Abstract
The Eustachian ridge is ablated as part of the cavotricuspid isthmus (CTI) involved in typical atrial flutter (AFL) ablation, but is itself rarely an arrhythmogenic focus. We report a case of a patient with dual tachycardia involving the CTI area. During an electrophysiology study including ablation of the CTI, a second slightly irregular local tachycardia with potentials on the distal ablation catheter was noticed. After termination of AFL during the CTI ablation, the local tachycardia was persistently recorded at the Eustachian ridge, without affecting the atrial tissue or the stable sinus rhythm. Additional radiofrequency ablation in this area terminated the local tachycardia.
Introduction
Typical atrial flutter (AFL) is dependent on muscular sleeves in the anatomical area of the cavotricuspid isthmus (CTI) [1,2]. The Eustachian ridge is ablated as part of standard catheter ablation of the macroreentrant circuit involved in typical AFL, but itself is rarely a site of arrhythmogenic foci [2,3,4]. We report a case of a patient with dual tachycardia involving the CTI area.
Case report
A 79-year-old male patient was referred to our hospital for an electrophysiology study (EPS) and catheter ablation because of persistent tachycardia. The patient had not undergone any previous ablation procedures nor had heart surgery. His 12-lead ECG on admission revealed atrial flutter with mostly 3:1 atrioventricular conduction (Figure 1). Echocardiography revealed a leh ventricular ejection fraction of 42% with diffuse hypokinesis, moderate mitral regurgitation and no other significant pathologies. EPS was performed under light sedation with midazolam and fentanyl.
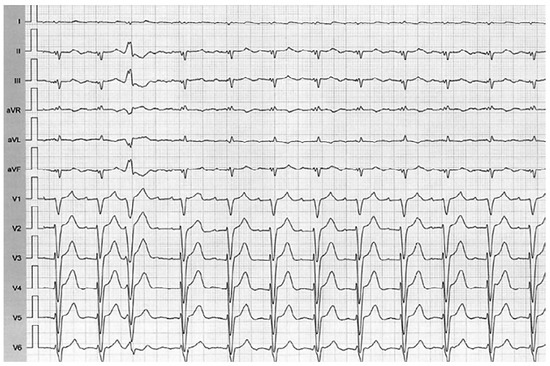
Figure 1.
Surface 12-lead electrocardiogram of the persistent tachycardia at admission.
Using entrainment mapping and an electroanatomic 3D mapping system (CARTO3, Biosense-Webster, Diamond Bar, CA, USA) with a steerable decapolar catheter (EZSteer AutoID, Biosense-Webster) and an irrigated-tip catheter (Navistar ThermoCool SmartTouch, Biosense-Webster), we identified typical “counterclockwise” AFL with a tachycardia cycle length (TCL) of 236 ms. Ablation along the CTI terminated the AFL. However, during mapping and ablation of the CTI, a second slightly irregular local tachycardia with potentials on the distal ablation catheter was noticed (TCL 210–254 ms) (Figure 2). Aher termination of AFL during the CTI ablation, the local tachycardia was persistently recorded at the Eustachian ridge, without affecting the atrial tissue or the stable sinus rhythm (Figure 3). Additional radiofrequency ablation in this area terminated the local tachycardia. Aherwards, only dissociated ectopic potentials on the mapping catheter could be noted (Figure 4). During a 3-month follow-up, the patient remained free of arrhythmia without antiarrhythmic drugs.
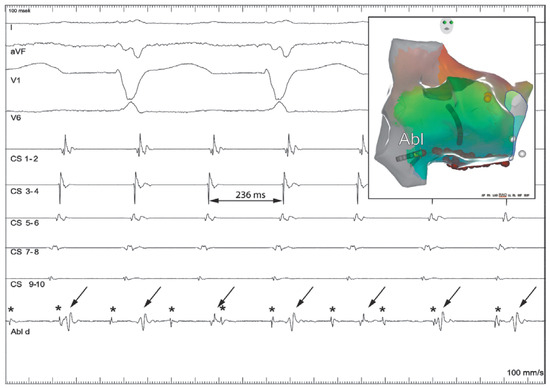
Figure 2.
