
Adapting a Participatory Group Programme for Caregivers of Children with Complex Neurodisability from Low-, Middle-Income Countries to a High-Income Setting: Moving from “Baby Ubuntu” to “Encompass”

 ,
,  , , , and
, , , and 
Abstract
1. Introduction
1.1. Family-Centred Care
1.2. The Ubuntu Hub
1.3. Frugal Innovations in the UK
- What should the content of the new programme be? What should the adapted content look like?
- How should the adapted programme be delivered in the new context?
- How can the new programme best reach diverse and underserved populations in the London boroughs?
2. Methods
- The formation of an adaptation team.
- Exploring the rationale for the intervention from local perspectives.
- Exploring the intervention fit of “Baby Ubuntu” for East London, UK.
- Gathering recommendations from local caregivers and healthcare professionals on the content and delivery of the intervention and how to reach diverse populations.
- Drafting the adapted programme manual and programme theory.
2.1. Adaptation Team
2.2. Local Perspectives
2.3. Exploration of the Context–Intervention Fit
2.4. Development of the Programme Manual and Programme Theory
3. Results
3.1. Context–Intervention Fit
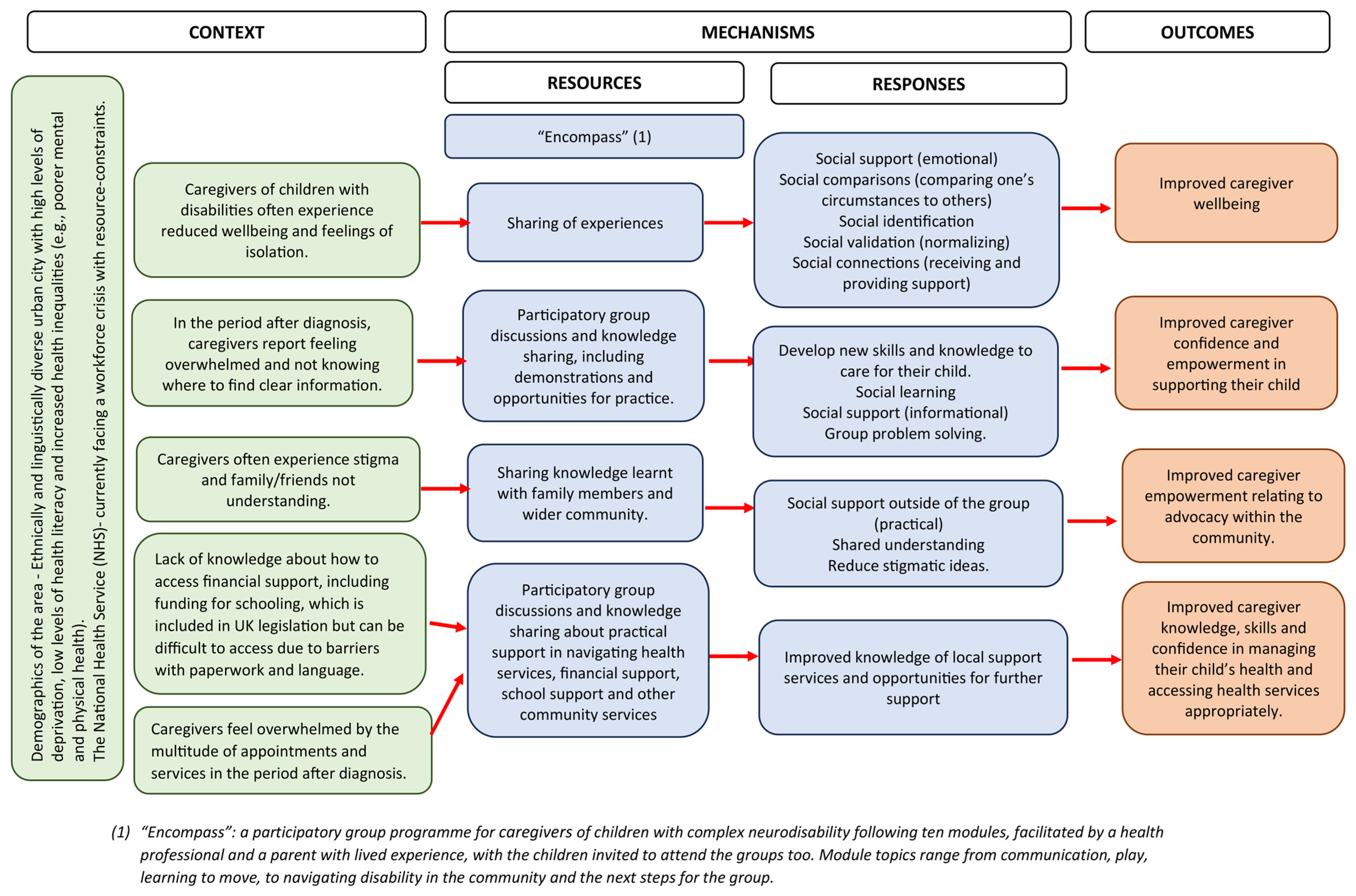
3.2. The Programme Theory
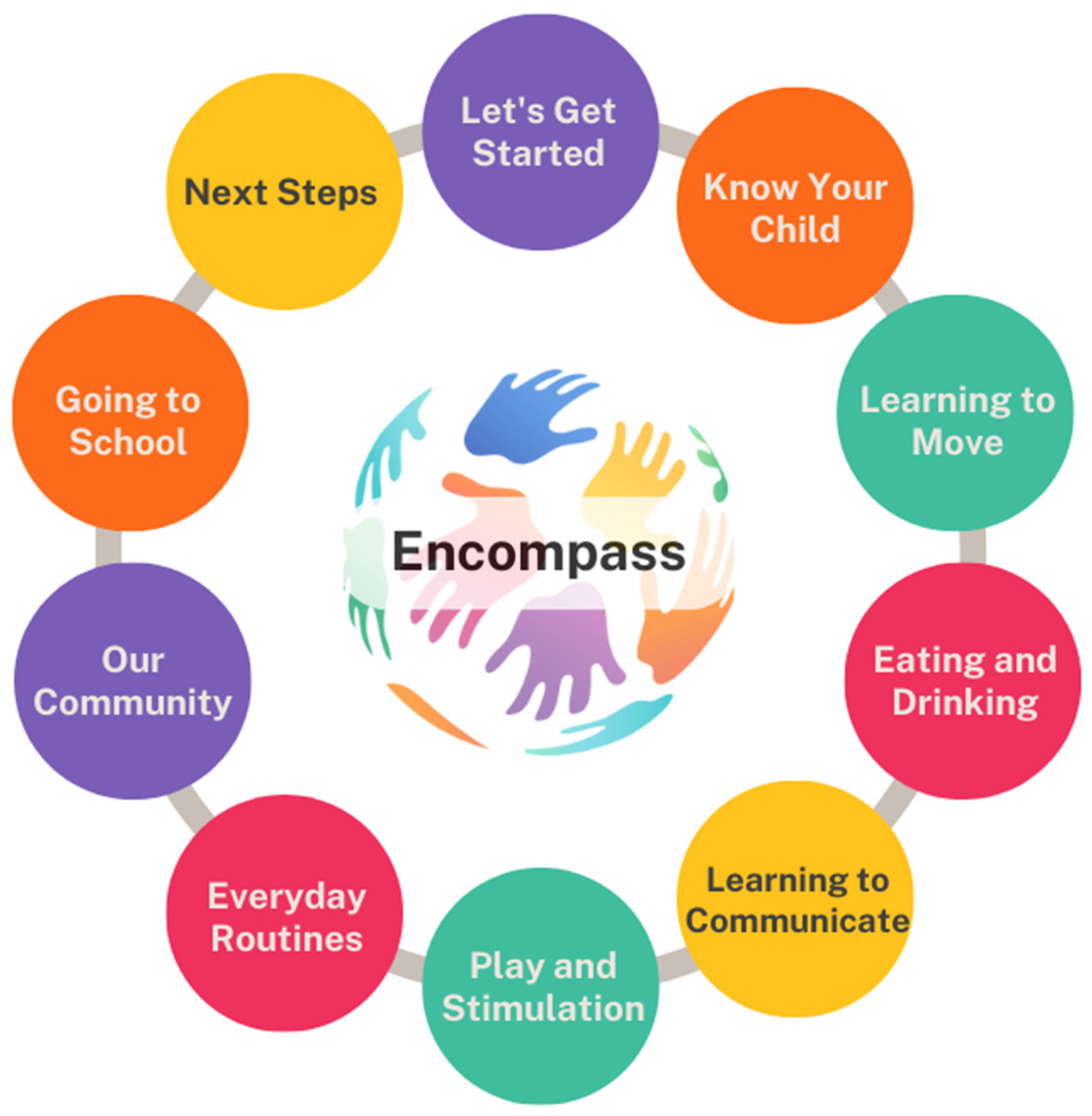
3.3. The “Encompass” Programme
3.4. Delivery Plan
3.5. Content
3.6. Reaching Diverse Populations
“But if they don’t feel comfortable [to share], you shouldn’t pressure them into saying, oh, tell us about your story or tell us your experience if you want. If they don’t then they just enjoy learning about the rest. As long as they’re comfortable.”C15
“I think some people won’t want to share their personal stories. But I guess once they meet up more and they become more comfortable with each other they may be able to start sharing.”C3
“I wouldn’t want to discuss my son with somebody whose child can’t even speak or needs to be fed. I would as a parent feel slightly awkward or uncomfortable because I don’t understand what they’re going through.”C16
“Diverse groups allow you to learn a little bit, but you can probably learn more if you have children of similar abilities.”C15
4. Discussion
4.1. Strengths and Limitations
4.2. Wider Generalisability
4.3. Implications and Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Operationalisation of the ADAPT Phases
| ADAPT Phase | Operationalisation for the Encompass Study |
| Formation of the adaptation team | The adaptation team was formed at the beginning of the project including the core research group, caregivers with lived experience, health professionals and academic researchers who were involved in the original development of the “Baby Ubuntu” programme and subsequent implementation and adaptations in LMICs, and professionals with expertise in relation to the clinical population, the development and evaluation of complex interventions, and the NHS/UK context. The adaptation team met every 6 months to explore key uncertainties, share local perspectives, develop the programme theory, and make decisions about the programme manual and delivery plan. |
