Summary
Ischaemic mitral regurgitation (IMR) is defined as functional MR with systolic re-striction of leaflet motion, apical and lateral displacement of the subvalvular appa-ratus, and annular dilatation in the presence of a morphologically normal mitral valve. IMR is usually caused by LV dilatation in the setting of ischaemic or idiopathic dilated cardiomyopathy (CMP). Left ventricular dilatation leads to dilatation of the mitral annulus and to apical and lateral displacement of one or both papillary muscles with tethering of the valve leaflets and consecutive IMR. Therefore, IMR begets IMR with a vicious cycle of increased volume load leading to ventricular dilatation, leading to more IMR etc. Although MR is thought to unload the LV, wall stress is increased due to LV dilatation according to Laplace’s law. IMR is therefore thought to be primarily a ventricular and not a valvular problem. IMR is known to be prognostically important irrespective of LV function and of IMR severity at rest, because it is very dynamic and sensitive to loading conditions. IMR may frequently be severe during daily activity inducing LV failure on the long term. Therefore, dynamic testing is becoming the method of choice for assessment of these patients. Medical therapy has been shown to be inferior to surgery in the setting of IMR. Although still controversial with regard to what surgical method may be best not only to correct IMR, but also to induce a change in LV size and shape—the so-called reverse remodeling—surgical treatment is indi-cated with a documented effective regurgitant orifice area (EROA) > 20 mm2 and a re-gurgitant volume (Rvol) > 30 mL by transthoracic echocardiography (TTE) at rest or with an increase of EROA > 13 mm2 in exercise TTE. Furthermore, intraoperative pro-vocative testing may help identify significant IMR. Correction of IMR is usually done by restrictive annuloplasty with aggressive undersizing of a conventional closed and semirigid annuloplasty ring. Improved LV function and a decreased need for cardiac transplantation has been seen in published series. With the advent of new rings and devices specifically designed for correction of IMR, results may further improve. Modern specific annuloplasty rings are designed to correct the down-and outward displacement of the subvalvular apparatus by inducing an acute valvular and ventricular reshaping. With the choice of various models, IMR may be corrected more precisely by selecting a type of ring according to the geometry of the regurgitant jet and the distor-tion of the valve leaflets. In case of ischaemic CMP, not only complete revascularisa-tion, but also resection of aneurysmatic myocardial scar tissue and surgical LV remod-eling is usually performed. With the help of new devices such as the ACORN CorCap® device further dilatation may effectively be prevented and may even improve LV func-tion in selected patients. Alternatively, cardiac transplantation, implantation of an as-sist device for destination therapy in patients not qualifying for cardiac transplanta-tion or resynchronisation therapy may be evaluated in very advanced cases.
Zusammenfassung
Die chronische ischämische Mitralinsuffizienz (iMI) ist definiert als funktionelle Mitralinsuffizienz hervorgerufen durch eine systolische Bewegungsbehinderung der Segel infolge Verlagerung des subvalvulären Apparates apikal und lateral, annulärer Erweiterung und morphologisch normalem Klappenapparat. Sie wird hervorgerufen durch eine regionale oder globale Dilatation des LV und begleitet häufig eine dilatative Kardiomyopathie oder eine KHK nach durchgemachtem Myokardinfarkt mit Remodeling. Die Präsenz einer chronischen bereits mässiggradigen iMI erhöht langfristig die kardiale Mortalität und das Risiko der Herzinsuffizienz erheblich. Sie sollte deshalb ab einer effective regurgitant orifice area (EROA) >20 mm2 oder einem Regurgitationsvolumen >30 mL, transthorakal echokardiographisch mittels PISA-Methode am wachen Patienten gemessen, behandelt werden. Die Korrektur der iMI wurde bis vor kurzem mittels sogenannter restriktiver Mitralanuloplastie vorgenommen, indem ein um zwei Grössen kleinerer konventioneller Anuloplastiering eingesetzt wurde. Damit sollte vor allem eine Reduktion des septolateralen Durchmessers erreicht werden, um die Verziehung der Segel in den Ventrikel, den sog. «tethering effect» auszugleichen. Erste klinische Resultate haben v.a. eine Abnahme der Notwendigkeit von Herztransplantationen und eine Verbesserung der LV-Funktion gezeigt. Allerdings war dieser Effekt nicht zuverlässig erzielbar und in vielen Fällen trat die iMI wieder auf. Mit der Neuentwicklung spezifischer Anuloplastieringe erhofft man sich wesentlich bessere Resultate und neueste Ergebnisse sind vielversprechend. Im Falle einer ischämischen Kardiomyopathie muss gleichzeitig eine vollständige Revaskularisation vorgenommen und ausgedehnte aneurysmatische Infarktnarben reseziert werden. Darüberhinaus kann mit dem ACORN-Netz zumindest eine weitere Dilatation des Herzens verhindert und in ausgewählten Fällen auch eine Verbesserung der LV-Funktion erreicht werden. Ausgewählte Patienten profitieren auch von einer Resynchronisationstherapie. Bei fortgeschrittenen Formen mit schwerer Dilatation und schwer eingeschränkter LV-Funktion muss alternativ die Herztransplantation oder ein Kunstherz zur sogenannten «destination therapy» erwogen werden.
