Summary
A case of a 40-year-old patient with known HIV-infection and new onset of exertional dyspnea with dizziness is presented. At the end of an extensive diagnostic investigation, the underlying exercise-induced second degree 3:1 atrioventricular (AV) block was revealed by means of an ergometry/bicycle stress test. After exclusion of reversible causes, a DDD pacemaker was implanted three months after the onset of symptoms. Thereafter, the patient was free from her complaints, but progressed to third degree AV block in the second year of follow-up.
Case
In April 2008, a 40-year-old nurse with known HIV infection (no intravenous drug use) since 1991 presented with new onset of exertional dyspnea, chest tightness and dizziness for one month ago. Whilst climbing stairs, the patient had recently begun to need to pause for breath. She complained about mild allergic coryza during springtime, but so far asthma had not been observed. Fever and shivering as well as palpitations, irregular pulse and syncope were denied. No cardiovascular risk factors (smoking, diabetes, hypertension, hypercholesterolemia, myocardial infarction in family history) were present. Antiretroviral treatment for HIV had been stopped in February 2007 due to allergic reaction and toxic liver failure, and the patient currently took no medication at all.
Clinical examination showed an afebrile patient in a good general condition with a low regular pulse (44 bpm) and normal blood pressure (109/59 mm Hg). Heart and lung auscultation were normal, and there was no edema or jugular ingurgitation. Varicosis was present, but no calf tenderness, and no lymphadenopathy.
No acute onset of dyspnoea and lack of risk factors argued against pulmonary embolism. With haemoglobin level at 118 g/L, anaemia could not explain the symptoms. Inflammation markers (leucocytes 4.7 g/L, CRP 5 mg/L), cardiac enzymes and serum lactate dehydrogenase (LDH, sensitive marker for PCP [Pneumocystis jiroveci pneumonia]) were normal. Resting ECG showed sinus bradycardia, but no ischaemia (Figure 1). No electrolyte disorders or thyroid dysfunction could be found. In the absence of antiretroviral therapy, the CD4 count had dropped to 270/μL (20%), but was still above the threshold of 200/μL, below which opportunistic infections like Pneumocystis jiroveci pneumonia (PCP) become more likely. A chest X-ray yielded a normal result (no interstitial infiltrates, no cardiac enlargement).
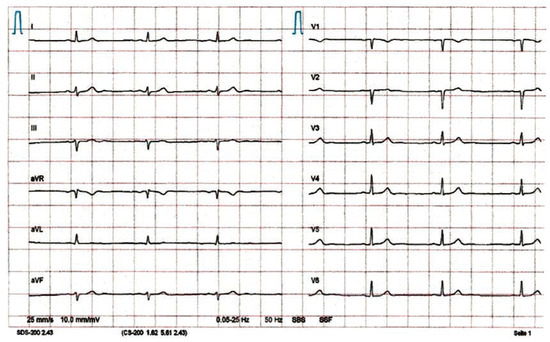
Figure 1.
Resting ECG: Sinus bradycardia 44 bpm, but no ischaemia.
To rule out exercise-induced asthma, lung function with the methacholine challenge test was performed which showed no abnormalities. As pulmonary hypertension constitutes one of the differential diagnoses of dyspnea in HIV-patients, the next step was echocardiography—again with normal result (no valvular defect, normal ejection fraction).
Finally, spiroergometry revealed a cardiac dysrhythmia as the cause of the patient’s symptoms. During the bicycle stress test with sufficient work load, dyspnoea, chest tightness and dizziness were associated with chronotropic incompetence (no appropriate increase of heart rate) (Figure 2). The corresponding ECG showed exercise-induced second degree 3:1 AV block (Figure 3). Intermittent second degree 2:1 AV block was documented with 24-h Holter monitoring a couple of days later (mean heart rate 48 bpm, minimum 33 bpm, maximum 73 bpm) (Figure 4).
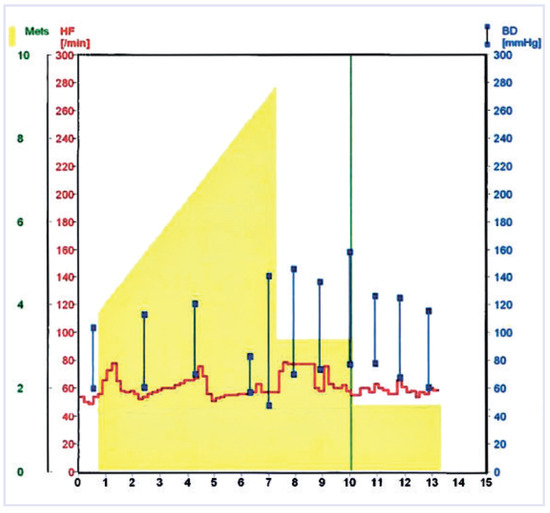
Figure 2.
Ergometry/Bicycle stress test: sufficient work load (120 watts, 9.2 METs [MET = metabolic equivalent, yellow area, green numbers], dyspnoea and dizziness at termination of the test), but no increase of heart rate (red line) and insufficient increase of blood pressure (blue).
