
Preferences of South African Adolescents Living with HIV in the Western Cape Province Regarding the Use of Digital Technology for Self-Management


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Participants
2.4. Data Collection
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Theme 1: Everyday Usage of Digital Technology
3.1.1. Subtheme 1.1: Integrating Digital Technology into Daily Life
“I use my smartphone for everything, from chatting with friends to doing my homework.”(Participant 1, aged 20, Focus group 1)
“Sometimes I’m using my sister’s laptop.”(Participant 3, aged 19, Focus group 2)
“Because I don’t even know how to use the other apps. That’s why I like Facebook and WhatsApp. That’s all I like.”(Participant 3, aged 19, Focus group 2)
“I once searched for an essay for my history, so I took notes from there, and then I did my essay because Facebook has a free mode.”(Participant 1, aged 16, Focus group 3)
“We are using computers, for example, the subject I do at school I’m doing computer application technology, and we also do the practical that can teach us the technology.”(Participant 3, aged 19, Focus group 2)
“I love TikTok and YouTube, even Facebook.”(Participant 2, aged 15, Focus group 6)
“Candy Crush and Bubble Shooter and 2248 are about numbers”(Participant 4, aged 21, Focus group 2)
3.1.2. Subtheme 1.2: Popular Digital Platforms and Their Uses
“It can be helpful by creating a WhatsApp group and also on Facebook creating a group because I don’t have data so there’s a free mode on Facebook.”(Participant 4, aged 21, Focus group 2)
“And I also use Google or YouTube when I’m watching movies.”(Participant 3, aged 19, Focus group 2)
“Most of the time I’m using TikTok because I enjoy watching videos and also WhatsApp, Facebook and YouTube.”(Participant 1, aged 19, Focus group 2)
3.2. Theme 2: Role of Digital Technology in Self-Management
Subtheme 2.1: Using Technology for Personal Health Management
“I use the phone to set alarms for my meals because I eat four times a day and to take my pills. The phone helps me to get a reminder to take my medication.”(Participant 2, aged 20, Focus group 4)
“I use my phone only for waking up as an alarm and also as a reminder for taking medication.”(Participant 5, aged 20, Focus group 4)
“I use the phone to search for healthy food.”(Participant 2, aged 20, Focus group 4)
“I had a boil on my armpit, so I went to Google and searched how to heal it and what caused it.”(Participant 1, aged 16, Focus group 3)
“There is an AI on my WhatsApp. The AI gives me advice, and I can talk to it about stuff that I can’t talk to my mother about.”(Participant 2, aged 18, Focus group 3)
3.3. Theme 3: Factors Influencing Digital Technology Use
3.3.1. Subtheme 3.1: Connectivity and Internet Access
“When there is load shedding, there’s a problem with the network, and also some people have Wi-Fi, so when there’s load shedding, they can’t use their Wi-Fi because the Wi-Fi is off, so there’s no Internet.”(Participant 4, aged 21, Focus group 2)
“I’m using Wi-Fi, but when I’m not at home, I’m using my phone data.”(Participant 6, aged 20, Focus group 4)
3.3.2. Subtheme 3.2: Privacy and Digital Security