| Assessing the rationale for intervention and considering intervention-context fit | We conducted a qualitative interview study to explore local perspectives about the rationale for the intervention, the intervention’s fit for the context, and local recommendations for the new programme manual and delivery plan. In this qualitative study, healthcare professionals and caregivers working with children with complex neurodisability were interviewed about their needs and priorities, which provided much of the rationale for the intervention. Participants from the qualitative study were also shown a presentation about the “Ubuntu” programme and asked general questions about the content, format, and ways to reach diverse groups. Subsequently, questions were asked about each module. The similarities and differences between the two contexts were explored in site visits by the lead researcher and in discussions with caregivers and healthcare professionals in each context. Intellectual property rights were considered throughout the process. |
| Planning for and undertaking adaptations | The manual and delivery plan were co-created through several iterative cycles. Based on feedback from the qualitative interviews and meetings with the adaptation team, the ten modules were decided upon. The parents with lived experience contributed heavily to the manual adaptation to ensure that pictures and examples were relevant to the local context. Having the initial developers of the programme on the adaptation team allowed for the core values of the programme to remain the same. The costs and resources required to test the intervention were managed by the lead researcher. Further information on the plan for evaluation, may be found in the pilot and feasibility study protocol [41]. |
| Implementing and maintaining the intervention at scale | This will be the next step after evaluating the intervention for feasibility and acceptability. A larger implementation study will be conducted with the view of exploring sustainability and cost-effectiveness. |
Appendix A.2. Examples of Specific Feedback and Adaptation Decisions
| Date | Meeting Attendee(s) | Themes/Questions | Decisions |
| January 2023 | KP and TS | Recruiting facilitators, manual, and home visits | No funding in the original grant for parent facilitators, agreed that this was a core value of the programme and funding needed to be sought for this. To apply fast-tracking learning to the manual during workshops, training and piloting. Home visits not needed for this group (already receiving therapy support for this). |
