. [Google Scholar] [CrossRef]
- Paulden, M. Why it’s Time to Abandon the ICER. PharmacoEconomics 2020, 38, 781–784. [Google Scholar] [CrossRef] [PubMed]
- Yoo, M.; Nelson, R.E.; Haaland, B.; Dougherty, M.; Cutshall, Z.A.; Kohli, R.; Beckstead, R.; Kohli, M. Cost-effectiveness analysis of 7 treatments in metastatic hormone-sensitive prostate cancer: A public-payer perspective. J. Natl. Cancer Inst. 2023, 115, 1374–1382. [Google Scholar] [CrossRef] [PubMed]
- Bank of Canada, Annual Exchange Rates. 2024. Available online: https://www.bankofcanada.ca (accessed on 2 April 2025).
- Saad, F.; Chilelli, A.; Hui, B.; Muratov, S.; Ganguli, A.; North, S.; Shayegan, B. Cost-effectiveness of enzalutamide versus apalutamide versus androgen deprivation therapy alone for the treatment of metastatic castration-sensitive prostate cancer in Canada. J. Med. Econ. 2022, 25, 583–590. [Google Scholar] [CrossRef]
- Efstathiou, E.; Wang, X.; Zurita, A.J.; Tu, S.-M.; Aparicio, A.; Wang, J.; Corn, P.G.; Subudhi, S.K.; Araujo, J.C.; Reece, L.K.; et al. A randomized study of finite abiraterone acetate (AA) plus leuprolide (LHRHa) versus LHRHa in biochemically recurrent non metastatic hormone naïve prostate cancer (M0HNPC). J. Clin. Oncol. 2018, 36 (Suppl. 15), 5002. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Freedland, S.J.; George, D.J.; Morgans, A.K. Treatment Intensification with Novel Hormonal Therapy in Castration-Sensitive Prostate Cancer: Patient Identification and Clinical Rationale. Clin. Genitourin. Cancer 2024, 22, 102171. [Google Scholar] [CrossRef]
- Serra-Burriel, M.; Martin-Bassols, N.; Perényi, G.; Vokinger, K.N. Drug Prices After Patent Expirations in High-Income Countries and Implications for Cost-Effectiveness Analyses. JAMA Health Forum. 2024, 5, e242530. [Google Scholar] [CrossRef]
- Vondeling, G.T.; Cao, Q.; Postma, M.J.; Rozenbaum, M.H. The Impact of Patent Expiry on Drug Prices: A Systematic Literature Review. Appl. Health Econ. Health Policy 2018, 16, 653–660. [Google Scholar] [CrossRef]
- Litvin, V.; Aprikian, A.; Dragomir, A. Cost-Effectiveness Analysis of Contemporary Advanced Prostate Cancer Management: A Markov Model for the Canadian Context. In Proceedings of the ISPOR Europe 2024, Barcelona, Spain, 17–20 November 2024. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Trial | Treatments | Health States | Sources |
|---|---|---|---|
| AFFIRM | Enzalutamide post docetaxel | mCRPC | [11] |
| ARAMIS | Darolutamide | nmCRPC | [12] |
| ADT alone | nmCRPC | ||
| ARANOTE | Darolutamide | low-risk mCSPC | [6] |
| high-risk mCSPC | |||
| ARASENS | Darolutamide and docetaxel | low-risk mCSPC | [7] |
| high-risk mCSPC | |||
| COU-AA-301 | Abiraterone post docetaxel | mCRPC | [9] |
| COU-AA-302 | Abiraterone | mCRPC | [10] |
| EMBARK | Enzalutamide (intermittent) | nmCSPC | [2] |
| ADT alone (intermittent) | nmCSPC | ||
| ENZAMET | Enzalutamide | low-risk mCSPC | [8] |
| high-risk mCSPC | |||
| Enzalutamide and docetaxel | low-risk mCSPC | ||
| high-risk mCSPC | |||
| Docetaxel | high-risk mCSPC | ||
| ADT alone | low-risk mCSPC | ||
| high-risk mCSPC | |||
| FIRSTANA | Docetaxel | mCRPC | [19] |
| GETUG-AFU 15 | Docetaxel | high-risk mCSPC | [20] |
| ADT alone | high-risk mCSPC | ||
| PEACE-1 | Abiraterone and docetaxel | low-risk mCSPC | [4] |
| high-risk mCSPC | |||
| Docetaxel | high-risk mCSPC | ||
| PRESIDE | Docetaxel | mCRPC | [21] |
| PREVAIL | Enzalutamide | mCRPC | [22] |
