Socioeconomic Patterning of Childhood Overweight Status in Europe


Abstract
:1. Introduction
2. Methods
2.1. Cross-Country Comparisons
2.2. Review of Literature on the Social Gradient in Childhood Overweight in European Countries
3. Results
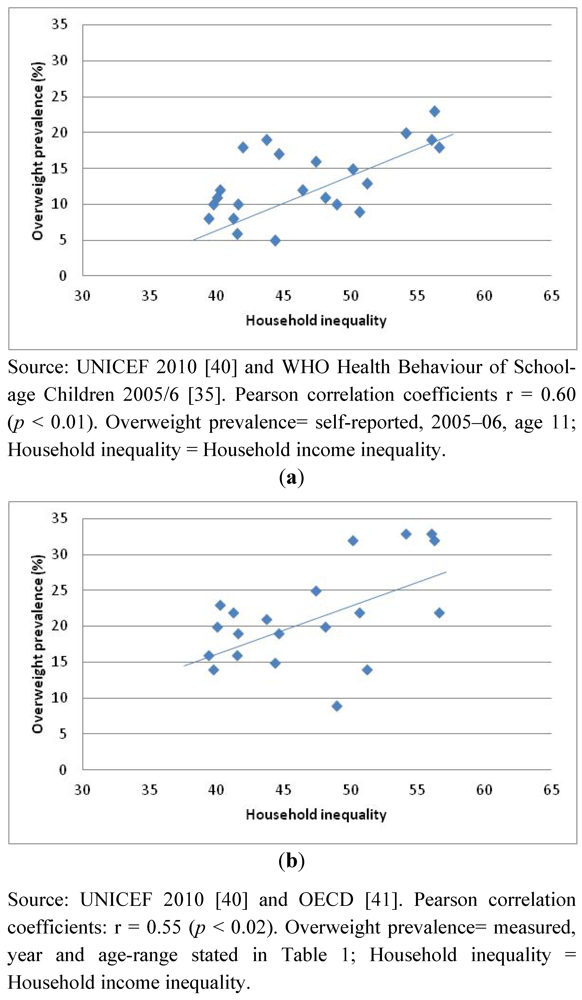
3.1. Results for Cross-Country Comparisons

{kind=link}
{kind=link}
| Income inequality *: households with children, 2008 a (%) | Overweight prevalence (self-reported, 2005-2006, age 11) b | Overweight prevalence (measured, year and age-range stated) c | |
|---|---|---|---|
| Greece | 56.6 | 18 | 22 (2003) 13–17 |
| Portugal | 56.2 | 23 | 32 (2003) 7–9 |
| Spain | 56 | 19 | 33 (2000) 13–14 |
| Italy | 54.1 | 20 | 33 (2006) 8–9 |
| Poland | 51.2 | 13 | 14 (2001) 7–9 |
| Belgium | 50.6 | 9 * | 22 (2005) 4–15 |
| United Kingdom | 50.1 | 15 ** | 32 (2004/8) 5–17 ** |
| Slovakia | 48.9 | 10 | 9 (1999) 11–17 |
| Germany | 48.1 | 11 | 20 (2002) 5–17 |
| Ireland | 47.4 | 16 | 25 (2007) 4–13 |
| Luxembourg | 46.4 | 12 | - |
| Hungary | 44.6 | 17 | 19 (2005) 7–18 |
| Switzerland | 44.3 | 5 | 15 (2007) 6–13 |
| Czech Republic | 43.7 | 19 | 21 (2005) 6–17 |
| Finland | 41.9 | 18 | - |
| France | 41.6 | 10 | 19 (2006) 11–17 |
| Netherlands | 41.5 | 6 | 16 (2003) 5–16 |
| Sweden | 41.2 | 8 | 22 (2001) 6–13 |
| Iceland | 40.2 | 12 | 23 (2003) 9 |
| Austria | 40 | 11 | 20 (2003) 8–12 |
| Denmark | 39.7 | 10 | 14 (1997) 5–16 |
| Norway | 39.4 | 8 | 16 (2005) 3–17 |
3.2. Variations in Childhood Overweight by Social Grouping over Time
3.2.1. Description of Studies
3.2.2. Influence of Socioeconomic Factors on the Distribution of Child Overweight over Time
4. Discussion
4.1. Strengths and Limitations
4.2. Potential Explanations in Those Studies Showing a Widening of the Social Gradient in Childhood Obesity in Europe
| ID | Country | Years range | Study design | Characteristics of study subjects | Indicators of child SES | Results |
|---|---|---|---|---|---|---|
| Brunt 2008 [46] | UK | 1995–2005 | National Community Child Health Database (NCCHD), over 11 years | N = 3756 – 4548 per year 3-year-old children in South Wales | Townsend Material Deprivation Score, which comprises assessments of unemployment, overcrowding, home and car ownership | Non- statistically significant greater rate of increase of overweight in children from the most deprived areas compared with those from the least deprived. |
| Kautiainen et al. 2009 [44] | Finland | 1979–2005 | 14 cross-sectional surveys, the Adolescent Health and Lifestyle Survey (AHLS) (biennial) | N = 3105 – 8390 per year 12–18 year olds (nationally representative sample) | Family structure (1 or 2 parents), degree of urbanization, area of residence, father or guardian’s occupational status, school achievement, mother and father’s employment status, mother’s education level | The increase in the prevalence of overweight over time did not differ between age groups. However an increasing trend over time in the prevalence of overweight was seen in 12-year-old girls with the least educated mothers, whereas among the other girls no statistically significant change was seen over time. |
| Lioret et al. 2009 [43] | France | 1998–2007 | Comparison of 2 cross sectional food consumption surveys (INCA 1, 1998/9 and INCA 2, 2006/7) | N = 1034 3–14 year olds | Health of household occupation and level of education; variables describing household wealth. | Though the prevalence of childhood overweight was significantly and inversely correlated to all SES indicators, there was no change in the strong inverse SES gradient of childhood overweight over time, from 1998 to 2007 |