Schlüsselwörter: Kardiomyopathien; Herzchirurgie; Mitralklappe
Background
Ischaemic mitral regurgitation (IMR) is defined as functional MR in the presence of a morphologically normal mitral valve. Common features of IMR are systolic restriction of leaflet motion (the so-called tethering effect), apical and lateral displacement of the subvalvular apparatus, annular dilatation and normal valve morphology (Figure 1A). Typically, patients with IMR present with LV dilatation and impaired systolic function in the setting of ischaemic or idiopathic dilated cardiomyopathy (CMP). Left ventricular dilatation leads to dilatation of the mitral annulus and to apical and lateral displacement of one or both papillary muscles with tethering of the valve leaflets and consecutive IMR. IMR is therefore thought to be primarily a ventricular and not a valvular problem. With idiopathic dilated CMP, dilatation is usually symmetrical, resulting in symmetrical mitral distortion and a central jet (Figure 1A,B). With ischaemic CMP an asymmetrical jet with tethering of the P3 segment of the mitral valve due to inferior infarction is frequently present (Figure 1C). However, a central jet may also be seen years after myocardial infarction with global ventricular dilatation due to remodeling. While acute IMR is thought to be frequent in the setting of AMI and may resolve spontaneously in milder forms [1], the prevalence of chronic IMR persisting after 6 weeks [2] is largely unknown. Its presence however, is known to significantly impair patient survival and increase the risk of congestive heart failure [1,3,4]. Clinically, patients may be asymptomatic with respect to IMR, presenting perhaps signs of myocardial ischaemia in coronary artery disease, but may also be symptomatic with dyspnea or signs of congestive heart failure in the most severe cases with impaired LV function, severe IMR and severely dilated LV.
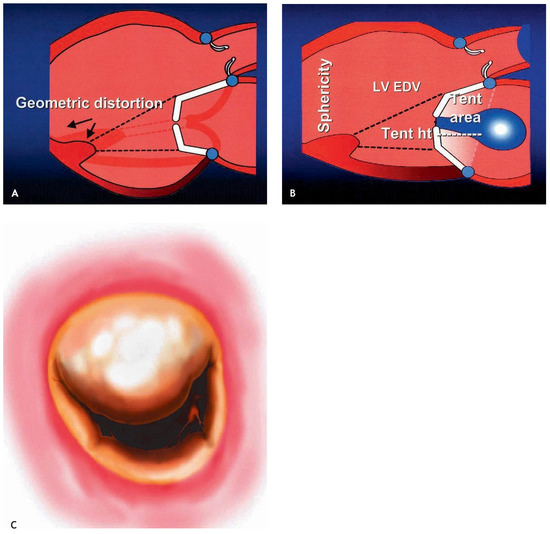
Figure 1.
(A) Ischaemic MR caused by geometric distortion of the valve following LV dilatation with apical and lateral displacement of the papillary muscle apparatus. (B) Ventricular displacement of the leaflets creates an area called tenting area with the tenting height (tent ht), an index of severity of valvular tethering. (LV EDV = LV enddiastolic volume). (C) Surgical view of the mitral valve from the left atrium demonstrating typical tethering of P3 in ischaemic cardiomyopathy following inferior myocardial infarction, resulting in IMR with an asymmetrical jet.
Echocardiographic evaluation
Echocardiographic assessment is the most important tool for the evaluation of mitral valve morphology and function. Usually, transthoracic echocardiography (TTE) provides accurate information on the severity of mitral regurgitation. However, grading of MR into mild, moderate and severe does not provide sufficient information, nor simple estimation of the severity based on visual impression of the regurgitant jet. Instead quantification of MR, preferentially by the PISA method, calculating EROA and RVol, should always be performed, if possible. Limitations of the PISAmethod are well recognised [5,6], being more accurate for central than eccentric regurgitant jets, and a circular than non-circular orifice. Flow convergence should be optimised from an apical view using a zoom mode. Results vary widely for calculations at different aliasing velocities and care must be taken to use the velocity at which the hemispheric formula applies best. Furthermore, for determination of EROA, it is essential that the CW Doppler signal be well aligned with the regurgitant jet [6]. The severity of MR should be assessed in the awake patient by TTE, because of representative afterload conditions. This is true for all mechanisms of MR, which may be reduced by sedation or general anaesthesia for TOE, except for MR due to a flail leaflet, which has been shown to be largely unaffected by afterload reduction with anesthesia [7,8]. Especially IMR is very dynamic in its severity and should be assessed under proper loading conditions in the awake patient. Based on the studies of the Mayo Clinic [3], demonstrating impaired survival depending on the severity of IMR, surgical correction of IMR is already indicated with EROA > 20 mm2 and RVol >30 mL, which represents half the values for surgery in all other aetiologies of MR (corresponding to moderate MR). In addition, another study by Lancelotti et al. [4] has shown, that an increase of EROA >13 mm2 in exercise TTE indicates prognostically important IMR in patients with EROA <20 mm2 provided by resting TTE.