| PROSELICA | Cabazitaxel post docetaxel | mCRPC | [23] |
| PROSPER | Enzalutamide | nmCRPC | [13] |
| ADT alone | nmCRPC | ||
| SPARTAN | Apalutamide | nmCRPC | [14] |
| ADT alone | nmCRPC | ||
| STAMPEDE | Abiraterone | low-risk mCSPC | [5] |
| high-risk mCSPC | |||
| nmCRPC | [24] | ||
| ADT alone | low-risk mCSPC | [5] | |
| high-risk mCSPC | |||
| TITAN | Apalutamide | low-risk mCSPC | [3] |
| high-risk mCSPC | |||
| TROPIC | Cabazitaxel post docetaxel | mCRPC | [25] |
| Health State | State-Specific Utility (Annual) | Sources |
|---|---|---|
| nmCSPC | 0.95 | [34] |
| mCSPC (low- and high-risk) | 0.85 | [35] |
| nmCRPC | 0.9 | [35,36,37] |
| mCRPC | 0.75 | [37] |
| Progressed mCRPC | 0.6 | [37] |
| Treatment | Treatment-Specific Disutility (Annual) | Sources |
| Abiraterone | −0.021 | [38] |
| Apalutamide | −0.019 | [38] |
| Cabazitaxel | −0.042 | [19,38,39] |
| Darolutamide | −0.019 | [38] |
| Docetaxel | −0.042 | [38] |
| Enzalutamide | −0.022 | [38] |
| Treatment | Cost (CAD, Monthly) | Sources |
| ADT | 322 | [40,41] |
| Abiraterone | 919 | [41] |
| Apalutamide | 3401 | [41] |
| Cabazitaxel | 4134 | [42] |
| Darolutamide | 3401 | [41] |
| Docetaxel | 103 | [40] |
| Enzalutamide | 3401 | [41] |
| Non-IV management | 92 | [40] |
| IV management | 455 | [40] |
| End-of-life | 1449 | [43] |
| Measure | Starting Health State | Rank | Incremental Benefit | Total Benefit | Treatment Sequence (nmCSPC, nmCRPC/mCSPC, mCRPC) * or (mCSPC, mCRPC) † | ARPI Use |
|---|---|---|---|---|---|---|
| QALYs | nmCSPC | 1 | 3.29 QALYs | 10.87 QALYs | (enza, adt, doce) * | early |
| 2 | 3.18 QALYs | 10.75 QALYs | (enza, adt, doce then caba) * | early | ||
| 3 | 1.99 QALYs | 9.57 QALYs | (adt, abi, doce) * | late | ||
| low-risk mCSPC | 1 | 2.23 QALYs | 7.34 QALYs | (enza, doce) † | early | |
| 2 | 2.02 QALYs | 7.13 QALYs | (abi, doce) † | early | ||
| 3 | 1.93 QALYs | 7.03 QALYs | (enza, doce then caba) † | early | ||
| high-risk mCSPC | 1 | 3.02 QALYs | 6.44 QALYs | (apa, doce) † | early | |
| 2 | 2.71 QALYs | 6.13 QALYs | (apa, doce then caba) † | early | ||
| 3 | 2.22 QALYs | 5.64 QALYs | (doce + daro, doce) † | early | ||
| LYs | nmCSPC | 1 | 3.03 LYs | 11.82 LYs | (enza, adt, doce) * | early |
| 2 | 2.82 LYs | 11.62 LYs | (enza, adt, doce then caba) * | early | ||
| 2 | 2.06 LYs | 10.86 LYs | (adt, abi, doce) * | late | ||
| low-risk mCSPC | 1 | 2.65 LYs | 9.30 LYs | (enza, doce) † | early | |
| 2 | 2.37 LYs | 9.02 LYs | (abi, doce) † | early | ||
| 3 | 2.11 LYs | 8.77 LYs | (enza, doce then caba) † | early | ||
| high-risk mCSPC | 1 | 3.57 LYs | 8.18 LYs | (apa, doce) † | early | |
| 2 | 3.02 LYs | 7.63 LYs | (apa, doce then caba) † | early | ||
| 3 | 2.74 LYs | 7.35 LYs | (doce + daro, doce) † | early |
| Starting Health State | Cost Effectiveness Threshold | Rank | Incremental NHB (QALY) | Total NHB (QALY) | Total Benefit (QALY) | Total Cost (CAD) | Treatment Sequence (nmCSPC, nmCRPC/mCSPC, mCRPC) * or (mCSPC, mCRPC) † | ARPI Use |
|---|---|---|---|---|---|---|---|---|
| nmCSPC | CAD 50K per QALY | 1 | 0.68 | 7.65 | 9.57 | 95,780 | (adt, abi, doce) * | late |
| 2 | 0.45 | 7.41 | 10.87 | 172,579 | (enza, adt, doce) * | early | ||
| 3 | 0.26 | 7.22 | 9.41 | 109,546 | (adt, abi, doce then caba) * | late | ||
| CAD 100K per QALY | 1 | 1.87 | 9.14 | 10.87 | 172,579 | (enza, adt, doce) * | early | |
| 2 | 1.66 | 8.93 | 10.75 | 181,883 | (enza, adt, doce then caba) * | early | ||