| Romon et al. 2005 [45] | France | 1989–1999 | Comparison of cross-sectional surveys of children in the final year of nursery school in the city of Lille, 1989 and 1999 | N = 705 in 1989 and 1258 in 1999) 5 year old nursery children | Occupation of the father or occupation of the single parent. Occupation divided into four classes: (I) Professional and managerial occupations; (II) Intermediate occupations (Employees, own account workers); (III) lower occupations (technical, semi routine and routine); (IV) unemployed | The change in the prevalence of overweight over time differed as a function of social class: in 1989 there were no significant differences between social classes whereas in 1999 there was a clear difference between classes both for overweight (p = 0.0005) and obesity (p = 0.04). |
| Semmler et al. 2009 [47] | UK | 1998–2005 | Subsample from the Twins Early Development Study. Comparison of socio-demographically and geographically matched families on the basis of parental weight status | N = 346 children aged 4 (1998/9) and followed up 7 years later | ‘Family SES’ refers to maternal education: Lower SES = GCSE or lessHigher SES = A level or above | The change in adiposity from ages 4 to 11 differed as a function of familial SES: at age 11, significantly more children from lower SES families (29%) than higher families (17%) were overweight (P = 0.046). |
| De Spiegelaere et al. 1998 [49] | Belgium | 1988–1994 | Retrospective cohort study on a sample of 12–15 year old adolescents born between 1976 and 1979, taken from six school medical centres in Brussels region. | N = 2607 adolescents aged about 12 at 1st examination and about 15 years at the 2nd, from five social groups | Five social groups were defined according to parents’ professions (Upper management/professionals, white collar workers, active self-employed and technicians, active manual workers, unemployed and dependent on state assistance) and the status of their activity (active or inactive: out of work, invalid, etc.) | Social inequalities in obesity increased between the first and second examination approximately two years apart: for the whole sample, there was a significant increase in the prevalence of obesity in the least-favoured social group (+3.3% (+/− 2.7%)). |
| Stamatakis et al. 2010 [48] | UK | 1997–2007 | Ten cross-sectional surveys, the Health Survey for England (annual, omitting 1999) | 5–10 year old children | Socioeconomic position was a composite score based on family household income (quintiles) and social class scales (I, II, III manual, III non manual, IV and V), based on occupation of the head of the household. | The gradient in the prevalence between high and low income groups was significant for overweight in boys (p = 0.04) and girls (P = 0.003) in 2006/7 and for obesity in girls in 2002/3 (p = 0.001), 2004/5 (p = 0.005) and 2006/7 (p = 0.04). The socioeconomic position (SEP) score gradient also increased over time, reaching significance in 2006/7 for boys’ overweight (p < 0.001) and obesity (p = 0.002) when obesity prevalence in the low SEP score group was twice than that in the higher groups. |
4.3. Implications for Further Research
5. Conclusion
Conflict of Interest
References
- Martinez, J.A.; Kearney, J.M.; Kafatos, A.; Paquet, S.; Martinez-Gonzalez, M.A. Variables independently associated with self-reported obesity in the European Union. Public Health Nutr. 1999, 2, 125–133. [Google Scholar]
