Pattern of Maternal Knowledge and Its Implications for Diarrhoea Control in Southern Malawi: Multilevel Thresholds of Change Analysis

Abstract
:1. Introduction
2. Methods
2.1. Area
2.2. Sample
2.3. Variables
2.3.1. Outcome Variables

{kind=link}
| Variable | Mean | Median | Min. | Max. | N = 1389 | % |
|---|---|---|---|---|---|---|
| What are the symptoms of diarrhoea? | ||||||
| 1. Watery stools | 1,171 | 84.3 | ||||
| 2. Increased number of stools | 183 | 13.2 | ||||
| 3. Loose stools | 383 | 27.6 | ||||
| 4. Loose stools and vomiting | 175 | 12.6 | ||||
| 5. Bloody stools | 183 | 13.2 | ||||
| 6. Stomach-ache | 492 | 35.4 | ||||
| What are the causes of diarrhoea | ||||||
| 1. Contaminated water | 765 | 55.1 | ||||
| 2. Contaminated food | 619 | 44.6 | ||||
| 3. Flies | 376 | 27.1 | ||||
| 4. Poor hygiene and sanitation practices | 703 | 50.6 | ||||
| 5. Poor sanitation practices | 111 | 8.0 | ||||
| What action do you take to prevent diarrhoea? | ||||||
| 1. Add disinfectant (water guard, chlorine, etc.) to water | 421 | 30.3 | ||||
| 2. Good water hygiene or management | 357 | 25.7 | ||||
| 3. Good food hygiene or management | 78 | 5.6 | ||||
| 4. Proper cleaning of cooking and eating utensils | 332 | 23.9 | ||||
| 5. Good sanitation | 278 | 20.0 | ||||
| 6. Hands washing | 307 | 22.1 | ||||
| Number of Symptoms identified | 2 | 2 | 0 | 5 | ||
| Zero or one symptom | 351 | 25.3 | ||||
| Two symptoms | 672 | 48.4 | ||||
| Three or more symptoms | 366 | 26.3 | ||||
| Number of Causes identified | 2 | 2 | 0 | 5 | ||
| No single cause mentioned | 61 | 4.4 | ||||
| One cause mentioned | 590 | 42.5 | ||||
| Two causes mentioned | 365 | 26.3 | ||||
| Three or more causes mentioned | 373 | 26.9 | ||||
| Prevention methods identified | 1 | 1 | 0 | 6 | ||
| No prevention method | 435 | 31.3 | ||||
| One prevention method | 404 | 29.1 | ||||
| Two prevention methods | 338 | 24.3 | ||||
| Three or more methods | 212 | 15.3 | ||||
| Overall knowledge | 5 | 5 | 0 | 14 | ||
| Zero to three points | 305 | 22.0 | ||||
| Four to five points | 498 | 35.9 | ||||
| Six to seven points | 438 | 31.5 | ||||
| Eight or more points | 148 | 10.7 |
2.3.2. Explanatory Variables Included in the Models
2.4. Statistical Analysis and Estimation
 such that s = 1, 2, 3. The responses on causes, prevention and overall knowledge have four categories each such that s = 1, 2, 3, 4. The last category in each case is taken as a reference.
such that s = 1, 2, 3. The responses on causes, prevention and overall knowledge have four categories each such that s = 1, 2, 3, 4. The last category in each case is taken as a reference.  and the probability that household i in community j will obtain a score higher than that represented by category s is
and the probability that household i in community j will obtain a score higher than that represented by category s is  . Then the cumulative response probabilities are defined as:
. Then the cumulative response probabilities are defined as:  (1)
(1) and for the other response variables
and for the other response variables  . Notice that the probabilities for the scores are cumulated downwards for convenience in interpretation of the results. A proportional odds model with a
. Notice that the probabilities for the scores are cumulated downwards for convenience in interpretation of the results. A proportional odds model with a  link is, therefore, given by:
link is, therefore, given by: (2)
(2) .