| February 2023 | Adaptation team | Population | Decided not to be too narrow with the population (i.e., not just cerebral palsy) but open up to wider complex neurodisability |
| May 2023 | Adaptation team | Online/in-person delivery How many family members to attend? Outcome measures Specific module discussions | Best for delivery to all to be in person so that group dynamics are not affected. Could consider a hybrid when the group is more established. To keep it to 1–2 family members per child. To consider measuring empowerment as opposed to children’s quality of life, which is often too distal to what the programme can achieve. Changing the name of ‘Everyday Activities’ to ‘Everyday Routines’ ‘Our Community’ module discussion of the importance of addressing stigma in the local communities ‘Going to School’ agreed on the importance of this new module |
| June 2023 | Parent partners and KP | Facilitators Module adaptations | Came up with a job description for the parent facilitator To have facilitators who understand the local contexts (should either work or live in the two boroughs where the study is taking place) Started working through modules 0–2 |
| October 2023 | KP and C.T. | Recruiting facilitators | Parent partners felt strongly that the parent facilitator should have lived experience of having a child with a complex neurodisability. We had many parents apply who had children with social communication difficulties or autism. Parent partners felt that they needed better representation and a space of their own as they often feel like they are in the back seat compared to parents of autistic children. |
| November 2023 | Adaptation team | Recruiting facilitators Venues Frequency of groups | Discussed the overrepresentation of parents of autistic children volunteering themselves to be facilitators and how others have found the same in the UK. Looking for community venues, discussed how it needs to be a neutral space that is accessible, clean and open. Decided on fortnightly groups across two school terms |
| March 2024 | Parent partners and KP | Module content | Adaptations made to modules 3–5 |
| April 2024 | KP and facilitators during training | Running of the groups Module content | It was decided that parents would benefit from text reminders (if they consented to this) the day before the groups to remind them Adaptations made to modules throughout the training |
| June 2024 | Parent partners and KP | Module content | Adaptations made for modules 6–10 |
References
- Rosenbaum, P. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child. Neurol. 2007, 49, 8–14. [Google Scholar]
- Colver, A.; Fairhurst, C.; Pharoah, P.O.D. Cerebral palsy. Lancet 2014, 383, 1240–1249. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health: Children and Youth Version: ICF-CY 2007; World Health Organization: Geneva, Switzerland, 2007; Available online: https://iris.who.int/handle/10665/43737 (accessed on 8 July 2025).