In patients without or insufficient preoperative echoardiographic evaluation an intraoperative loading test may be performed [9,10,11] (Figure 2). Future studies will have to elucidate, how patients with IMR will best be selected for surgical correction. To avoid overlooking an important IMR, all patients scheduled for coronary revascularization, whether it be interventionally or surgically, should undergo TTE assessment. Suspicion should be high in patients with a history of inferoposterior or anterior infarction, impaired LV function (EF <45%), enlarged LV and dyspnea as the leading symptom and IMR aggressively sought after. Assessment of the symmetry of the jet and the tethering is helpful for surgical evaluation and selection of the type of annuloplasty ring [12,13,14].
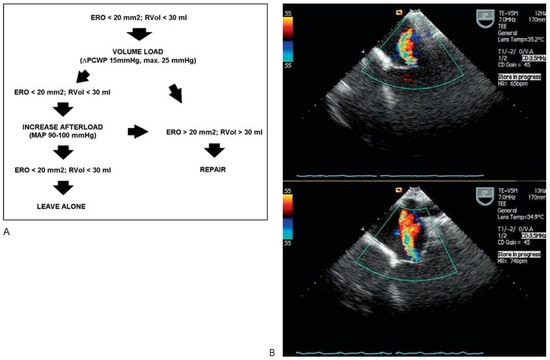
Figure 2.
(A) Protocol of the intraoperative loading test. Rapid filling to increase preload conditions is performed after aortic cannulation with the aid of the cardiopulmonary bypass machine. (B) Assessment of changes in IMR by transoesophageal echocardiography before (above) and during the loading test (below), showing significant worsening of IMR, indicating the need for surgical correction. ERO = effective regurgitant orifice area; MAP = mean arterial pressure; PCWP = pulmonary capillary wedge pressure; RVol = regurgitant volume.
Indications and surgical techniques for correction of ischaemic MR
Indications for correction of IMR and the best technique to be used are still controversial. However, surgical correction of IMR may be based on several notions: Various studies have demonstrated, that patients with IMR have a significantly worse outcome with regard to cardiac death and rehospitalisations because of heart failure than patients without [3,4,15,16]. To date, the notion that important IMR will not resolve spontaneously after coronary revascularisation is gaining progressive acceptance [15,17,18,19]. It may even worsen significantly after revascularisation alone [2]. Furthermore, several studies have shown, that revascularisation alone, either surgically or interventionally without addressing IMR results in impaired patient outcome [2,18,19]. On the other hand, many studies have demonstrated, that not only does correction of IMR not add to the risk of surgery [18,20], but also has a positive effect, at least on the short and mid term postoperatively [17,18,19,21]. Furthermore, interventional or surgical revascularisation is superior to medical therapy alone concerning long-term outcome in this setting [22].

Table 1.
Patients’ baseline characteristics.
Table 1.
Patients’ baseline characteristics.
 |
IMR may present within a broad clinical spectrum. On one hand, it may be only mild and accompany CAD with preserved LV function, normal LV size and predominantly angina pectoris. In this situation, myocardial revascularisation alone would suffice. On the other hand, IMR may be severe in the setting of ischaemic CMP with severely impaired LV function, dilated LV and predominantly clinical signs of heart failure. In this situation, treatment should not be restricted to myocardial revascularisation alone, but include restoration of mitral valve function [9,10] (class IIB recommendation of the ACC/AHA Guidelines [23]). Treatment of IMR in patients presenting in between these two extremes is still controversial and subject of ongoing debate. However, there are data to indicate benefit from MV repair in such patients [2,19,23]. We, like others [3] address IMR whenever an EROA >20 mm2 or RVol >30 mL is demonstrated in the awake patient in the setting of chronic ischaemia, present at least 6 weeks after acute myocardial infarction [2]. Therefore, IMR earlier after acute myocardial infarction or in the setting of an acute coronary syndrome is only addressed surgically when deemed severe (EROA >40 mm2, RVol >60 mL), since milder forms of MR are frequent in up to 60% of patients and may resolve spontaneously [1]. Correction of IMR was until now primarily addressed by aggressive undersizing of a conventional closed and semirigid annuloplasty ring [21], performing a so-called restrictive