Estimating the Associated Burden of Illness and Healthcare Utilization of Newly Diagnosed Patients Aged ≥65 with Mantle Cell Lymphoma (MCL) in Ontario, Canada

Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Data Sources
2.3. Selection of General Population Controls
2.4. Study Outcomes
2.5. Stratification
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Study Population
3.2. Patient Characteristics
3.3. Healthcare Resource Utilization
3.4. Direct Healthcare Costs
3.5. Stratified Analysis
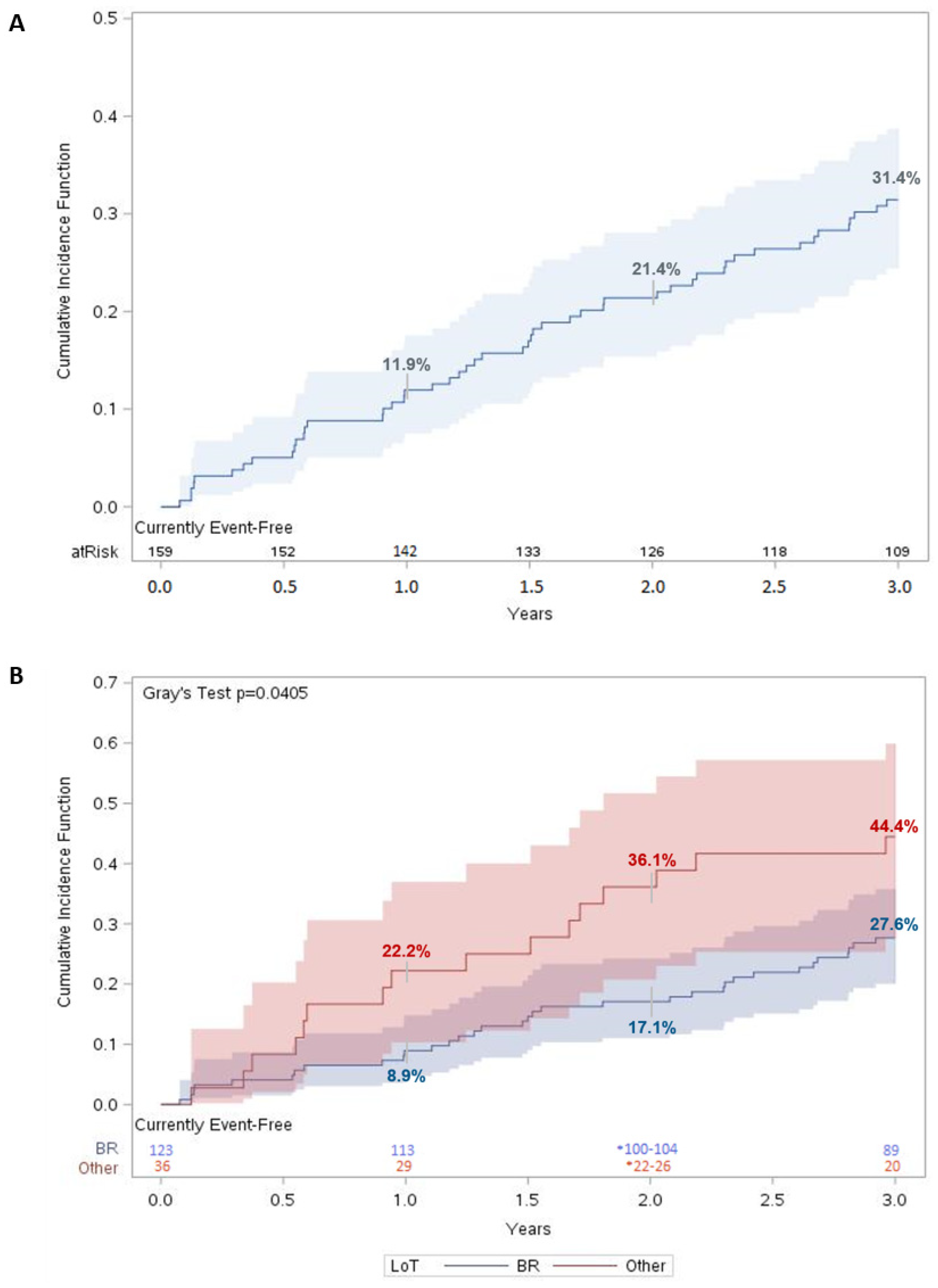
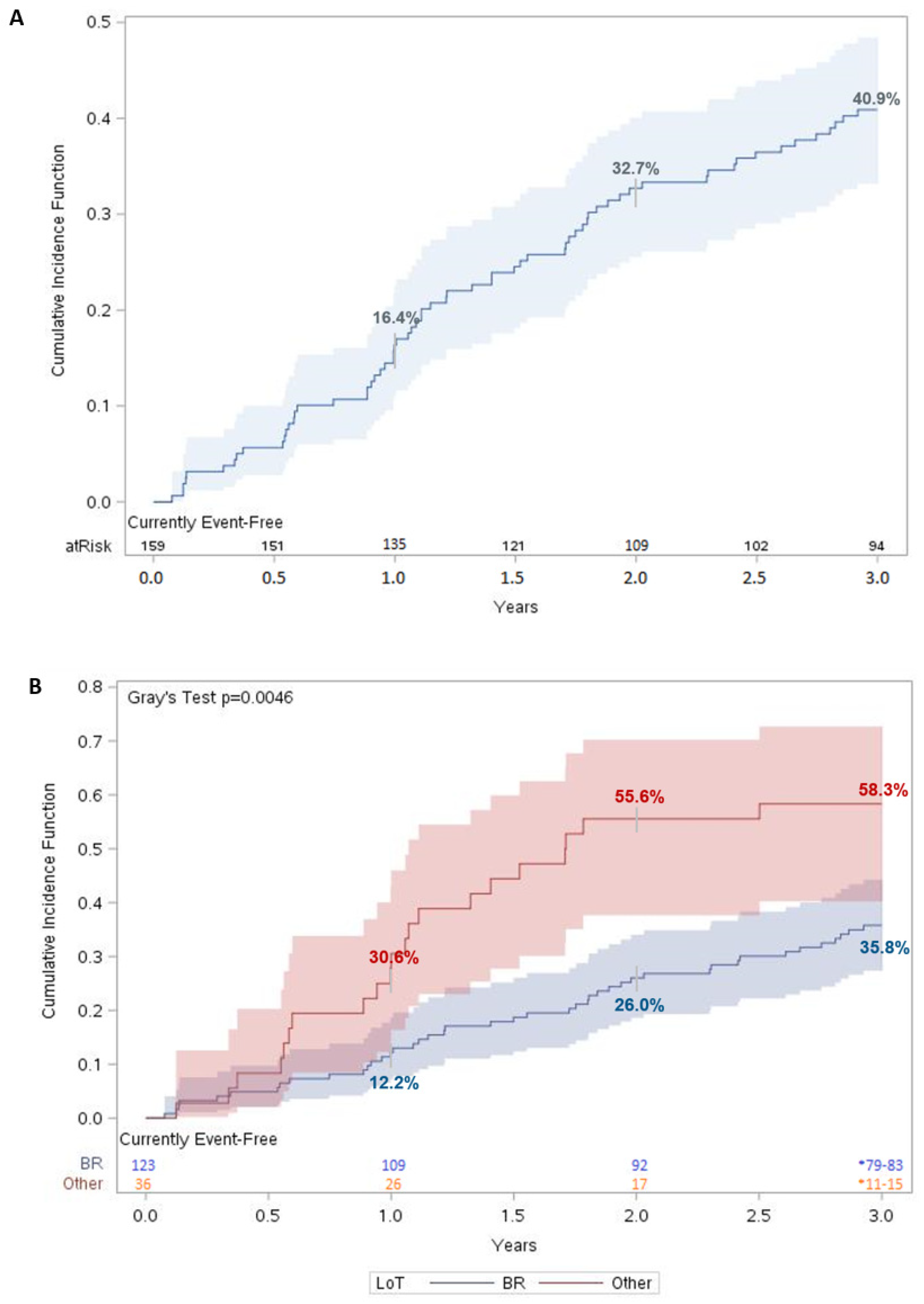
3.6. Survival Outcomes and Time to Next Treatment or Death
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sapkota, S.; Shaikh, H. Non-Hodgkin Lymphoma. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Candian Cancer Society Mantle Cell Lymphoma. Available online: https://cancer.ca/en/cancer-information/cancer-types/non-hodgkin-lymphoma/what-is-non-hodgkin-lymphoma/mantle-cell-lymphoma (accessed on 7 November 2022).
- Ibrutinib for Mantle Cell Lymphoma (Final Clinical Guidance Report). Available online: https://www.cadth.ca/sites/default/files/pcodr/pcodr_ibrutinib_imbruvica_mcl_fn_cgr.pdf (accessed on 4 October 2022).
- McKay, P.; Leach, M.; Jackson, B.; Robinson, S.; Rule, S. Guideline for the Management of Mantle Cell Lymphoma. Br. J. Haematol. 2018, 182, 46–62. [Google Scholar] [CrossRef]