- Patel, D.R.; Neelakantan, M.; Pandher, K.; Merrick, J. Cerebral palsy in children: A clinical overview. Transl. Pediatr. 2020, 9 (Suppl. S1), S125–S135. [Google Scholar] [CrossRef] [PubMed]
- Nygård, C.; Clancy, A. Unsung heroes, flying blind-A metasynthesis of parents’ experiences of caring for children with special health-care needs at home. J. Clin. Nurs. 2018, 27, 3179–3196. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Cerebral Palsy in Under 25s: Assessment and Management (NG62); National Institute for Health and Care Excellence (NICE): London, UK, 2017; Available online: https://www.nice.org.uk/guidance/ng62/resources/cerebral-palsy-in-under-25s-assessment-and-management-pdf-1837570402501 (accessed on 8 July 2025).
- The National Confidential Enquiry into Patient Outcome and Death. Each and Every Need. [Internet]. London. 2018. Available online: https://www.ncepod.org.uk/2018report1/downloads/EachAndEveryNeed_ShortReport.pdf (accessed on 30 January 2024).
- Carter, B.; Bennett, C.V.; Jones, H.; Bethel, J.; Perra, O.; Wang, T.; Kemp, A. Healthcare use by children and young adults with cerebral palsy. Dev. Med. Child. Neurol. 2021, 63, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, D.L.; Shlobin, N.A.; Winterhalter, E.; Lam, S.K.; Raskin, J.S. Gaps in transitional care to adulthood for patients with cerebral palsy: A systematic review. Childs Nerv. Syst. 2023, 39, 3083–3101. [Google Scholar] [CrossRef] [PubMed]
- McCann, D.; Bull, R.; Winzenberg, T. The daily patterns of time use for parents of children with complex needs: A systematic review. J. Child. Health Care 2012, 16, 26–52. [Google Scholar] [CrossRef] [PubMed]
- Gokcin Eminel, A.; Kahraman, T.; Genc, A. Physical workload during caregiving activities and related factors among the caregivers of children with cerebral palsy. Ir. J. Med. Sci. 2021, 190, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Cohn, L.N.; Pechlivanoglou, P.; Lee, Y.; Mahant, S.; Orkin, J.; Marson, A.; Cohen, E. Health Outcomes of Parents of Children with Chronic Illness: A Systematic Review and Meta-Analysis. J. Pediatr. 2020, 218, 166–177.e2. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, H.; Erkin, G.; Nalbant, L. Depression and anxiety levels in mothers of children with cerebral palsy: A controlled study. Eur. J. Phys. Rehabil. Med. 2013, 49, 823–827. [Google Scholar] [PubMed]
- Hayles, E.; Harvey, D.; Plummer, D.; Jones, A. Parents’ Experiences of Health Care for Their Children With Cerebral Palsy. Qual. Health Res. 2015, 25, 1139–1154. [Google Scholar] [CrossRef] [PubMed]
- Davis, E.; Shelly, A.; Waters, E.; Boyd, R.; Cook, K.; Davern, M. The impact of caring for a child with cerebral palsy: Quality of life for mothers and fathers. Child Care Health Dev. 2010, 36, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Pevalin, D.J. Socio-economic inequalities in health and service utilization in the London Borough of Newham. Public. Health 2007, 121, 596–602. [Google Scholar] [CrossRef] [PubMed]
- London Borough of Tower Hamlets. Tower Hamlets Annual Public Health Report 2022 [Internet]. p. 2022. Available online: https://www.towerhamlets.gov.uk/Documents/Public-Health/TowerHamletsPublicHealthReport2022.pdf (accessed on 8 July 2025).
- Trust for London. Poverty and Inequality Data [Internet] 2024. Available online: https://trustforlondon.org.uk/data/boroughs/ (accessed on 28 February 2024).
- GeoData Institute. Health Literacy GeoData UK [Internet] 2019. Available online: http://healthliteracy.geodata.uk/ (accessed on 30 January 2024).
- Aston-Mansfield. Newham: Key Statistics. A Detailed Profile of Key Statistics About Newham by Aston-Mansfield’s Community Involvement Unit [Internet] 2017. Available online: https://www.aston-mansfield.org.uk/wp-content/themes/aston_mansfield/uploads/Newham_Statistics_2017.pdf (accessed on 30 January 2024).
