
Pet Flea and Tick Control Exposure During Pregnancy and Early Life Associated with Decreased Cognitive and Adaptive Behaviors in Children with Developmental Delay and Autism Spectrum Disorder

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Diagnostic and Outcome Measurements
2.3. Household Insecticide Exposure
2.4. Confounders
2.5. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Distribution of MSEL and VABS DQs
3.3. Distribution of Insecticide Exposure
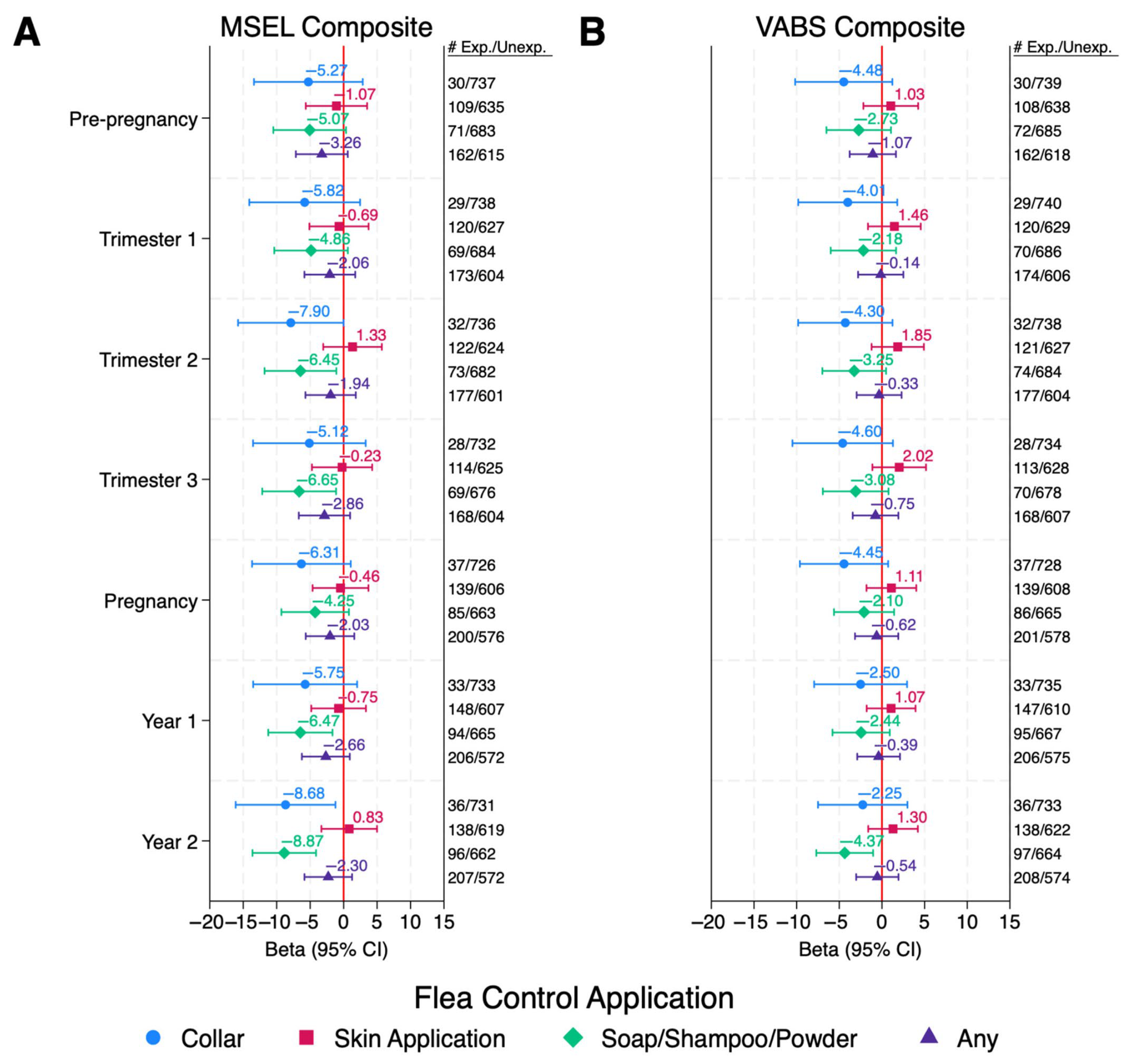
3.4. Insecticide Exposure and Neurodevelopmental Skills
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADI-R | Autism Diagnostic Interview–Revised |
| ADOS-2 | Autism Diagnostic Observation Schedules-2 |
| ASD | Autism spectrum disorder |
| CHARGE | Childhood Autism Risk from Genetics and the Environment |
| CI | Confidence interval |
| DAG | Directed Acyclic Graph |
| DD | Developmental delay without autism spectrum disorder |
| DDS | Department of Developmental Services |
| DQ | Developmental quotients |
| EPA | Environmental Protection Agency |
| FDR | False discovery rate |
| GABA | Gamma-aminobutyric acid |
| GP | General population |
| MSEL | Mullen Scales of Early Learning |
| nAChRs | Nicotinic acetylcholine receptors |
| NHW | Non-Hispanic white |
| OP | Organophosphorus |
| QFDR | Q-value after FDR correction |
| RC | Regional Centers |
| SCQ | Social Communication Questionnaire |
| SES | Socioeconomic status |
| TD | Typical development |
| VABS | Vineland Adaptive Behavior Scales |
References
- Zablotsky, B.; Black, L.I.; Maenner, M.J.; Schieve, L.A.; Danielson, M.L.; Bitsko, R.H.; Blumberg, S.J.; Kogan, M.D.; Boyle, C.A. Prevalence and trends of developmental disabilities among children in the United States: 2009–2017. Pediatrics 2019, 144, e20190811. [Google Scholar] [CrossRef]
- Gidziela, A.; Ahmadzadeh, Y.I.; Michelini, G.; Allegrini, A.G.; Agnew-Blais, J.; Lau, L.Y.; Duret, M.; Procopio, F.; Daly, E.; Ronald, A.; et al. A meta-analysis of genetic effects associated with neurodevelopmental disorders and co-occurring conditions. Nat. Hum. Behav. 2023, 7, 642–656. [Google Scholar] [CrossRef]
- Bourgeron, T. From the genetic architecture to synaptic plasticity in autism spectrum disorder. Nat. Rev. Neurosci. 2015, 16, 551–563. [Google Scholar] [CrossRef] [PubMed]
- Hallmayer, J.; Cleveland, S.; Torres, A.; Phillips, J.; Cohen, B.; Torigoe, T.; Miller, J.; Fedele, A.; Collins, J.; Smith, K.; et al. Genetic heritability and shared environmental factors among twin pairs with autism. Arch. Gen. Psychiatry 2011, 68, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Lyall, K.; Schweitzer, J.B.; Schmidt, R.J.; Hertz-Picciotto, I.; Solomon, M. Inattention and hyperactivity in association with autism spectrum disorders in the CHARGE study. Res. Autism Spectr. Disord. 2017, 35, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mazina, V.; Gerdts, J.; Trinh, S.; Ankenman, K.; Ward, T.; Dennis, M.Y.; Girirajan, S.; Eichler, E.E.; Bernier, R. Epigenetics of autism-related impairment: Copy number variation and maternal infection. J. Dev. Behav. Pediatr. 2015, 36, 61–67. [Google Scholar] [CrossRef]
