A Systematic Review of SBRT Boost for Cervical Cancer Patients Who Cannot Benefit from Brachytherapy



Abstract

1. Introduction
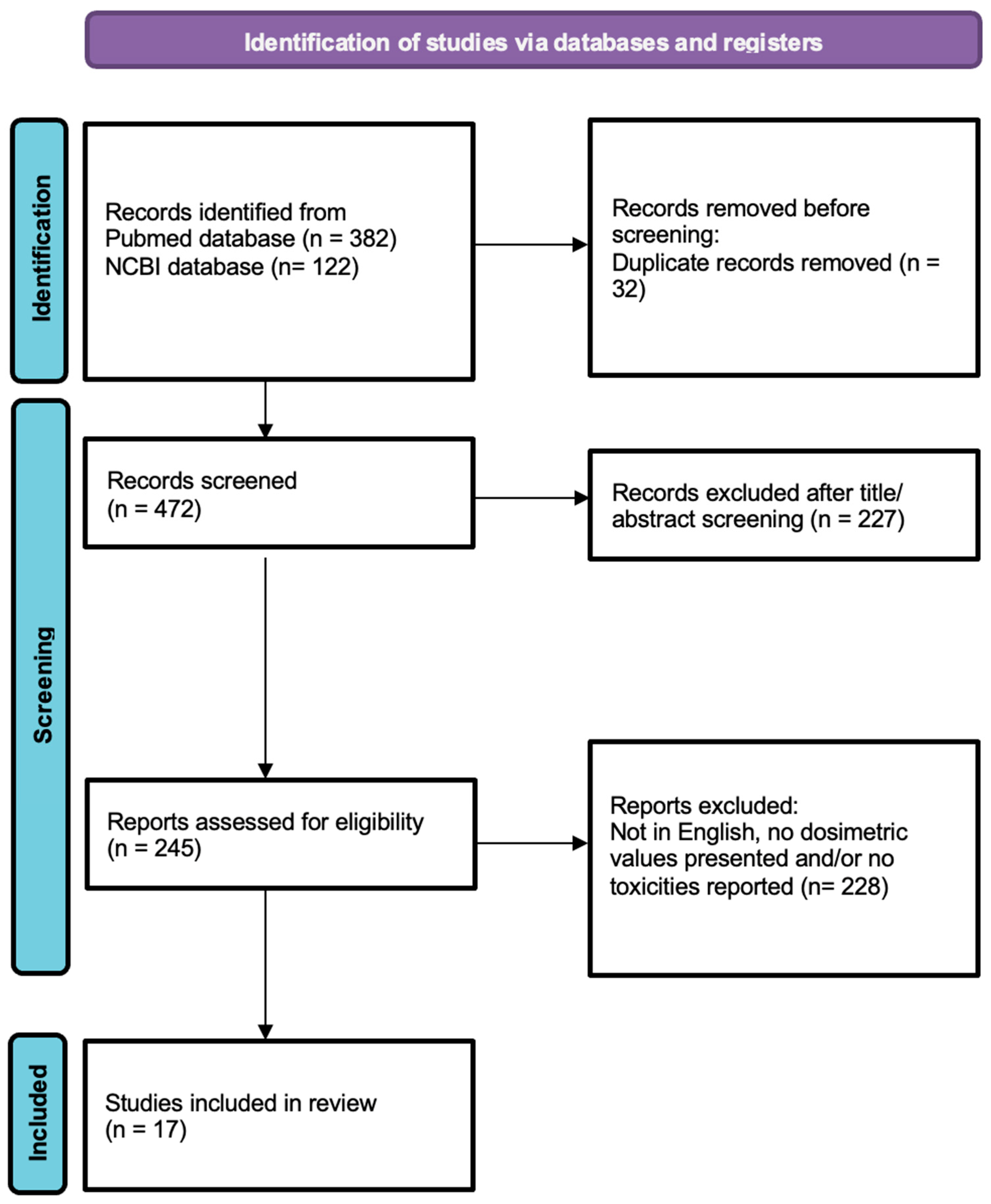
2. Materials and Methods
3. Results
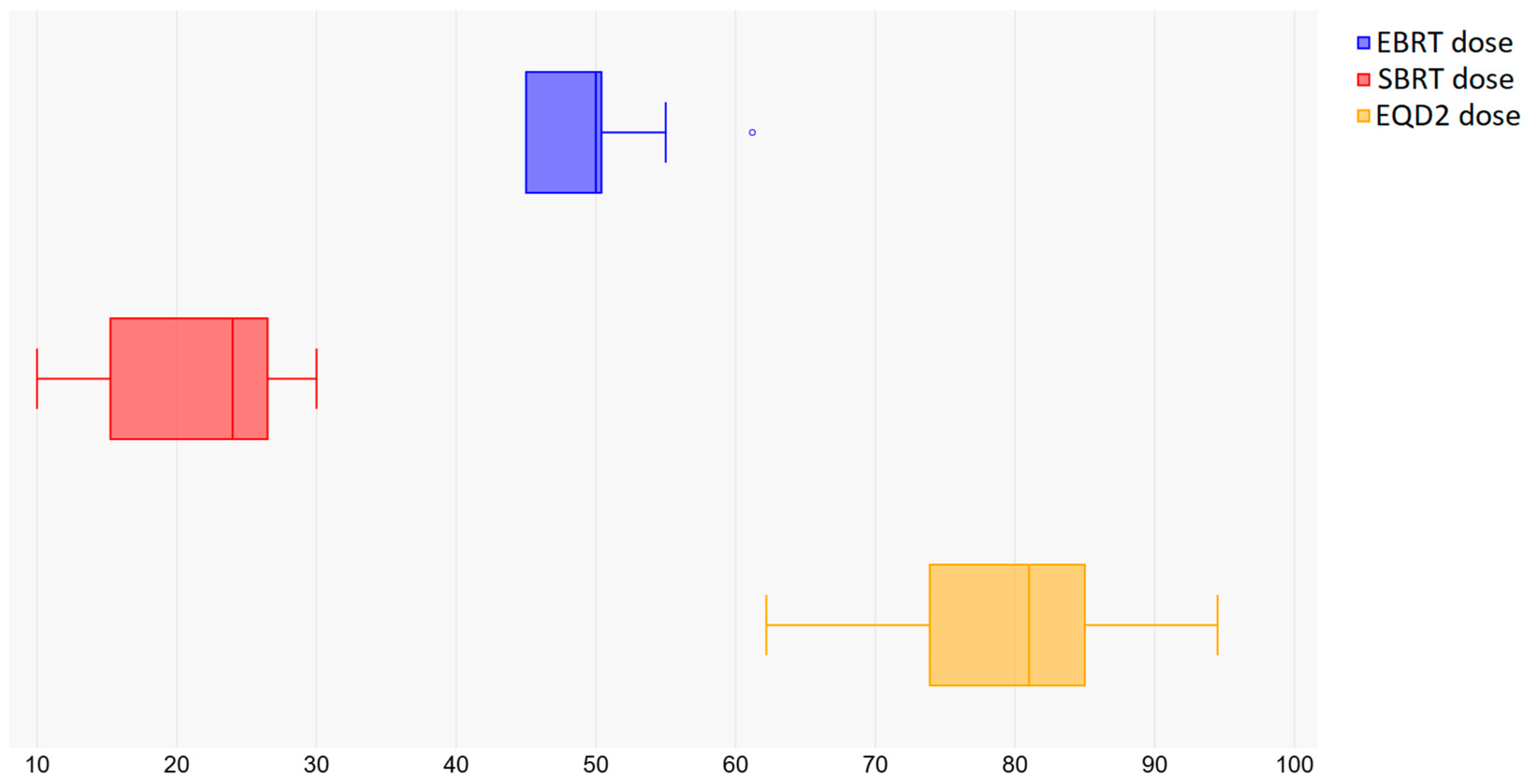
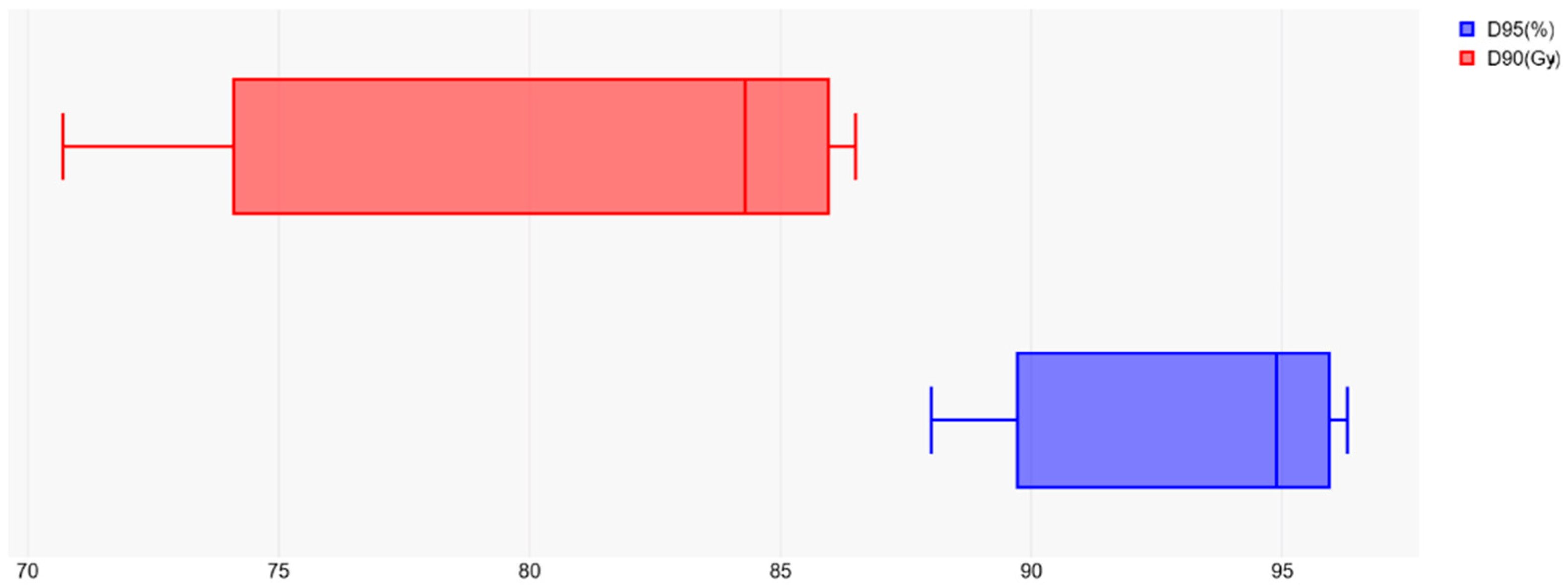
3.1. Prescribed Dose and Fractionation: Tumor Volume Dosimetry
3.2. Organ at Risk Dosimetry
4. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Number of Patients/Staging | EBRT Dose/Boost Dose Gy (Fr) | EQD2 α/β = 10/ EQD2 α/β = 3 (Gy) | Median Follow-Up (Months) | Overall Survival | Local Control | Toxicities |
|---|---|---|---|---|---|---|---|
| Kang et al. [49] | 97 IB–IVB | 45–50.4 (25–28)/25–30 (5–6) | 75.5–87.1/83.2–96.1 | 50 | Progression-free survival: 80% at 3 years | 93% at 3 years | 2 patients with late rectal bleeding |
| Castelnaud-Marchand et al. [50] | 225 IB1–IVA | 44–50.4 (25–28)/15 (3) | 62.8–68.3/ 68–72.4 | 38.8 | OS: 76.1% at 3 years | 86.4% at 3 years | 18 late genitourinary and gastrointestinal toxicities in 14 patients |
| Simpson et al. [51] | 76 IB1–IVA | 43.2–50.4 (24–28)/25–30 (3–5) | 78.5–89.6/94.3–102.4 | 17 | OS: 75% at 2 years | 94.2% at 2 years | 2 patients with intractable nausea and vomiting |
