Abstract
This study was designed to understand the status of HIV/AIDS knowledge, attitude and practice (KAP) among different populations and to provide scientific evidences for further health education. Three rounds of questionnaires were administered among service industry workers who were selected through stratified cluster sampling. Study subjects included hotel attendants, employees of beauty parlors and service workers of transportation industry. Data were analyzed using the analytical hierarchy process. All demonstrated high KAP overall. Synthetic scoring indexes of the three surveys were above 75%. However, the correct response rate on questions whether mosquito bite can transmit HIV/AIDS and what is the relationship between STD with HIV was unsatisfactory (lower than expected); and their attitudes towards people living with HIV and AIDS need to be improved. Moreover, the effect of health education on these groups was unclear. In conclusion, analytical hierarchy process is a valid method in estimating overall effect of HIV/AIDS health education. Although the present status of HIV/AIDS KAP among the service industry workers was relatively good, greater efforts should be made to improve their HIV transmission knowledge, attitude and understanding of the relationship between STDs and HIV.
Introduction
The global HIV epidemic has caused widespread concern because of its high fatality rate without treatment and its difficulty to control. The cumulative number of people living with HIV in China has reached 650,000 since the first case was discovered in 1985[1], and the infection rate is rapidly rising. There is no vaccine or cure for HIV. One key for preventing and controlling HIV is to popularize HIV knowledge leading to healthy or safe lifestyles among the public, so health education is the only valid mean of controlling AIDS’ epidemic [2].Health education of HIV has been implemented for many years in China; however, their assessment of health educational effect is usually done by single index.Relying on single methods of assessment has its disadvantages, for it cannot attain integrated results.Therefore, it is necessary to assess the integrated effect of health education in a way which incorporates variables, including knowledge, attitude and practice.
The analytical hierarchy process (AHP) is a decision aiding method developed by Saaty [3]. It is a systematic analysis technique for solving multiple criteria decision problems. The objective of this paper is to establish an integrated assessment method for assessing the actual effect of health education among different population. AHP is applied to establish the integrated assessment model.
Subjects and Methods
Subjects
A total of 655 subjects who were working as hotel waiters, beauty salon stewards, barbers and long-distance truck drivers were selected from the registered system of a Chinese city by stratified and cluster sampling (10%).
Methods
The questionnaire was based on the WHO model for questionnaire design for which reliability and validity of the questionnaire were established. Contents of the questionnaire included the general characteristics of study participants and their knowledge, attitude and practice regarding HIV. Health education campaign was initiated after the baseline investigation. Health education included hanging posters, intensive training, scolumns in newspapers and magazines, radio spots, television promotions and SMS. The same questionnaire used at baseline was administered at one week and 24 weeks. The basic description of the data in this study can also be found in “To evaluate the effect of health education about AIDS’ knowledge, attitude and practice among service industries attendants” [4]. In this paper, AHP is used to assess the integrated effect of health education on HIV.
The Analytic Hierarchy Process
The analytic hierarchy process (AHP), which was first developed by Saaty, has been an effective tool in structuring and modeling multi-objective problems [5]. AHP can assist decision makers with the evaluation of problems in the form of a hierarchy of references through a series of pair-wise comparisons of relative criteria. Briefly, relative weights are determined through pair-wise comparison. The method can break down the unstructured complex scorecard problems and then turn them into component parts. Hierarchical orders are then arranged by forming value tree structures. A major strength of AHP is the pair-wise comparison as described in the following section where the influence of the elements of a particular level over those of a lower level is measured. Subjective judgments on the relative importance of each part are represented by assigning numerical values; the numerical values are selected in accordance with Fig.1. The comparison is based on an expert’s opinion and the experience gained from the observation and continuous learning of the system behavior [6]. The relative importance is then used to construct a preference matrix, from which the weighs for each variable will be extracted [5].

Figure 1:.
Pair-wise comparison scales (importance).
Indexes and the Tree Structure
Indexes and their variable names
Indexes about HIV knowledge, attitude and practice and their variable names are presented in table1.

Table1:.