annuloplasty, preferably with a rigid closed annuloplasty ring [24] (Figure 3). Use of open or flexible rings are associated with an unacceptably high recurrence rate [25]. Some authors have advocated additional chordal cutting [26], relocation of the posterior PM by a traction suture [27], posterior leaflet patch extension or application of the Alfieri stitch [28] for correction of IMR. However, none of these various techniques have found widespread use, probably due to the production of unpredictable results and a lack of long-term data on durability and efficacy [27]. Early results reported by the Cleveland Clinic using restrictive annuloplasty alone have shown a decreased need for cardiac transplantation and improved LV function. However, just by eliminating MR not all LVs responded with a clinically beneficial re-remodeling and in many patients MR reoccurred [21,29]. With vigorous down-sizing, MR recurrence could be reduced in recent series [21] and LV function was shown to improve consistently [17]. With the advent of new rings and devices specifically designed for correction of IMR, results may further improve [30]. Modern specific annuloplasty rings (Figure 4) are designed to correct the down-and outward displacement of the subvalvular apparatus caused by LV remodeling by in- and upward reshaping at the anular level. Interestingly, computer animated simulations showed decreased stress forces on the subvalvular apparatus and the leaflets after correction than before, and instant spherical reshaping and a decrease in size of the LV in animal and early clinical studies [Alfieri et al.; unpublished data]. Furthermore, the most recently developed Geoform ring (Edwards Lifesciences Inc., Irvine, CA, USA) is thought to equally well address the usually more central MR seen in dilated cardiomyopathy (CMP) and the usually more posteriorly excentric MR in ischaemic CMP. These specific rings should be implanted without down-sizing and with deep well-anchored sutures along the mitral annulus.
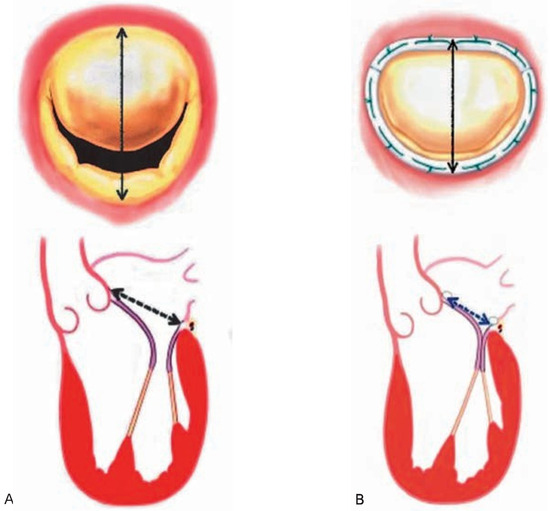
Figure 3.
Principles of restrictive annuloplasty. (A) Presence of annular dilatation and symmetrical tethering of the anterior and posterior leaflet resulting in loss of coaptation surface and central IMR. (B) Implantation of a down-sized rigid annuloplasty ring reduces the septo-lateral distance, thus allowing the valve to close correctly again, abolishing IMR.
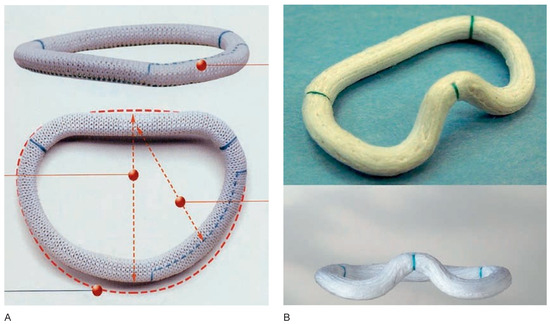
Figure 4.
Modern specific IMR annuloplasty rings. (A) The Etlogix annuloplasty ring (Edwards Lifesciences Inc., Irvine, CA, USA) designed for correction of asymmetrical IMR. Tethering of P3 is counteracted by reduction of the septo-lateral diameter between A2 and P2 by 25% and between A2 and P3 by 33% in comparison to a conventional annuloplasty ring, and by a relative downward shifting of the annulus at P3. (B) The GeoForm annuloplasty ring (Edwards Lifesciences Inc., Irvine, CA, USA) designed for correction of symmetrical IMR. With its bone-shaped design, septo-lateral distance is maximally reduced. The three-dimensional design of the ring counteracts the apical downand outward displacement of the subvalvular apparatus and the LV wall, leading to an acute reverse remodeling of the LV and to a competent valve.
Despite the advent of these new technologies, the question remains, if a severely dilated LV should be treated with additional measures. Threshold values for LV dilatation may be used to select those patients probably responding well to mitral annuloplasty alone from those with irreversible LV dilatation and impaired function [13]. In case of ischaemic CMP, not only complete revascularisation, but also resection of aneurysmatic myocardial scar tissue and surgical LV remodeling as proposed by Dor [31] should be performed. Furthermore, by wrapping the heart with the ACORN CorCap® device further dilatation can effectively be prevented and may even improve LV function in selected patients [32,33]. Alternatively in very advanced cases, cardiac transplantation may be evaluated. Many of these patients already profit from resynchronisation therapy when presenting for surgery.