| Charra–Brunaud et al. [52] | 117 IB1–IVA | 45 (25)/10–20 (2–4) | 56.8–69.3/59.2–75.2 | 24.3 | OS: 74% at 2 years | 78.5% at 2 years | 1.2% of patients with genitourinary and gastrointestinal toxicities |
| Pötter et al. [47] | 156 IB1–IVA | 45–50.4 (25–28)/ 28 (4) | 83.9–89.2/99.2–104.4 | 42 | OS: 68% at 3 years | 95% at 3 years | 3 patients with genitourinary and 5 patients with gastrointestinal toxicities |
| Tan et al. [53] | 28 IB1–IIIB | 45 (25)/21 (3) | 74/85.2 | 23 | N/A | 93% at 3 years | 2 patients with rectal bleeding |
5. Conclusions
6. Future Directions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| WHO | World Health Organization |
| WCRF | World Cancer Research Fund |
| SBRT | Stereotactic body radiation therapy |
| SABR | Stereotactic ablative radiotherapy |
| HIV | Human immunodeficiency viruses |
| EQD2 | Equivalent dose in 2 Gy fractions |
| EBRT | External beam radiotherapy |
| Fr | Fraction |
| D95 | The dose received by 95% of the tumor volume |
| D90 | The dose received by 90% of the tumor volume |
| D2cc | Minimum dose to the most irradiated contiguous volume of 2cc |
| D1cc | Minimum dose to the most irradiated contiguous volume of 1cc |
| OS | Overall survival |
| 3D-CRT | Three-dimensional conformal radiation therapy |
References
- World Health Organization. Cervical Cancer. Available online: www.who.int/news-room/fact-sheets/detail/cervical-cancer (accessed on 25 November 2024).