Indexes about AIDS’ KAP and their variable names
The Tree Structure
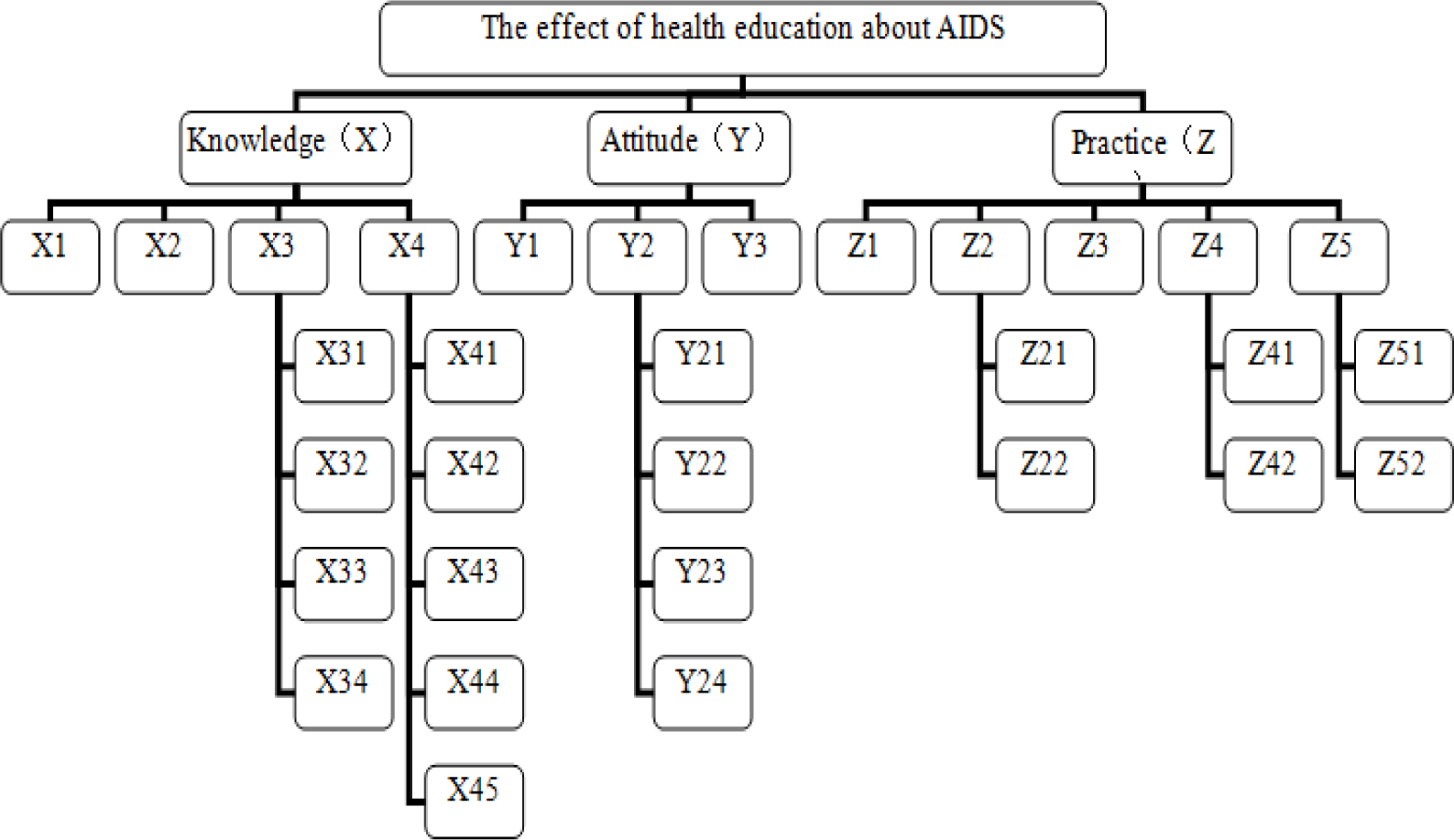
The overall goal is divided into four levels. The first level is the overall goal (the effect of KAP health education about HIV); the second is the three major variables (knowledge, attitude and practice); the third and the fourth are n alternatives that must be compared and assessed. The tree structure is showed in figure 2.