“If I give you my phone to do the research and then there’s going to be like, WhatsApp and all of those apps, then I put like a fingerprint to get into it because you need my fingerprint to get into it. That way, I will feel safer.”(Participant 4, aged 15, Focus group 4)
3.3.3. Subtheme 3.3: Assessing Information Credibility
“I’m not actually sure if I must trust the Internet because when I must do my research tasks, they give me answers to other questions that I did not ask, but then if I must write that down and go back to school, they say no, this is not right, do this over.”(Participant 4, aged 15, Focus group 4)
“I don’t like this, so I would rather go ask the person who does the job himself how and why.”(Participant 4, aged 15, Focus group 4)
“I will say that I trust it because when someone tells me about something, and then I am not sure about it, I’ll go to Google and Google it and see if it is true or not. So, I trust it.”(Participant 4, aged 21, Focus group 2)
“The schoolwork I was also getting right because of Google.”(Participant 2, aged 21, Focus group 5)
“Because everything that I’m searching for, it is giving a clue but not the real thing.”(Participant 1, aged 20, Focus group 1)
3.3.4. Subtheme 3.4: Family and Peer Dynamics
“My family is very supportive. All of them would like phone just to remind me and say, listen, you must not forget about you tablets”(Participant 4, aged 15, Focus group 4)
“Yes, especially with TikTok. I didn’t like this before and then my dad said I must download it because there’s a child who likes to cook like you, so then I downloaded it.”(Participant 2, aged 21, Focus group 5)
“If it’s coming from friends, I ignore it, but if it’s coming from one of the family members, that’s when I will start to give more attention to it.”(Participant 5, aged 19, Focus group 1)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ALHIV | Adolescents Living with HIV |
| DHT | Digital Health Technology |
| CHCs | Community Health Centers |
| HIV | Human Immunodeficiency Virus |
| mHealth | Mobile Health |
| ATLAS.ti | Qualitative Data Analysis Software |
| SMS | Short Message Service |
References
- The Joint United Nation Programme on HIV/AIDS. IN DANGER: UNAIDS Global AIDS Update 2022; UNAIDS: Geneva, Switzerland, 2022; Available online: https://www.unaids.org/en/resources/documents/2022/in-danger-global-aids-update (accessed on 30 May 2023).
- Zhou, S.A.-O.; Cluver, L.A.-O.X.; Shenderovich, Y.; Toska, E.A.-O. Uncovering ART adherence inconsistencies: An assessment of sustained adherence among adolescents in South Africa. J. Int. AIDS Soc. 2021, 24, e25832. [Google Scholar] [CrossRef] [PubMed]
- Human Sciences Research Council. SABSSM VI Shows Prevalence Peak Shift to Older People 2023. Available online: https://hsrc.ac.za/news/public-health/sabssm-vi-shows-prevalence-peak-shift-to-older-people/ (accessed on 30 May 2023).
- Human Sciences Research Council. New HIV Survey Highlights Progress and Ongoing Disparities in South Africa’s HIV Epidemic; Human Sciences Research Council: Pretoria, South Africa, 2019. [Google Scholar]
- Simbayi, L.C.; Zuma, K.; Zungu, N.; Moyo, S.; Marinda, E.; Jooste, S.; Mabaso, M.; Ramlagan, S.; North, A.; Van Zyl, J.; et al. South African National HIV Prevalence, Incidence, Behaviour and Communication Survey, 2017; HSRC Press: Cape Town, South Africa, 2019. [Google Scholar]