. (3)
(3) is a predictor variable whose slope coefficients,
is a predictor variable whose slope coefficients,  , are not the same across response categories and hence allowing fixed cut-point thresholds to vary across observations. Thus:
, are not the same across response categories and hence allowing fixed cut-point thresholds to vary across observations. Thus:
 is now our threshold value while
is now our threshold value while  is defined as a baseline threshold. Model (3) which includes multilevel random effects is known as the multilevel thresholds of change model (MTCM) [11]
is defined as a baseline threshold. Model (3) which includes multilevel random effects is known as the multilevel thresholds of change model (MTCM) [11]3. Results
| Variable | Mean | Median | Min. | Max. | N = 1389 | % | |
|---|---|---|---|---|---|---|---|
| Mother attended School | |||||||
| 1. None | 290 | 20.9 | |||||
| 2. Primary | 812 | 58.5 | |||||
| 3. At least secondary | 287 | 20.7 | |||||
| Type of Health Facility | |||||||
| 1. Government hospital | 417 | 30.0 | |||||
| 2. Government health centre | 672 | 48.4 | |||||
| 3. Christian Association of Malawi (CHAM) | 189 | 13.6 | |||||
| 4. Local health post | 21 | 1.5 | |||||
| 5. Local private clinic | 90 | 6.5 | |||||
| Whether Non Governmental Organisation(NGO) | |||||||
| 1. Exists | 611 | 44.0 | |||||
| 2. Does not exist | 778 | 56.0 | |||||
| Whether Health Surveillance Assistant (HSA) | |||||||
| 1. Exists | 951 | 68.5 | |||||
| 2. Does not exist | 438 | 31.5 | |||||
| Maternal age | 35 | 30 | 15 | 89 | 1,389 | 100 | |
| Variable | Estimate | 95% CI |
|---|---|---|
| Threshold | ||
 | −1.465 | (−1.986,−0.944) |
 | 1.053 | (0.508,1.598) |