| 3 | 1.34 | 8.61 | 9.57 | 95,780 | (adt, abi, doce) * | late | ||
| low-risk mCSPC | CAD 50K per QALY | 1 | 0.15 | 4.59 | 7.13 | 126,870 | (abi, doce) † | early |
| 2 | 0 | 4.44 | 5.11 | 33,505 | (adt, doce) † | none | ||
| 3 | 0.00 | 4.44 | 5.58 | 57,168 | (adt, abi) † | late | ||
| CAD 100K per QALY | 1 | 1.09 | 5.86 | 7.13 | 126,870 | (abi, doce) † | early | |
| 2 | 0.58 | 5.35 | 6.84 | 148,756 | (abi, doce then caba) † | early | ||
| 3 | 0.24 | 5.01 | 5.58 | 57,168 | (adt, abi) † | late | ||
| high-risk mCSPC | CAD 50K per QALY | 1 | 0.65 | 3.60 | 5.45 | 92,454 | (abi, doce) † | early |
| 2 | 0.06 | 3.01 | 4.52 | 75,713 | (doce + abi, doce) † | early | ||
| 3 | 0.00 | 2.96 | 3.85 | 44,807 | (adt, abi) † | late | ||
| CAD 100K per QALY | 1 | 1.34 | 4.52 | 5.45 | 92,454 | (abi, doce) † | early | |
| 2 | 0.89 | 4.08 | 5.64 | 156,020 | (doce + daro doce) † | early | ||
| 3 | 0.71 | 3.89 | 5.06 | 117,143 | (abi, doce then caba) † | early | ||
| Starting Health State | Cost Effectiveness Threshold | Rank | Incremental NHB (LY) | Total NHB (LY) | Total Benefit (LY) | Total Cost (CAD) | Treatment Sequence (nmCSPC, nmCRPC/mCSPC, mCRPC) * or (mCSPC, mCRPC) † | ARPI Use |
| nmCSPC | CAD 50K per LY | 1 | 0.76 | 8.95 | 10.86 | 95,780 | (adt, abi, doce) * | late |
| 2 | 0.21 | 8.40 | 10.59 | 109,546 | (adt, abi, doce then caba) * | late | ||
| 3 | 0.18 | 8.37 | 11.82 | 172,579 | (enza, adt, doce) * | early | ||
| CAD 100K per LY | 1 | 1.60 | 10.10 | 11.82 | 172,579 | (enza, adt, doce) * | early | |
| 2 | 1.41 | 9.90 | 10.86 | 95,780 | (adt, abi, doce) * | late | ||
| 3 | 1.31 | 9.80 | 11.62 | 181,883 | (enza, adt, doce then caba) * | early | ||
| low-risk mCSPC | CAD 50K per LY | 1 | 0.50 | 6.48 | 9.02 | 126,870 | (abi, doce) † | early |
| 2 | 0.04 | 6.02 | 7.16 | 57,168 | (adt, abi) † | late | ||
| 3 | 0 | 5.98 | 6.65 | 33,505 | (adt, doce) † | none | ||
| CAD 100K per LY | 1 | 1.43 | 7.75 | 9.02 | 126,870 | (abi, doce) † | early | |
| 2 | 0.70 | 7.02 | 8.51 | 148,756 | (abi, doce then caba) † | early | ||
| 3 | 0.27 | 6.59 | 7.16 | 57,168 | (adt, abi) † | late | ||
| high-risk mCSPC | CAD 50K per LY | 1 | 1.10 | 5.24 | 7.09 | 92,454 | (abi, doce) † | early |
| 2 | 0.39 | 4.54 | 6.05 | 75,713 | (doce + abi, doce) † | early | ||
| 3 | 0.08 | 4.23 | 7.35 | 156,020 | (doce + daro, doce) † | early | ||
| CAD 100K per LY | 1 | 1.79 | 6.16 | 7.09 | 92,454 | (abi, doce) † | early | |
| 2 | 1.41 | 5.79 | 7.35 | 156,020 | (doce + daro, doce) † | early | ||
| 3 | 0.92 | 5.29 | 6.05 | 75,713 | (doce + abi, doce) † | early |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Litvin, V.; Aprikian, A.G.; Dragomir, A. Cost-Effectiveness Analysis of Contemporary Advanced Prostate Cancer Treatment Sequences. Curr. Oncol. 2025, 32, 240. https://doi.org/10.3390/curroncol32040240
Litvin V, Aprikian AG, Dragomir A. Cost-Effectiveness Analysis of Contemporary Advanced Prostate Cancer Treatment Sequences. Current Oncology. 2025; 32(4):240. https://doi.org/10.3390/curroncol32040240
Chicago/Turabian StyleLitvin, Valentyn, Armen G. Aprikian, and Alice Dragomir. 2025. "Cost-Effectiveness Analysis of Contemporary Advanced Prostate Cancer Treatment Sequences" Current Oncology 32, no. 4: 240. https://doi.org/10.3390/curroncol32040240
APA StyleLitvin, V., Aprikian, A. G., & Dragomir, A. (2025). Cost-Effectiveness Analysis of Contemporary Advanced Prostate Cancer Treatment Sequences. Current Oncology, 32(4), 240. https://doi.org/10.3390/curroncol32040240