- Kuhlthau, K.A.; Bloom, S.; Van Cleave, J.; Knapp, A.A.; Romm, D.; Klatka, K.; Homer, C.J.; Newacheck, P.W.; Perrin, J.M. Evidence for Family-Centered Care for Children With Special Health Care Needs: A Systematic Review. Acad. Pediatr. 2011, 11, 136–143.e8. [Google Scholar] [CrossRef] [PubMed]
- McConkey, R.; O’Hagan, P.; Corcoran, J. Parental Perceptions of Family-Centred Supports for Children with Developmental Disabilities. Int. J. Environ. Res. Public Health 2023, 20, 4205. [Google Scholar] [CrossRef] [PubMed]
- Kuo, D.Z.; Houtrow, A.J.; Arango, P.; Kuhlthau, K.A.; Simmons, J.M.; Neff, J.M. Family-Centered Care: Current Applications and Future Directions in Pediatric Health Care. Matern. Child. Health J. 2012, 16, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Prest, K.; Wilson, E.; Vassiliadou, I.; Ali, S.; Lakhanpaul, M.; Morris, C.; Tann, C.; Harniess, P.; Lewis-Jackson, S.; Kuper, H.; et al. ‘There was nothing, just absolute darkness’: Understanding the needs of those caring for children and young people with complex neurodisability in a diverse UK context: A qualitative exploration in the ENCOMPASS study. Child Care Health Dev. 2024, 50, e13303. [Google Scholar] [CrossRef] [PubMed]
- Heys, M.; Lakhanpaul, M.; Allaham, S.; Manikam, L.; Owugha, J.; Oulton, K.; Morris, C.; Martin, K.R.; Tann, C.; Martin, J.; et al. Community-based family and carer-support programmes for children with disabilities. Paediatr. Child. Health 2020, 30, 180–185. [Google Scholar] [CrossRef]
- Knowles, M.S.; Holton, E.F.; Swanson, R.A. The Adult Learner: The Definitive Classic in Adult Education and Human Resource Development, 6th ed.; Elsevier: Amsterdam, The Netherlands; Boston, MA, USA, 2005; 378p. [Google Scholar]
- Nanyunja, C.; Sadoo, S.; Kohli-Lynch, M.; Nalugya, R.; Nyonyintono, J.; Muhumuza, A.; Katumba, K.R.; Trautner, E.; Magnusson, B.; Kabugo, D.; et al. Early care and support for young children with developmental disabilities and their caregivers in Uganda: The Baby Ubuntu feasibility trial. Front. Pediatr. 2022, 10, 981976. [Google Scholar] [CrossRef] [PubMed]
- Zuurmond, M.; O’Banion, D.; Gladstone, M.; Carsamar, S.; Kerac, M.; Baltussen, M.; Tann, C.J.; Nyante, G.G.; Polack, S.; Martinuzzi, A. Evaluating the impact of a community-based parent training programme for children with cerebral palsy in Ghana. PLoS ONE 2018, 13, e0202096. [Google Scholar] [CrossRef] [PubMed]
- Smythe, T.; Reichenberger, V.; Pinzón, E.M.; Hurtado, I.C.; Rubiano, L.; Kuper, H. The feasibility of establishing parent support groups for children with congenital Zika syndrome and their families: A mixed-methods study. Wellcome Open Res. 2023, 6, 158. [Google Scholar] [CrossRef] [PubMed]
- Duttine, A.; Smythe, T.; Calheiros de Sa, M.R.; Ferrite, S.; Moreira, M.E.; Kuper, H. Juntos: A Support Program for Families Impacted by Congenital Zika Syndrome in Brazil. Glob. Health Sci. Pr. 2020, 8, 846–857. [Google Scholar] [CrossRef] [PubMed]
- Nalugya, R.; Nambejja, H.; Nimusiima, C.; Kawesa, E.S.; van Hove, G.; Seeley, J.; Mbazzi, F.B. Obuntu bulamu: Parental peer-to-peer support for inclusion of children with disabilities in Central Uganda. Afr. J. Disabil. 2023, 12, 948. [Google Scholar] [CrossRef] [PubMed]
- Tann, C.J.; Kohli-Lynch, M.; Nalugya, R.; Sadoo, S.; Martin, K.; Lassman, R.; Nanyunja, C.; Musoke, M.; Sewagaba, M.; Nampijja, M.; et al. Surviving and Thriving. Infants Young Child. 2021, 34, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Tann, C.; Baganizi, E. Evaluating a Programme of Early Assessment, Care and Support for Children at Risk of Developmental Disabilities and Their Caregivers in Rwanda: The PDC/Baby Ubuntu Trial [Internet]. ISRCTN; 2024 Jul Report No.: ISRCTN17523514. Available online: https://www.isrctn.com/ISRCTN17523514 (accessed on 24 May 2025).