- Sandin, S.; Lichtenstein, P.; Kuja-Halkola, R.; Hultman, C.; Larsson, H.; Reichenberg, A. The Heritability of Autism Spectrum Disorder. JAMA 2017, 318, 1182–1184. [Google Scholar] [CrossRef]
- Stone, D.L.; Sudakin, D.L.; Jenkins, J.J. Longitudinal trends in organophosphate incidents reported to the National Pesticide Information Center, 1995–2007. Environ. Health 2009, 8, 18. [Google Scholar] [CrossRef]
- Williams, M.K.; Rundle, A.; Holmes, D.; Reyes, M.; Hoepner, L.A.; Barr, D.B.; Camann, D.E.; Perera, F.P.; Whyatt, R.M. Changes in pest infestation levels, self-reported pesticide use, and permethrin exposure during pregnancy after the 2000–2001 US Environmental Protection Agency restriction of organophosphates. Environ. Health Perspect. 2008, 116, 1681–1688. [Google Scholar] [CrossRef]
- Saillenfait, A.-M.; Ndiaye, D.; Sabaté, J.-P. Pyrethroids: Exposure and health effects–an update. Int. J. Hyg. Environ. Health 2015, 218, 281–292. [Google Scholar] [CrossRef]
- Eskenazi, B.; Marks, A.R.; Bradman, A.; Harley, K.; Barr, D.B.; Johnson, C.; Morga, N.; Jewell, N.P. Organophosphate pesticide exposure and neurodevelopment in young Mexican-American children. Environ. Health Perspect. 2007, 115, 792–798. [Google Scholar] [CrossRef]
- Roberts, E.M.; English, P.B.; Grether, J.K.; Windham, G.C.; Somberg, L.; Wolff, C. Maternal residence near agricultural pesticide applications and autism spectrum disorders among children in the California Central Valley. Environ. Health Perspect. 2007, 115, 1482–1489. [Google Scholar] [CrossRef] [PubMed]
- Shelton, J.F.; Geraghty, E.M.; Tancredi, D.J.; Delwiche, L.D.; Schmidt, R.J.; Ritz, B.; Hansen, R.L.; Hertz-Picciotto, I. Neurodevelopmental disorders and prenatal residential proximity to agricultural pesticides: The CHARGE study. Environ. Health Perspect. 2014, 122, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Furlong, M.A.; Barr, D.B.; Wolff, M.S.; Engel, S.M. Prenatal exposure to pyrethroid pesticides and childhood behavior and executive functioning. Neurotoxicology 2017, 62, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Gunier, R.B.; Bradman, A.; Harley, K.G.; Kogut, K.; Eskenazi, B. Prenatal residential proximity to agricultural pesticide use and IQ in 7-year-old children. Environ. Health Perspect. 2017, 125, 057002. [Google Scholar] [CrossRef]
- Hicks, S.D.; Wang, M.; Fry, K.; Doraiswamy, V.; Wohlford, E.M. Neurodevelopmental delay diagnosis rates are increased in a region with aerial pesticide application. Front. Pediatr. 2017, 5, 116. [Google Scholar] [CrossRef]