- Chem, E.D.; Ferry, A.; Seeley, J.; Weiss, H.A.; Simms, V. Health-related needs reported by adolescents living with HIV and receiving antiretroviral therapy in sub-Saharan Africa: A systematic literature review. J. Int. AIDS Soc. 2022, 25, e25921. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.; Burton, P. Child and adolescent mental health and the digital world: A double-edged sword. In South African Child Gauge 2021/2022; Tomlinson, M., Kleintjes, S., Lake, L., Eds.; Children’s Institute, University of Cape Town: Cape Town, South Africa, 2022. [Google Scholar]
- Henwood, R.; Patten, G.; Barnett, W.; Hwang, B.; Metcalf, C.; Hacking, D.; Wilkinson, L. Acceptability and use of a virtual support group for HIV-positive youth in Khayelitsha, Cape Town using the MXit social networking platform. AIDS Care 2016, 28, 898–903. [Google Scholar] [CrossRef]
- Zanoni, B.C.; Sibaya, T.; Cairns, C.; Haberer, J.E. Barriers to Retention in Care are Overcome by Adolescent-Friendly Services for Adolescents Living with HIV in South Africa: A Qualitative Analysis. AIDS Behav. 2019, 23, 957–965. [Google Scholar] [CrossRef]
- Weyers, L.; Crowley, T.; Tokwe, L. Digital technology for HIV self-management in low- and middle-income countries: A scoping review of adolescents’ preferences. AIDS Care 2024, 36, 1805–1814. [Google Scholar] [CrossRef]
- Radovic, A.; Badawy, S.M. Technology Use for Adolescent Health and Wellness. Pediatrics 2020, 145, S186–S194. [Google Scholar] [CrossRef] [PubMed]
- Hightow-Weidman, L.B.; Muessig, K.E.; Bauermeister, J.; Zhang, C.; LeGrand, S. Youth, Technology, and HIV: Recent Advances and Future Directions. Curr. HIV/AIDS Rep. 2015, 12, 500–515. [Google Scholar] [CrossRef]
- Badawy, S.M.; Shah, R.; Beg, U.; Heneghan, M.B. Habit Strength, Medication Adherence, and Habit-Based Mobile Health Interventions Across Chronic Medical Conditions: Systematic Review. J. Med. Internet Res. 2020, 22, e17883. [Google Scholar] [CrossRef]
- Tarantino, N.; Lartey, M.; Arnold, T.; Brown, L.; Kwara, A.; Guthrie, K. Preferences for a Game-Based SMS Adherence Intervention Among Young People Living with HIV in Ghana: A Qualitative Study. AIDS Behav. 2022, 26, 2169–2181. [Google Scholar] [CrossRef]
- Zanoni, B.C.; Archary, M.; Subramony, T.; Sibaya, T.; Psaros, C.; Haberer, J.E. “It was not okay because you leave your friends behind”: A prospective analysis of transition to adult care for adolescents living with perinatally-acquired HIV in South Africa. Vulnerable Child. Youth Stud. 2021, 16, 206–220. [Google Scholar] [CrossRef]
- Mulawa, M.I.; Hoare, J.; Knippler, E.T.; Mtukushe, B.; Matiwane, M.; Muessig, K.E.; Al-Mujtaba, M.; Wilkinson, T.H.; Platt, A.; Egger, J.R.; et al. MASI, a Smartphone App to Improve Treatment Adherence Among South African Adolescents and Young Adults With HIV: Protocol for a Pilot Randomized Controlled Trial. JMIR Res. Protoc. 2023, 12, e47137. [Google Scholar] [CrossRef] [PubMed]
- Adams, L.; Crowley, T. Adolescent human immunodeficiency virus self-management: Needs of adolescents in the Eastern Cape. Afr. J. Prim. Health Care Fam. Med. 2021, 13, 2756. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.; Halim, N.K.; Raeside, R.; Jia, S.S.; Hyun, K.; Boroumand, F.; Mandoh, M.; Singleton, A.C.; Phongsavan, P.; Redfern, J.; et al. How Helpful and What Is the Quality of Digital Sources of Healthy Lifestyle Information Used by Australian Adolescents? A Mixed Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 12844. [Google Scholar] [CrossRef]