- Bhatti, Y.A.; Prime, M.; Harris, M.; Wadge, H.; McQueen, J.; Patel, H.; Carter, A.W.; Parston, G.; Darzi, A. The search for the holy grail: Frugal innovation in healthcare from low-income or middle-income countries for reverse innovation to developed countries. BMJ Innov. 2017, 3, 212–220. [Google Scholar] [CrossRef]
- Koerich, G.V.; Cancellier, É.L.P.D.L. Frugal Innovation: Origins, evolution and future perspectives. Cad. Ebapebr. 2019, 17, 1042–1056. [Google Scholar] [CrossRef]
- Harris, M. Decolonizing Healthcare Innovation Low-Cost Solutions from Low-Income Countries, 1st ed.; Routledge: London, UK, 2023. [Google Scholar]
- Harris, M.; Marti, J.; Watt, H.; Bhatti, Y.; Macinko, J.; Darzi, A.W. Explicit Bias Toward High-Income-Country Research: A Randomized, Blinded, Crossover Experiment of English Clinicians. Health Aff. 2017, 36, 1997–2004. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Weisberger, E.; Silver, D.; Dadwal, V.; Macinko, J. That’s not how the learning works—The paradox of Reverse Innovation: A qualitative study. Glob. Health 2016, 12, 36. [Google Scholar] [CrossRef] [PubMed]
- The King’s Fund. The NHS in a Nutshell [Internet] 2024. Available online: https://www.kingsfund.org.uk/projects/nhs-in-a-nutshell (accessed on 31 January 2024).
- Harris, M.; Bhatti, Y.; Buckley, J.; Sharma, D. Fast and frugal innovations in response to the COVID-19 pandemic. Nat. Med. 2020, 26, 814–817. [Google Scholar] [CrossRef] [PubMed]
- Prest, K.; Harden, A.; Barnicot, K.; Heys, M. A coadapted community-based participatory group programme for parents/carers of children with complex neurodisability (Encompass-2): A pilot and feasibility study protocol. Pilot. Feasibility Stud. 2025, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.; Campbell, M.; Copeland, L.; Craig, P.; Movsisyan, A.; Hoddinott, P.; Littlecott, H.; O’Cathain, A.; Pfadenhauer, L.; Rehfuess, E.; et al. Adapting interventions to new contexts—The ADAPT guidance. BMJ 2021, 374, n1679. [Google Scholar] [CrossRef] [PubMed]
- Smits, D.W.; van Meeteren, K.; Klem, M.; Alsem, M.; Ketelaar, M. Designing a tool to support patient and public involvement in research projects: The Involvement Matrix. Res. Involv. Engagem. 2020, 6, 30. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, A.W.; Kragh-Sørensen, A.; Børgesen, K.; Behrens, K.E.; Andersen, T.; Kidholm, M.L.; Rothmann, M.J.; Ketelaar, M.; Janssens, A. Roles, outcomes, and enablers within research partnerships: A rapid review of the literature on patient and public involvement and engagement in health research. Res. Involv. Engagem. 2023, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- Leask, C.F.; Sandlund, M.; Skelton, D.A.; Altenburg, T.M.; Cardon, G.; Chinapaw, M.J.M.; De Bourdeaudhuij, I.; Verloigne, M.; Chastin, S.F.M.; on behalf of the GrandStand, Safe Step and Teenage Girls on the Move Research Groups. Framework, principles and recommendations for utilising participatory methodologies in the co-creation and evaluation of public health interventions. Res. Involv. Engagem. 2019, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Albayrak, I.; Biber, A.; Çalışkan, A.; Levendoglu, F. Assessment of pain, care burden, depression level, sleep quality, fatigue and quality of life in the mothers of children with cerebral palsy. J. Child. Health Care 2019, 23, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Mbatha, N.L.; Mokwena, K.E. Parental Stress in Raising a Child with Developmental Disabilities in a Rural Community in South Africa. Int. J. Environ. Res. Public Health 2023, 20, 3969. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M. Featured Article: Depressive Symptoms in Parents of Children With Chronic Health Conditions: A Meta-Analysis. J. Pediatr. Psychol. 2019, 44, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Dambi, J.M.; Jelsma, J.; Mlambo, T. Caring for a child with Cerebral Palsy: The experience of Zimbabwean mothers. Afr. J. Disabil. 2015, 4, 168. [Google Scholar] [CrossRef] [PubMed]
- Eyong, K.I.; Ekanem, E.E.; Asindi, A.A. Challenges of care givers of children with cerebral palsy in a developing country. Int. J. Contemp. Pediatr. 2017, 4, 1128–1131. [Google Scholar] [CrossRef]
- Jagosh, J. Realist Synthesis for Public Health: Building an Ontologically Deep Understanding of How Programs Work, For Whom, and In Which Contexts. Annu. Rev. Public. Health 2019, 40, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Pawson, R. The Science of Evaluation: A Realist Manifesto; SAGE: Newcastle upon Tyne, UK, 2013; 244p. [Google Scholar]
- Greenhalgh, J.; Manzano, A. Understanding ‘context’ in realist evaluation and synthesis. Int. J. Soc. Res. Methodol. 2022, 25, 583–595. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Borek, A.J.; Abraham, C.; Greaves, C.J.; Gillison, F.; Tarrant, M.; Morgan-Trimmer, S.; McCabe, R.; Smith, J.R. Identifying change processes in group-based health behaviour-change interventions: Development of the mechanisms of action in group-based interventions (MAGI) framework. Health Psychol. Rev. 2019, 13, 227–247. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Borek, A.J.; Abraham, C.; Smith, J.R.; Greaves, C.J.; Tarrant, M. A checklist to improve reporting of group-based behaviour-change interventions. BMC Public Health 2015, 15, 963. [Google Scholar] [CrossRef] [PubMed]
- Lam, P.; Stanschus, S.; Zaman, R.; Cichero, J.A.Y. The International Dysphagia Diet Standardisation Initiative (IDDSI) framework: The Kempen pilot. Br. J. Neurosci. Nurs. 2017, 13, S18–S26. [Google Scholar] [CrossRef]