Early experience with the use of specific annuloplasty rings for correction of IMR at our institution (University Hospital Bern) is promising. Between Januar 2002 to February 2006, restrictive annuloplasty was performed in 17 patients exclusively with ischaemic CMP. With the availability of specific rings, the Etlogix [ER] (n = 36; Edwards Lifesciences Inc., Irvine, CA, USA) and Geoform ring [GR] (n = 11) were used for repair of significant ischaemic MR (EROA >20 mm2, RVol >30 mL) in 47 patients between April 2004 and May 2006. In 42 patients, additional procedures, mainly coronary artery bypass surgery (n = 37) were concomitantly performed. Low mean mitral gradients were measured early postoperatively (ER: 4.6 ± 1.7; GR: 3.7 ± 1.9 mm Hg; p = 0.5) and no important residual MR was observed (Figure 5A,B). No early death or stroke occurred. ICU and hospital stay were 3.6 ± 4.7 and 15.9 ± 14.6 days, respectively. During a total observation period of 17.1 ± 7.3 months for ER and 6.7 ± 2.9 for GR, one late death and no reoperation occurred. Echocardiographic controls showed no recurrent MR and improved LV function in the majority of patients (Figure 5C,D). Our experience demonstrates, that these new specific annuloplasty rings allow effective and durable correction of IMR. On-going follow-up will allow to assess their impact on long-term survival and cardiac function. In comparison to published mortality rates of up to 10–12% [34,35], our results compare favorably.
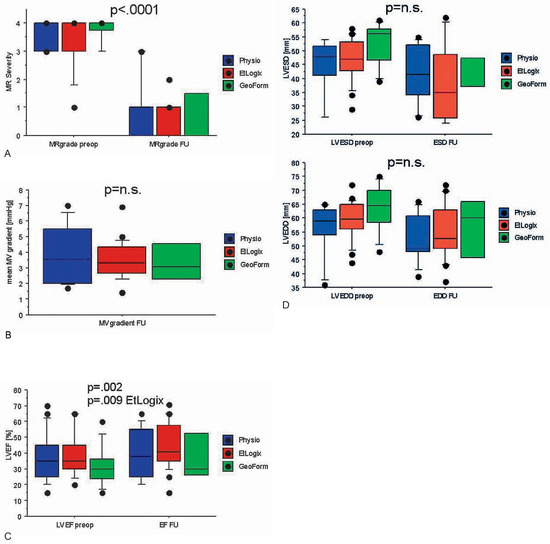
Figure 5.
Effect of annuloplasty in IMR. (A) IMR is successfully eliminated with all three types of rings (Physio: Conventional semi-rigid annuloplasty ring used for restrictive annuloplasty in IMR). (B) Low transmitral mean gradients during follow-up were measured in all groups. (C) Improvement in LVEF was significant overall and especially with the use of the EtLogix ring. (D) Although not significantly, LV dimensions decreased both end-systolic (above) and end-diastolic (below) in all three groups during follow-up.
Alternative approaches to IMR
A multitude of newly designed surgical and percutaneous catheter-based devices are currently being evaluated in animal and clinical studies for the treatment of IMR. Among them, the Coapsys® device (Myocor Inc., Maple Grove, MN, USA) adopts the concept of septolateral cinching proposed by Fukamachi [36] for surgical correction of IMR. Animal studies have shown effective elimination of IMR [37] and although clinical experience with 34 implants reported last year is still small, 1-year results appear promising [38]. The same concept is percutaneously applied with the PS3TM device (Ample Medical Inc., Foster City, CA, USA), having been reported to be implanted in 2 patients only so far [39,40] with good short-term results. With the VikingTM device (Edwards Lifesciences Inc., Irvine, CA, USA), a catheter-based annuloplasty is performed across the coronary sinus [41]. Early results of 5 patients reported last year was disappointing with device separation and recurrent MR, provoking discontinuation of patient enrollment [42]. Another percutaneous device, the MitraClip (Evalve Inc., Redwood City, CA, USA) allows edge-to-edge leaflet plication by a clip, restoring leaflet coaptation and reducing MR [43]. This technique is adopted from the open edge-to-edge repair propagated by Alfieri [28]. However, without combined annuloplasty, results may be less durable [44]. Results reported from the EVEREST phase I trial in 2005 demonstrated the need for surgical mitral repair due to device failure in 5 of 24 patients within 30 days. At 6 months follow-up, 13 patients presented with grade £2 residual MR and 2 with grade £3. It was concluded, that the device is safe and that it reduces IMR in a significant proportion of patients to 6 months [43]. The on-going phase II randomised trial will allow evaluation of the risk-benefit profile of this technique.