- Xin, W. A Multi-Center, Prospective Clinical Study of Zanubrutinib, Rituximab and Combination Chemotherapy in Patients With Newly-Diagnosed Aggressive B-Cell Non-Hodgkin Lymphoma. 2021. Available online: https://clinicaltrials.gov (accessed on 28 September 2022).
- Lymphoma: Clinical Practice Guideline. Available online: https://www.albertahealthservices.ca/assets/info/hp/cancer/if-hp-cancer-guide-lyhe002-lymphoma.pdf (accessed on 4 October 2022).
- Monga, N.; Tam, C.; Garside, J.; Davids, M.S.; Ward, K.; Quigley, J.; Parisi, L.; Tapprich, C. Clinical Efficacy and Safety of First-Line Treatments in Patients with Mantle Cell Lymphoma: A Systematic Literature Review. Crit. Rev. Oncol. Hematol. 2021, 158, 103212. [Google Scholar] [CrossRef]
- Monga, N.; Garside, J.; Quigley, J.; Hudson, M.; O’Donovan, P.; O’Rourke, J.; Tapprich, C.; Parisi, L.; Davids, M.S.; Tam, C. Systematic Literature Review of the Global Burden of Illness of Mantle Cell Lymphoma. Curr. Med. Res. Opin. 2020, 36, 843–852. [Google Scholar] [CrossRef]
- NCCN Guidelines for Patients Mantle Cell Lymphoma; National Comprehensive Cancer Network: Plymouth Meeting, PA, USA, 2021; Volume 58.
- Drug Formulary. Available online: https://www.cancercareontario.ca/en/drugformulary/regimens (accessed on 4 October 2022).