Dual tachycardia recorded with the ablation catheter positioned at the Eustachian ridge. Ablation/mapping catheter is positioned at the Eustachian ridge (smaller picture – RAO projection): arrows pointing at the atrial flutter (AFL) potentials and asterisks (*) at the persistent local tachycardia potentials. Shown are surface leads I, aVF, V1 and V6 and intracardiac electrograms from the coronary sinus distal to proximal (CS 1 to 10) and ablation/mapping catheter (Abl d).
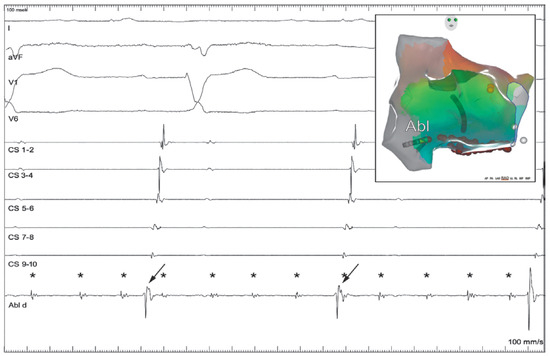
Figure 3.
Local tachycardia with slightly irregular cycle length and exit block without affecting sinus rhythm. Ablation/mapping catheter is at the area of Eustachian ridge: arrows pointing at atrial (sinus rhythm) potentials and asterisks (*) at the persistent local tachycardia with slight irregularity, without affecting or being affected by the sinus rhythm. Distal ablation/mapping catheter is located at the area of Eustachian ridge (smaller picture – RAO projection). Shown are surface leads I, aVF, V1 and V6 and intracardiac electrograms from coronary sinus distal to proximal (CS 1 to 10) and ablation/mapping catheter (Abl d).
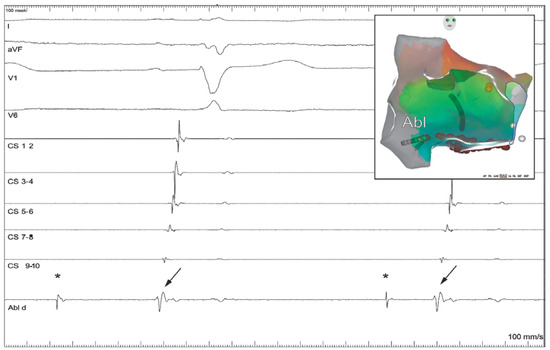
Figure 4.
Dissociated potentials recorded at the Eustachian ridge. Ablation/mapping catheter is at the area of Eustachian ridge: arrows pointing at atrial (sinus rhythm) potentials and asterisks (*) at the dissociated ectopic potentials recorded by the distal ablation/mapping catheter located at the area of Eustachian ridge (smaller picture – RAO projection). Shown are surface leads I, aVF, V1 and V6 and intracardiac electrograms from coronary sinus distal to proximal (CS 1 to 10) and ablation/mapping catheter (Abl d).
Discussion
To the authors’ best knowledge, this is the first case report of a patient with concomitant dual tachycardia originating from the CTI area, specifically the Eustachian ridge. Although several case reports and articles about intra-CTI re-entry and focal intra-CTI tachycardia exist in the literature, the current case features several interesting specific findings.
First, the CTI has been described as a muscular area of fast conduction, low arrhythmogenic potential and very uncommon origin of ectopic activity [2,3]. In our case, the patient had a persistent concomitant dual tachycardia: typical AFL (TCL 236 ms) and a local persistent tachycardia with a slightly irregular TCL (210–254 ms). Earlier papers described intra-CTI atrial tachycardias either aher the CTI ablation that terminated typical AFL or during the initial EPS as the only tachycardia, but never as two concomitant tachycardias [5,6,7,8,9]. Manita et al. speculated whether atrial tachycardia coexisted with AFL, and was then unmasked aher CTI ablation had terminated AFL. In our case, both tachycardias occurred at the same time: AFL as the clinical tachycardia and a local tachycardia, which, although faster, did not influence AFL (Figure 2) [7]. The only explanation for this is that the electrically active tissue at the Eustachian ridge was, at least at the time of the procedure, electrically isolated. In addition, two prior reports described the inferior vena cava as an origin of an arrhythmogenic focus triggering paroxysmal atrial fibrillation [4,10].