| No School | (Reference group) | |
| Primary school | ||
 | −0.233 | (−0.572,0.106) |
 | −0.572 | (−0.935,−0.209) |
| Secondary School | ||
| | −0.364 | (−0.795,0.067) |
| | −0.534 | (−0.975,−0.093) |
| Government hospital | (Reference group) | |
| Government Health centre | ||
| | 0.238 | (−0.148,0.624) |
| | 0.323 | (−0.055,0.701) |
| CHAM | ||
| | 0.684 | (0.092,1.276) |
| | 1.331 | (0.725,1.937) |
| Health Post | ||
| | 1.023 | (0.049,1.997) |
| | 1.307 | (−0.081,2.695) |
| Local private clinic | ||
| | −0.063 | (−0.806,0.680) |
| | −0.170 | (−0.781,0.441) |
| Age | ||
| | −0.306 | (−0.453,−0.159) |
| | 0.028 | (−0.113,0.169) |
| NGO exists | (Reference group) | |
NGO does not exist  | 0.275 | (−0.011,0.561) |
| HSA exists | (Reference group) | |
| HSA does not exist | −0.091 | (−0.328,0.146) |
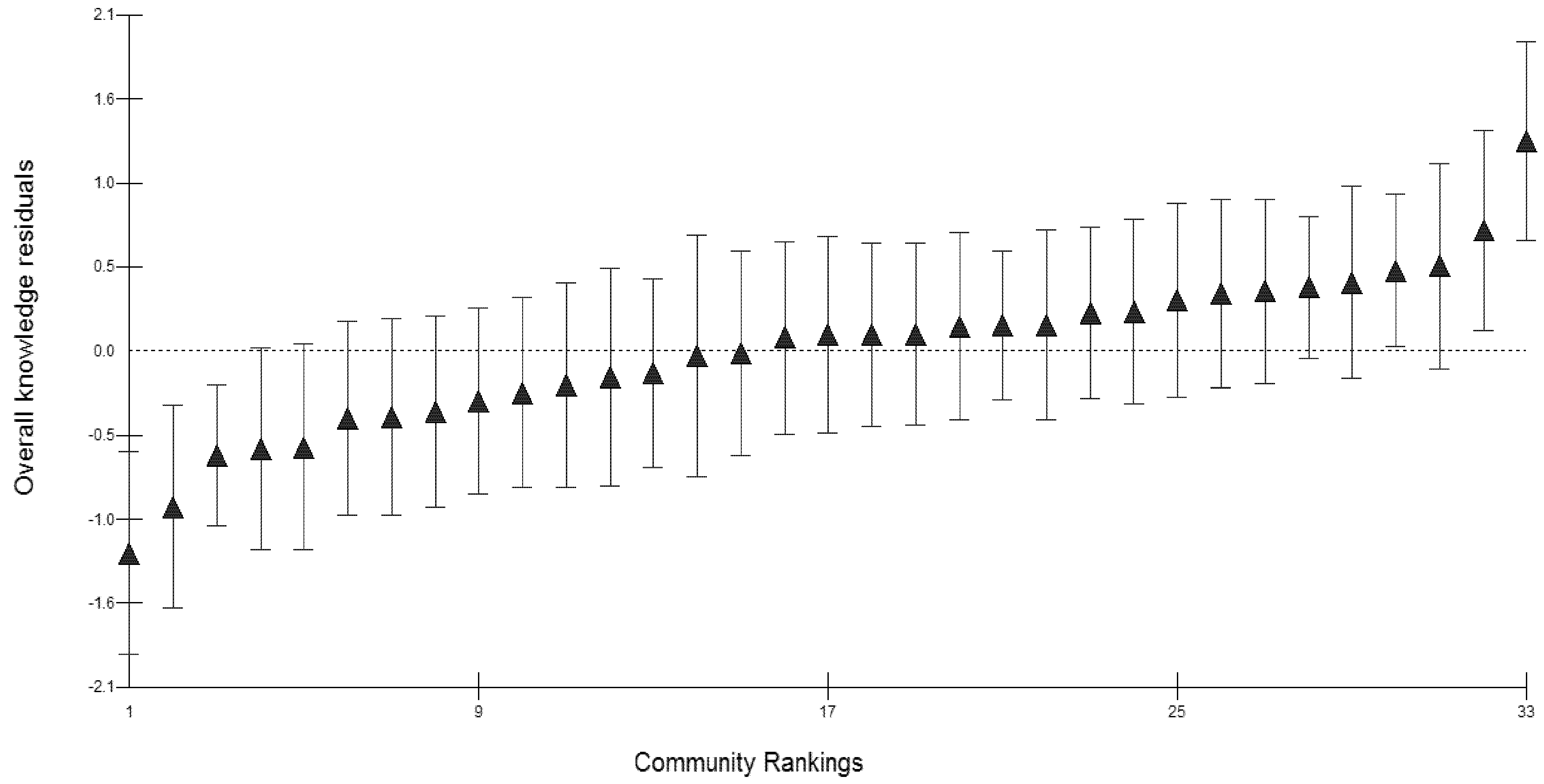
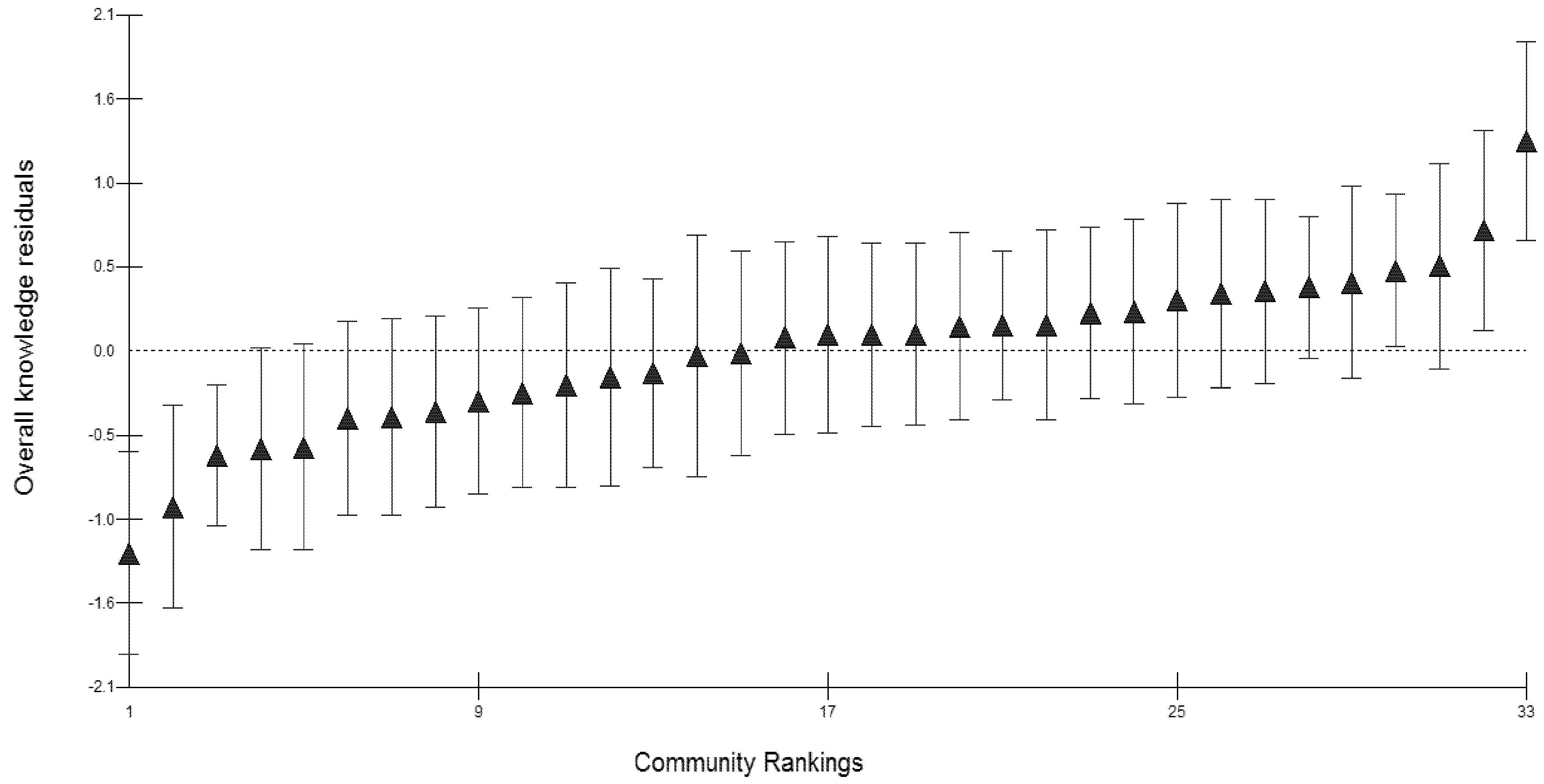
Community effects  | 0.623 | (0.219,1.027) |
| Variable | Causes of diarrhoea | Prevention methods | Overall knowledge on diarrhoea | |||
|---|---|---|---|---|---|---|
| estimate | 95% CI | estimate | 95% CI | estimate | 95% CI | |
Threshold  | −4.122 | (−4.782,−3.461) | −0.803 | (−1.160,−0.446) | −1.653 | (−2.235,−1.071) |
 | −0.756 | (−1.211,−0.301) | 0.737 | (0.380,1.094) | −0.137 | (−0.691,0.418) |
 | 0.615 | (0.158,1.072) | 2.209 | (1.750,2.668) | 1.281 | (0.601,1.961) |
Primary school  | −0.069 | (−0.339,0.201) | −0.090 | (−0.349,0.169) | −0.289 | (−0.554,−0.024) |
 | ||||||
 | ||||||
| Secondary School | 0.070 | (−0.275,0.415) | −0.415 | (−0.740,−0.090) | −0.418 | (−0.757,−0.079) |
| | ||||||
| | ||||||
| Health centre | 0.625 | (0.307,0.942) | −0.170 | (−0.491,0.151) | 0.199 | (−0.118,0.516) |
| | −0.583 | (−0.902,−0.263) | ||||