- Molarius, A.; Seidell, J.C.; Sans, S.; Tuomilehto, J.; Kuulasmaa, K. Educational level, relative body weight, and changes in their association over 10 years: An international perspective from the WHO MONICA Project. Am. J. Public Health 2000, 90, 1260–1268. [Google Scholar] [CrossRef]
- Cavelaars, A.E.; Kunst, A.E.; Mackenbach, J.P. Socio-economic differences in risk factors for morbidity and mortality in the European Community: An international comparison. J. Health psychol. 1997, 2, 353–372. [Google Scholar]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.J.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E. European Union Working Group on Socioeconomic Inequalities in Health. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef]
- Giskes, K.; van Lenthe, F.J.; Turrell, G.; Kamphuis, C.B.; Brug, J.; Mackenbach, J.P. Socioeconomic position at different stages of the life course and its influence on body weight and weight gain in adulthood: A longitudinal study with 13-year follow-up. Obesity (Silver Spring) 2008, 16, 1377–1381. [Google Scholar] [CrossRef]
- Wardle, J.; Griffith, J. Socioeconomic status and weight control practices in British adults. J. Epidemiol. Community Health 2001, 55, 185–190. [Google Scholar]
- Wardle, J.; Waller, J.; Jarvis, M.J. Sex differences in the association of socioeconomic status with obesity. Am. J. Public Health 2002, 92, 1299–1304. [Google Scholar]
- Zaninotto, P.; Head, J.; Stamatakis, E.; Wardle, H.; Mindell, J. Trends in obesity among adults in England from 1993 to 2004 by age and social class and projections of prevalence to 2012. J. Epidemiol. Community Health 2009, 63, 140–146. [Google Scholar]
- Sobal, J.; Stunkard, A.J. Socioeconomic status and obesity: A review of the literature. Psychol. Bull. 1989, 105, 260–275. [Google Scholar]
- OECD, Obesity and the Economics of Prevention: Fit not Fat; OECD: Paris, France, 2010.
- Borodulin, K.; Makinen, T.; Fogelholm, M.; Lahti-Koski, M.; Prattala, R. Trends and socioeconomic differences in overweight among physically active and inactive Finns in 1978–2002. Prev. Med. 2007, 45, 157–162. [Google Scholar]
- LahtiI-Koski, M.; Vartiainen, E.; Mannisto, S.; Pietinen, P. Age, education and occupation as determinants of trends in body mass index in Finland from 1982 to 1997. Int. J. Obes. Related Metab. Disord. 2000, 24, 1669–1676. [Google Scholar]
- Charafeddine, R.; Van Oyen, H.; Demarest, S. Trends in social inequalities in obesity: Belgium, 1997 to 2004. Prev. Med. 2009, 48, 54–58. [Google Scholar]
- Czernichow, S.; Vergnaud, A.C.; Maillard-Teyssier, L.; Peneau, S.; Bertrais, S.; Mejean, C.; Vol, S.; Tichet, J.; Hercberg, S. Trends in the prevalence of obesity in employed adults in central-western France: A population-based study, 1995–2005. Prev. Med. 2009, 48, 262–266. [Google Scholar]
- GutierrezFisac, J.L.; Regidor, E.; Rodriguez, C. Trends in obesity differences by educational level in Spain. J. Clin. Epidemiol. 1996, 49, 351–354. [Google Scholar]
- Galobardes, B.; Costanza, M.C.; Bernstein, M.S.; Delhumeau, C.; Morabia, A. Trends in risk factors for lifestyle-related diseases by socioeconomic position in Geneva, Switzerland, 1993–2000: Health inequalities persist. Am. J. Public Health 2003, 93, 1302–1309. [Google Scholar] [CrossRef]
- Goodman, E.; Adler, N.E.; Daniels, S.R.; Morrison, J.A.; Slap, G.B.; Dolan, L.M. Impact of objective and subjective social status on obesity in a biracial cohort of adolescents. Obes. Res. 2003, 11, 1018–1026. [Google Scholar]