- Bitto Urbanova, L.; Madarasova Geckova, A.; Dankulincova Veselska, Z.; Capikova, S.; Holubcikova, J.; van Dijk, J.P.; Reijneveld, S.A. Technology supports me: Perceptions of the benefits of digital technology in adolescents. Front. Psychol. 2022, 13, 970395. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Youth-Centred Digital Health Interventions: A Framework for Planning, Developing and Implementing Solutions with and for Young People; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child. Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Hennink, M.; Kaiser, B.N. Sample sizes for saturation in qualitative research: A systematic review of empirical tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef]
- Varga-Atkins, T.; McIsaac, J.; Willis, I. Focus Group meets Nominal Group Technique: An effective combination for student evaluation? Innov. Educ. Teach. Int. 2017, 54, 289–300. [Google Scholar] [CrossRef]
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef]
- Lincoln, Y.S.; Guba, E.G.; Pilotta, J.J. Naturalistic Inquiry: Beverly Hills, CA: Sage Publications, 1985, 416 pp., $25.00 (Cloth). Int. J. Intercult. Relat. 1985, 9, 438–439. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Couns. Psychother. Res. 2021, 21, 37–47. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual. Res. Psychol. 2021, 18, 328–352. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Toward good practice in thematic analysis: Avoiding common problems and be(com)ing a knowing researcher. Int. J. Transgend Health 2023, 24, 1–6. [Google Scholar] [CrossRef]
- L’Engle, K.L.; Mangone, E.R.; Parcesepe, A.M.; Agarwal, S.; Ippoliti, N.B. Mobile Phone Interventions for Adolescent Sexual and Reproductive Health: A Systematic Review. Pediatrics 2016, 138, e20160884. [Google Scholar] [CrossRef] [PubMed]
- Chory, A.; Callen, G.; Nyandiko, W.; Njoroge, T.; Ashimosi, C.; Aluoch, J.; Scanlon, M.; McAteer, C.; Apondi, E.; Vreeman, R. A Pilot Study of a Mobile Intervention to Support Mental Health and Adherence Among Adolescents Living with HIV in Western Kenya. AIDS Behav. 2022, 26, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Bhana, A.; Abas, M.A.; Kelly, J.; van Pinxteren, M.; Mudekunye, L.A.; Pantelic, M. Mental health interventions for adolescents living with HIV or affected by HIV in low- and middle-income countries: Systematic review. BJPsych Open 2020, 6, e104. [Google Scholar] [CrossRef] [PubMed]
- Zanoni, B.C.; Archary, M.; Sibaya, T.; Musinguzi, N.; Haberer, J.E. Transition from pediatric to adult care for adolescents living with HIV in South Africa: A natural experiment and survival analysis. PLoS ONE 2020, 15, e0240918. [Google Scholar] [CrossRef]
- Sánchez, S.A.; Ramay, B.M.; Zook, J.; de Leon, O.; Peralta, R.; Juarez, J.; Cocohoba, J. Toward improved adherence: A text message intervention in an human immunodeficiency virus pediatric clinic in Guatemala City. Medicine 2021, 100, e24867. [Google Scholar] [CrossRef]
