Summary
We report a case of percutaneous coronary intervention complicated by guide wire entrapment secondary to incidental stent crushing after unprompted stent recoil. The guide wire could be successfully removed together with the stent by contraction of the latter. This case illustrates one latent risk of acute stent recoil and the subsequent management of this unusual complication.
Case report
A 65-year-old female was admitted at our institution with acute infero-posterior ST segment elevation myocardial infarction. She complained of typical chest pain starting 6 hours before admission. Her known cardiovascular risk factors were diabetes mellitus, dyslipidaemia, arterial hypertension and current smoking (40 pack-years). She underwent coronary angiography, which revealed a thrombotic occlusion of the right coronary artery (RCA), a high-grade stenosis of the left anterior descending artery (LAD) and two high-grade stenosis of the circumflex artery (LCx). The RCA was promptly recanalised and a second percutaneous coronary intervention procedure was planed one week later.
During this second intervention, the control angiography demonstrated a good result in the RCA and PCI of the LAD (Figure 1A [arrow], 1B, 1C) was performed with implantation of one 2.5/12-mm-everolimuseluting stent (Promus®, Boston Scientific, USA) and good final angiographic result. Subsequently, the serial high-grade stenosis of the LCx were undertaken (Figure 1D, 1F). The distal lesion of the LCx was predilated with a 2.5/14-mm-balloon (Falcon®, Invatec, Italy) and a 2.25/12-mm-everolimus-eluting stent (Promus®, Boston Scientific, USA) was implanted. The proximal lesion was then pre-dilated with the same material and a 2.75/15-mm-everolimus-eluting stent (Xience V®, Guidant Corporation, USA) was implanted with 14 atm. During PCI of the proximal lesion, a second guide wire was positioned into a 2 mm first obtuse marginal branch (OM1) and was jailed to the wall by the stent strut. Accordingly to the provisional T-stenting technique, both guide wires were then exchanged: the BMW® (Abbott Vascular, USA) guide wire was advanced into the OM1 while the Whisper® LS (Abbott Vascular, USA) guide wire was retrieved (Figure 2A). At this step, some recoil (Figure 2B, asterisks) in the stent was noted. A 1.5/10-mm-balloon (TIN®, Schwager Medica, Switzerland) was advanced, but some resistance was noted and the balloon stayed stacked into the left main coronary artery (Figure 3A). Thereafter, retrieval of the BMW® guide wire was no more possible and the proximal struts of the stent seemed compacted against the OM1 take-off (Figure 3B). Next, a 0.014″ Choice PT Extra Support® (Boston Scientific, USA) guide wire was advanced but failed to cross the stent lumen and passed between the stent and the vessel’s wall. The Whisper® LS guide wire was positioned into the LAD to increase anchoring power and protect the LAD in potential complication of left main coronary artery. Three inflations with 10 atm were performed along the stent, which induced back crushing of the stent (fig. 3C). This latter allowed mobilisation and retrieval of both the jailed BMW® guide wire and the compacted stent into the guiding catheter. The ex vivo macroscopic examination of the material demonstrated a complex entrapment of the guide wire in the stent struts (Figure 4A). Finally, a new 2.75/15-mm-everolimus-eluting stent (Xience V®, Abbott Vascular, USA) could be implanted in the initial position. A control angiography showed no dissection or perforation. The final result was satisfactory. Recovery was uneventful and the patient was discharged after 2 days. Acetylsalicylic acid was prescribed lifelong, and clopidogrel was prescribed for 12 months.
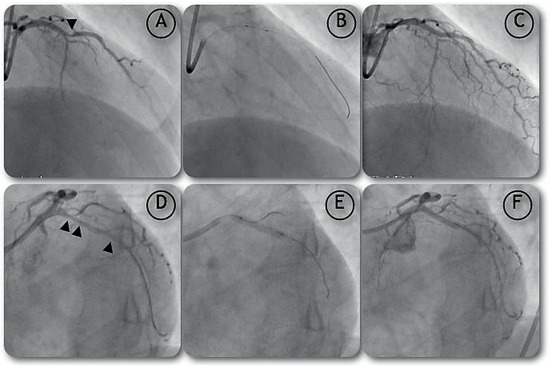
Figure 1.
Initial percutaneous coronary interventions. A. RAO cranial view demonstrating a high grade stenosis of the LAD artery (arrow). B. Percutaneous coronary intervention with one 2.5/12-mm-everolimus-eluting stent. C. Final result. D. LAO caudal view with serial high-grade stenosis of LCx. E. Percutaneous coronary intervention of the proximal stenosis with one 2.75/15-mm-everolimus-eluting stent. F. Angiographic result after stent implantation in proximal LCx.
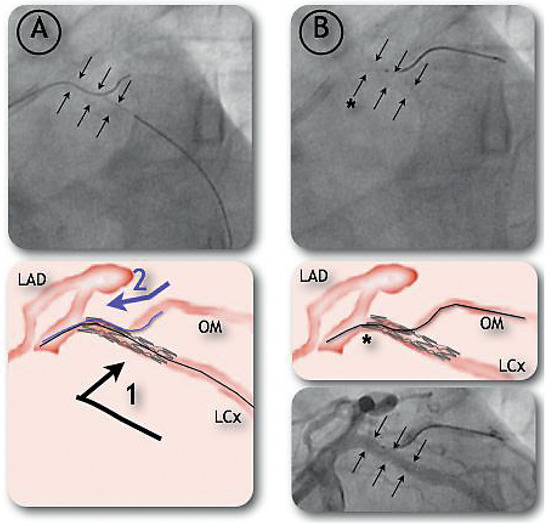
Figure 2.