- Lyall, K.; Croen, L.A.; Sjödin, A.; Yoshida, C.K.; Zerbo, O.; Kharrazi, M.; Windham, G.C. Polychlorinated biphenyl and organochlorine pesticide concentrations in maternal mid-pregnancy serum samples: Association with autism spectrum disorder and intellectual disability. Environ. Health Perspect. 2017, 125, 474–480. [Google Scholar] [CrossRef]
- Brown, A.S.; Cheslack-Postava, K.; Rantakokko, P.; Kiviranta, H.; Hinkka-Yli-Salomäki, S.; McKeague, I.W.; Surcel, H.-M.; Sourander, A. Association of maternal insecticide levels with autism in offspring from a national birth cohort. Am. J. Psychiatry 2018, 175, 1094–1101. [Google Scholar] [CrossRef]
- von Ehrenstein, O.S.; Ling, C.; Cui, X.; Cockburn, M.; Park, A.S.; Yu, F.; Wu, J.; Ritz, B. Prenatal and infant exposure to ambient pesticides and autism spectrum disorder in children: Population based case-control study. BMJ 2019, 364, l962. [Google Scholar] [CrossRef]
- Bennett, D.H.; Busgang, S.A.; Kannan, K.; Parsons, P.J.; Takazawa, M.; Palmer, C.D.; Schmidt, R.J.; Doucette, J.T.; Schweitzer, J.B.; Gennings, C.; et al. Environmental exposures to pesticides, phthalates, phenols and trace elements are associated with neurodevelopment in the CHARGE study. Environ. Int. 2022, 161, 107075. [Google Scholar] [CrossRef]
- Goodrich, A.J.; Tancredi, D.J.; Ludeña, Y.J.; Bennett, D.H.; Hertz-Picciotto, I.; Schmidt, R.J. Professionally and non-professionally applied household insecticides during pregnancy and early life and their associations with autism spectrum disorder and developmental delay in the CHARGE case-control study. Environ. Res. 2025, 267, 120651. [Google Scholar] [CrossRef]
- Domingues, V.F.; Nasuti, C.; Piangerelli, M.; Correia-Sá, L.; Ghezzo, A.; Marini, M.; Abruzzo, P.M.; Visconti, P.; Giustozzi, M.; Rossi, G.; et al. Pyrethroid pesticide metabolite in urine and microelements in hair of children affected by autism spectrum disorders: A preliminary investigation. Int. J. Environ. Res. Public Health 2016, 13, 388. [Google Scholar] [CrossRef]
- Barkoski, J.M.; Philippat, C.; Tancredi, D.; Schmidt, R.J.; Ozonoff, S.; Barr, D.B.; Elms, W.; Bennett, D.H.; Hertz-Picciotto, I. In utero pyrethroid pesticide exposure in relation to autism spectrum disorder (ASD) and other neurodevelopmental outcomes at 3 years in the MARBLES longitudinal cohort. Environ. Res. 2021, 194, 110495. [Google Scholar] [CrossRef]
- Lee, K.-S.; Lim, Y.-H.; Lee, Y.A.; Shin, C.H.; Kim, B.-N.; Hong, Y.-C.; Kim, J.I. The association of prenatal and childhood pyrethroid pesticide exposure with school-age ADHD traits. Environ. Int. 2022, 161, 107124. [Google Scholar] [CrossRef] [PubMed]
- National Pet Owners Survey. Business/Finance Fact Sheet. Available online: https://Americanpetproducts.org/Uploads/NPOS/21-22BusinessandFinance.pdf (accessed on 6 January 2024).