- Hardeman, W.; Griffin, S.; Johnston, M.; Kinmonth, A.L.; Wareham, N.J. Interventions to prevent weight gain: A systematic review of psychological models and behaviour change methods. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 131–143. [Google Scholar]
- Kumar, B.N.; Holmboe-Ottesen, G.; Lien, N.; Wandel, M. Ethnic differences in body mass index and associated factors of adolescents from minorities in Oslo, Norway: A cross-sectional study. Public Health Nutr. 2004, 7, 999–1008. [Google Scholar]
- Kumar, B.N.; Meyer, H.E.; Wandel, M.; Dalen, I.; Holmboe-Ottesen, G. Ethnic differences in obesity among immigrants from developing countries, in Oslo, Norway. Int. J. Obes. (Lond.) 2006, 30, 684–690. [Google Scholar] [CrossRef]
- Daryani, A.; Kocturk, T.; Andersson, A.; Karlstro, B.; Vessby, B.; Becker, W. Reported macronutrient intake and metabolic risk factors: Immigrant women from Iran and Turkey compared with native Swedish women. Scand. J. Food Nutr. 2006, 50, 166–172. [Google Scholar]
- Dowse, G.; Zimmet, P. The thrifty genotype in non-insulin dependent diabetes. BMJ 1993, 306, 532–533. [Google Scholar]
- Lobstein, T.; Millstone, E.; PorGrow Research, T. Context for the PorGrow study: Europe’s obesity crisis. Obes. Rev. 2007, 8, 7–16. [Google Scholar]
- Jackson-Leach, R.; Lobstein, T. Estimated burden of paediatric obesity and comorbidities in Europe. Part 1. The increase in the prevalence of child obesity in Europe is itself increasing. Int. J. Pediatr. Obes. 2006, 1, 26–32. [Google Scholar] [CrossRef]
- Lobstein, T.; Baur, L.; Uauy, R. TaskForce IIO. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5, 4–104. [Google Scholar] [CrossRef]
- Branca, F.; Nikogosian, H.; Lobstein, T. The challenge of obesity in the European Region and the strategies for response. Copenhagen: World Health Organization, Regional Office for Europe, 2007. Available online: http://www.euro.who.int/document/E90711.pdf (accessed on 30 June 2008).
- Salanave, B.; Peneau, S.; Rolland-Cachera, M.F.; Hercberg, S.; Castetbon, K. Stabilization of overweight prevalence in French children between 2000 and 2007. Int. J. Pediatr. Obes. 2009, 4, 66–72. [Google Scholar]
- Cattaneo, A.; Monasta, L.; Stamatakis, E.; Lioret, S.; Castetbon, K.; Frenken, F.; Manios, Y.; Moschonis, G.; Sawa, S.; Zaborskis, A.; et al. Overweight and obesity in infants and pre-school children in the European Union: A review of existing data. Obes. Rev. 2010, 11, 389–398. [Google Scholar] [CrossRef]
- Lazzeri, G.; Rossi, S.; Pammolli, A.; Pilato, V.; Pozzi, T.; Giacchi, M.V. Underweight and overweight among children and adolescents in Tuscany (Italy). Prevalence and short-term trends. J. Prev. Med. Hyg. 2008, 49, 13–21. [Google Scholar]
- Aeberli, I.; Ammann, R.S.; Knabenhans, M.; Molinari, L.; Zimmermann, M.B. Decrease in the prevalence of paediatric adiposity in Switzerland from 2002 to 2007. Public Health Nutr. 2010, 13, 806–811. [Google Scholar]
- Lissner, L.; Sohlstrom, A.; Sundblom, E.; Sjoberg, A. Trends in overweight and obesity in Swedish schoolchildren 1999–2005: Has the epidemic reached a plateau? Obes. Rev. 2010, 11, 553–559. [Google Scholar]
- Hébel, P. French Observatory on Consumption. Centre de recherche pour l’étude et l’observation des conditions de vie, Paris, France. Personal Communication, 2012..
- CREDOC, Survey on the Behaviours and Consumption of the French population (Enquete CCAF: Comportements et Consommations Alimentaires des Français). Unpublished, Centre de recherche pour l’étude et l’observation des conditions de vie (CREDOC), Paris, France, 2010.