Angiographic and schematic illustrations of the percutaneous coronary intervention of the proximal stenosis of circumflex artery (LCx) after stenting (delineated by the arrows). A. According to the “provisional T-stenting technique”, the BMW® guide wire (black, 1) was retrieved from distal LCx and intro duced into the first obtuse marginal branch (OM). Then, the Whisper® guide wire (blue, 2) was removed. B. At this point, some stent recoil was noted (asterisks), with a suboptimal result in both branches (LCx, OM; bottom).
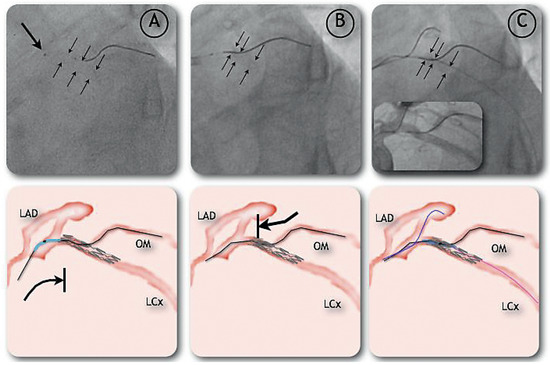
Figure 3.
Angiographic and schematic illustrations of the guide wire entrapment and its jailbreak using reverse crush technique. A. Some resistance was noted by advancing the 1.5/10-mm-balloon, which finally got stacked into the left main coronary artery. B. At this point, retrieval of the BMW® guide wire (black) was no more possible and changes in the stent geometry was noted with compaction of proximal struts towards OM (first obtuse marginal branch) take-off. C. Deflation of the stent: A 0.014” Choice PT Extra Support guide wire (pink) was advanced into LCx but failed to cross the stent lumen. The Whisper® guide wire (blue) was positioned into the LAD in order to increase anchoring. The 1.5/10-mm-TIN®-balloon was then mounted on the Choice PT® guide wire and its inflation led to back crushing and partial deflation of the stent.
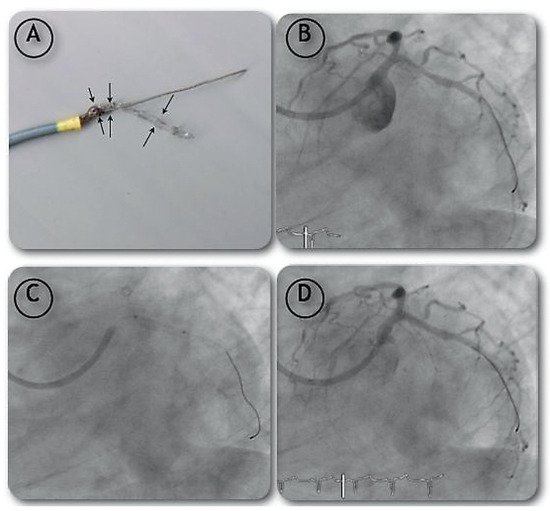
Figure 4.
New stent implantation and final result. A. Ex vivo examination of the retrieved material demonstrating a complex entrapment of the guide wire in the stent struts. B. Angiographic result at this point. C. Successful implantation of a new 2.75/15-mm-everolimus-eluting stent. D. Final result.
Discussion
In order to limit the risk of side-branch occlusion and subsequent peri-interventional infarction, balloon dilatation of side-branch ostium through the stent strut mesh opening is an accepted technique when a metallic stent is placed over secondary branches take-off. The present case report underlines the risk of disturbing the normal stent architecture by crushing some stent struts while introducing the balloon.
This extensive stent strut deformity was here preceded by stent recoil. This case report therefore also emphasises one of the possible dangers of acute recoil, and demonstrates once again [1] that new generations of drug-eluting stents with thinner stent struts are especially at risk.
Finally, it shows that partial deflation of an underexpanded stent is feasible and could be attempted in such cases. On one hand, stent dislodgement and/or embolisation occur from time to time. In such cases, various techniques have been anecdotally reported so far with an overall success rate from 71 to 86% [2,3]. Retrieval techniques included passing through the stent with a low-profile angioplasty balloon catheter or Basket retrieval device, twirling two guide wires around the stent, use of dedicated devices such as gooseneck snare and Cook retained fragment retrieval device, or finally use of materials made for other purposes, such as myocardial biopsy or biliary forceps. In some cases, stent deployment or crushing may be a good alternative to retrieval [3]. On the other hand, guide wire entrapment is very rare and is usually followed by guide wire rupture after a too brisk pull away manoeuvre from an exhausted operator. The present case report testifies that – even when serendipitous – a gentle deflation of the stent by reverse crushing could help to retrieve a stacked stent and may save both time and exasperation.
Conflicts of Interest
There is no conflict
of interest.
References
- Baeriswyl, B.; Adorjan, P.; Cook, S. Caught up, then pushed down: the tribulations of one underexpanded coronary stent. Kardiovaskuläre Medizin. 2007, 10, 366–369. [Google Scholar]
- Eggebrecht, H.; Haude, M.; von Birgelen, C.; Oldenburg, O.; Baumgart, D.; Herrmann, J.; et al. Non surgical retrieval of embolized coronary stent. Catheter Cardiovasc Interv. 2000, 51, 432–440. [Google Scholar] [PubMed]
- Brilakis, E.S.; Best, P.J.; Elesber, A.A.; Barsness, G.W.; Lennon, R.J.; Holmes, D.R., Jr.; et al. Incidence, retrieval methods, and outcomes of stent loss during percutaneous coronary intervention: a large single-center experience. Catheter Cardiovasc Interv. 2005, 66, 333–340. [Google Scholar] [CrossRef] [PubMed]




© 2009 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.