| | −0.357 | (−0.764,0.051) | ||||
| CHAM | 1.044 | (0.518,1.569) | 0.220 | (−0.237,0.677) | 0.940 | (0.436,1.444) |
| | −0.211 | (−0.652,0.230) | ||||
| | −0.053 | (−0.610,0.504) | ||||
| Health Post | −0.244 | (−1.085,0.597) | −0.092 | (−1.127,0.943) | 0.054 | (−0.765,0.873) |
| | −0.716 | (−1.633,0.201) | ||||
| | −0.019 | (−1.366,1.327) | ||||
| Local private clinic | 0.844 | (0.276,1.412) | 0.247 | (−0.312,0.806) | 0.442 | (−0.099,0.983) |
| | 0.127 | (−0.412,0.666) | ||||
| | 0.150 | (−0.558,0.858) | ||||
| Age | 0.126 | (0.020,0.232) | 0.180 | (0.074,0.286) | 0.002 | (−0.008,0.012) |
| | 0.008 | (0.000,0.016) | ||||
| | 0.025 | (0.009,0.041) | ||||
| No NGO | −0.030 | (−0.297,0.237) | 0.278 | (0.002,0.554) | 0.207 | (−0.056,0.470) |
| | 0.142 | (−0.117,0.401) | ||||
| | −0.007 | (−0.336,0.322) | ||||
| No HSA | 1.040 | (0.507,1.573) | 0.617 | (0.362,0.872) | 0.605 | (0.380,0.830) |
| | 0.571 | (0.320,0.822) | 0.466 | (0.217,0.715) | ||
| | 0.611 | (0.323,0.899) | 0.578 | (0.225,0.931) | ||
| Community effects ( ) | 0.352 | (0.085,0.619) | 0.063 | (−0.027,0.153) | 0.366 | (0.107,0.625) |
4. Discussion
5. Conclusions
Acknowledgements
References
- Fewtrell, L.; Colford, J.M. Water, Sanitation and Hygiene: Interventions and Diarrhoea. A Systematic Review and Meta-Analysis; Health Nutrition and Population Discussion Paper (HNP); The World Bank: Washington, DC, USA, 2004. [Google Scholar]
- Morse, T.D. A Public Health Approach to Reducing Diarrhoea Caused by Infectious Diseases in Children Less Than 5 Years of Age—the Example of Childhood Cryptosporidiosis in Malawi. Ph.D. Thesis, University of Strathclyde, Glasgow, UK, 2006. [Google Scholar]
