Case Description
A 47-year-old female presented sudden loss of consciousness. On the arrival of the medical team the initial cardiac rhythm was ventricular fibrillation, which was successfully treated with cardiopulmonary resuscitation (CPR) and electric defibrillation. Her ECG on admission is shown below (Figure 1). A transthoracic echocardiogram showed a severely dilated and akinetic right ventricle (RV) as well as a severely hypokinetic left ventricle (Figure 2). Pulmonary embolism complicated with sudden cardiac death was suspected, and the patient was treated by intravenous thrombolysis.
Do you agree with the diagnosis of pulmonary embolism?
What is your interpretation of the ECG?

Figure 1.
Twelve-lead ECG of a 47-year-old female following resuscitated sudden cardiac death.


Figure 2.
Transthoracic echocardiogram performed on admission. Parasternal short axis (A) and apical four-chamber (B) views showing a severely dilated right ventricle.

Discussion
A subsequent thoracic CT-scan showed a right inferior segmentary pulmonary embolism; it also confirmed dilatation of the RV, but additionally revealed the presence of a thrombus at the apex of the RV which had not been visualised on the echocardiogram.
However, after review of the ECG, arrhythmogenic right ventricular cardiomyopathy (ARVC) was also suspected. Indeed, leads V1 to V4 show prominent epsilon waves at the end of the QRS complex, which reflect delayed activation of the RV and are highly suggestive of ARVC (although in rare cases they have been described with other diseases such as sarcoidosis, Brugada syndrome and RV infarction) [1,2,3,4]. Furthermore, inverted T waves are seen not only in V2 and V3, also characteristic of ARVC (and likewise compatible with right ventricular pressure overload, as with pulmonary embolism), but also in V4 to V6, which correlates with left ventricular involvement [5]. Finally, other findings suggestive of ARVC in this ECG include QRS duration >110 msec and reduced R waves in V1 to V3, as well as the presence of a premature ventricular complex with a left bundle branch pattern (indicating a right ventricular origin), which can be seen in the precordial leads [1,6].
Along with the clinical events, ECG and echocardiographic findings, cardiac magnetic resonance imaging (Figure 3) and single-averaged ECG confirmed the diagnosis of ARVC. The subsequent hospital stay was marked by full haemodynamic and neurological recovery, and the patient received an implantable cardioverter-defibrillator. She was discharged on betablockers, angiotensin-converting enzyme inhibitors and anticoagulation therapy.
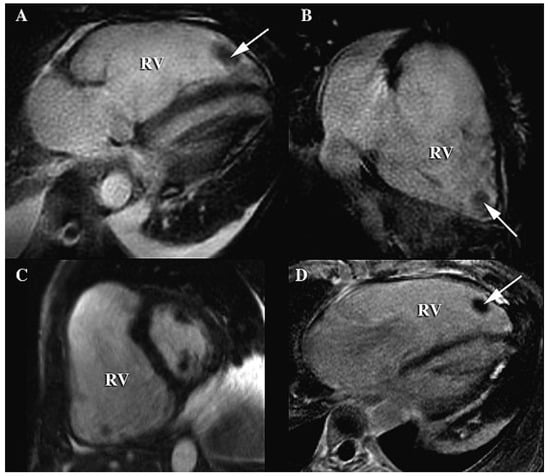
Figure 3.
Cardiac magnetic resonance imaging; cine SSFP sequences in four-chamber (A), two-right-chamber (B) and short-axis (C) views showing massive dilatation of the right ventricle (RV) with global thinning of the anterior wall and a severely diminished ejection fraction (20%). Paradoxical motion of the interventricular septum was also demonstrated, with protrusion of the septum towards the left ventricle, clearly visible during early diastole on C. The small thrombus at the apex of the RV seen on the CT-scan was also present (arrows) and was particularly visible on the late-enhancement (PSIR) sequence in the four-chamber view (D).
The present case is remarkable for several features. First and foremost is the extremely severe extent of the ARVC in this patient, with massive dilatation of the right ventricle and also involvement of the left ventricle. Moreover, this translated into a caricatural aspect of the ECG, with giant epsilon waves and T wave inversion in all precordial leads. Finally, the patient was admitted with pulmonary embolism, which is a rare but known complication of ARVC [7]. The emboli most certainly originated from the RV thrombus, and possibly contributed to triggering the ventricular arrhythmia due to the sudden increase in afterload in an already impaired RV. Alternatively, the thrombus may have migrated to the lungs following CPR and electric defibrillation, after ventricular fibrillation solely secondary to the ARVC. Of note, the CT scan showed only segmentary pulmonary embolism, but was performed after the administration of thrombolysis, which probably dissolved most of the emboli and therefore possibly led to underestimation of the initial extent of the embolic event.
Conflicts of Interest
The authors report no conflict of interest.
References
- Gemayel, C.; Pelliccia, A.; Thompson, P.D. Arrhythmogenic right ventricular cardiomyopathy. J Am Coll Cardiol. 2001, 38, 1773–1781. [Google Scholar] [CrossRef] [PubMed]
- Santucci, P.A.; Morton, J.B.; Picken, M.M.; Wilber, D.J. Electroanatomic mapping of the right ventricle in a patient with a giant epsilon wave, ventricular tachycardia, and cardiac sarcoidosis. J Cardiovasc Electrophysiol. 2004, 15, 1091–1094. [Google Scholar] [CrossRef] [PubMed]
- Ozeke, O.; Cavus, U.Y.; Atar, I.; Ozin, B.; Ilkay, E. Epsilon-like electrocardiographic pattern in a patient with Brugada syndrome. Ann Noninvasive Electrocardiol. 2009, 14, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Zorio, E.; Arnau, M.A.; Rueda, J.; Almenar, L.; Osa, A.; Martínez-Dolz, L.; Osca, J.; Palencia, M.A. The presence of epsilon waves in a patient with acute right ventricular infarction. Pacing Clin Electrophysiol. 2005, 28, 245–247. [Google Scholar] [CrossRef] [PubMed]
- Corrado, D.; Basso, C.; Thiene, G.; McKenna, W.J.; Davies, M.J.; Fontaliran, F.; Nava, A.; Silvestri, F.; Blomstrom-Lundqvist, C.; Wlodarska, E.K.; et al. Spectrum of clinico-pathologic manifestations of arrhythmogenic right ventricular cardiomyopathy/dysplasia.Amulticenter study. J. Am Coll Cardiol. 1997, 30, 1512–1520. [Google Scholar] [CrossRef] [PubMed]
- Sen-Chowdhry, S.; Lowe, M.D.; Sporton, S.C.; McKenna, W.J. Arrhythmogenic right ventricular cardiomyopathy: clinical presentation, diagnosis, and management. Am J Med. 2004, 117, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Wlodarska, E.K.; Wozniak, O.; Konka, M.; Rydlewska-Sadowska, W.; Biederman, A.; Hoffman, P. Thromboembolic complications in patients with arrhythmogenic right ventricular dysplasia/cardiomyopathy. Europace 2006, 8, 596–600. [Google Scholar] [CrossRef] [PubMed]

© 2009 by the author. Attribution - Non-Commercial - NoDerivatives 4.0