In summary, IMR in the setting of ischaemic and dilated CMP is frequent and has been shown to have a negative impact on patient survival. Quantitative assessment under resting conditions is standard today and indicative for surgical treatment, but IMR may be underestimated because of its dynamic nature. Therefore, evaluation during exercise testing is very helpful, especially in borderline cases. Despite established threshold values for the severity of IMR, the indication for surgical treatment must be individualised, especially in patients with moderate IMR, in whom surgical treatment remains controversial. Additional surgical measures should be considered in severe LV dilatation and alternative treatment strategies discussed in patients with end-stage CMP.
Informed Consent Statement
The permission to reprint the figures has been granted by Edwards Lifesciences, USA, for which we are very grateful.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bursi, F.; Enriquez-Sarano, M.; Nkomo, V.T.; Jacobsen, S.J.; Weston, S.A.; Meverden, R.A.; et al. Heart failure and death after myocardial infarction in the community: The emerging role of mitral regurgitation. Circulation 2005, 111, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Lam, B.K.; Gillinov, A.M.; Blackstone, E.H.; Rajeswaran, J.; Yuh, B.; Bhudia, S.K.; et al. Importance of moderate ischemic mitral regurgitation. Ann Thorac Surg. 2005, 79, 462–470; discussion–470. [Google Scholar] [CrossRef] [PubMed]
- Grigioni, F.; Enriquez-Sarano, M.; Zehr, K.J.; Bailey, K.R.; Tajik, A.J. Ischemic mitral regurgitation: Long-term outcome and prognostic implications with quantitative Doppler assessment. Circulation 2001, 103, 1759–1764. [Google Scholar] [CrossRef]
- Lancellotti, P.; Lebrun, F.; Pierard, L.A. Determinants of exercise-induced changes in mitral regurgitation in patients with coronary artery disease and left ventricular dysfunction. J Am Coll Cardiol. 2003, 42, 1921–1928. [Google Scholar] [CrossRef]
- Simpson, I.A.; Shiota, T.; Gharib, M.; Sahn, D.J. Current status of flow convergence for clinical applications: Is it a leaning tower of «PISA»? J Am Coll Cardio. 1996, 27, 504–509. [Google Scholar] [CrossRef]
- Zoghbi, W.A.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Kraft, C.D.; Levine, R.A.; et al. Recommendations for evaluation of the severity of native valvular regurgitation with twodimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003, 16, 777–802. [Google Scholar] [CrossRef] [PubMed]
- Grewal, K.S.; Malkowski, M.J.; Piracha, A.R.; Astbury, J.C.; Kramer, C.M.; Dianzumba, S.; et al. Effect of general anesthesia on the severity of mitral regurgitation by transesophageal echocardiography. Am J Cardiol. 2000, 85, 199–203. [Google Scholar] [CrossRef]
- Bach, D.S.; Deeb, G.M.; Bolling, S.F. Accuracy of intraoperative transesophageal echocardiography for estimating the severity of functional mitral regurgitation. Am J Cardiol. 1995, 76, 508–512. [Google Scholar] [CrossRef]
- Byrne, J.G.; Aklog, L.; Adams, D.H. Assessment and management of functional or ischaemic mitral regurgitation. Lancet 2000, 355, 1743–1744. [Google Scholar] [CrossRef]
- Adams, D.H.; Filsoufi, F.; Aklog, L. Surgical treatment of the ischemic mitral valve. J Heart Valve Dis. 2002, 11 (Suppl 1), S21–S25. [Google Scholar]
- Dion, R.; Benetis, R.; Elias, B.; Guennaoui, T.; Raphael, D.; Van Dyck, M.; et al. Mitral valve procedures in ischemic regurgitation. J Heart Valve Dis. 1995, 4 (Suppl 2), S124–S129; discussion S9–S31. [Google Scholar]
- Bax, J.J.; Schinkel, A.F.; Boersma, E.; Elhendy, A.; Rizzello, V.; Maat, A.; et al. Extensive left ventricular remodeling does not allow viable myocardium to improve in left ventricular ejection fraction after revascularization and is associated with worse longterm prognosis. Circulation 2004, 110 (Suppl 1), II18–22. [Google Scholar] [CrossRef]
- Braun, J.; Bax, J.J.; Versteegh, M.I.; Voigt, P.G.; Holman, E.R.; Klautz, R.J.; et al. Preoperative left ventricular dimensions predict reverse remodeling following restrictive mitral annuloplasty in ischemic mitral regurgitation. Eur J Cardiothorac Surg 2005, 27, 847–853. [Google Scholar] [CrossRef] [PubMed]