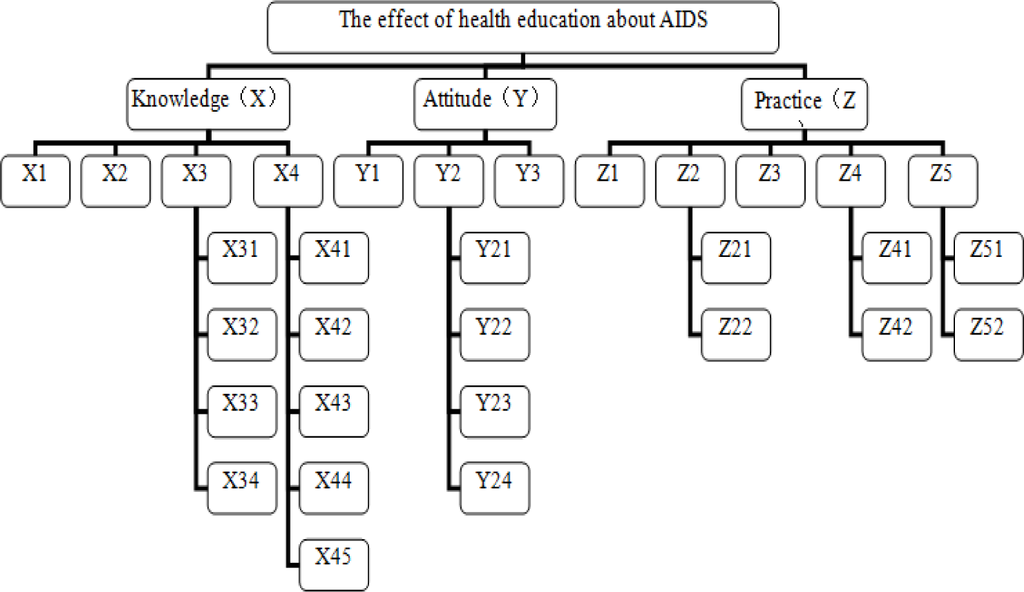
Figure 2:.
The tree structure about AIDS’ KAP investigation
Determination of weight
The AHP method is a matrix-based approach. It is a theory for measuring impact priorities in a hierarchical structure [5].
After a matrix has been formed, the relative weights of each element need to be derived. The method uses the pair-wise comparison of the relative influence of factors taken two at a time and arranged in the form of a matrix. If we denote the relative influence ith factor with respect to jth factor by aij, then, 1/aij represents the relative influence of jth factor with respect to ith factor. The (n×n) reciprocal judgment matrix obtained by arranging these pair-wise comparison ratios is used to compute the priority vector. Matrix [A] shows the relative importance among knowledge, attitude and practice. The pair-wise comparison matrix [A] for calculating weights are listed below, see formula (1) and formula (2).
| A | X | Y | Z | W |
|---|---|---|---|---|
| X | 1(a11) | 5(a12) | 3(a13) | 0.6267 |
| Y | 1/5(a21) | 1(a22) | 1/4(a23) | 0.0936 |
| Z | 1/3(a31) | 4(a32) | 1(a33) | 0.2797 |
Weights of others matrices can be attained according to the same process. The relative importance of four indexes about AIDS’ knowledge is showed in matrix [BX].
| BX | X1 | X2 | X3 | X4 | W |
|---|---|---|---|---|---|
| X1 | 1 | 1/2 | 1/3 | 1/3 | 0.1089 |
| X2 | 2 | 1 | 1/2 | 1/2 | 0.1887 |
| X3 | 3 | 2 | 1 | 1 | 0.3512 |
| X4 | 3 | 2 | 1 | 1 | 0.3512 |
The relative importance of three indexes about AIDS’ attitude is showed in matrix [BY].
| BY | Y1 | Y2 | Y3 | W |
|---|---|---|---|---|
| Y1 | 1 | 1/2 | 1/5 | 0.1125 |
| Y2 | 2 | 1 | 1/5 | 0.1786 |
| Y3 | 5 | 5 | 1 | 0.7088 |
The relative importance of five indexes about AIDS’ practice is showed in matrix [BZ].
| BZ | Z1 | Z2 | Z3 | Z4 | Z5 | W |
|---|---|---|---|---|---|---|
| Z1 | 1 | 1 | 4 | 2 | 1/3 | 0.1997 |
| Z2 | 1 | 1 | 4 | 2 | 1/3 | 0.1997 |
| Z3 | 1/4 | 1/4 | 1 | 1/3 | 1/4 | 0.0574 |
| Z4 | 1/2 | 1/2 | 3 | 1 | 1/3 | 0.1244 |
| Z5 | 3 | 3 | 4 | 3 | 1 | 0.4187 |
The relative importance of four indexes about AIDS’ routes of transmission is showed in matrix [CX3].