- World Cancer Research Fund. Cervical Cancer Statistics, 15 November 2024. Available online: www.wcrf.org/preventing-cancer/cancer-statistics/cervical-cancer-statistics/#:~:text=Related%20content-,Latest%20cervical%20cancer%20data,ASR%20%3D%20age%2Dstandardised%20rates (accessed on 12 January 2024).
- Skowronek, J. Current status of brachytherapy in cancer treatment—Short overview. J. Contemp. Brachytherapy 2017, 9, 581–589. [Google Scholar] [CrossRef]
- Barraclough, L.H.; Swindell, R.; Livsey, J.E.; Hunter, R.D.; Davidson, S.E. External Beam Boost for Cancer of the Cervix Uteri When Intracavitary Therapy Cannot Be Performed. Int. J. Radiat. Oncol. 2008, 71, 772–778. [Google Scholar] [CrossRef]
- Logsdon, M.D.; Eifel, P.J. FIGO IIIB squamous cell carcinoma of the cervix: An analysis of prognostic factors emphasizing the balance between external beam and intracavitary radiation therapy. Int. J. Radiat. Oncol. 1999, 43, 763–775. [Google Scholar] [CrossRef] [PubMed]
- Mollà, M.; Escude, L.; Nouet, P.; Popowski, Y.; Hidalgo, A.; Rouzaud, M.; Linero, D.; Miralbell, R. Fractionated stereotactic radiotherapy boost for gynecologic tumors: An alternative to brachytherapy? Int. J. Radiat. Oncol. 2005, 62, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Higginson, D.S.; Morris, D.E.; Jones, E.L.; Clarke-Pearson, D.; Varia, M.A. Stereotactic body radiotherapy (SBRT): Technological innovation and application in gynecologic oncology. Gynecol. Oncol. 2011, 120, 404–412. [Google Scholar] [CrossRef]
- Seo, Y.S.; Kim, M.; Yoo, S.Y.; Cho, C.K.; Choi, C.W.; Kim, J.H.; Han, C.J.; Park, S.C.; Lee, B.H.; Kim, Y.H.; et al. Preliminary result of stereotactic body radiotherapy as a local salvage treatment for inoperable hepatocellular carcinoma. J. Surg. Oncol. 2010, 102, 209–214. [Google Scholar] [CrossRef]
- King, C.R.; Brooks, J.D.; Gill, H.; Pawlicki, T.; Cotrutz, C.; Presti, J.C., Jr. Stereotactic body radiotherapy for localized prostate cancer: Interim results of a prospective phase II clinical trial. Int. J. Radiat. Oncol. 2009, 73, 1043–1048. [Google Scholar] [CrossRef]
- Timmerman, R.; Paulus, R.; Galvin, J.; Michalski, J.; Straube, W.; Bradley, J.; Fakiris, A.; Bezjak, A.; Videtic, G.; Johnstone, D.; et al. Stereotactic Body Radiation Therapy for Inoperable Early Stage Lung Cancer. JAMA 2010, 303, 1070–1076. [Google Scholar] [CrossRef]
- Svedman, C.; Sandström, P.; Pisa, P.; Blomgren, H.; Lax, I.; Kälkner, K.-M.; Nilsson, S.; Wersäll, P. A prospective Phase II trial of using extracranial stereotactic radiotherapy in primary and metastatic renal cell carcinoma. Acta Oncol. 2006, 45, 870–875. [Google Scholar] [CrossRef] [PubMed]
- Lo, S.S.; Fakiris, A.J.; Chang, E.L.; Mayr, N.A.; Wang, J.Z.; Papiez, L.; Teh, B.S.; McGarry, R.C.; Cardenes, H.R.; Timmerman, R.D. Stereotactic body radiation therapy: A novel treatment modality. Nat. Rev. Clin. Oncol. 2009, 7, 44–54. [Google Scholar] [CrossRef]
- Kubicek, G.J.; Xue, J.; Xu, Q.; Asbell, S.O.; Hughes, L.; Kramer, N.; Youssef, A.; Chen, Y.; Aikens, J.; Saul, H.; et al. Stereotactic Body Radiotherapy as an Alternative to Brachytherapy in Gynecologic Cancer. BioMed. Res. Int. 2013, 2013, 898953. [Google Scholar] [CrossRef]
- Facondo, G.; Vullo, G.; DE Sanctis, V.; Valeriani, M.; Ascolese, A.M.; Massaro, M.; Anzellini, D.; Osti, M.F. Stereotactic Body Radiation Therapy Boost in Patients With Cervical Cancer Ineligible for Brachytherapy. Cancer Diagn. Progn. 2021, 1, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Pontoriero, A.; Iatì, G.; Aiello, D.; Pergolizzi, S. Stereotactic Radiotherapy in the Retreatment of Recurrent Cervical Cancers, Assessment of Toxicity, and Treatment Response. Technol. Cancer Res. Treat. 2016, 15, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Turna, M.; Rzazade, R.; Küçükmorkoç, E.; Küçük, N.; Canoğlu, M.D.; Çağlar, H.B. Dose escalation with stereotactic body radiotherapy for cervical cancer treatment. BMC Cancer 2024, 24, 1281. [Google Scholar] [CrossRef]
- Haas, J.A.; Witten, M.R.; Clancey, O.; Episcopia, K.; Accordino, D.; Chalas, E. CyberKnife Boost for Patients with Cervical Cancer Unable to Undergo Brachytherapy. Front. Oncol. 2012, 2, 19296. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.-H.; Tien, H.-J.; Hsiao, S.-M.; Wei, M.-C.; Wu, W.-Y.; Sun, H.-D.; Wang, L.-Y.; Hsieh; Chen, Y.-J.; Shueng, P.-W.; et al. Stereotactic body radiation therapy via helical tomotherapy to replace brachytherapy for brachytherapy-unsuitable cervical cancer patients—A preliminary result. OncoTargets Ther. 2013, 6, 59–66. [Google Scholar] [CrossRef]