Second, the local tachycardia mostly had a shorter TCL when compared with AFL, although it was slightly irregular (210–254 ms) (Figure 2). All previously reported intra-CTI atrial tachycardias had significantly longer TCLs when compared with AFL [5,6,7,8,9]. However, one can only speculate on the TCL of a hypothetical clinical tachycardia in the absence of exit block, and also whether the morphology on the surface ECG would resemble AFL as in previous reports [5,6,7,8,9,11].
Third, aher blocking the CTI and terminating the AFL, the local tachycardia persisted, but did not influence global atrial activation and, to our knowledge, did not result in other clinical tachycardias, proving exit block from this area [5,6,7,8,9]. It is unknown whether the entrance and exit block of the local tachycardia was created during the CTI ablation or whether it was preexisting. Mechanistically, there are two possible explanations of the tachycardia’s origin. Aher additional ablation at the Eustachian ridge, termination of the local tachycardia was noted with dissociated potentials, which favours focal ectopic tachycardia (Figure 4). However, the possibility of local micro-reentry cannot be ruled out.
In conclusion, this case demonstrates a rare origin of ectopic activity originating from the Eustachian ridge. Electrophysiologists should be aware of this possibility when performing ablation of CTI-dependent AFL. Whether the focus should be ablated (as we did in our case) owing to the possibility of the focal activity, causing clinical atrial tachycardias or triggering atrial fibrillation, remains unknown.
References
- Cabrera, J.A.; Sanchez Quintana, D.; Ho, S.Y.; Medina, A.; Anderson, R.H. The architecture of the atrial musculature between the orifice of the inferior caval vein and the tricuspid valve: the anatomy of the isthmus. J Cardiovasc Electrophysiol. 1998, 9, 1186–1195. [Google Scholar] [CrossRef] [PubMed]
- Asirvatham, S.J. Correlative anatomy and electrophysiology for the interventional electrophysiologist: right atrial flutter. J Cardiovasc Electrophysiol. 2009, 20, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.S.; Wu, T.J.; Hwang, C.; Zhou, S.; Okuyama, Y.; Hamabe, A.; et al. Thoracic veins and the mechanisms of non-paroxysmal atrial fibrillation. Cardiovasc Res. 2002, 54, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Scavée, C.; Jaïs, P.; Weerasooriya, R.; Haïssaguerre, M. The inferior vena cava: an exceptional source of atrial fibrillation. J Cardiovasc Electrophysiol. 2003, 14, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Itoh, T.; Yoshida, Y.; Morishima, I.; Yamada, T. Focal intra-cavotricuspid isthmus atrial tachycardias occurring aher typical atrial flutter ablation: incidence and electrocardiographic and electrophysiological characteristics. J Interv Card Electrophysiol. 2018. [CrossRef]
- Yang, Y.; Varma, N.; Keung, E.C.; Scheinman, M.M. Reentry within the cavotricuspid isthmus: an isthmus dependent circuit. Pacing Clin Electrophysiol. 2005, 28, 808–818. [Google Scholar] [CrossRef] [PubMed]
- Manita, M.; Kaneko, Y.; Taniguchi, Y.; Nakajima, T.; Ito, T.; Kurabayashi, M.; Nagai, R. Typical atrial flutterlike tachycardia developing aher inferior vena cava-tricuspid annulus isthmus ablation. Pacing Clin Electrophysiol. 2001, 24, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Varma, N.; Badhwar, N.; Tanel, R.E.; Sundara, S.; Lee, R.J.; et al. Pros-pective observations in the clinical and electrophysiological characteristics of intra-isthmus reentry. J Cardiovasc Electrophysiol. 2010, 21, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Saoudi, N.; Latcu, D.G. Intra isthmus reentry: another form of typical atrial flutter? J Cardiovasc Electrophysiol. 2010, 21, 1107–1108. [Google Scholar] [CrossRef] [PubMed]
- Mansour, M.; Ruskin, R.; Keane, D. Initiation of atrial fibrillation by ectopic beats originating from the ostium of the inferior vena cava. J Cardiovasc Electrophysiol. 2002, 13, 1292–1295. [Google Scholar] [CrossRef] [PubMed]
- Milliez, P.; Richardson, A.W.; Obioha Ngwu, O.; Zimetbaum, P.J.; Papageorgiou, P.; Josephson, M.E. Variable electrocardiographic characteristics of isthmus-dependent atrial flutter. J Am Coll Cardiol. 2002, 40, 1125–1132. [Google Scholar] [CrossRef] [PubMed]




© 2018 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.