- Tumwine, J.K.; Thompson, J.; Katua-Katua, M.; Mujwajuzi, M.; Johnstone, N.; Wood, E.; Porras, I. Diarrhoea and effects of different water sources, sanitation and hygiene behaviour in East Africa. Trop. Med. Int. Health 2002, 7, 750–757. [Google Scholar]
- Suchman, E.A. Sociomedical variations among ethnic groups. Am. J. Sociol. 1964, 70, 319–331. [Google Scholar]
- Maina-Ahlberg, B. Beliefs and Practices Related to Measles and Acute Diarrhoea. In Maternal and Child Health in Rural Kenya: An Epidemiological Study; Ginneken, J.K., Muller, A.S., Eds.; Routledge: London, UK, 1984; Volume Chapter 24, pp. 323–332. [Google Scholar]
- Liefbroer, A.C.; Elzinga, C.H. Intergenerational Transmission of Behavioural Patterns: Similarity of Parents’ and Children’s Family Life Trajectories; Draft Paper; Dept of Social Research Methodology, Vrije Universiteit: Amsterdam,The Netherlands, 2006. [Google Scholar]
- Sadique, M.Z.; Asadullah, M. Impact of Public Health Program and Maternal Education on Immunisation Behaviour of Children in Rural Bangladesh. In Proceedings of the the Annual Meeting of the Economics of Population Health: Inaugural Conference of the American Society of Health Economists, TBA, Madison, WI, USA, 4 June 2006.
- Measure DHS Demographic and Health Surveys. Malawi Demographic and Health Survey 2004; Calverton, MD, USA. Available online: www.measuredhs.com (accessed on 20 May 2010).
- Kandala, N.B.; Magadi, M.A.; Madise, N.J. An investigation of district spatial variations of childhood diarrhoea and fever morbidity in Malawi. Soc. Sci. Med. 2006, 62, 1138–1152. [Google Scholar]
- World Health Statistics. Country Health System Fact Sheet 2006; Malawi, 2006. Available online: http://www.who.int/whosis/en/ (accessed on 7 March 2012).