- Tang, C.; Kuruvilla, J. Optimal Frontline Management of Mantle Cell Lymphoma: Can We Agree? Expert. Rev. Hematol. 2018, 11, 911–914. [Google Scholar] [CrossRef] [PubMed]
- Van der Jagt, R.; Laneuville, P.; MacDonald, D.; Stewart, D.; Christofides, A.; Sehn, L.H. A Canadian Perspective on Bendamustine for the Treatment of Chronic Lymphocytic Leukemia and Non-Hodgkin Lymphoma. Curr. Oncol. 2012, 19, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.R.; Poirier, A.; Woods, R.R.; Ellison, L.F.; Billette, J.-M.; Demers, A.A.; Zhang, S.X.; Yao, C.; Finley, C.; Fitzgerald, N.; et al. Projected Estimates of Cancer in Canada in 2022. CMAJ 2022, 194, E601–E607. [Google Scholar] [CrossRef] [PubMed]
- Monga, N.; Garside, J.; Davids, M.S.; Tam, C.; Ward, K.; Fotheringham, I.; O’Donovan, P.; Parisi, L.; Tapprich, C. Systematic Literature Review of Economic Evaluations, Costs/Resource Use, and Quality of Life in Patients with Mantle Cell Lymphoma. Pharmacoecon. Open 2021, 5, 175–186. [Google Scholar] [CrossRef]
- Government of Canada, S.C. Income of Individuals by Age Group, Sex and Income Source, Canada, Provinces and Selected Census Metropolitan Areas. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1110023901 (accessed on 28 October 2022).
- Postal Code OM Conversion File Plus (PCCF+). Available online: https://www150.statcan.gc.ca/n1/en/catalogue/82F0086X (accessed on 28 October 2022).
- ICES Data Dictionary. Available online: https://datadictionary.ices.on.ca/Applications/DataDictionary/Default.aspx (accessed on 28 October 2022).
- Wodchis, W.P.; Bushmeneva, K.; Nikitovic, M.; McKillop, I. Guidelines on Person-Level Costing Using Administrative Databases in Ontario; University of Toronto: Toronto, ON, Canada, 2013; Volume 71. [Google Scholar]
- Ames, J.B.; Djerboua, M.; Terrault, N.A.; Booth, C.M.; Flemming, J.A. Rising Healthcare Costs and Utilization among Young Adults with Cirrhosis in Ontario: A Population-Based Study. Can. J. Gastroenterol. Hepatol. 2022, 2022, 6175913. [Google Scholar] [CrossRef] [PubMed]
- Hudesman, D.P.; Chakravarty, S.D.; Emond, B.; Ellis, L.A.; Lefebvre, P.; Sadik, K.; Scher, J.U. Healthcare Resource Utilization and Costs Associated with Inflammatory Bowel Disease among Patients with Chronic Inflammatory Diseases: A Retrospective Cohort Study. BMC Rheumatol. 2020, 4, 16. [Google Scholar] [CrossRef] [PubMed]
- Kabadi, S.M.; Byfield, S.D.; Le, L.; Olufade, T. Adverse Events and Economic Burden among Patients Receiving Systemic Treatment for Mantle Cell Lymphoma: A Real-World Retrospective Cohort Study. Anticancer Res. 2021, 41, 927–936. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Tan, L.; Yuan, L.; Zhan, H.; Chen, Y.; Chen, W. PCN51 Disease Burden of Mantle CELL Lymphoma UNDER Current Treatment Pattern in China. Value Health Reg. Issues 2020, 22, S14. [Google Scholar] [CrossRef]
- New Drug Funding Program. Available online: https://www.cancercareontario.ca/en/Funding/New_Drug_Funding_Program (accessed on 17 May 2023).
- Seung, S.J.; Hurry, M.; Hassan, S.; Walton, R.N.; Evans, W.K. Cost-of-Illness Study for Non-Small-Cell Lung Cancer Using Real-World Data. Curr. Oncol. 2019, 26, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Sutradhar, R.; Li, Q.; Athale, U.; Bassal, M.; Breakey, V.; Gibson, P.J.; Patel, S.; Silva, M.; Zabih, V.; et al. Health Care Utilisation and Costs Associated with Different Treatment Protocols for Newly Diagnosed Childhood Acute Lymphoblastic Leukaemia: A Population-Based Study in Ontario, Canada. Eur. J. Cancer 2021, 151, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Boidart, A.; Darveau, M.; Déry, N.; Racine, M.-C. Real-World Budget Impact of Listing a Biosimilar of Rituximab. Can. J. Hosp. Pharm. 2020, 73, 13–18. [Google Scholar] [CrossRef] [PubMed]
- De Cock, E.; Kritikou, P.; Sandoval, M.; Tao, S.; Wiesner, C.; Carella, A.M.; Ngoh, C.; Waterboer, T. Time Savings with Rituximab Subcutaneous Injection versus Rituximab Intravenous Infusion: A Time and Motion Study in Eight Countries. PLoS ONE 2016, 11, e0157957. [Google Scholar] [CrossRef] [PubMed]
- Martin, P.; Chadburn, A.; Christos, P.; Weil, K.; Furman, R.R.; Ruan, J.; Elstrom, R.; Niesvizky, R.; Ely, S.; Diliberto, M.; et al. Outcome of Deferred Initial Therapy in Mantle-Cell Lymphoma. J. Clin. Oncol. 2009, 27, 1209–1213. [Google Scholar] [CrossRef] [PubMed]
- New Directions for Mantle Cell Lymphoma in 2022|American Society of Clinical Oncology Educational Book. Available online: https://ascopubs.org/doi/full/10.1200/EDBK_349509 (accessed on 4 October 2022).
- Janssen Research & Development, LLC. A Randomized, Double-Blind, Placebo-Controlled Phase 3 Study of the Bruton’s Tyrosine Kinase (BTK) Inhibitor, PCI-32765 (Ibrutinib), in Combination with Bendamustine and Rituximab (BR) in Subjects with Newly Diagnosed Mantle Cell Lymphoma. 2022. Available online: https://clinicaltrials.gov (accessed on 28 September 2022).