- De Simone, R.; Wolf, I.; Mottl-Link, S.; Hoda, R.; Mikhail, B.; Sack, F.U.; et al. A clinical study of annular geometry and dynamics in patients with ischemic mitral regurgitation: New insights into asymmetrical ring annuloplasty. Eur J Cardiothorac Surg. 2006, 29, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Pellizon, G.; Grines, C.L.; Cox, D.A.; Stuckey, T.; Tcheng, J.; Garcia, E.; et al. Importance of mitral regurgitaiton in patients undergoing percutaneuous coronary intervention for acute myocardial infarction. J Am Coll Cardiol. 2004, 43, 1368–1374. [Google Scholar] [CrossRef]
- Grossi, E.A.; Crooke, G.A.; DiGiorgi, P.L.; Schwartz, C.F.; Jorde, U.; Applebaum, R.M.; et al. Impact of moderate functional mitral insufficiency in patients undergoing surgical revascularization. Circulation 2006, 114 (1 Suppl), I573–I576. [Google Scholar] [CrossRef] [PubMed]
- Bax, J.J.; Braun, J.; Somer, S.T.; Klautz, R.; Holman, E.R.; Versteegh, M.I.; et al. Restrictive annuloplasty and coronary revascularization in ischemic mitral regurgitation results in reverse left ventricular remodeling. Circulation 2004, 110 (11 Suppl 1), II103–II108. [Google Scholar] [CrossRef]
- Kim, Y.H.; Czer, L.S.; Soukiasian, H.J.; De Robertis, M.; Magliato, K.E.; Blanche, C.; et al. Ischemic mitral regurgitation: Revascularization alone versus revascularization and mitral valve repair. Ann Thorac Surg. 2005, 79, 1895–1901. [Google Scholar] [CrossRef]
- Prifti, E.; Bonacchi, M.; Frati, G.; Giunti, G.; Babatasi, G.; Sani, G. Ischemic mitral valve regurgitation grade II–III: Correction in patients with impaired left ventricular function undergoing simultaneous coronary revascularization. J Heart Valve Dis. 2001, 10, 754–762. [Google Scholar]
- Paparella, D.; Mickleborough, L.L.; Carson, S.; Ivanov, J. Mild to moderate mitral regurgitation in patients undergoing coronary bypass grafting: Effects on operative mortality and longterm significance. Ann Thorac Surg. 2003, 76, 1094–1100. [Google Scholar] [CrossRef]
- Wu, A.H.; Aaronson, K.D.; Bolling, S.F.; Pagani, F.D.; Welch, K.; Koelling, T.M. Impact of mitral valve annuloplasty on mortality risk in patients with mitral regurgitation and left ventricular systolic dysfunction. J Am Coll Cardiol. 2005, 45, 381–387. [Google Scholar] [CrossRef]
- Trichon, B.H.; Glower, D.D.; Shaw, L.K.; Cabell, C.H.; Anstrom, K.J.; Felker, G.M.; et al. Survival after coronary revascularization, with and without mitral valve surgery, in patients with ischemic mitral regurgitation. Circulation 2003, 108 (Suppl 1), II103–II110. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bonow, R.O.; Carabello, B.A.; Kanu, C.; de Leon, A.C., Jr.; Faxon, D.P.; Freed, M.D.; et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): Developed in collaboration with the Society of Cardiovascular Anesthesiologists: Endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation 2006, 114, e84–e231. [Google Scholar] [PubMed]
- Grossi, E.A.; Bizekis, C.S.; LaPietra, A.; Derivaux, C.C.; Galloway, A.C.; Ribakove, G.H.; et al. Late results of isolated mitral annuloplasty for «functional» ischemic mitral insufficiency. J Card Surg. 2001, 16, 328–332. [Google Scholar] [CrossRef] [PubMed]
- McGee, E.C.; Gillinov, A.M.; Blackstone, E.H.; Rajeswaran, J.; Cohen, G.; Najam, F.; et al. Recurrent mitral regurgitation after annuloplasty for functional ischemic mitral regurgitation. J Thorac Cardiovasc Surg. 2004, 128, 916–924. [Google Scholar] [CrossRef]
- Messas, E.; Guerrero, J.L.; Handschumacher, M.D.; Conrad, C.; Chow, C.M.; Sullivan, S.; et al. Chordal cutting: A new therapeutic approach for ischemic mitral regurgitation. Circulation 2001, 104, 1958–1963. [Google Scholar] [CrossRef]
- Kron, I.L.; Green, G.R.; Cope, J.T. Surgical relocation of the posterior papillary muscle in chronic ischemic mitral regurgitation. Ann Thorac Surg. 2002, 74, 600–601. [Google Scholar] [CrossRef]
- Alfieri, O.; Maisano, F.; De Bonis, M.; Stefano, P.L.; Torracca, L.; Oppizzi, M.; et al. The double-orifice technique in mitral valve repair: A simple solution for complex problems. J Thorac Cardiovasc Surg. 2001, 122, 674–681. [Google Scholar] [CrossRef]