- Rust, M.K. Recent advancements in the control of cat fleas. Insects 2020, 11, 668. [Google Scholar] [CrossRef] [PubMed]
- Mullen, E.M. Mullen Scales of Early Learning Manual; American Guidance Service: Crowley, TX, USA, 1995. [Google Scholar]
- Sparrow, S.S.; Balla, D.A.; Cicchetti, D.V. Vineland Adaptive Behavior Scales Interview Edition Expanded Form Manual; American Guidance Service: Crowley, TX, USA, 1984. [Google Scholar]
- Hertz-Picciotto, I.; Croen, L.A.; Hansen, R.; Jones, C.R.; van de Water, J.; Pessah, I.N. The CHARGE study: An epidemiologic investigation of genetic and environmental factors contributing to autism. Environ. Health Perspect. 2006, 114, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef]
- Lord, C.R.M.; DiLavore, P.C.; Risi, S. Autism Diagnostic Observation Schedule Manual; Western Psychological Services: Los Angeles, CA, SUA, 2003. [Google Scholar]
- Lord, C.; Pickles, A.; McLennan, J.; Rutter, M.; Bregman, J.; Folstein, S.; Fombonne, E.; Leboyer, M.; Minshew, N. Diagnosing autism: Analyses of data from the Autism Diagnostic Interview. J. Autism Dev. Disord. 1997, 27, 501–517. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef]
- Rutter, M.; Le Couteur, A.; Lord, C. Autism diagnostic interview-revised. West. Psychol. Serv. 2003, 29, 30. [Google Scholar]
- Eaves, L.C.; Wingert, H.D.; Ho, H.H.; Mickelson, E.C. Screening for autism spectrum disorders with the social communication questionnaire. J. Dev. Behav. Pediatr. 2006, 27, S95–S103. [Google Scholar] [CrossRef]
- Chandler, S.; Charman, T.; Baird, G.; Simonoff, E.; Loucas, T.; Meldrum, D.; Scott, M.; Pickles, A. Validation of the social communication questionnaire in a population cohort of children with autism spectrum disorders. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 1324–1332. [Google Scholar] [CrossRef]
- Textor, J.; van der Zander, B.; Gilthorpe, M.S.; Liskiewicz, M.; Ellison, G.T. Robust causal inference using directed acyclic graphs: The R package ‘dagitty’. Int. J. Epidemiol. 2016, 45, 1887–1894. [Google Scholar] [CrossRef]
- He, X.; Tu, Y.; Song, Y.; Yang, G.; You, M. The relationship between pesticide exposure during critical neurodevelopment and autism spectrum disorder: A narrative review. Environ. Res. 2022, 203, 111902. [Google Scholar] [CrossRef] [PubMed]
- Carlisle, G.K. The social skills and attachment to dogs of children with autism spectrum disorder. J. Autism Dev. Disord. 2015, 45, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Wright, H.; Hall, S.; Hames, A.; Hardiman, J.; Mills, R.; PAWS Project Team; Mills, D. Pet dogs improve family functioning and reduce anxiety in children with autism spectrum disorder. Anthrozoös 2015, 28, 611–624. [Google Scholar] [CrossRef]