- Bond, D.A.; Martin, P.; Maddocks, K.J. Relapsed Mantle Cell Lymphoma: Current Management, Recent Progress, and Future Directions. J. Clin. Med. 2021, 10, 1207. [Google Scholar] [CrossRef] [PubMed]
- Greenwell, I.B.; Valla, K.; Caulfield, S.; Switchenko, J.M.; Staton, A.; Flowers, C.; Maly, J.; Blum, K.A.; Grover, N.; Mathews, S.; et al. Outcomes in Mantle Cell Lymphoma for Elderly Patients Undergoing Autologous Stem Cell Transplant in CR1. Biol. Blood Marrow Transplant. 2017, 23, S265–S266. [Google Scholar] [CrossRef]
- Bhatt, V.R. Cancer in Older Adults: Understanding Cause and Effects of Chemotherapy-Related Toxicities. Future Oncol. 2019, 15, 2557–2560. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic and Clinical Characteristics | MCL Patients N = 159 | Controls N = 636 | Absolute Standardized Difference | |
|---|---|---|---|---|
| Sex | Female | 51 (32.1%) | 204 (32.1%) | 0.00 |
| Male | 108 (67.9%) | 432 (67.9%) | 0.00 | |
| Age | Mean, SD | 75.3 ± 6.2 | 74.7 ± 6.5 | 0.09 |
| Median (IQR) | 75 (70–80) | 74 (69–80) | n.a. | |
| Min–Max | 65–92 | 65–96 | n.a. | |
| 65–74 years | 77 (48.4%) | 331 (52%) | 0.07 | |
| 75+ years | 82 (51.6%) | 305 (48%) | 0.07 | |
| Rural residence | Urban | 135 (84.9%) | 547 (86%) | 0.03 |
| Rural | 24 (15.1%) | 89 (14%) | 0.03 | |
| Income quintile | Q1, lowest | 24 (15.1%) | 121 (19%) | 0.10 |
| Q2 | 33 (20.8%) | 131 (20.6%) | 0.00 | |
| Q3 | 29 (18.2%) | 117 (18.4%) | 0.00 | |
| Q4 | 33 (20.8%) | 131 (20.6%) | 0.00 | |
| Q5, highest | 40 (25.2%) | 136 (21.4%) | 0.09 | |
| New Ontario resident at diagnosis | * 1–5 | * 10–14 | 0.00 | |
| Local Health Integration Network | 1. Erie St. Clair | 9 (5.7%) | 36 (5.7%) | 0.00 |
| 2. South West | 9 (5.7%) | 36 (5.7%) | 0.00 | |
| 3. Waterloo Wellington | 10 (6.3%) | 40 (6.3%) | 0.00 | |
| 4. Hamilton Niagara Haldimand Brant | 15 (9.4%) | 60 (9.4%) | 0.00 | |
| 5. Central West | 7 (4.4%) | 28 (4.4%) | 0.00 | |
| 6. Mississauga Halton | 7 (4.4%) | 28 (4.4%) | 0.00 | |
| 7. Toronto Central | 17 (10.7%) | 68 (10.7%) | 0.00 | |
| 8. Central | 19 (11.9%) | 76 (11.9%) | 0.00 | |
| 9. Central East | 21 (13.2%) | 84 (13.2%) | 0.00 | |
| 10. South East | 8 (5%) | 32 (5%) | 0.00 | |
| 11. Champlain | 13 (8.2%) | 52 (8.2%) | 0.00 | |
| 12. North Simcoe Muskoka | 7 (4.4%) | 28 (4.4%) | 0.00 | |
| 13. North East | 11 (6.9%) | 44 (6.9%) | 0.00 | |
| 14. North West | 6 (3.8%) | 24 (3.8%) | 0.00 | |
| Cancer history (assessed within a 5-year lookback) ^ | Any cancer | 15 (9.4%) | 60 (9.4%) | 0.00 |
| Charlson co-morbidity index (assessed within a 2-year lookback) | 0 | 23 (14.5%) | 65 (10.2%) | 0.13 |
| 1 | 7 (4.4%) | 18 (2.8%) | 0.08 | |
| 2 | * 2–6 | * 16–20 | 0.03 | |
| 3+ | * 1–5 | * 16–20 | 0.04 | |
| Missing | 119 (74.8%) | 520 (81.8%) | 0.17 | |
| Comorbidities, any time before index date (ICES-derived cohorts) | Diabetes mellitus | 38 (23.9%) | 197 (31%) | 0.16 |
| Congestive heart failure (CHF) | 9 (5.7%) | 56 (8.8%) | 0.12 | |
| Chronic obstructive pulmonary disease (COPD) | 35 (22%) | 130 (20.4%) | 0.04 | |
| Rheumatoid arthritis (RA) | * 1–5 | * 20–24 | 0.15 | |
| Crohn’s/Colitis | * 1–5 | * 1–5 | 0.08 | |
| Time from index date to end of follow-up, days | Mean, SD | 915.3 ± 321.5 | 1,029.7 ± 207.9 | 0.42 |
| Median (IQR) | 1,095 (841–1,095) | 1,095 (1,095–1,095) | n.a. | |