- Hedeker, D.; Mermelstein, R.J. A multilevel thresholds of change model for analysis of stages of change data. Multivar. Behav. Res. 1998, 33, 427–455. [Google Scholar]
- Fielding, A. Why use arbitrary points scores? Ordered categories in models of education progress. J. R. Stat. Soc. Ser. A 1999, 162, 303–330. [Google Scholar]
- Leyland, A.H.; Goldstein, H. Multilevel Modelling of Health Statistics; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2001. [Google Scholar]
- Fielding, A.; Yang, M.; Goldstein, H. Multilevel ordinal models for examination grades. Stat. Model. 2003, 3, 127–153. [Google Scholar]
- Rasbash, J.; Steele, F.; Browne, W.; Prosser, B. A User’s Guide to MLwiN Version 2.0; Centre for Multilevel Modelling, University of Bristol: Bristol, UK, 2004; pp. 102–136. [Google Scholar]
- Browne, W.J. MCMC Estimation in MLwiN; Centre for Multilevel Modelling Institute of Education, University of London: London, UK, 2003. [Google Scholar]
- Berrington, A.M.; Hu, Y.; Ramirez-Ducoing, K.; Smith, P.W.F. Multilevel Modelling of Repeated Ordinal Measures: An Application to Attitude Towards Divorce; Southampton Statistical Sciences Research Institute Applications and Policy Working Paper M05/10 and ESRC Research Methods Programme Working Paper No 26; The University of Manchester: Manchester, UK, 2005. [Google Scholar]
- Ziba, C.; Slutsker, L.; Chitsulo, L.; Steketee, R.W. Use of malaria prevention measures in Malawian households. Trop. Med. Parasitol. 1994, 45, 70–73. [Google Scholar]
- Uza, M.; Phommpida, S.; Toma, T.; Takakura, M.; Manivong, K.; Bounyadeth, S.; Kobayashi, J.; Koja, Y.; Ozasa, Y.; Miyagi, I. Knowledge and behaviour relating to malaria in malaria endemic villages of Khammouane province, Lao PDR. South. Asian J. Trop. Med. Public Health 2002, 33, 246–254. [Google Scholar]
- Nieto, T.; Méndez, F.; Carrasquilla, G. Knowledge, beliefs and practices relevant for malaria control in an endemic urban area of the Colombian Pacific. Soc. Sci. Med. 1999, 49, 601–609. [Google Scholar]
- Verhaeghen, P.; Salthouse, T.A. Meta-analyses of age-cognition relations in adulthood: Estimates of linear and nonlinear age effects and structural models. Psychol. Bull. 1997, 122, 231–249. [Google Scholar]
- Schroeder, D.H.; Salthouse, T.A. Age-related effects on cognition between 20 and 50 years of age. Personal. Individ. Differ. 2004, 36, 393–404. [Google Scholar]
- Masangwi, S.J.; Morse, T.D.; Ferguson, N.; Zawdie, G.; Grimason, A.M.; Namangale, J.J. Behavioural and environmental determinants of childhood diarrhoea in Chikwawa, Malawi. Desalination 2009, 248, 684–691. [Google Scholar] [CrossRef]
2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Masangwi, S.J.; Grimason, A.M.; Morse, T.D.; Kazembe, L.; Ferguson, N.; Jabu, G.C. Pattern of Maternal Knowledge and Its Implications for Diarrhoea Control in Southern Malawi: Multilevel Thresholds of Change Analysis. Int. J. Environ. Res. Public Health 2012, 9, 955-969. https://doi.org/10.3390/ijerph9030955
Masangwi SJ, Grimason AM, Morse TD, Kazembe L, Ferguson N, Jabu GC. Pattern of Maternal Knowledge and Its Implications for Diarrhoea Control in Southern Malawi: Multilevel Thresholds of Change Analysis. International Journal of Environmental Research and Public Health. 2012; 9(3):955-969. https://doi.org/10.3390/ijerph9030955
Chicago/Turabian StyleMasangwi, Salule Joseph, Anthony Martin Grimason, Tracy Dawn Morse, Lawrence Kazembe, Neil Ferguson, and George Christopher Jabu. 2012. "Pattern of Maternal Knowledge and Its Implications for Diarrhoea Control in Southern Malawi: Multilevel Thresholds of Change Analysis" International Journal of Environmental Research and Public Health 9, no. 3: 955-969. https://doi.org/10.3390/ijerph9030955
APA StyleMasangwi, S. J., Grimason, A. M., Morse, T. D., Kazembe, L., Ferguson, N., & Jabu, G. C. (2012). Pattern of Maternal Knowledge and Its Implications for Diarrhoea Control in Southern Malawi: Multilevel Thresholds of Change Analysis. International Journal of Environmental Research and Public Health, 9(3), 955-969. https://doi.org/10.3390/ijerph9030955