- Shrewsbury, V.; Wardle, J. Socioeconomic status and adiposity in childhood: A systematic review of cross-sectional studies 1990–2005. Obesity (Silver Spring) 2008, 16, 275–284. [Google Scholar] [CrossRef]
- Currie, C.; Gabhainn, S.; Godeau, E.; Roberts, C.; Smith, R.; Currie, D.; Picket, W.; Richter, M.; Morgan, A.; Barnekow, V. Inequalities in Young People’s Health. HBSC International Report from the 2005/2006 Survey; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2008. [Google Scholar]
- Due, P.; Damsgaard, M.T.; Rasmussen, M.; Holstein, B.E.; Wardle, J.; Merlo, J.; Currie, C.; Ahluwalia, N.; Sorensen, T.I.; Lynch, J.; et al. Socioeconomic position, macroeconomic environment and overweight among adolescents in 35 countries. Int. J. Obes. (Lond.) 2009, 33, 1084–1093. [Google Scholar]
- Van Rossem, L.; Silva, L.M.; Hokken-Koelega, A.; Arends, L.R.; Moll, H.A.; Jaddoe, V.W.; Hofman, A.; Mackenbach, J.P.; Raat, H. Socioeconomic status is not inversely associated with overweight in preschool children. J. Pediatr. 2010, 157, 929–935. [Google Scholar]
- Howe, L.D.; Tilling, K.; Galobardes, B.; Smith, G.D.; Ness, A.R.; Lawlor, D.A. Socioeconomic disparities in trajectories of adiposity across childhood. Int. J. Pediatr. Obes. 2011, 6, e144–e153. [Google Scholar]
- Pinot De Moira, A.; Power, C.; Li, L. Changing influences on childhood obesity: A study of 2 generations of the 1958 british birth cohort. Am. J. Epidemiol. 2010, 171, 1289–1298. [Google Scholar]
- Currie, C.; Currie, D.; Menchini, L.; Richardson, D.; Roberts, C. Comparing Inequality in the Well-Being of Children in Economically Advanced Countries: A Methodology; Innocenti Working Paper (IWP-2010-19, revised version December 2011); UNICEF Innocenti Research Centre: Florence, Italy, 2011. Available online: http://www.unicef-irc.org/publications/pdf/iwp_2010_19.pdf (accessed on 20 January 2012).
- Sassi, F. Obesity and the Economics of Prevention: Fit not Fat; Organization for Economic Cooperation and Development (OECD): Paris, France, 2010. Available online: http://dx.doi.org/10.1787/888932315944 (accessed on 20 January 2012).
- Cole, T.; Bellizzi, M.; Flegal, K.; Dietz, W. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar]
- Lioret, S.; Touvier, M.; Dubuisson, C.; Dufour, A.; Calamassi-Tran, G.; Lafay, L.; Volatier, J.L.; Maire, B. Trends in child overweight rates and energy intake in France from 1999 to 2007: Relationships with socioeconomic status. Obesity (Silver Spring) 2009, 17, 1092–1100. [Google Scholar] [CrossRef]
- Kautiainen, S.; Koivisto, A.-M.; Koivusilta, L.; Lintonen, T.; Virtanen, S.M.; Rimpela, A. Sociodemographic factors and a secular trend of adolescent overweight in Finland. Int. J. Pediatr. Obes. 2009, 4, 360–370. [Google Scholar]
- Romon, M.; Duhamel, A.; Collinet, N.; Weill, J. Influence of social class on time trends in BMI distribution in 5-year-old French children from 1989 to 1999. Int. J. Obes. (Lond.) 2005, 29, 54–59. [Google Scholar] [CrossRef]
- Brunt, H.; Lester, N.; Davies, G.; Williams, R. Childhood overweight and obesity: Is the gap closing the wrong way? J. Public Health 2008, 30, 145–152. [Google Scholar] [CrossRef]
- Semmler, C.; Ashcroft, J.; van Jaarsveld, C.H.; Carnell, S.; Wardle, J. Development of overweight in children in relation to parental weight and socioeconomic status. Obesity (Silver Spring) 2009, 17, 814–820. [Google Scholar] [CrossRef]