| Min–Max | 28–1,095 | 66–1,095 | n.a. | |
| BOI Outcomes | Year 1 | Year 2 | Year 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Number of Patients | MCL Patients | Controls | p-Value | MCL Patients | Controls | p-Value | MCL Patients | Controls | p-Value |
| N = 159 | N = 636 | N = 140 | N = 611 | N = 125 | N = 581 | ||||
| Person years | |||||||||
| Mean, SD | 0.94 ± 0.19 | 0.98 ± 0.11 | n.a. | 0.94 ± 0.18 | 0.98 ± 0.12 | n.a. | 0.94 ± 0.20 | 0.99 ± 0.09 | n.a. |
| Median, IQR | 1 (1–1) | 1 (1–1) | 1 (1–1) | 1 (1–1) | 1 (1–1) | 1 (1–1) | |||
| Healthcare resource utilization (HCRU) | |||||||||
| Attending physician specialty | |||||||||
| Medical oncologist | 15 (9.4%) | * 1–5 | n.a. | * 10–14 | * 1–5 | n.a. | * 6–10 | * 1–5 | n.a. |
| Hematologist | 73 (45.9%) | * 1–5 | n.a. | 58 (41.4%) | * 1–5 | n.a. | 36 (28.8%) | * 1–5 | n.a. |
| Internal medicine | 24 (15.1%) | 26 (4.1%) | n.a. | 11 (7.9%) | 31 (5.1%) | n.a. | 10 (8%) | 23 (4%) | n.a. |
| Family practice/GP | 33 (20.8%) | 404 (63.5%) | n.a. | 46 (32.9%) | 396 (64.8%) | n.a. | 56 (44.8%) | 379 (65.2%) | n.a. |
| Other | 14 (8.8%) | 157 (24.7%) | n.a. | 13 (9.3%) | 134 (21.9%) | n.a. | 12 (9.6%) | 127 (21.9%) | n.a. |
| No attending physician | 0 (0%) | 42 (6.6%) | n.a. | * 1–5 | * 43–47 | n.a. | * 1–5 | * 45–49 | n.a. |
| GP visits | |||||||||
| Mean, SD | 12.4 ± 15.7 | 7.9 ± 10.0 | <0.0001 | 9.8 ± 10.4 | 7.9 ± 10.4 | 0.0467 | 10.9 ± 13.1 | 8.4 ± 13.0 | 0.0377 |
| Median, IQR | 8 (5–15) | 5 (2–10) | 6.5 (4–12.5) | 5 (2–10) | 7 (3–14) | 5 (2–10) | |||
| Oncologist and hematologist visits | |||||||||
| Mean, SD | 18.0 ± 14.8 | 0.4 ± 3.5 | <0.0001 | 10.8 ± 11.1 | 0.4 ± 2.5 | <0.0001 | 8.3 ± 9.6 | 0.3 ± 2.0 | <0.0001 |
| Median, IQR | 18 (5–26) | 0 (0–0) | 8 (5–13) | 0 (0–0) | 5 (2–9) | 0 (0–0) | |||
| Other specialist visits | |||||||||
| Mean, SD | 27.0 ± 24.5 | 9.7 ± 14.0 | <0.0001 | 18.0 ± 21.0 | 9.8 ± 15.0 | <0.0001 | 18.2 ± 21.0 | 9.4 ± 13.9 | <0.0001 |
| Median, IQR | 21 (11–35) | 5 (2–12) | 11 (5–21.5) | 5 (2–12) | 12 (5–22) | 5 (2–10) | |||
| Inpatient hospitalizations | |||||||||
| Mean, SD | 0.8 ± 1.2 | 0.2 ± 0.7 | <0.0001 | 0.6 ± 1.2 | 0.2 ± 0.5 | <0.0001 | 0.5 ± 0.9 | 0.2 ± 0.6 | <0.0001 |
| Median, IQR | 0 (0–1) | 0 (0–0) | 0 (0–1) | 0 (0–0) | 0 (0–1) | 0 (0–0) | |||
| Emergency department visits | |||||||||
| Mean, SD | 1.5 ± 1.8 | 0.6 ± 1.3 | <0.0001 | 1.3 ± 2.0 | 0.6 ± 1.3 | <0.0001 | 1.0 ± 1.5 | 0.6 ± 1.3 | 0.0090 |
| Median, IQR | 1 (0–2) | 0 (0–1) | 0 (0–2) | 0 (0–1) | 0 (0–2) | 0 (0–1) | |||
| Direct healthcare costs | |||||||||
| Total direct costs | |||||||||
| Mean, SD | 77,554.7 ± 40,788.5 | 11,123.8 ± 24,515.1 | <0.0001 | 40,093.0 ± 28,719.7 | 10,891.1 ± 24,060.6 | <0.0001 | 36,059.2 ± 36,302.9 | 11,233.9 ± 26,261.2 | <0.0001 |
| Median, IQR | 83,931.0 (50,942.0–105,899.0) | 3,105.0 (1,234.5–8,567.5) | 31,853.5 (25,054.5–54,577.5) | 2,974.0 (1,200.0–8,884.0) | 23,500.0 (14,945.0–40,162.0) | 2,589.0 (1,159.0–6,743.0) | |||
| GP costs | |||||||||
| Mean, SD | 463.1 ± 807.6 | 281.6 ± 526.7 | 0.0022 | 437.7 ± 808.2 | 280.9 ± 548.7 | 0.0135 | 475.2 ± 927.7 | 301.5 ± 751.8 | 0.0266 |
| Median, IQR | 191.0 (19.0–529.0) | 101.0 (3.5–306.5) | 175.0 (11.0–450.0) | 88.0 (0–286.0) | 127.0 (10.0–452.0) | 82.0 (0–273.0) | |||