- Borek, A.J.; McDonald, B.; Fredlund, M.; Bjornstad, G.; Logan, S.; Morris, C. Healthy Parent Carers programme: Development and feasibility of a novel group-based health-promotion intervention. BMC Public Health 2018, 18, 270. [Google Scholar] [CrossRef] [PubMed]
- Albert, A.; Islam, S.; Haklay, M.; McEachan, R.R.C. Nothing about us without us: A co-production strategy for communities, researchers and stakeholders to identify ways of improving health and reducing inequalities. Health Expect. 2023, 26, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Duggleby, W.; Peacock, S.; Ploeg, J.; Swindle, J.; Kaewwilai, L.; Lee, H. Qualitative Research and Its Importance in Adapting Interventions. Qual. Health Res. 2020, 30, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, J.; Paparini, S.; Papoutsi, C.; James, H.; Greenhalgh, T.; Shaw, S.E. Mobilising context as complex and dynamic in evaluations of complex health interventions. BMC Health Serv. Res. 2023, 23, 1430. [Google Scholar] [CrossRef] [PubMed]
- McCoy, D.; Kapilashrami, A.; Kumar, R.; Rhule, E.; Khosla, R. Developing an agenda for the decolonization of global health. Bull. World Health Organ. 2023, 102, 130. [Google Scholar] [CrossRef] [PubMed]
- Tuck, E.; Yang, K.W. Decolonization Is not a Metaphor. Decolon. Indig. Educ. Soc. 2012, 1, 1–40. [Google Scholar]
- Smythe, T.; Le, G.; Owen, R.; Ayana, B.; Hansen, L.; Lavy, C. The development of a training course for clubfoot treatment in Africa: Learning points for course development. BMC Med. Educ. 2018, 18, 163. [Google Scholar] [CrossRef] [PubMed]
- Smythe, T.; Owen, R.; Le, G.; Uwizeye, E.; Hansen, L.; Lavy, C. The feasibility of a training course for clubfoot treatment in Africa: A mixed methods study. PLoS ONE 2018, 13, e0203564. [Google Scholar] [CrossRef] [PubMed]
- Lavy, C. Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences [Internet]. Africa Clubfoot Training (ACT). Available online: https://www.ndorms.ox.ac.uk/research/research-groups/global-surgery/projects/africa-clubfoot-training-act (accessed on 8 July 2025).
- Bonell, C.; Prost, A.; Melendez-Torres, G.J.; Davey, C.; Hargreaves, J.R. Will it work here? A realist approach to local decisions about implementing interventions evaluated as effective elsewhere. J. Epidemiol. Community Health 2021, 75, 46–50. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Similarities | Differences |
|---|---|
|
|
| Intervention Element | Description | Comparison with “Baby Ubuntu” Groups |
|---|---|---|
| Intervention Design | (Covering Items 7 and 8 on the TIDieR Checklist) | |
| General setting | There were varied responses about whether to conduct the group sessions online or in a hybrid option; however, the decision was made to conduct the groups in-person due to the practical activities that are part of the programme and to allow social connections to form in-person during the breaks in an informal setting. Online optionality should be explored in the future, particularly as some caregivers explained that they would prefer it. “Every person is different you know. Like for me it would be better at first video”. C11 “I miss the interaction, I miss going [to a previous in-person group], I miss being in that environment. I hate this online thing being at home, I think it really becomes impersonal when you’re online.” C16 The in-person meeting will be at a local community venue in London, UK (e.g., a library or community hall). | “Baby Ubuntu” groups are always in-person in a community location |
| Venue characteristics | A large room with space for mats on the floor and chairs to create an informal circular shape for the meeting. Extra space for buggies and wheelchairs, and refreshments during the break. The room should be accessible, along with accessible toilets. | “Baby Ubuntu” groups may be held in a community centre, hospital or even outdoors at times. |
| Total number of group sessions | 10 | 11 |
| Length of group sessions | Two hours, with a break in the middle for refreshments and to allow caregivers to meet informally. | Timings vary for the groups, and they could take up a whole morning. |
| Frequency of group sessions | Every two weeks in term-time only. | This varies and could be every week, every two weeks or every month. |
| Duration of the intervention | Approximately 6 months. | The same, approximately 6 months. |
| Intervention content (Covering items 3, 4, 6, 11 on the TIDieR checklist) | ||
| Session content | The sessions cover 10 modules, each with its own topic and accompanying activities and discussion points. | The sessions cover 11 modules, each with its own topic, activities, and discussion points. |
| Sequencing of sessions | The sessions run from module 1 to 10 sequentially. The “Baby Ubuntu” team developed the sequence of modules as each session builds on the others. This allows for caregivers to practise the skills they have learnt to build their confidence as the groups progress. Caregivers have the opportunity to discuss previous modules with the facilitators if they need to miss one. | The sessions run from module 1 to 11 sequentially. |
| Participants’ materials | Participants will be provided with an A4 page handout after each session to take home with them. [Regarding handouts] “When you’re with the child, you wanna have something physically you can hold it like look through it and read it…. Sometimes you’re not going to be like oh, let me take out the laptop and look it up.” C15 | Some of the modules have handouts for caregivers to take home with them after each group. |