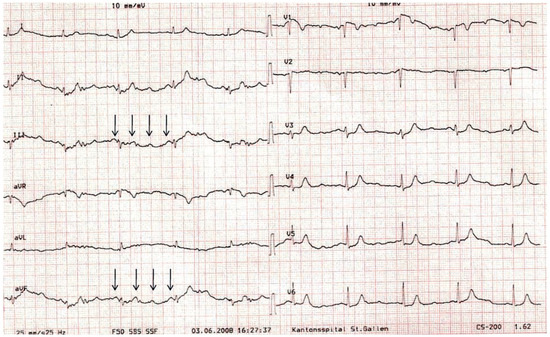
Figure 3.
ECG of the bicycle stress test shown in Figure 2 (minute 6): second degree 3:1 AV block (best seen in lead V1, II, III, aVF; arrows show P waves). QRS of conducted beats (57 bpm; sinus rate (P waves): 171 bpm) is not wide suggesting possible location of the block in the His bundle.
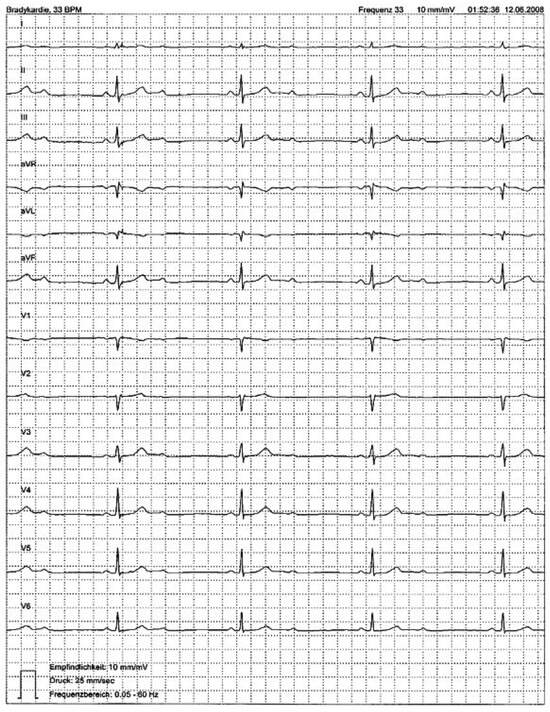
Figure 4.
24-h Holter monitoring: second degree 2:1 AV block (heart rate: 33 bpm; sinus rate [P-waves]: 66 bpm).
Borreliosis as a treatable cause of atrioventricular block could be excluded (negative serology). In June 2008 (i.e., three months after the onset of dyspnoea), a DDD pacemaker (SJM Zephyr XL DR) was implanted (stimulation, whenever heart rate <50 bpm). Thereafter, the patient was free of complaints. The proportion of ventricle stimulation increased over time, from 25% in October 2008 to 81% in February 2010 (progression to third degree atrioventricular block). With regard to the HIV, in August 2008, another antiretroviral therapy was initiated which is currently effective and well tolerated.
Discussion
Extensive diagnostic work-up including anamnesis, clinical examination, laboratory analyses, rest ECG, chest X-ray, lung function with methacholine challenge test and echocardiography was frustrating for this middle-aged HIV-infected woman with a new onset of effort dyspnoea, chest tightness and dizziness. It was not until a bicycle stress test was performed that the underlying exercise-induced second degree 3:1 AV block could be diagnosed.
Major causes of AV block are increased vagal tone (e.g., due to athletic training, sleep), fibrosis and sclerosis of the conduction system (50%) [1] (Lev’s disease in older and Lenegre’s disease in younger patients), ischaemic heart disease (40%) [1], cardiomyopathy and myocarditis (including borreliosis [2,3]), congenital heart disease, familial AV block, hyperkalaemia, infiltrative malignancies (e.g., lymphoma), neonatal lupus syndrome, severe hypo- or hyperthyreoidism, trauma, degenerative neuromuscular diseases, antiarrhythmic drugs, cardiac surgery or catheter ablation of arrhythmias.
The AV node is relatively resistant to permanent injury by infarction or infection, and normal function can be recovered over time. Permanent damage occurs more readily to the bundle of His [4]. Second degree AV block Mobitz type I (Wenckebach block) is mostly localised above the His bundle and often reversible, whereas second degree AV block Mobitz type II is mostly intra- or infra-Hissian and thus irreversible. In the case of 2:1 conduction (Figure 4), when prolongation of the PR interval before the block cannot be assessed, atropine test or exercise ECG testing can help to differentiate between second degree AV block type I and II. In type I, AV conduction improves with a prolongation of the Wenckebach periodic (or transition to first degree AV block). In type II, AV conduction deteriorates with transition to 3:1 or 4:1 block, as observed in our patient (Figure 3).