| CX3 | X31 | X32 | X33 | X34 | W |
|---|---|---|---|---|---|
| X31 | 1 | 2 | 2 | 1 | 0.3333 |
| X32 | 1/2 | 1 | 1 | 1/2 | 0.1667 |
| X33 | 1/2 | 1 | 1 | 1/2 | 0.1667 |
| X34 | 1 | 2 | 2 | 1 | 0.3333 |
Weights of five indexes about AIDS’ routes of no transmission are equal (w=1/5=0.2) in matrix [CX4] because they show the same function. Weights of four indexes about the attitude to AIDS’ patients and HIV-carriers are equal (w=1/4=0.25) in matrix [CY2] because they show the same function. Weights of two indexes about sex are equal (w=1/2=0.5) in matrix [CZ2] because they show the same function. Weights of two indexes about the practice to AIDS’ patients and HIV-carriers are showed in matrix [CZ4].
| CZ4 | Z41 | Z42 | W |
|---|---|---|---|
| Z41 | 1 | 1/2 | 0.3333 |
| Z42 | 2 | 1 | 0.6667 |
Weights of two indexes about the behavior of AIDS’ knowledge are showed in matrix [CZ5].
| CZ5 | Z51 | Z52 | W |
|---|---|---|---|
| Z51 | 1 | 1/2 | 0.3333 |
| Z52 | 2 | 1 | 0.6667 |
The Consistency Test
The consistency index (CI) and the critical ratio (CR) of every matrix must be calculated in order to judge the consistency of matrix. The matrix is considered to be consistent and accepted if the value of CR is less than 0.10[5]. Otherwise, it must be adjusted. The consistency test of matrix [A] is done as follows according to the formula (3), (4), (5), (6).
Where RI is the random index and the numerical values are attained in accordance to table 2.
Table 2:.
The values of the random index
With the same calculation procedure, consistency tests are conducted for others matrices. The results of the consistency tests are showed in Table 3.
Table 3:.
The results of the consistency tests
Calculation of the Integrated Assessment Index (IAI)
The integrated assessment index is a useful index for assessing overall goal. It is calculated according to the formula (7). The Integrated indexes of three investigations are showed in table 4.