- Cheng, H.-Y.; Liang, J.-A.; Hung, Y.-C.; Yeh, L.-S.; Chang, W.-C.; Lin, W.-C.; Chen, S.-W. Stereotactic body radiotherapy for pelvic boost in gynecological cancer patients with local recurrence or unsuitable for intracavitary brachytherapy. Taiwan. J. Obstet. Gynecol. 2021, 60, 111–118. [Google Scholar] [CrossRef]
- Guckenberger, M.; Bachmann, J.; Wulf, J.; Mueller, G.; Krieger, T.; Baier, K.; Richter, A.; Wilbert, J.; Flentje, M. Stereotactic body radiotherapy for local boost irradiation in unfavourable locally recurrent gynaecological cancer. Radiother. Oncol. 2010, 94, 53–59. [Google Scholar] [CrossRef]
- Lee, T.H.; Song, C.; Kim, I.A.; Kim, J.-S.; Kim, Y.B.; Kim, K.; No, J.H.; Suh, D.H.; Chung, J.-B.; Eom, K.-Y. Stereotactic ablative body radiotherapy boost for cervical cancer when brachytherapy boost is not feasible. Radiat. Oncol. 2021, 16, 148. [Google Scholar] [CrossRef]
- Marnitz, S.; Köhler, C.; Budach, V.; Neumann, O.; Kluge, A.; Wlodarczyk, W.; Jahn, U.; Gebauer, B.; Kufeld, M. Brachytherapy-emulating robotic radiosurgery in patients with cervical carcinoma. Radiat. Oncol. 2013, 8, 109. [Google Scholar] [CrossRef]
- Albuquerque, K.; Tumati, V.; Lea, J.; Ahn, C.; Richardson, D.; Miller, D.; Timmerman, R. A Phase II Trial of Stereotactic Ablative Radiation Therapy as a Boost for Locally Advanced Cervical Cancer. Int. J. Radiat. Oncol. 2019, 106, 464–471. [Google Scholar] [CrossRef]
- Jorcano, S.; Mollà, M.; Escudé, L.; Sanz, S.; Hidalgo, A.; Toscas, J.I.; Linero, D.; Miralbell, R. Hypofractionated Extracranial Stereotactic Radiotherapy Boost for Gynecologic Tumors: A Promising Alternative to High-Dose Rate Brachytherapy. Technol. Cancer Res. Treat. 2010, 9, 509–514. [Google Scholar] [CrossRef]
- Dalwadi, S.; Echeverria, A.; Jhaveri, P.; Bui, T.; Waheed, N.; Tran, D.; Bonnen, M.; Ludwig, M. Non-invasive stereotactic ablative boost in patients with locally advanced cervical cancer. Int. J. Gynecol. Cancer 2020, 30, 1684–1688. [Google Scholar] [CrossRef] [PubMed]
- Hadi, I.; Eze, C.; Schönecker, S.; von Bestenbostel, R.; Rogowski, P.; Nierer, L.; Bodensohn, R.; Reiner, M.; Landry, G.; Belka, C.; et al. MR-guided SBRT boost for patients with locally advanced or recurrent gynecological cancers ineligible for brachytherapy: Feasibility and early clinical experience. Radiat. Oncol. 2022, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- Kemmerer, E.; Hernandez, E.; Ferriss, J.S.; Valakh, V.; Miyamoto, C.; Li, S.; Micaily, B. Use of Image-Guided Stereotactic Body Radiation Therapy in Lieu of Intracavitary Brachytherapy for the Treatment of Inoperable Endometrial Neoplasia. Int. J. Radiat. Oncol. 2012, 85, 129–135. [Google Scholar] [CrossRef]
- Lazzari, R.; Riva, G.; Augugliaro, M.; Vavassori, A.; Dicuonzo, S.; Cattani, F.; Comi, S.; Colombo, N.; Jereczek-Fossa, B.A. Intensity modulated radiation therapy boost in locally-advanced cervical cancer in the absence of brachytherapy. Int. J. Gynecol. Cancer 2020, 30, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, M.; Dogan, A.; Ozyigit, G.; Erturk, E.; Yildiz, F.; Selek, U.; Ulger, S.; Colak, F.; Zorlu, F. Comparison of intracavitary brachytherapy and stereotactic body radiotherapy dose distribution for cervical cancer. Brachytherapy 2011, 11, 125–129. [Google Scholar] [CrossRef]
- Dahbi, Z.; Fadila, K.; Vinh-Hung, V. Brachytherapy Versus Stereotactic Body Radiotherapy for Cervical Cancer Boost: A Dosimetric Comparison. Cureus 2023, 15, e37235. [Google Scholar] [CrossRef]
- Ito, K.; Nakajima, Y.; Ogawa, H.; Furusawa, A.; Murofushi, K.N.; Kito, S.; Kino, N.; Yasugi, T.; Uno, T.; Karasawa, K. Phase I/II study of stereotactic body radiotherapy boost in patients with cervical cancer ineligible for intracavitary brachytherapy. Jpn. J. Radiol. 2024, 42, 909–917. [Google Scholar] [CrossRef]
- Gill, B.S.; Lin, J.F.; Krivak, T.C.; Sukumvanich, P.; Laskey, R.A.; Ross, M.S.; Lesnock, J.L.; Beriwal, S. National Cancer Data Base Analysis of Radiation Therapy Consolidation Modality for Cervical Cancer: The Impact of New Technological Advancements. Int. J. Radiat. Oncol. 2014, 90, 1083–1090. [Google Scholar] [CrossRef]