- Fields, V.L.; Soke, G.N.; Reynolds, A.; Tian, L.H.; Wiggins, L.; Maenner, M.; DiGuiseppi, C.; Kral, T.V.; Hightshoe, K.; Schieve, L.A. Pica, autism, and other disabilities. Pediatrics 2021, 147, e20200462. [Google Scholar] [CrossRef]
- Mayes, S.D.; Zickgraf, H. Atypical eating behaviors in children and adolescents with autism, ADHD, other disorders, and typical development. Res. Autism Spectr. Disord. 2019, 64, 76–83. [Google Scholar] [CrossRef]
- Miramontes Gonzalez, P.; Li, L. Evaluating the environmental persistence of liquid crystal monomers indoors and outdoors. Environ. Sci. Technol. Lett. 2023, 11, 216–222. [Google Scholar] [CrossRef]
- Shin, H.-M.; McKone, T.E.; Tulve, N.S.; Clifton, M.S.; Bennett, D.H. Indoor residence times of semivolatile organic compounds: Model estimation and field evaluation. Environ. Sci. Technol. 2013, 47, 859–867. [Google Scholar] [CrossRef]
- Bass, C.; Field, L.M. Neonicotinoids. Curr. Biol. 2018, 28, R772–R773. [Google Scholar] [CrossRef]
- Tomizawa, M.; Casida, J.E. Neonicotinoid insecticide toxicology: Mechanisms of selective action. Annu. Rev. Pharmacol. Toxicol. 2005, 45, 247–268. [Google Scholar] [CrossRef]
- Bradford, B.R.; Whidden, E.; Gervasio, E.D.; Checchi, P.M.; Raley-Susman, K.M. Neonicotinoid-containing insecticide disruption of growth, locomotion, and fertility in Caenorhabditis elegans. PLoS ONE 2020, 15, e0238637. [Google Scholar] [CrossRef]
- Kara, M.; Yumrutas, O.; Demir, C.F.; Ozdemir, H.H.; Bozgeyik, I.; Coskun, S.; Eraslan, E.; Bal, R. Insecticide imidacloprid influences cognitive functions and alters learning performance and related gene expression in a rat model. Int. J. Exp. Pathol. 2015, 96, 332–337. [Google Scholar] [CrossRef]
- Duzguner, V.; Erdogan, S. Chronic exposure to imidacloprid induces inflammation and oxidative stress in the liver & central nervous system of rats. Pestic. Biochem. Physiol. 2012, 104, 58–64. [Google Scholar] [CrossRef]
- Wei, F.; Cheng, F.; Li, H.; You, J. Imidacloprid affects human cells through mitochondrial dysfunction and oxidative stress. Sci. Total Environ. 2024, 951, 175422. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Alder, N.N.; Starkweather, A.R.; Chen, M.-H.; Matson, A.P.; Xu, W.; Balsbaugh, J.L.; Cong, X. Associations of mitochondrial function, stress, and neurodevelopmental outcomes in early life: A systematic review. Dev. Neurosci. 2022, 44, 438–454. [Google Scholar] [CrossRef] [PubMed]
- Rosa, M.E.; Oliveira, R.S.; de Faria Barbosa, R.; Hyslop, S.; Dal Belo, C.A. Recent advances on the influence of fipronil on insect behavior. Curr. Opin. Insect Sci. 2024, 101251. [Google Scholar] [CrossRef]
- Wang, X.; Martínez, M.A.; Wu, Q.; Ares, I.; Martínez-Larrañaga, M.R.; Anadón, A.; Yuan, Z. Fipronil insecticide toxicology: Oxidative stress and metabolism. Crit. Rev. Toxicol. 2016, 46, 876–899. [Google Scholar] [CrossRef]