- Bolling, S.F. Mitral valve reconstruction in the patient with heart failure. Heart Fail Rev. 2001, 6, 177–185. [Google Scholar] [CrossRef]
- Daimon, M.; Fukuda, S.; Adams, D.H.; McCarthy, P.M.; Gillinov, A.M.; Carpentier, A.; et al. Mitral valve repair with Carpentier-McCarthy-Adams IMR ETlogix annuloplasty ring for ischemic mitral regurgitation: Early echocardiographic results from a multi-center study. Circulation 2006, 114 (Suppl), I588–I593. [Google Scholar] [CrossRef]
- Dor, V. Left ventricular reconstruction for ischemic cardiomyopathy. J Card Surg. 2002, 17, 180–187. [Google Scholar] [CrossRef]
- Oz, M.C.; Konertz, W.F.; Kleber, F.X.; Mohr, F.W.; Gummert, J.F.; Ostermeyer, J.; et al. Global surgical experience with the Acorn cardiac support device. J Thorac Cardiovasc Surg. 2003, 126, 983–991. [Google Scholar] [CrossRef]
- Pilla, J.J.; Blom, A.S.; Brockman, D.J.; Bowen, F.; Yuan, Q.; Giammarco, J.; et al. Ventricular constraint using the acorn cardiac support device reduces myocardial akinetic area in an ovine model of acute infarction. Circulation 2002, 106 (Suppl 1), I207–I211. [Google Scholar] [CrossRef] [PubMed]
- Grossi, E.A.; Goldberg, J.D.; LaPietra, A.; Ye, X.; Zakow, P.; Sussman, M.; et al. Ischemic mitral valve reconstruction and replacement: Comparison of long-term survival and complications. J Thorac Cardiovasc Surg. 2001, 122, 1107–1124. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.H.; Kim, M.J.; Kang, S.J.; Song, J.M.; Song, H.; Hong, M.K.; et al. Mitral valve repair versus revascularization alone in the treatment of ischemic mitral regurgitation. Circulation 2006, 114 (Suppl), I499–I503. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Fukamachi, K.; Inoue, M.; Doi, K.; Schenk, S.; Nemeh, H.; Faber, C.; et al. Reduction of mitral regurgitation using the Coapsys device: A novel ex vivo method using excised recipients’ hearts. Asaio J. 2005, 51, 82–84. [Google Scholar] [CrossRef] [PubMed]
- Tibayan, F.A.; Rodriguez, F.; Langer, F.; Zasio, M.K.; Bailey, L.; Liang, D.; et al. Does septal-lateral annular cinching work for chronic ischemic mitral regurgitation? J Thorac Cardiovasc Surg. 2004, 127, 654–663. [Google Scholar] [CrossRef][Green Version]
- Mishra, Y.K.; Mittal, S.; Jaguri, P.; Trehan, N. Coapsys mitral annuloplasty for chronic functional ischemic mitral regurgitation: 1-year results. Ann Thorac Surg. 2006, 81, 42–46. [Google Scholar] [CrossRef]
- Palacios, I.F.; Condado, J.A.; Brandi, S.; Rodriguez, V.; Bosch, F.; Silva, G.; et al. Safety and feasibility of acute percutaneous septal sinus shortening: First-in-human experience. Catheter Cardiovasc Interv. 2007, 69, 513–518. [Google Scholar] [CrossRef]
- Rogers, J.H.; Macoviak, J.A.; Rahdert, D.A.; Takeda, P.A.; Palacios, I.F.; Low, R.I. Percutaneous septal sinus shortening: A novel procedure for the treatment of functional mitral regurgitation. Circulation 2006, 113, 2329–2334. [Google Scholar] [CrossRef]
- Kaye, D.M.; Byrne, M.; Alferness, C.; Power, J. Feasibility and short-term efficacy of percutaneous mitral annular reduction for the therapy of heart failure-induced mitral regurgitation. Circulation 2003, 108, 1795–1797. [Google Scholar] [CrossRef][Green Version]
- Webb, J.G.; Harnek, J.; Munt, B.I.; Kimblad, P.O.; Chandavimol, M.; Thompson, C.R.; et al. Percutaneous transvenous mitral annuloplasty: Initial human experience with device implantation in the coronary sinus. Circulation 2006, 113, 851–855. [Google Scholar] [CrossRef]
- Feldman, T.; Wasserman, H.S.; Herrmann, H.C.; Gray, W.; Block, P.C.; Whitlow, P.; et al. Percutaneous mitral valve repair using the edge-to-edge technique: Six-month results of the EVEREST Phase I Clinical Trial. J Am Coll Cardiol. 2005, 46, 2134–2140. [Google Scholar] [CrossRef]
- Maisano, F.; Caldarola, A.; Blasio, A.; De Bonis, M.; La Canna, G.; Alfieri, O. Midterm results of edge-to-edge mitral valve repair without annuloplasty. J Thorac Cardiovasc Surg. 2003, 126, 1987–1997. [Google Scholar] [CrossRef]





© 2007 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.