- Abiodun, O.; Ladi-Akinyemi, B.; Olu-Abiodun, O.; Sotunsa, J.; Bamidele, F.; Adepoju, A.; David, N.; Adekunle, M.; Ogunnubi, A.; Imhonopi, G.; et al. A Single-Blind, Parallel Design RCT to Assess the Effectiveness of SMS Reminders in Improving ART Adherence Among Adolescents Living with HIV (STARTA Trial). J. Adolesc. Health 2021, 68, 728–736. [Google Scholar] [CrossRef]
- Giovanelli, A.; Ozer, E.M.; Dahl, R.E. Leveraging Technology to Improve Health in Adolescence: A Developmental Science Perspective. J. Adolesc. Health 2020, 67, S7–S13. [Google Scholar] [CrossRef]
- Gunnlaugsson, G.A.-O.; Whitehead, T.A.-O.; Baboudóttir, F.N.; Baldé, A.; Jandi, Z.; Boiro, H.; Einarsdóttir, J.A.-O. Use of Digital Technology among Adolescents Attending Schools in Bissau, Guinea-Bissau. Int. J. Environ. Res. Public Health 2020, 17, 8937. [Google Scholar] [CrossRef]
- Allen, T.; Reda, S.; Martin, S.; Long, P.; Franklin, A.; Bedoya, S.Z.; Wiener, L.; Wolters, P.L. The Needs of Adolescents and Young Adults with Chronic Illness: Results of a Quality Improvement Survey. Children 2022, 9, 500. [Google Scholar] [CrossRef] [PubMed]
- Mulawa, M.I.; Mtukushe, B.; Knippler, E.T.; Matiwane, M.; Al-Mujtaba, M.; Muessig, K.E.; Hoare, J.; Hightow-Weidman, L.B. Supporting Adolescents With HIV in South Africa Through an Adherence-Supporting App: Mixed Methods Beta-Testing Study. JMIR Form. Res. 2023, 7, e47575. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.M.; Lee, S.; Islam, S.M.S.; Kim, S.Y. Theories Applied to m-Health Interventions for Behavior Change in Low- and Middle-Income Countries: A Systematic Review. Telemed. e-Health 2018, 24, 727–741. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.F.; Dorrington, R.E.; Moolla, H. HIV epidemic drivers in South Africa: A model-based evaluation of factors accounting for inter-provincial differences in HIV prevalence and incidence trends. S. Afr. J. HIV Med. 2017, 18, 695. [Google Scholar] [CrossRef]

{kind=link}
| Category | Sub-Category | Total (N = 29) |
|---|---|---|
| Age (in years) | 15–19 | 17 (58.6%) |
| 20–24 | 12 (41.4%) | |
| Sex | Female | 19 (65.5%) |
| Male | 10 (34.5%) | |
| Highest level of education | Middle School Grades 8–10 | 10 (34.5%) |
| High School Grades 11–12 | 15 (51.7%) | |
| Post-School Education | 4 (13.8%) |
| Theme | Subtheme | Code |
|---|---|---|
| 1. Everyday usage of digital technology | 1.1 Integrating digital technology into daily life | Smartphone usage |
| Shared devices | ||
| Television viewing | ||
| Computer usage | ||
| Communication through technology | ||
| Using technology for education | ||
| Technology for entertainment purposes | ||
| Accessing health information through technology | ||
| 1.2 Popular digital platforms and their uses | Using Facebook | |
| Playing games | ||
| Using Google | ||
| Using Instagram | ||
| Using TikTok | ||
| Using WhatsApp | ||
| Using YouTube | ||
| 2. The role of digital technology in self-management | 2.1 Using technology for personal health management | Using a smartphone to set alarms for health reminders |
| Using a smartphone to track health metrics | ||
| 3. Factors that influence digital technology use | 3.1 Connectivity and internet access | Power outages affecting Wi-Fi connectivity |
| Availability of mobile data | ||