- Stamatakis, E.; Wardle, J.; Cole, T.J. Childhood obesity and overweight prevalence trends in England: Evidence for growing socioeconomic disparities. Int. J. Obes. (Lond.) 2010, 34, 41–47. [Google Scholar] [CrossRef]
- De Spiegelaere, M.; Dramaix, M.; Hennart, P. Social class and obesity in 12-year-old children in Brussels: Influence of gender and ethnic origin. Eur. J. Pediatr. 1998, 157, 432–435. [Google Scholar]
- Nettle, D. Why are there social gradients in preventative health behavior? A perspective from behavioral ecology. PLoS One 2010, 5. [Google Scholar]
- McMillen, I.C.; MacLaughlin, S.M.; Muhlhausler, B.S.; Gentili, S.; Duffield, J.L.; Morrison, J.L. Developmental origins of adult health and disease: The role of periconceptional and foetal nutrition. Basic Clin. Pharmacol. Toxicol. 2008, 102, 82–89. [Google Scholar]
- Kramer, M.; Séguin, L.; Lydon, J.; Goulet, L. Socio-economic disparities in pregnancy outcome: Why do the poor fare so poorly? Paediatr. Perinat. Epidemiol. 2000, 14, 194–210. [Google Scholar] [CrossRef]
- Matijasevich, A.; Victora, C.G.; Lawlor, D.A.; Golding, J.; Menezes, A.M.; Araujo, C.L.; Barros, A.J.; Santos, I.S.; Barros, F.C.; Smith, G.D. Association of socioeconomic position with maternal pregnancy and infant health outcomes in birth cohort studies from Brazil and the UK. J. Epidemiol. Community Health 2012, 66, 127–135. [Google Scholar]
- Huang, J.S.; Lee, T.A.; Lu, M.C. Prenatal programming of childhood overweight and obesity. Matern. Child Health J. 2007, 11, 461–473. [Google Scholar]
- Monasta, L.; Batty, G.D.; Cattaneo, A.; Lutje, V.; Ronfani, L.; van Lenthe, F.J.; Brug, J. Early-life determinants of overweight and obesity: A review of systematic reviews. Obes. Rev. 2010, 11, 695–708. [Google Scholar]
- Parsons, T.J.; Power, C.; Logan, S.; Summerbell, C.D. Childhood predictors of adult obesity: A systematic review. Int. J. Obes. (Lond.) 1999, 23, S1–S107. [Google Scholar] [CrossRef]
- Bundred, P.; Kitchiner, D.; Buchan, I. Prevalence of overweight and obese children between 1989 and 1998: Population based series of cross sectional studies. BMJ 2001, 322, 326–328. [Google Scholar]
- Robertson, A.; Lobstein, T.; Knai, C. Obesity and Socio-Economic Groups in Europe: Evidence Review and Implications for Action; Health and Consumer Protection Directorate General of the European Commission: Brussels, Belgium, 2007. Available online: http://ec.europa.eu/health/ph_determinants/life_style/nutrition/documents/ev20081028_rep_en.pdf (accessed on 16 March 2012).
- Barker, D.J. Obesity and early life. Obes. Rev. 2007, 8, 45–49. [Google Scholar]
- Snethen, J.A.; Hewitt, J.B.; Goretzke, M. Childhood obesity: The infancy connection. J. Obstet. Gynecol. Neonatal Nurs. 2007, 36, 501–510. [Google Scholar]
- Olafsdottir, A.S.; Skuladottir, G.V.; Thorsdottir, I.; Hauksson, A.; Steingrimsdottir, L. Combined effects of maternal smoking status and dietary intake related to weight gain and birth size parameters. BJOG 2006, 113, 1296–1302. [Google Scholar]
- French Ministry of Health, La Naissance en France en 1995. Enquête Nationale Périnatale; Ministere du Travail et des Affaires Sociales, French Ministry of Health: Paris, France, 1995.
- French Ministry of Health, Enquête nationale périnatale 2003; Ministry of Health/INSERM, French Ministry of Health: Paris, France, 2005.
- French Ministry of Health, Enquête nationale périnatale 1998; Ministry of Health: Paris, France, 2001.