| Oncologist and hematologist costs | |||||||||
| Mean, SD | 907.3 ± 820.8 | 170.5 ± 132.8 | <0.0001 | 309.2 ± 392.2 | 213.7 ± 177.6 | <0.0001 | 259.5 ± 392.2 | 222.0 ± 184.4 | <0.0001 |
| Median, IQR | 860.0 (86.0–1,556.0) | 127.0 (91.0–254.0) | 203.0 (0–505.0) | 174.0 (123.0–285.0) | 81.0 (0–296.0) | 170.0 (103.0–264.0) | |||
| Other specialist costs | |||||||||
| Mean, SD | 3,349.4 ± 2,575.7 | 1,427.3 ± 2,085.8 | <0.0001 | 2,194.6 ± 2,449.3 | 1,326.0 ± 1,806.2 | <0.0001 | 2,324.3 ± 2,651.9 | 1,244.7 ± 1,719.2 | <0.0001 |
| Median, IQR | 2,674.0 (1,687.0–4,082.0) | 715.0 (240.0–1,682.0) | 1,212.0 (570.0–2,883.0) | 719.0 (231.0–1,672.0) | 1,329.0 (568.0–2,628.0) | 666.0 (241.0–1,343.0) | |||
| Inpatient hospitalization costs | |||||||||
| Mean, SD | 8,953.6 ± 19,016.9 | 2,367.3 ± 8,420.3 | <0.0001 | 6,037.6 ± 16,122.6 | 2,611.9 ± 9,147.3 | 0.0012 | 5,956.4 ± 13,823.6 | 3,022.2 ± 14,013.1 | 0.0319 |
| Median, IQR | 0 (0–11,472.0) | 0 (0–0) | 0 (0–5,539.0) | 0 (0–0) | 0 (0–6,799.0) | 0 (0–0) | |||
| Same-day surgery costs | |||||||||
| Mean, SD | 839.8 ± 1,155.6 | 330.2 ± 1,036.3 | <0.0001 | 384.2 ± 1,219.4 | 299.6 ± 848.8 | 0.4026 | 401.8 ± 1,161.7 | 244.5 ± 769.9 | 0.0746 |
| Median, IQR | 0 (0–1,555.0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | |||
| ED costs | |||||||||
| Mean, SD | 673.4 ± 890.0 | 239.1 ± 572.2 | <0.0001 | 577.8 ± 1,042.1 | 255.9 ± 570.0 | <0.0001 | 439.5 ± 711.5 | 253.4 ± 571.2 | 0.0034 |
| Median, IQR | 341.0 (0–958.0) | 0 (0–238.0) | 0 (0–741.0) | 0 (0–274.0) | 0 (0–675.0) | 0 (0–248.0) | |||
| Cancer clinics costs | |||||||||
| Mean, SD | 19,332.4 ± 11,850.8 | 522.7 ± 7637.9 | 0.0902 | 9,963.8 ± 8640.4 | 442.2 ± 7318.0 | 0.1505 | 7,823.9 ± 9,453.7 | 482.4 ± 7,849.8 | 0.1614 |
| Median, IQR | 21,862.0 (10,789.0–27,584.0) | 0 (0–0) | 7,829.0 (5,832.0–11,597.5) | 0 (0–0) | 4,385.0 (1,674.0–9,034.0) | 0 (0–0) | |||
| Public drug plan (ODB) costs | |||||||||
| Mean, SD | 2,791.1 ± 3,981.5 | 1,723.9 ± 4,383.8 | 0.0014 | 2,747.5 ± 5,751.2 | 1,584.7 ± 3,251.9 | 0.0044 | 4,699.6 ± 16,895.9 | 1,811.3 ± 4,196.1 | 0.0043 |
| Median, IQR | 1,112.0 (555.0–3,389.0) | 728.0 (2,14.5–1,734.0) | 934.5 (314.0–2,355.5) | 695.0 (191.0–1,683.0) | 852.0 (285.0–1,971.0) | 599.0 (166.0–1,698.0) | |||
| NDFP chemotherapy drug costs | |||||||||
| Mean, SD | 31,804.5 ± 20,979.9 | n.a. | 0.1575 | 12,871.7 ± 12,576.0 | n.a. | 0.1491 | 8,616.0 ± 11,849.0 | n.a. | 0.3159 |
| Median, IQR | 36,480.0 (13,042.0–48,362.0) | n.a. | 12,723.0 (0–15,715.5) | n.a. | 6,562.0 (0–10,306.0) | n.a. | |||
| Aggregated costs for other services ^ | |||||||||
| Mean, SD | 8,731.1 ± 11,754.2 | 4,299.5 ± 13,807.9 | <0.0001 | 4,806.5 ± 5,550.9 | 4,071.9 ± 13,606.4 | 0.2573 | 5,344.7 ± 9,005.5 | 3,935.3 ± 11,220.9 | 0.1254 |
| Median, IQR | 6,187.0 (3,877.0–9,006.0) | 787.5 (398.5–1,815.5) | 2,913.5 (1,940.0–5,936.0) | 748.0 (422.0–1,902.0) | 2,746.0 (1,785.0–5,527.0) | 650.0 (406.0–1,605.0) | |||
| BOI Outcomes | BR | Other | ||||
|---|---|---|---|---|---|---|
| Number of Patients | Year 1 | Year 2 | Year 3 | Year 1 | Year 2 | Year 3 |
| (N = 123) | (N = 112) | (N = * 101–105) | (N = 36) | (N = 28) | (N = * 22–26) | |
| Person years | ||||||
| Mean, SD | 0.95 ± 0.18 | 0.95 ± 0.18 | 0.94 ± 0.18 | 0.90 ± 0.23 | 0.93 ± 0.18 | 0.92 ± 0.26 |