- O’donnell, B.; Shiao, J.C.; Pezzi, T.A.; Waheed, N.; Sharma, S.; Bonnen, M.D.; Ludwig, M.S. Stereotactic Body Radiation Therapy, Intensity-Modulated Radiation Therapy, and Brachytherapy Boost Modalities in Invasive Cervical Cancer. Int. J. Gynecol. Cancer 2018, 28, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Major, T.; Fröhlich, G.; Ágoston, P.; Polgár, C.; Takácsi-Nagy, Z. The value of brachytherapy in the age of advanced external beam radiotherapy: A review of the literature in terms of dosimetry. Strahlenther. Onkol. 2021, 198, 93–109. [Google Scholar] [CrossRef]
- Ito, K.; Kito, S.; Nakajima, Y.; Shimizuguchi, T.; Ogawa, H.; Nihei, K.; Tanaka, H.; Kino, N.; Yasugi, T.; Karasawa, K. Determining the recommended dose of stereotactic body radiotherapy boost in patients with cervical cancer who are unsuitable for intracavitary brachytherapy: A phase I dose-escalation study. Ultrasound Med. Biol. 2019, 49, 856–861. [Google Scholar] [CrossRef]
- Chan, P.; Yeo, I.; Perkins, G.; Fyles, A.; Milosevic, M. Dosimetric comparison of intensity-modulated, conformal, and four-field pelvic radiotherapy boost plans for gynecologic cancer: A retrospective planning study. Radiat. Oncol. 2006, 1, 13. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, K.; Tanimoto, H.; Fujita, K.; Hashimoto, Y.; Murakami, Y.; Kenjo, M.; Kaneyasu, Y.; Wadasaki, K.; Ito, K. Early clinical outcomes of 3D-conformal radiotherapy using accelerated hyperfractionation without intracavitary brachytherapy for cervical cancer. Gynecol. Oncol. 2007, 104, 11–14. [Google Scholar] [CrossRef]
- Ito, H.; Kutuki, S.; Nishiguchi, I.; Shigematsu, N.; Kuribayashi, T.; Uematsu, M.; Nakayama, T.; Ka, W.-J.; Takemasa, K.; Ando, Y.; et al. Radiotherapy for cervical cancer with high-dose rate brachytherapy—Correlation between tumor size, dose and failure. Radiother. Oncol. 1994, 31, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Petereit, D.G.; Sarkaria, J.N.; Potter, D.M.; Schink, J.C. High-dose-rate versus low-dose-rate brachytherapy in the treatment of cervical cancer: Analysis of tumor recurrence—The University of Wisconsin experience. Int. J. Radiat. Oncol. 1999, 45, 1267–1274. [Google Scholar] [CrossRef]
- Toita, T.; Kakinohana, Y.; Ogawa, K.; Adachi, G.; Moromizato, H.; Nagai, Y.; Maehama, T.; Sakumoto, K.; Kanazawa, K.; Murayama, S. Combination external beam radiotherapy and high-dose-rate intracavitary brachytherapy for uterine cervical cancer: Analysis of dose and fractionation schedule. Int. J. Radiat. Oncol. 2003, 56, 1344–1353. [Google Scholar] [CrossRef]
- Pourquier, H.; Dubois, J.B.; Delard, R. Cancer of the uterine cervix: Dosimetric guidelines for prevention of late rectal and rectosigmoid complications as a result of radiotherapeutic treatment. Int. J. Radiat. Oncol. 1982, 8, 1887–1895. [Google Scholar] [CrossRef]
- Cheng, J.C.-H.; Peng, L.-C.; Chen, Y.-H.; Huang, D.Y.; Wu, J.-K.; Jian, J.J.-M. Unique role of proximal rectal dose in late rectal complications for patients with cervical cancer undergoing high-dose-rate intracavitary brachytherapy. Int. J. Radiat. Oncol. 2003, 57, 1010–1018. [Google Scholar] [CrossRef]
- Park, H.J.; Chang, A.R.; Seo, Y.; Cho, C.K.; Jang, W.-I.; Kim, M.S.; Choi, C. Stereotactic Body Radiotherapy for Recurrent or Oligometastatic Uterine Cervix Cancer: A Cooperative Study of the Korean Radiation Oncology Group (KROG 14-11). Anticancer Res. 2015, 35, 5103–5110. [Google Scholar]
- Gultekin, M.; Yilmaz, M.T.; Sari, S.Y.; Yildiz, D.; Ozyigit, G.; Yildiz, F. Stereotactic body radiotherapy boost in patients with cervical cancer. J. Obstet. Gynaecol. 2022, 42, 3033–3040. [Google Scholar] [CrossRef] [PubMed]
- Gadda, I.R.; Khan, N.A.; Wani, S.Q.; Baba, M.H. To evaluate the use of tandem and cylinder as an intracavitary brachytherapy device for carcinoma of the cervix with regard to local control and toxicities. J. Cancer Res. Ther. 2022, 18, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Chopra, S.; Mulani, J.; Mittal, P.; Singh, M.; Shinde, A.; Gurram, L.; Scaria, L.; Aravindakshan, D.; Kohle, S.; Rane, P.; et al. Early outcomes of abbreviated multi-fractionated brachytherapy schedule for cervix cancer during COVID-19 pandemic. Brachytherapy 2022, 22, 125–131. [Google Scholar] [CrossRef]
- Pötter, R.; Georg, P.; Dimopoulos, J.C.A.; Grimm, M.; Berger, D.; Nesvacil, N.; Georg, D.; Schmid, M.P.; Reinthaller, A.; Sturdza, A.; et al. Clinical outcome of protocol based image (MRI) guided adaptive brachytherapy combined with 3D conformal radiotherapy with or without chemotherapy in patients with locally advanced cervical cancer. Radiother. Oncol. 2011, 100, 116–123. [Google Scholar] [CrossRef]