- Dubois, L.; Girard, M. Social inequalities in infant feeding during the first year of life. The Longitudinal Study of Child Development in Quebec (LSCDQ 1998–2002). Public Health Nutr. 2003, 6, 773–783. [Google Scholar]
- Wijndaele, K.; Lakshman, R.; Landsbaugh, J.R.; Ong, K.K.; Ogilvie, D. Determinants of early weaning and use of unmodified cow’s milk in infants: A systematic review. J. Am. Diet. Assoc. 2009, 109, 2017–2028. [Google Scholar]
- Arenz, S.; von Kries, R. Protective effect of breastfeeding against obesity in childhood. Can a meta-analysis of observational studies help to validate the hypothesis? Adv. Exp. Med. Biol. 2005, 569, 40–48. [Google Scholar] [CrossRef]
- Hilson, J.A.; Rasmussen, K.M.; Kjolhede, C.L. Excessive weight gain during pregnancy is associated with earlier termination of breast-feeding among White women. J. Nutr. 2006, 136, 140–146. [Google Scholar]
- Hilson, J.A.; Rasmussen, K.M.; Kjolhede, C.L. High prepregnant body mass index is associated with poor lactation outcomes among white, rural women independent of psychosocial and demographic correlates. J. Hum. Lact. 2004, 20, 18–29. [Google Scholar]
- Baker, J.L.; Michaelsen, K.F.; Sorensen, T.I.; Rasmussen, K.M. High prepregnant body mass index is associated with early termination of full and any breastfeeding in Danish women. Am. J. Clin. Nutr. 2007, 86, 404–411. [Google Scholar]
- Viswanathan, M.; Siega-Riz, A.M.; Moos, M.K.; Deierlein, A.; Mumford, S.; Knaack, J.; Thieda, P.; Lux, L.; Lohr, K.N. Outcomes of Maternal Weight Gain. In Evidence Reports/Technology Assessessments; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008; pp. 1–223. [Google Scholar]
- Whitaker, R.C.; Phillips, S.M.; Orzol, S.M.; Burdette, H.L. The association between maltreatment and obesity among preschool children. Child Abuse Negl. 2007, 31, 1187–1199. [Google Scholar]
- Mathieson, A.; Koller, T. Addressing the Socioeconomic Determinants of Healthy Eating Habits and Physical Activity Levels among Adolescents; World Health Organization: Copenhagen, Denmark, 2006. [Google Scholar]
- Eisenmann, J.C.; Gundersen, C.; Lohman, B.J.; Garasky, S.; Stewart, S.D. Is food insecurity related to overweight and obesity in children and adolescents? A summary of studies, 1995–2009. Obes. Rev. 2011, 12, e73–e83. [Google Scholar]
- Lohman, B.J.; Stewart, S.; Gundersen, C.; Garasky, S.; Eisenmann, J.C. Adolescent overweight and obesity: Links to food insecurity and individual, maternal, and family stressors. J. Adolesc. Health 2009, 45, 230–237. [Google Scholar] [CrossRef]
- Cullen, K.W.; Ash, D.M.; Warneke, C.; de Moor, C. Intake of soft drinks, fruit-flavored beverages, and fruits and vegetables by children in grades 4 through 6. Am. J. Public Health 2002, 92, 1475–1478. [Google Scholar] [CrossRef]
- Cribb, V.L.; Jones, L.R.; Rogers, I.S.; Ness, A.R.; Emmett, P.M. Is maternal education level associated with diet in 10-year-old children? Public Health Nutr. 2011, 14, 2037–2048. [Google Scholar] [CrossRef]
- Naska, A.; Bountziouka, V.; Trichopoulou, A.; Participants, D. Soft drinks: Time trends and correlates in twenty-four European countries. A cross-national study using the DAFNE (Data Food Networking) databank. Public Health Nutr. 2010, 13, 1346–1355. [Google Scholar] [CrossRef]
- Sallis, J.F.; Zakarian, J.M.; Hovell, M.F.; Hofstetter, C.R. Ethnic, socioeconomic, and sex differences in physical activity among adolescents. J. Clin. Epidemiol. 1996, 49, 125–134. [Google Scholar] [CrossRef]
- Booth, S.L.; Sallis, J.F.; Ritenbaugh, C.; Hill, J.O.; Birch, L.L.; Frank, L.D.; Glanz, K.; Himmelgreen, D.A.; Mudd, M.; Popkin, B.M.; et al. Environmental and societal factors affect food choice and physical activity: Rationale, influences, and leverage points. Nutr. Rev. 2001, 59, S21–S39, discussion S57–S65.. [Google Scholar]