| Median, IQR | 1 (1–1) | 1 (1–1) | 1 (1–1) | 1 (1–1) | 1 (1–1) | 1 (1–1) |
| Healthcare resource utilization (HCRU) | ||||||
| Attending physician specialty | ||||||
| Medical oncologist | 9 (7.3%) | * 6–10 | * 4–8 | 6 (16.7%) | * 1–5 | * 1–5 |
| Hematologist | 61 (49.6%) | 52 (46.4%) | * 31–35 | 12 (33.3%) | 6 (21.4%) | * 1–5 |
| Internal medicine | 18 (14.6%) | * 6–10 | * 5–9 | 6 (16.7%) | * 1–5 | * 1–5 |
| Family practice/GP | 23 (18.7%) | 34 (30.4%) | 42 (41.2%) | 10 (27.8%) | 12 (42.9%) | 14 (60.9%) |
| Other | * 9–13 | * 8–12 | * 7–11 | * 1–5 | * 1–5 | * 1–5 |
| No attending physician | 0 (0%) | * 1–5 | * 1–5 | 0 (0%) | 0 (0%) | * 1–5 |
| GP visits | ||||||
| Mean, SD | 12.0 ± 16.2 | 9.2 ± 9.8 | 10.8 ± 13.8 | 13.5 ± 14.0 | 12.4 ± 12.4 | 11.3 ± 9.5 |
| Median, IQR | 7 (5–14) | 6 (4–12) | 7 (3–12) | 11 (3–17) | 8 (5–17) | 10 (4–16) |
| Oncologist and hematologist visits | ||||||
| Mean, SD | 18.0 ± 14.1 | 10.7 ± 10.7 | 8.6 ± 10.0 | 18.0 ± 17.2 | 11.3 ± 12.9 | 6.7 ± 7.8 |
| Median, IQR | 19 (5–26) | 8 (5–13) | 5 (2–10) | 16 (6–22) | 7 (3–16) | 5 (2–8) |
| Other specialist visits | ||||||
| Mean, SD | 23.8 ± 18.1 | 15.6 ± 16.9 | 17.2 ± 18.9 | 38.2 ± 37.5 | 27.4 ± 31.5 | 22.3 ± 28.8 |
| Median, IQR | 19 (11–32) | 10 (5–20) | 12 (5–22) | 28 (13–45) | 14 (8–35) | 11 (5–27) |
| Inpatient hospitalizations | ||||||
| Mean, SD | 0.7 ± 1.0 | 0.6 ± 1.1 | 0.5 ± 0.9 | 1.2 ± 1.5 | 0.9 ± 1.5 | 0.6 ± 0.9 |
| Median, IQR | 0 (0–1) | 0 (0–1) | 0 (0–1) | 1 (0–2) | 0 (0–2) | 0 (0–1) |
| ED visits | ||||||
| Mean, SD | 1.4 ± 1.8 | 1.1 ± 1.8 | 1.0 ± 1.5 | 1.6 ± 1.9 | 1.8 ± 2.5 | 1.1 ± 1.6 |
| Median, IQR | 1 (0–2) | 0 (0–1) | 0 (0–1) | 1 (0–3) | 1 (0–3) | 0 (0–2) |
| Direct healthcare costs | ||||||
| Total direct costs | ||||||
| Mean, SD | 79,302.5 ± 41,021.2 | 39,424.3 ± 25,727.5 | 37,340.9 ± 37,134.5 | 71,583.1 ± 39,968.5 | 42,767.9 ± 38,934.2 | 30,375.2 ± 32,497.0 |
| Median, IQR | 87,738.0 (51,445.0–109,025.0) | 31,123.0 (25,055.0–52,479.0) | 24,557.0 (15,091.0–45,068.0) | 59,583.0 (50,019.0–81,740.0) | 32,051.0 (24,349.0–56,171.0) | 21,001.0 (13,126.0–33,795.0) |
| GP costs | ||||||
| Mean, SD | 450.9 ± 816.0 | 380.9 ± 686.4 | 485.8 ± 996.8 | 504.7 ± 787.9 | 665.0 ± 1,165.6 | 428.6 ± 535.4 |
| Median, IQR | 191.0 (19.0–515.0) | 174.0 (11.0–430.0) | 122.0 (10.0–435.0) | 173.0 (25.0–701.0) | 182.0 (21.0–661.0) | 215.0 (14.0–694.0) |
| Oncologist and hematologist costs | ||||||
| Mean, SD | 932.8 ± 837.5 | 324.9 ± 418.5 | 290.6 ± 443.9.0 | 818.0 ± 769.8 | 259.4 ± 298.8 | 169.1 ± 152.0 |
| Median, IQR | 802.0 (91.0–1,580.0) | 203.0 (0–505.0) | 71.0 (0–327.0) | 899.0 (17.0–1,337.0) | 149.0 (0–395.0) | 165.0 (34.0–292.0) |
| Other specialist costs | ||||||
| Mean, SD | 3,113.2 ± 2,256.4 | 1,995.0 ± 2,149.9 | 2,169.6 ± 2,521.1 | 4,156.6 ± 3,366.8 | 2,985.3 ± 3,321.1 | 3,090.1 ± 3,185.6 |
| Median, IQR | 2,605.0 (1,664.0–3,932.0) | 1,231.0 (532.0–2,735.0) | 1,247.0 (553.0–2,458.0) | 3,386.0 (2,341.0–4,634.0) | 1,064.0 (716.0–4,802.0) | 1,844.0 (718.0–4,029.0) |
| Inpatient hospitalization costs | ||||||
| Mean, SD | 6,483.9 ± 10,150.0 | 4,781.0 ± 12,581.3 | 5,617.7 ± 13,803.6 | 17,391.7 ± 34,333.4 | 11,064.0 ± 25,587.3 | 7,458.7 ± 14,121.9 |
| Median, IQR | 0 (0–10,135.0) | 0 (0–4,678.0) | 0 (0–4,189.0) | 4,646.0 (0–19,108.0) | 0 (0–15,813.0) | 0 (0–12,644.0) |