- Kamrava, M.; Banerjee, R. Brachytherapy in the treatment of cervical cancer: A review. Int. J. Women’s Health 2014, 6, 555–564. [Google Scholar] [CrossRef]
- Kang, H.-C.; Shin, K.H.; Park, S.-Y.; Kim, J.-Y. 3D CT-based high-dose-rate brachytherapy for cervical cancer: Clinical impact on late rectal bleeding and local control. Radiother. Oncol. 2010, 97, 507–513. [Google Scholar] [CrossRef]
- Castelnau-Marchand, P.; Chargari, C.; Maroun, P.; Dumas, I.; Del Campo, E.R.; Cao, K.; Petit, C.; Martinetti, F.; Tafo-Guemnie, A.; Lefkopoulos, D.; et al. Clinical outcomes of definitive chemoradiation followed by intracavitary pulsed-dose rate image-guided adaptive brachytherapy in locally advanced cervical cancer. Gynecol. Oncol. 2015, 139, 288–294. [Google Scholar] [CrossRef]
- Simpson, D.R.; Scanderbeg, D.J.; Carmona, R.; McMurtrie, R.M.; Einck, J.; Mell, L.K.; McHale, M.T.; Saenz, C.C.; Plaxe, S.C.; Harrison, T.; et al. Clinical Outcomes of Computed Tomography-Based Volumetric Brachytherapy Planning for Cervical Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 150–157. [Google Scholar] [CrossRef]
- Charra-Brunaud, C.; Harter, V.; Delannes, M.; Haie-Meder, C.; Quetin, P.; Kerr, C.; Castelain, B.; Thomas, L.; Peiffert, D. Impact of 3D image-based PDR brachytherapy on outcome of patients treated for cervix carcinoma in France: Results of the French STIC prospective study. Radiother. Oncol. 2012, 103, 305–313. [Google Scholar] [CrossRef]
- Tan, L.T.; Coles, C.E.; Hart, C.; Tait, E. Clinical impact of computed tomography-based image-guided brachytherapy for cervix cancer using the tandem-ring applicator—The Addenbrooke’s experience. Clin. Oncol. (R. Coll. Radiol.) 2009, 21, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.; Eifel, P.J.; Lu, J.; Grigsby, P.W.; Levenback, C.; Stevens, R.E.; Rotman, M.; Gershenson, D.M.; Mutch, D.G. Pelvic Radiation with Concurrent Chemotherapy Compared with Pelvic and Para-Aortic Radiation for High-Risk Cervical Cancer. N. Engl. J. Med. 1999, 340, 1137–1143. [Google Scholar] [CrossRef]
- Chen, S.-W.; Liang, J.-A.; Hung, Y.-C.; Yeh, L.-S.; Chang, W.-C.; Lin, W.-C.; Chang, Y.-Y. Effectiveness of Image-guided Brachytherapy in Patients With Locally Advanced Cervical Squamous Cell Carcinoma Receiving Concurrent Chemoradiotherapy. Anticancer Res. 2019, 39, 3015–3024. [Google Scholar] [CrossRef] [PubMed]
- Panizza, D.; Faccenda, V.; Lucchini, R.; Daniotti, M.C.; Trivellato, S.; Caricato, P.; Pisoni, V.; De Ponti, E.; Arcangeli, S. Intrafraction Prostate Motion Management During Dose-Escalated Linac-Based Stereotactic Body Radiation Therapy. Front. Oncol. 2022, 12, 883725. [Google Scholar] [CrossRef]
- Dincer, N.; Ugurluer, G.; Mustafayev, T.Z.; Serkizyan, A.; Aydin, G.; Güngör, G.; Yapici, B.; Atalar, B.; Özyar, E. Dosimetric comparison of stereotactic MR-guided radiation therapy (SMART) and HDR brachytherapy boost in cervical cancer. Brachytherapy 2023, 23, 18–24. [Google Scholar] [CrossRef]
- Ma, T.M.; Harkenrider, M.M.; Yashar, C.M.; Viswanathan, A.N.; Mayadev, J.S. Understanding the underutilization of cervical brachytherapy for locally advanced cervical cancer. Brachytherapy 2019, 18, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Williamson, C.W.; Mayadev, J. Underutilization of brachytherapy for cervical cancer in the United States. Brachytherapy 2023, 22, 15–20. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology. Cervical Cancer, Version 1. 2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf (accessed on 1 March 2025).
- Holschneider, C.H.; Petereit, D.G.; Chu, C.; Hsu, I.C.; Ioffe, Y.J.; Klopp, A.H.; Pothuri, B.; Chen, L.M.; Yashar, C. Brachytherapy: A critical component of primary radiation therapy for cervical cancer: From the Society of Gynecologic Oncology (SGO) and the American Brachytherapy Society (ABS). Gynecol. Oncol. 2019, 152, 540–547. [Google Scholar] [CrossRef]


| Study | Number of Patients and Staging | Target Volume Description/Median Tumor Volume | Reasons for Ineligibility for Brachytherapy |
|---|---|---|---|
| Kubicek et al. [13] 2013 | 11 N/A | GTV—MRI + physical exam CTV—Whole cervix PTV—5 mm from the CTV Median tumor volume: 9.163 cm3 | Size and location (1), bleeding (1), proximity to bladder and bowel (1), comorbid conditions (1), difficulty visualizing tumor (1), unable to place sleeve or other problems (6) |
| Facondo et al. [14] 2021 | 9 IIA/IIB—3/2 IIIB/IIIC—1/1 IVA—2 | CTV—Whole cervix PTV—5 mm from the CTV Median tumor volume: 60.11 cm3 | Patient refusal (2), cervical stenosis (5), thrombocytopenia (2) |