- Inoue, S.; Ohya, Y.; Odagiri, Y.; Takamiya, T.; Ishii, K.; Kitabayashi, M.; Suijo, K.; Sallis, J.F.; Shimomitsu, T. Association between perceived neighborhood environment and walking among adults in 4 cities in Japan. J. Epidemiol. 2010, 20, 277–286. [Google Scholar]
- Lachapelle, U.; Frank, L.; Saelens, B.E.; Sallis, J.F.; Conway, T.L. Commuting by public transit and physical activity: Where you live, where you work, and how you get there. J. Phys. Act. Health 2011, 8, S72–S82. [Google Scholar]
- Patrick, K.; Norman, G.J.; Calfas, K.J.; Sallis, J.F.; Zabinski, M.F.; Rupp, J.; Cella, J. Diet, physical activity, and sedentary behaviors as risk factors for overweight in adolescence. Arch. Pediatr. Adolesc. Med. 2004, 158, 385–390. [Google Scholar] [CrossRef]
- van Dyck, D.; Cardon, G.; Deforche, B.; Owen, N.; Sallis, J.F.; de Bourdeaudhuij, I. Neighborhood walkability and sedentary time in Belgian adults. Am. J. Prev. Med. 2010, 39, 25–32. [Google Scholar]
- Guignon, N.; Collet, M.; Gonzalez, L.; de Saint Pol, T.; Guthmann, J.; Fonteneau, L. La santé des enfants en grande section de maternelle en 2005–2006; No 737; Direction de la recherche, des études, de l’évaluation et des statistiques (DREES): Paris, France, 2010. [Google Scholar]
- Iversen, A.C.; Kraft, P. Does socio-economic status and health consciousness influence how women respond to health related messages in media? Health Educ. Res. 2006, 21, 601–610. [Google Scholar] [CrossRef]
- King’s Fund Health Development Agency, Public Attitudes to Public Health Policy; King’s Fund: London, UK, 2004.
- Adler, N.E.; Boyce, T.; Chesney, M.A.; Cohen, S.; Folkman, S.; Kahn, R.L.; Syme, S.L. Socioeconomic status and health. The challenge of the gradient. Am. Psychol. 1994, 49, 15–24. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar]
- Law, C.; Power, C.; Graham, H.; Merrick, D. Obesity and health inequalities. Obes. Rev. 2007, 8, 19–22. [Google Scholar]
- Braveman, P.A.; Cubbin, C.; Egerter, S.; Chideya, S.; Marchi, K.S.; Metzler, M.; Posner, S. Socioeconomic status in health research: One size does not fit all. J. Am. Med. Assoc. 2005, 294, 2879–2888. [Google Scholar]
- Sobal, J. Obesity and socioeconomic status: A framework for examining relationships between physical and social variables. Med. Anthropol. 1991, 13, 231–247. [Google Scholar]
- Kuepper-Nybelen, J.; Lamerz, A.; Bruning, N.; Hebebrand, J.; Herpertz-Dahlmann, B.; Brenner, H. Major differences in prevalence of overweight according to nationality in preschool children living in Germany: Determinants and public health implications. Arch. Dis. Child. 2005, 90, 359–363. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Knai, C.; Lobstein, T.; Darmon, N.; Rutter, H.; McKee, M. Socioeconomic Patterning of Childhood Overweight Status in Europe. Int. J. Environ. Res. Public Health 2012, 9, 1472-1489. https://doi.org/10.3390/ijerph9041472
Knai C, Lobstein T, Darmon N, Rutter H, McKee M. Socioeconomic Patterning of Childhood Overweight Status in Europe. International Journal of Environmental Research and Public Health. 2012; 9(4):1472-1489. https://doi.org/10.3390/ijerph9041472
Chicago/Turabian StyleKnai, Cécile, Tim Lobstein, Nicole Darmon, Harry Rutter, and Martin McKee. 2012. "Socioeconomic Patterning of Childhood Overweight Status in Europe" International Journal of Environmental Research and Public Health 9, no. 4: 1472-1489. https://doi.org/10.3390/ijerph9041472
APA StyleKnai, C., Lobstein, T., Darmon, N., Rutter, H., & McKee, M. (2012). Socioeconomic Patterning of Childhood Overweight Status in Europe. International Journal of Environmental Research and Public Health, 9(4), 1472-1489. https://doi.org/10.3390/ijerph9041472