Since symptomatic AV block is a recognised indication for pacemaker implantation irrespective of the anatomical localisation [5], further examinations specifying the site of the AV block (e.g., electrophysiology study with His bundle ECG) would have been only of academic value. After ruling out reversible/treatable causes (negative borreliosis serology, normal electrolytes and TSH, normal inflammation markers and cardiac enzymes, no medication, no prior cardiac invasive procedure) a dual chamber pacemaker was implanted, resolving the patient’s symptoms. During the second year of follow-up, progression to third degree AV block was observed.
Given the young age of the patient and the course of the disease, Lenegre’s disease (progressive, fibrotic, sclerodegenerative affliction of the conduction system in younger individuals) [6] seems the most probable diagnosis. Basically, familial AV block [7] must be considered too, but the patient’s family history was not suggestive of a hereditary aetiology.
However, cardiac dysrhythmia is not the first thing to consider in an untreated HIV-positive patient with dyspnoea on exertion. Particularly, in the case of advanced immunosuppression (i.e., CD4 count <200/μL), Pneumocystis jiroveci pneumonia (PCP) forms a major differential diagnosis [8].
Nevertheless, patients with advanced HIV infection can also have a variety of cardiovascular manifestations including pericarditis, myocarditis, cardiomyopathy, pulmonary vascular disease and pulmonary hypertension, valvular disease (e.g., due to endocarditis in intravenous drug users) and an increased incidence of vascular disease including premature coronary atherosclerosis [9]. Besides, a 24-h Holter monitoring study in 21 HIV-infected patients revealed an unexpectedly high incidence of conduction disturbances: one patient (4.8%) with intermittent Mobitz type I second degree AV block, two patients (9.5%) with paroxistic 2:1 AV block and one patient (4.8%) with a bifascicular block [10]. Electrocardiogramm abnormalities including new onset atrioventricular block and bundle branch block resulted in premature termination of a study of concurrent atazanavir- and lopinavir/ritonavir-treatment in HIV patients with extensive antiretroviral resistance [11]. However, the patient depicted in this case report had not taken antiretroviral drugs for more than one year, when her symptoms appeared.
Whether the progressive atrioventricular conduction disturbance in the presented case is idiopathic (Lenegre’s disease) or associated with HIV-infection remains unclear (no biopsy or MRI was performed). Irrespective of HIV infection, spiroergometry has proven to be a useful second-stage diagnostic tool to differentiate between respiratory and cardiovascular system effort dyspnoea, if the initial evaluation with standard tests is non-diagnostic.
Conflicts of Interest
The authors have no conflict of interest to disclose.
References
- Zoob, M.; Smith, K.S. The aetiology of complete heart-block. Br Med J. 1963, 5366, 1149. [Google Scholar]
- Lelovas, P.; Dontas, I.; Bassiakou, E.; Xanthos, T. Cardiac implications of Lyme disease, diagnosis and therapeutic approach. Int J Cardiol. 2008, 129, 15–21. [Google Scholar]
- Pasquier, M.; Péter, O.; Frochaux, V.; Imsand, C.; Vogt, P.; Girod, G. Atrioventricular heart block in Lyme disease. Rev Med Suisse. 2006, 2, 415–417. [Google Scholar]
- Mangrum, J.M.; Dimarco, J.P. The evaluation and management of bradycardia. NEJM 2000, 342, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Lemke, B.; Nowak, B.; Pfeiffer, D. Leitlinien zur Herzschrittmachertherapie. Z Kardiol. 2005, 94, 704–720. [Google Scholar] [CrossRef]
- Le Guludec-Chéron, D.; Sebag, C.; Davy, J.M.; Lainé, J.F.; Slama, M.; Kevorkian, M.; et al. Infranodal chronic auriculo-ventricular block in subjects under 50 years of age. Arch Mal Coeur Vaiss. 1986, 79, 23–29. [Google Scholar]
- Probst, V.; Kyndt, F.; Potet, F.; et al. Haploinsufficiency in combination with aging causes SCN5A-linked hereditary Lenegre disease. J Am Coll Cardiol. 2003, 41, 643. [Google Scholar] [CrossRef]
- Wallace, J.M.; Hansen, N.I.; Lavange, L.; Glassroth, J.; Browdy, B.L.; Rosen, M.J.; et al. Respiratory disease trends in the pulmonary complications of HIV infection study cohort. Am J Respir Crit Care Med. 1997, 155, 72. [Google Scholar] [CrossRef] [PubMed]
- Sudano, I.; Spieker, L.E.; Noll, G.; Corti, R.; Weber, R.; Lüscher, T.F. Cardiovascular disease in HIV infection. Am Heart J. 2006, 151, 1147–1155. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, J.; Mota-Miranda, A.; Cruz, A.; Gomes, M.H.; Oliveira, P.; Rocha-Gonçalves, F.; et al. Dysrhythmic profile of human immunodeficiency virus infected patients. Int J Cardiol. 1995, 49, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Rathbun, C.R.; Liedtke, M.D.; Blevins, S.M.; Harrison, D.; Lockhart, S.M.; Salvaggio, M.; et al. Electrocardiogram abnormalities with atazanavir and lopinavir/ritonavir. HIV Clin Trials. 2009, 10, 328–336. [Google Scholar] [CrossRef] [PubMed]




© 2010 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.