- Suzuki, T.; Hirai, A.; Khidkhan, K.; Nimako, C.; Ichise, T.; Takeda, K.; Mizukawa, H.; Nakayama, S.M.; Nomiyama, K.; Hoshi, N. The effects of fipronil on emotional and cognitive behaviors in mammals. Pestic. Biochem. Physiol. 2021, 175, 104847. [Google Scholar] [CrossRef]
- Lu, M.; Du, J.; Zhou, P.; Chen, H.; Lu, C.; Zhang, Q. Endocrine disrupting potential of fipronil and its metabolite in reporter gene assays. Chemosphere 2015, 120, 246–251. [Google Scholar] [CrossRef]
- Ramírez, V.; Gálvez-Ontiveros, Y.; González-Domenech, P.J.; Baca, M.Á.; Rodrigo, L.; Rivas, A. Role of endocrine disrupting chemicals in children’s neurodevelopment. Environ. Res. 2022, 203, 111890. [Google Scholar] [CrossRef]
- Werler, M.M.; Pober, B.R.; Nelson, K.; Holmes, L.B. Reporting accuracy among mothers of malformed and nonmalformied infants. Am. J. Epidemiol. 1989, 129, 415–421. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| ASD (n = 810) | DD (n = 192) | TD (n = 531) | |
|---|---|---|---|
| Male Sex (%) | 677 (83.6%) | 136 (70.8%) | 432 (81.4%) |
| Child’s Race/Ethnicity A | |||
| Non-Hispanic White | 381 (47.0%) | 65 (34.2%) | 271 (51.3%) |
| Hispanic | 254 (31.4%) | 91 (47.9%) | 148 (28.0%) |
| Other | 175 (21.6%) | 34 (17.9%) | 109 (20.6%) |
| Year of Conception | 2004 (2000, 2009) | 2004 (2002, 2007) | 2004 (2002, 2007) |
| Season of Conception | |||
| Nov–Feb | 268 (33.6%) | 60 (31.7%) | 165 (31.7%) |
| Mar–Jun | 267 (33.5%) | 64 (33.9%) | 185 (35.5%) |
| Jul–Oct | 262 (32.9%) | 65 (34.4%) | 171 (32.8%) |
| Child’s Age at Assessment (months) | 47.0 (39.0, 54.0) | 47.0 (42.0, 54.0) | 44.0 (35.0, 52.0) |
| Mother’s Race/Ethnicity B | |||
| Non-Hispanic White | 451 (56.0%) | 84 (43.8%) | 340 (64.6%) |
| Hispanic | 199 (24.7%) | 74 (38.5%) | 105 (20.0%) |
| Other | 156 (19.4%) | 34 (17.7%) | 81 (15.4%) |
| Mother’s Age at Conception (yrs) C | 30.0 (26.0, 34.0) | 28.0 (24.0, 33.0) | 30.0 (26.0, 34.0) |
| ≥35 yrs (% yes) | 174 (21.8%) | 36 (19.0%) | 104 (20.0%) |
| Father’s Age at Conception (yrs) D | 32.0 (28.0, 37.0) | 31.0 (25.0, 37.0) | 32.0 (28.0, 36.0) |
| ≥35 yrs (% yes) | 271 (34.5%) | 62 (33.9%) | 179 (34.6%) |
| Maternal Pre-pregnancy BMI E | 24.5 (21.8, 29.2) | 25.2 (21.9, 29.7) | 24.2 (21.6, 28.2) |
| Underweight | 31 (3.9%) | 4 (2.1%) | 15 (2.8%) |
| Normal | 406 (50.7%) | 84 (44.9%) | 286 (54.3%) |
| Overweight | 181 (22.6%) | 56 (29.9%) | 137 (26.0%) |
| Obese | 183 (22.8%) | 43 (23.0%) | 89 (16.9%) |
| Gestational Age < 37 weeks (% yes) F | 83 (10.5%) | 32 (16.9%) | 48 (9.2%) |
| Parity G | |||
| 1 | 399 (49.4%) | 68 (35.4%) | 211 (40.0%) |
| 2 | 282 (34.9%) | 67 (34.9%) | 203 (38.4%) |
| 3+ | 126 (15.6%) | 57 (29.7%) | 114 (21.6%) |
| Gestational Diabetes (% yes) H | 78 (9.7%) | 20 (10.5%) | 30 (5.7%) |