| Same-day surgery costs | ||||||
| Mean, SD | 892.9 ± 1,114.1 | 471.1 ± 1,347.2 | 438.6 ± 1,254.7 | 658.6 ± 1,287.8 | n.a. | n.a. |
| Median, IQR | 0 (0–1,690.0) | 0 (0–460.0) | 0 (0–0) | 0 (0–837.0) | n.a. | n.a. |
| ED costs | ||||||
| Mean, SD | 632.0 ± 857.9 | 469.5 ± 859.5 | 429.5 ± 707.1 | 814.9 ± 991.7 | 1,011.0 ± 1,519.9 | 484.0 ± 745.4 |
| Median, IQR | 340.0 (0–938.0) | 0 (0–621.0) | 0 (0–687.0) | 512.0 (0–1,481.0) | 395.0 (0–1,670.0) | 0 (0–675.0) |
| Cancer clinics costs | ||||||
| Mean, SD | 20,942.5 ± 12,340.3 | 9,841.0 ± 7,866.4 | 8,052.1 ± 9,535.7 | 13,831.3 ± 7,933.6 | 10,454.8 ± 11,385.8 | 6,812.1 ± 9,218.1 |
| Median, IQR | 25,106.0 (11,707.0–29,167.0) | 8,249.0 (5,860.0–11,535.0) | 5,474.0 (1,957.0–9,921.0) | 14,022.0 (8,595.0–17,864.0) | 7,688.0 (2,210.0–15,774.0) | 3,914.0 (0–8,647.0) |
| ODB costs | ||||||
| Mean, SD | 2,210.5 ± 3,147.2 | 2,708.7 ± 6,205.2 | 5,246.0 ± 18,568.3 | 4,774.9 ± 5,639.6 | 2,902.5 ± 3,457.8 | 2,276.7 ± 4,316.9 |
| Median, IQR | 1,000.0 (465.0–2,488.0) | 872.0 (267.0–2,191.0) | 859.0 (285.0–2,026.0) | 1,755.0 (896.0–8,319.0) | 1,375.0 (438.0–4,062.0) | 737.0 (266.0–1,887.0) |
| NDFP chemotherapy drug costs | ||||||
| Mean, SD | 35,590.8 ± 21,638.1 | 14,180.9 ± 13,138.7 | 9,716.0 ± 12,695.9 | 18,868.2 ± 11,508.0 | 7,635.0 ± 8,305.6 | 3,737.7 ± 4,566.0 |
| Median, IQR | 43,185.0 (17,189.0–52,399.0) | 13,136.0 (6,075.0–15,850.0) | 7,032.0 (0–11,752.0) | 21,396.0 (8,384.0–26,922.0) | 4,864.0 (0–14,540.0) | 0 (0–8,320.0) |
| Aggregated costs for other services ^ | ||||||
| Mean, SD | 8,349.0 ± 12,665.6 | 4,519.8 ± 5,536.0 | 5,158.4 ± 8,755.6 | 10,036.7 ± 7,890.4 | 5,953.4 ± 5,561.2 | 6,170.7 ± 10,212.1 |
| Median, IQR | 5,638.0 (3,638.0–8,019.0) | 2,748.0 (1,853.0–5,241.0) | 2,781.0 (1,748.0–5,409.0) | 7,996.0 (4,886.0–11,106.0) | 3,550.0 (2,305.0–8,771.0) | 2,735.0 (1,839.0–6,148.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anglin, P.; Elia-Pacitti, J.; Eberg, M.; Muratov, S.; Kukaswadia, A.; Sharma, A.; Ewara, E.M. Estimating the Associated Burden of Illness and Healthcare Utilization of Newly Diagnosed Patients Aged ≥65 with Mantle Cell Lymphoma (MCL) in Ontario, Canada. Curr. Oncol. 2023, 30, 5529-5545. https://doi.org/10.3390/curroncol30060418
Anglin P, Elia-Pacitti J, Eberg M, Muratov S, Kukaswadia A, Sharma A, Ewara EM. Estimating the Associated Burden of Illness and Healthcare Utilization of Newly Diagnosed Patients Aged ≥65 with Mantle Cell Lymphoma (MCL) in Ontario, Canada. Current Oncology. 2023; 30(6):5529-5545. https://doi.org/10.3390/curroncol30060418
Chicago/Turabian StyleAnglin, Peter, Julia Elia-Pacitti, Maria Eberg, Sergey Muratov, Atif Kukaswadia, Arushi Sharma, and Emmanuel M. Ewara. 2023. "Estimating the Associated Burden of Illness and Healthcare Utilization of Newly Diagnosed Patients Aged ≥65 with Mantle Cell Lymphoma (MCL) in Ontario, Canada" Current Oncology 30, no. 6: 5529-5545. https://doi.org/10.3390/curroncol30060418
APA StyleAnglin, P., Elia-Pacitti, J., Eberg, M., Muratov, S., Kukaswadia, A., Sharma, A., & Ewara, E. M. (2023). Estimating the Associated Burden of Illness and Healthcare Utilization of Newly Diagnosed Patients Aged ≥65 with Mantle Cell Lymphoma (MCL) in Ontario, Canada. Current Oncology, 30(6), 5529-5545. https://doi.org/10.3390/curroncol30060418