Table 4:.
The results of evaluating integrated in three investigations among service industries attendants.
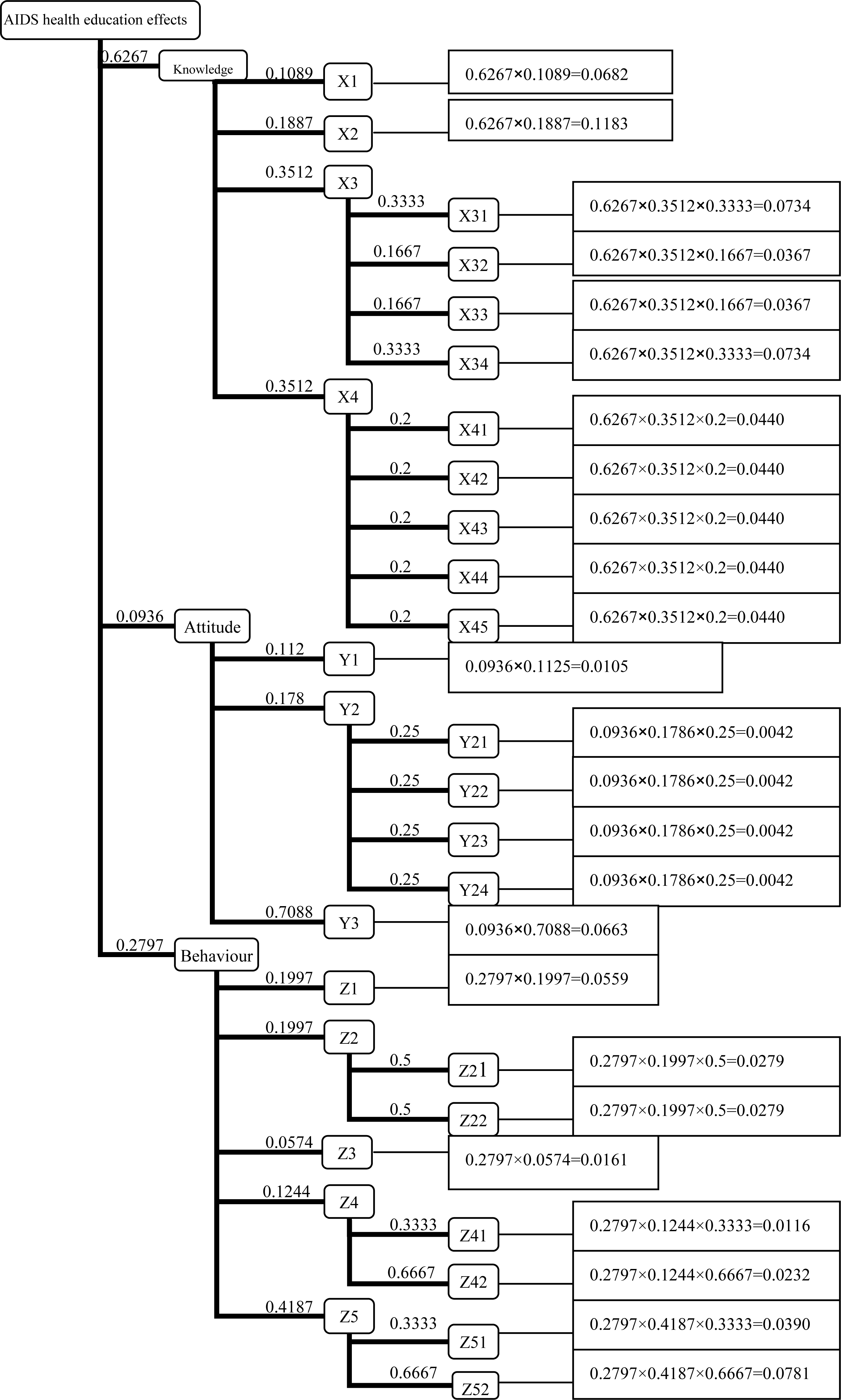
Where Ci is combination weight and Pi is the percentage of correct answers of the same objective question. Combination weight (Ci) is calculated by multiplying weights of all indexes in every level according to the principle of probability multiplication. The calculation processes are presented in figure 3.
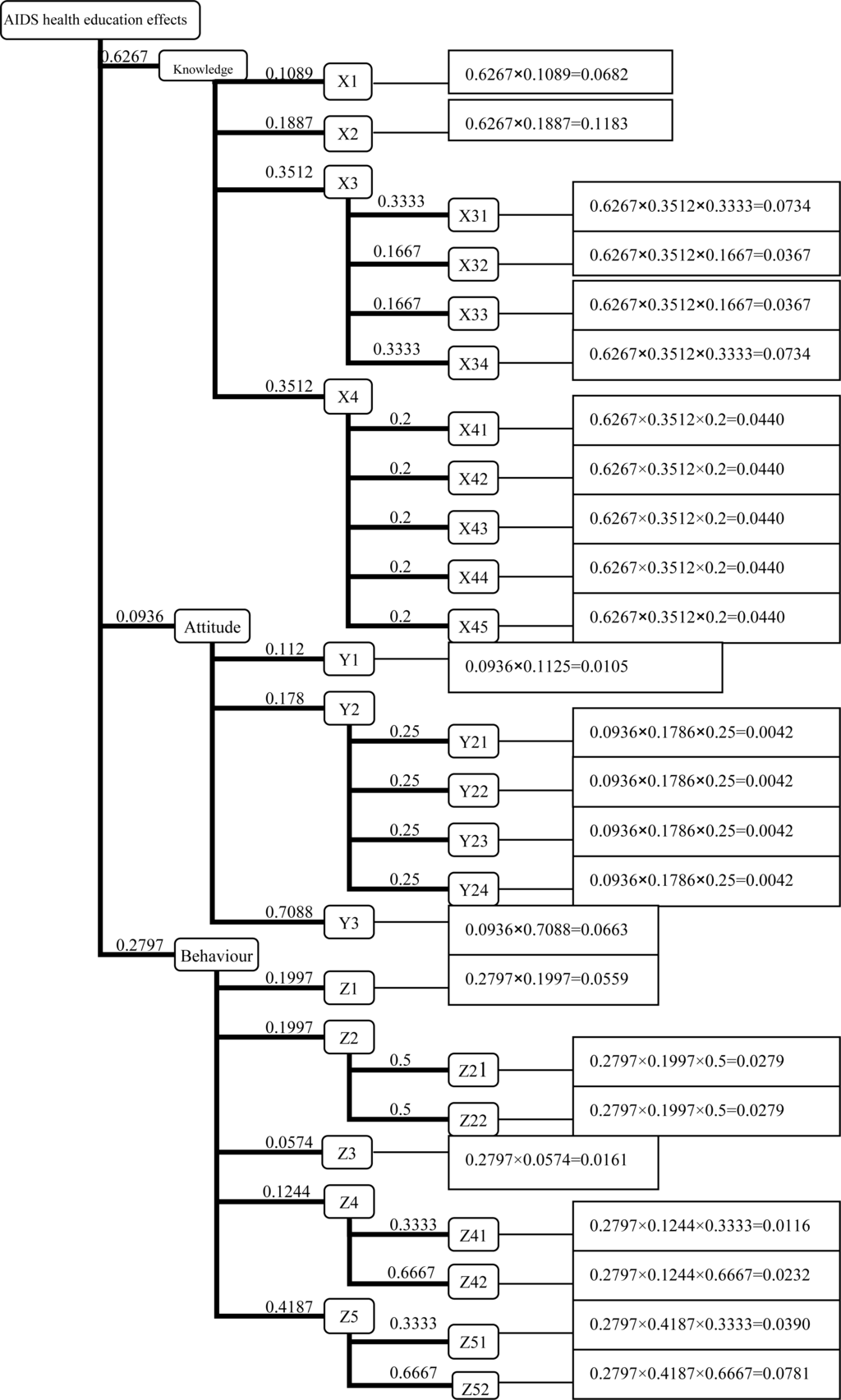
Figure 3:.
The calculation of combination weigh of every alternative
Results and Discussion
The overall results of HIV KAP among service industries workers are good. Their integrated assessment indexes (IAI) of three investigations are above 75%. IAI went up significantly after health education and, the effect of health education was maintained. Although the knowledge rate of most questions is in accordance with Chinese standard (above 75%) [7], there are still many shortcomings that urgently need to be improved. For example, only 52.4% of people knew that insect’s bites do not transmit HIV. Although knowledge rate of mosquito bites is significantly rising after health education, it dropped to the primary level (56.3%) six months later. The results about the attitude to AIDS’ patients and HIV-carriers are not ideal, and health education was not shown to be effective in changing attitude. In addition, the result of a vague relationship between STIs and HIV is showed in term of subjects’ practice. Only 51.3% of people knew that STIs should be treated in order to prevent HIV transmission. From these results, we can learn that some aspects must be further strengthened in future health education programs in order to prevent and control the HIV epidemic effectively.