| Had any mental health condition before or during pregnancy (% yes) I | 247 (42.7%) | 54 (33.3%) | 101 (22.3%) |
| Mother Born in US (% yes) J | 600 (74.6%) | 141 (73.4%) | 441 (83.2%) |
| Private Health Insurance K | 629 (78.8%) | 115 (60.5%) | 442 (84.5%) |
| Home Ownership (% yes) L | 512 (63.7%) | 103 (54.5%) | 396 (75.1%) |
| Financial Hardship (%yes) M | 168 (20.8%) | 54 (28.6%) | 80 (15.1%) |
| Mother’s Education | |||
| Some College | 122 (15.1%) | 64 (33.3%) | 69 (13.0%) |
| AA or Technical Degree | 325 (40.1%) | 73 (38.0%) | 177 (33.3%) |
| Bachelor’s Degree | 242 (29.9%) | 42 (21.9%) | 197 (37.1%) |
| Graduate Degree or higher | 121 (14.9%) | 13 (6.8%) | 88 (16.6%) |
| Lived in single-family home | |||
| Pre-pregnancy N | 504 (66.8%) | 119 (68.0%) | 382 (75.8%) |
| Entire Pregnancy O | 486 (63.6%) | 109 (60.6%) | 380 (73.9%) |
| Year 1 P | 505 (65.8%) | 108 (60.0%) | 396 (76.9%) |
| Year 2 Q | 529 (69.2%) | 113 (63.1%) | 412 (80.2%) |
| Child’s birth address in urban area R | 736 (92.0%) | 171 (91.0%) | 470 (89.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goodrich, A.J.; Tancredi, D.J.; Ludeña, Y.J.; Roudneva, E.; Schmidt, R.J.; Hertz-Picciotto, I.; Bennett, D.H. Pet Flea and Tick Control Exposure During Pregnancy and Early Life Associated with Decreased Cognitive and Adaptive Behaviors in Children with Developmental Delay and Autism Spectrum Disorder. Int. J. Environ. Res. Public Health 2025, 22, 1149. https://doi.org/10.3390/ijerph22071149
Goodrich AJ, Tancredi DJ, Ludeña YJ, Roudneva E, Schmidt RJ, Hertz-Picciotto I, Bennett DH. Pet Flea and Tick Control Exposure During Pregnancy and Early Life Associated with Decreased Cognitive and Adaptive Behaviors in Children with Developmental Delay and Autism Spectrum Disorder. International Journal of Environmental Research and Public Health. 2025; 22(7):1149. https://doi.org/10.3390/ijerph22071149
Chicago/Turabian StyleGoodrich, Amanda J., Daniel J. Tancredi, Yunin J. Ludeña, Ekaterina Roudneva, Rebecca J. Schmidt, Irva Hertz-Picciotto, and Deborah H. Bennett. 2025. "Pet Flea and Tick Control Exposure During Pregnancy and Early Life Associated with Decreased Cognitive and Adaptive Behaviors in Children with Developmental Delay and Autism Spectrum Disorder" International Journal of Environmental Research and Public Health 22, no. 7: 1149. https://doi.org/10.3390/ijerph22071149
APA StyleGoodrich, A. J., Tancredi, D. J., Ludeña, Y. J., Roudneva, E., Schmidt, R. J., Hertz-Picciotto, I., & Bennett, D. H. (2025). Pet Flea and Tick Control Exposure During Pregnancy and Early Life Associated with Decreased Cognitive and Adaptive Behaviors in Children with Developmental Delay and Autism Spectrum Disorder. International Journal of Environmental Research and Public Health, 22(7), 1149. https://doi.org/10.3390/ijerph22071149