| Pontoriero et al. [15] 2015 | 5 II/IIB—1/2 III—2 | GTV—MRI + physical exam PTV—2 mm from the GTV Median tumor volume: 20 cm3 | Size and location (1), comorbidities (2), proximity to bladder and bowel (1), stenotic and short vaginal stump (1) |
| Turna et al. [16] 2024 | 40 IIA/IIB—2/5 IIIC—30 IVA—3 | GTV—MRI + PET-CT + physical exam CTV—GTV + Whole cervix PTV—CTV + 5 mm Median tumor volume: 47 cm3 | Medical (12), technical (13), patient refusal (15) |
| Haas et al. [17] 2012 | 6 IIB—4 IV/IVA—1/1 | GTV—Whole cervix, with fiducial markers | Anatomy (3), medical (2), patient refusal (1) |
| Hsieh et al. [18] 2013 | 9 IIB—4 IIIB—3 IVA—2 | GTV- MRI + CT + physical exam CTV—GTV + 7 mm PTV—CTV + 7 mm Median tumor volume: 41.6 cm3 | To uncannulate the cervical os (4), anaphylactic shock in anesthesia (1), CVA with poor medical condition (1), myoma with contact bleeding (1), old age (1), bed rest with poor medical condition (1) |
| Cheng et al. [19] 2021 | 25 IA/IB2—6/3 II/IIB—1/4 IIIA/IIB/IIIC—2/3/2 IVA/IVB—2/2 | CTV—Gross disease, superior half of the vagina, presacral region and regional lymph nodes (common, internal and external iliac) PTV—CTV + 8–15 mm Median tumor volume: 26.5 cm3 | Patient refusal (2), comorbidity (3), fistula (2), laterality of tumor location (4) |
| Guckenberger et al. [20] 2009 | 16 N/A | GTV—Residual macroscopic tumor in a planning CT image acquired at the end of the conventionally fractionated irradiation series to account for tumor regression CTV—GTV + 2–3 mm PTV—CTV + 5 mm Median GTV volume: 45 cm3 Median PTV volume: 92 cm3 | Large volume, peripheral location of the recurrent gynecological tumors |
| Lee et al. [21] 2021 | 25 I—1 II—10 III—9 IV—5 | CTV—All gross tumors, cervix, uterus, parametria and upper vagina CTV nodal—Common iliac, internal iliac, external iliac, obturator and presacral lymph nodes PTV—CTV + 5 mm Median tumor volume: 120 cm3 | Failure of intracavitary device insertion because of a narrow vagina or cervical os fibrosis (20), large tumor (2), extreme obesity (1), intolerable pain (1), unable to position appropriately due to left spastic hemiplegia (1) |
| Marnitz et al. [22] 2013 | 11 IIB—9 IIIB—2 | CTV—Whole cervix + MRI PTV—CTV + 0 mm Median tumor volume: 48.9 cm3 | Uterus bi-collis and bi-cornis (1), patient refusal (10) |
| Albuquerque et al. [23] 2019 | 15 IB2–IVB | CTVcervix—Included all gross tumors, the uninvolved cervix, uterus, parametria and 2 cm of vagina beyond the vaginal tumor involvement CTVnodal—Included the common iliac, external iliac, internal iliac, obturator and pre-sacral nodes, with para-aortic nodes if involved PTVnodal—CTVnodal + 7 mm PTVcervix—CTVcervix + 10–12 mm | Medically unfit, patient refusal, tumor extent required IBT for coverage |
| Jorcano et al. [24] 2010 | 26 IB/IC—10/7 IIA/IIB—2/5 IIIB—2 | CTV1 (primary treatment)—Pelvic lymph nodes +/− para-aortic nodes + tumor bed CTV 2 (Boost)—Vaginal vault, defined as 3 cm of vagina from the vaginal apex PTV—CTV2 + 6–10 mm | N/A |
| Molla et al. [6] 2005 | 16 IB2—9 IIB—6 IIIB—1 | CTV2 (boost)—Vaginal vault, uterus–parametria, tumor residual or tumor relapse PTV—CTV + 6 or 10 mm | N/A |
| Dalwadi et al. [25] 2020 | 25 N/A | CTV—Macroscopic tumor and the remaining cervix PTV—CTV + 5 mm | Medical (9), technical (7), patient refusal (9) |
| Hadi et al. [26] 2022 | 10 N/A | CTV—Macroscopic tumor and adjacent areas considered to contain microscopic spread PTV—CTV + 5 mm Median CTV volume: 35.2 cm3 Median PTV volume: 43.5 cm3 | Infiltration on the pelvic wall or on the urinary bladder wall, on the pelvic floor or on the urethra (8), contact with rectosigmoid junction and left ovary (1), not suitable for anesthesia (1) |
| Kemmerer et al. [27] 2012 | 11 IA/IB—2/7 IIB—1 IIIC1—1 | CTV—A uniform 1 cm expansion around the endometrial cavity and any radiographically identified tumor mass with MRI images | N/A |
| Lazzari et al. [28] 2020 | 25 IIB—2 IIIB/IIIC1/IIIC2—3/9/2 IVA/IVB—2/6 | CTV—Cervix, uterus, parametria, ovaries, vaginal tissues (based on vaginal extension), involved lymph nodes and relevant draining lymph-nodal groups | Proximity to bladder and bowel (6), unfit for general anesthetic/comorbid conditions (9), isolation/no compliance (5), unfavorable anatomy (5) |
| Study/Year | External Dose (Gy/Fr) | Boost Dose (Gy/Fr) | EQD2 α/β = 10/ EQD2 α/β = 3 (Gy) | Follow-Up (Months) | Overall Survival (%)/Local control (%) | Toxicity | |||
|---|---|---|---|---|---|---|---|---|---|