In this paper, an integrated method for assessing and comparing the effect of health education was described. When incorporating all variables in the integrated assessment model, the AHP can be a useful method to evaluate health education campaigns comprehensively. The IAI values of three investigations obtained by using the AHP to reflect the results of all questions about AIDS’ knowledge, attitude and practice. In comparison with the results of assessments reported by other researchers, we conclude that this integrated assessment method is a more useful, reasonable, and acceptable method for the assessment of the effectiveness of health education.

References
- China Ministry of Health and UN Theme Group on HIV/AIDS in China. Assessment Report on HIV/AIDS in China in 2004; People’s Health Press: Beijing, 2004; pp. 1–65. [Google Scholar]
- Lijun, Y; Hongguan, F; Xiaojing, Y. Health education is the most valid vaccine of controlling HIV/AIDS prevalence. J. Chinese Health Education 2000, 16(1), 47. [Google Scholar]
- Saaty, TL. A scaling method for priorities in hierarchical structures. J. Math. Psychol 1997, 15, 234–281. [Google Scholar]
- Jianyan, L; Fengjie, W; Hong, L. To evaluate the effect of health education about AIDS’ knowledge, attitude and practice among service industries attendants. J. Chinese Public Health. 2004, 20 Supplement, 81–82. [Google Scholar]
- Saaty, TL. The analytic hierarchy process, planning, priority setting, resource allocation, The Wharton School, University of Pennsylvania; McGraw-Hill: New York, 1980; pp. 15–32. [Google Scholar]
- Ayyub, BM. Guidelines on Expert-Opinion Elicitation of Probabilities and Consequence for Corps Facilities. Institute for Water Resources. USACE 1999, 1–23. [Google Scholar]
- The China Ministry of Health. The Medium-long Programs of Preventing and Controlling HIV/AIDS in China (1998–2010). Chinese Journal of AIDS & STD 1999, 5(1), 45–48. [Google Scholar]
© 2007 MDPI All rights reserved.