| Wi-Fi availability | ||
| Signal accessibility | ||
| 3.2 Privacy and digital security | Feeling secure with applications | |
| Feeling secure with the internet | ||
| 3.3 Assessing information credibility | Trust in online information | |
| 3.4 Family and peer dynamics | Emotional support from family members | |
| Family attendance at clinic appointments | ||
| Peer influence on technology use | ||
| Social media peer pressure | ||
| Clinic and medication reminders from family | ||
| Family restrictions on technology | ||
| 3.5 Digital technology literacy | Lack of knowledge of specific apps | |
| Parental lack of technology literacy |
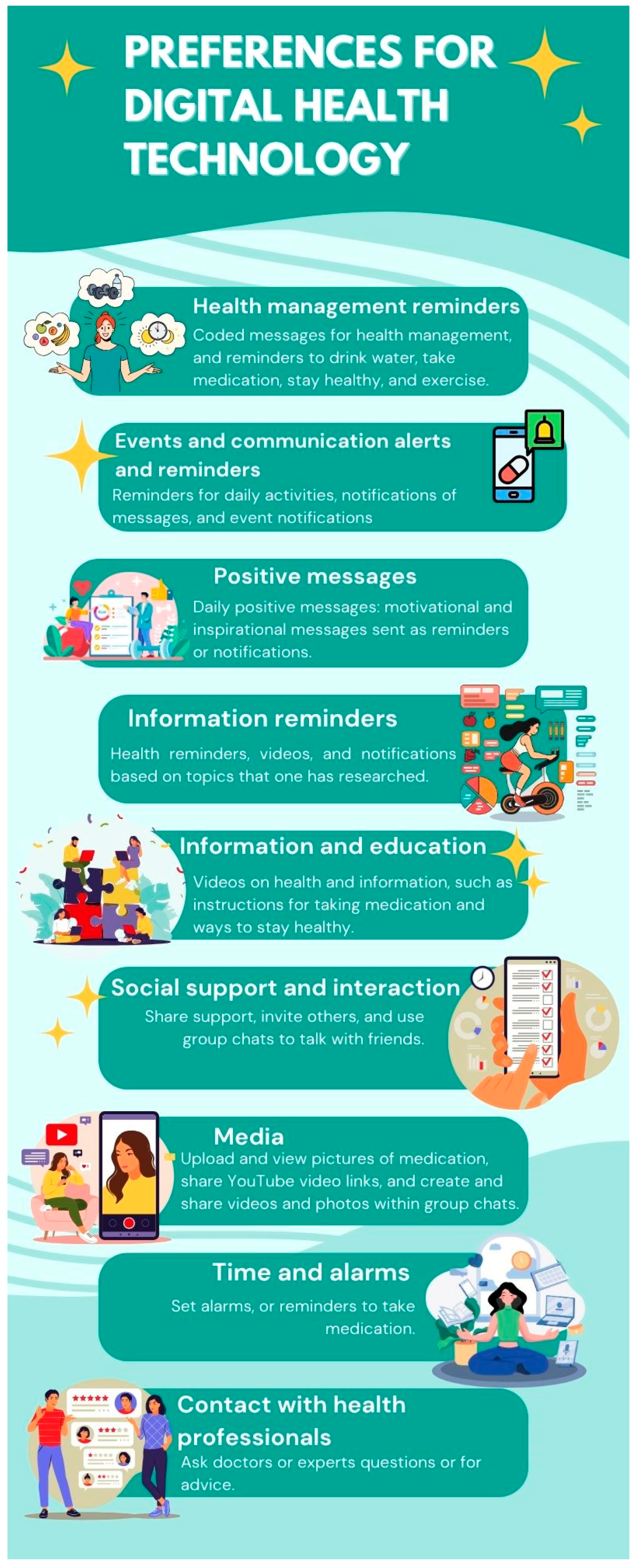
| Theme | Participant Ideas | Score (N = 29) |
|---|---|---|
| Information and education | Videos on health and information, such as instructions for taking medication and ways to stay healthy. | 13 (44.8%) |
| Health management reminders | Coded messages for health management, and reminders to drink water, take medication, stay healthy, and exercise. | 12 (41.4%) |
| Social support and interaction | Share support, invite others, and use a group chats to talk with friends. | 6 (20.7%) |
| Events and communication, alerts, and reminders | Reminders for daily activities, notifications of messages, and notifications that an event is about to start. | 5 (17.2%) |
| Positive messages | Daily positive messages: motivational and inspirational messages sent as reminders or notifications. | 4 (13.8%) |
| Media | Upload and view pictures of medication, share YouTube video links, and create and share videos and photos within group chats. | 4 (13.8%) |
| Information reminders | Reminders about what one should do or videos on health, and notifications on topics that one has researched to obtain more information. | 3 (10.3%) |
| Time and alarms | Set alarms or reminders to take medication. | 3 (10.3%) |
| Contact with health professionals | Ask doctors or experts questions or for advice. | 2 (6.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weyers, L.; Crowley, T.; Tokwe, L. Preferences of South African Adolescents Living with HIV in the Western Cape Province Regarding the Use of Digital Technology for Self-Management. Int. J. Environ. Res. Public Health 2025, 22, 972. https://doi.org/10.3390/ijerph22070972
Weyers L, Crowley T, Tokwe L. Preferences of South African Adolescents Living with HIV in the Western Cape Province Regarding the Use of Digital Technology for Self-Management. International Journal of Environmental Research and Public Health. 2025; 22(7):972. https://doi.org/10.3390/ijerph22070972
Chicago/Turabian StyleWeyers, Leonie, Talitha Crowley, and Lwandile Tokwe. 2025. "Preferences of South African Adolescents Living with HIV in the Western Cape Province Regarding the Use of Digital Technology for Self-Management" International Journal of Environmental Research and Public Health 22, no. 7: 972. https://doi.org/10.3390/ijerph22070972
APA StyleWeyers, L., Crowley, T., & Tokwe, L. (2025). Preferences of South African Adolescents Living with HIV in the Western Cape Province Regarding the Use of Digital Technology for Self-Management. International Journal of Environmental Research and Public Health, 22(7), 972. https://doi.org/10.3390/ijerph22070972