| Genitourinary | Gastrointestinal | ||||||||
| Acute | Late | Acute | Late | ||||||
| Kubicek et al. [13] 2013 | 45–50.4/25–28 | 5–27.5/1–5 | 50.5–80.8/ 51.2–89.95 | 14 | N/A | Grade 2–2 (18%) | N/A | Grade 2–2 (18%) | Grade 3–1 (9%) |
| Facondo et al. [14] 2021 | 50.4–61.6/28 | 15–25/3–5 | 80.8–92.4/ 88.38–106.6 | 16 | 2 years (70%)/N/A | Grade 1–2 (22%) | Grade 2–2 (22%) | Grade 1–1 (11%) | Grade 2–2 (22%) |
| Pontoriero et al. [15] 2015 | 45/25 | BT: 10–15/2–3 SBRT: 15–20/3–4 | 81.5–88.8 Gy/ 83.2–92.2 | 12 | 1 year/60% | Grade 1–3 (60%) Grade 2–1 (20%) | N/A | Grade 1–1 (20%) Grade 2–1 (20%) | N/A |
| Turna et al. [16] 2024 | 45/25 | 30/5 | 84.25/97.2 | 16 | N/A | Grade 0–36 (90%) Grade 1–2 (5%) Grade 2–2 (5%) | N/A | Grade 0–37 (92.5%) Grade 1–1 (2.5%) Grade 2–1 (2.5%) Grade 3–1 (2.5%) | N/A |
| Haas et al. [17] 2012 | 50.4–61.2/28–34 | 19.5–20/3–5 | 76.37–82/ 85.43–86.75 | 14 | N/A | Grade 1–4 (66%) Grade 2–4 (66%) | N/A | Grade 1–4 (66%) Grade 2–4 (66%) | N/A |
| Hsieh et al. [18] 2013 | 50–54/25–27 | 16–27/8–9 | 65.56–83.25/ 64.38–87.6 | 36 | 3 years (46.9%)/77.8% | Grade 1–8 (88%) Grade 2–1 (11%) | N/A | Grade 1–7 (78%) Grade 2–1 (11%) Grade 3–1 (11%) | Grade 2–3 (33%) |
| Cheng et al. [19] 2021 | 45–54/25–27 | 8–30/4–6.5 | 62.5–89.5/ 85–94 | 12 | N/A/ 80.8% | Grade 1–1 (4%) Grade 2–1 (4%) | Grade 1–1 (4%) Grade 2–2 (8%) | Grade 1–8 (32%) Grade 2–1 (4%) Grade 3–2 (8%) | Grade 2–1 (4%) Grade 3–2 (8%) |
| Guckenberger et al. [20] 2009 | 50/25 | 10–20/ 2–4 | 62.5–75/ 66–82 | 22 | 3 years (34%)/81% | Grade 2–3 (16%) | Grade 2–2 (10%) | Grade 2–3 (16%) | Grade 4–3 (16%) |
| Lee et al. [21] 2021 | 44–50.4/22–28 | 25/5 | 75.5–80.81/ 84–88.38 | 34 | 3 years (77.1%)/ 80.9% | Grade 1–3 (14.3%) Grade 2–5 (23.8%) Grade 3–2 (9.5%) | N/A | Grade 1–6 (28.6%) Grade 2–2 (9.5%) | N/A |
| Marnitz et al. [22] 2013 | 50.4/28 | 30/5 | 90/102.38 | 6 | 2 years (96%)/95% | Grade 1–9 (81.81%) Grade 2–2 (18.18%) | N/A | Grade 1–9 (81.81%) Grade 2–2 (18.18%) | N/A |
| Albuquerque et al. [23] 2019 | 45/25 | 28/4 | 83.92/99.2 | 19 | 2 years—53.3%/70.1% | N/A | N/A | Grade 1–6 (40%) Grade 2–7 (46.66%) Grade 3–6 (40%) | N/A |
| Jorcano et al. [24] 2010 | 45–50.4/25–28 | 14/2 | 64.1–69.4/ 71.2–76.4 | 47 | 3 years/95% | Grade 0–19 (73%) Grade 1–1 (3.8%) Grade 2–5 (19.23%) Grade 3–1 (3.8%) | Grade 0–20 (76.9%) Grade 1–4 (15.38%) Grade 2–1 (3.8%) | Grade 0–6 (23%) Grade 1–11 (42.3%) Grade 2–8 (30.7%) Grade 3–1 (3.8%) | Grade 0–15 (57.69%) Grade 1–7 (26.92%) Grade 2–2 (7.69%) Grade 3–1 (3.8%) |
| Molla et al. [6] 2005 | 45–50.4/25–28 | 14/2 (n = 12) 20/5 (n = 4) | 65–75.4/ 73–78.4 | 18 | N/A | Grade 0–12 (75%) Grade 1–1 (6.25%) Grade 2–3 (11.53%) | Grade 0–16 (100%) | Grade 0–9 (56.25%) Grade 1–2 (12.5%) Grade 2–2 (12.5%) | Grade 0–14 (87.5%) Grade 1–1 (6.25%) Grade 3–1 (6.25%) |
| Dalwadi et al. [25] 2020 | 45–50.4/25–28 | 24–30/4–5 | 76.25–89.56/ 86.4–102.38 | 25 | 2 years—(95.5%)/95.5% | N/A | Grade 2–1 (4%) | N/A | Grade 2–1 (4%) |
| Hadi et al. [26] 2022 | 50–55/25 | 10–16/2–4 | 69.3–83.9/ 66–90.2 | 9 | N/A/90% | Grade 1–4 (40%) | Grade 1–3 (30%) | Grade 1–5 (50%) | Grade 1–4 (40%) |
| Kemmerer et al. [27] 2012 | 45/25 | 30/5 | 84.25/97.2 | 10 | 1.5 years/57% | Grade 1–2 (18%) | N/A | Grade 1–8 (73%) Grade 3–1 (9%) | N/A |
| Lazzari et al. [28] 2020 | 45–50.4/25–28 | 25/5 | 75.5–80.8/ 83.2–88.38 | 26 | 2 years (67%)/78% | Acute genitourinary and gastrointestinal toxicity: Grade 0–15 (60%), grade 1–7 (28%), grade 2–3 (12%) Late genitourinary and gastrointestinal toxicity: Grade 0–16 (67%), grade 1–2 (21%), grade 2–3 (12%) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gazsi, I.; Marcu, L.G. A Systematic Review of SBRT Boost for Cervical Cancer Patients Who Cannot Benefit from Brachytherapy. Curr. Oncol. 2025, 32, 170. https://doi.org/10.3390/curroncol32030170
Gazsi I, Marcu LG. A Systematic Review of SBRT Boost for Cervical Cancer Patients Who Cannot Benefit from Brachytherapy. Current Oncology. 2025; 32(3):170. https://doi.org/10.3390/curroncol32030170
Chicago/Turabian StyleGazsi, Iozsef, and Loredana G. Marcu. 2025. "A Systematic Review of SBRT Boost for Cervical Cancer Patients Who Cannot Benefit from Brachytherapy" Current Oncology 32, no. 3: 170. https://doi.org/10.3390/curroncol32030170
APA StyleGazsi, I., & Marcu, L. G. (2025). A Systematic Review of SBRT Boost for Cervical Cancer Patients Who Cannot Benefit from Brachytherapy. Current Oncology, 32(3), 170. https://doi.org/10.3390/curroncol32030170