| Activities during the sessions | The groups predominantly follow a participatory learning approach, and although the facilitators have manuals, the activities tend to include some imparting of information, key points for discussion, examples from other settings and activities for the group to practice. “Yeah, so kind of keeping the structure that [Baby Ubuntu] have. You know how they have an ice breaker activity, then there is like a little teaching moment, and then we have the discussion and so kind of keeping the right balance is in essential.” H4 | The same. |
| Methods for checking the fidelity of delivery | A fidelity checklist has been developed, which is an adaptation of one that the “Baby Ubuntu” team have used in implementation. | The “Baby Ubuntu” team have a fidelity checklist that they use. |
| Participants | ||
| Group composition | The groups consist of caregivers of children with complex neurodisability under the age of five years. Up to two adults will be invited to attend per child. This does not necessarily need to be the parent, but someone who is involved in the everyday care of the child. Efforts will be made to encourage fathers to attend, if possible, as they tend to be left out of intervention and research activities. “My brother plays a very active role in our family setting. Although I’m close to my mom and dad, my brother is the one that used to come and help all the time with [my child].” C16 “You just predominantly find mothers attending things and that’s just because for my observations anyway, that dad actually struggle a lot more actually emotionally. Their lives aren’t ordinarily impacted as dramatically as moms’ lives are, so sometimes dads don’t feel the urgency to come to these sorts of things. They can still go to work… so I think that’s why sometimes it’s harder to reach dads. So absolutely they should both come, but that’s the problem. Dad is more likely at work.” C1 Siblings will be invited to the ‘Play and Stimulation’ sessions, and any other carers or family/community members will be invited to the ‘Our Community’ session. The reason for choosing children under 5 to attend is an attempt to capture the group of children and their caregivers who were recently diagnosed, as well as their families moving through this key transition phase. Some families may not be ready to join a group shortly after diagnosis and may need time to first adjust before committing. Others reported that the information would still be relevant 3 years post-diagnosis. [When to invite families] “The earlier you could get people the better because you just feel so alone, and you want answers.” C13 “For me, immediately after I was not quite focused on [interventions or groups]. We were still in shock for almost one year.” C2 | “Baby Ubuntu” is a programme for children with developmental disabilities under the age of 3 and their caregivers. Siblings are invited to the ‘play and stimulation’ session, and other carers, family members, and community members are invited to the ‘our community’ session. |
| Continuity of participants’ group membership | The participants who enrol in a group are expected to continue throughout the modules until the final session, unless they opt out or are unable to continue attending. | The same. |
| Group size | The groups will aim to have 10 caregivers at a time. | Groups aim to have 8–10 caregivers at a time. |
| Facilitators (Covers item 5 on the TIDieR checklist) | ||
| Number of facilitators | Two facilitators deliver the sessions together. | The same. |
| Continuity of facilitators’ group assignment | The same two facilitators who begin with a group are expected to complete all modules with the same group, unless circumstances do not allow this. | The same. |
| Facilitators’ professional background | One facilitator will be an expert parent with lived experience, and the other will be a health professional, in this case, an occupational therapist, or physiotherapist. “I think [the facilitator] needs to definitely be a trained professional, the OT, or whoever it is, but then definitely you would need like a parent/carer facilitator because they’ve just got that relatability and… they can help the professional deliver it in a way that’s going to be better received by the parents, because sometimes you know professionals are passionate about their jobs, and even though they see all of these kids every day, it’s not their life, they will go home. I think it is important to have that relatability.” C1 | The same, although the health professional may have another role besides occupational therapy or physiotherapy. They could be a community healthcare worker. |
| Facilitators’ personal characteristics | It was agreed that both facilitators should have experience in either navigating (expert parent) or delivering (health professional) healthcare in the local setting. Although there was discussion about whether the facilitators should be able to communicate in frequently spoken languages as an addition to English (e.g., Bengali), consensus was reached that this would not be essential for the role. Facilitators were expected to be able to read and communicate in English in order to deliver the contents of the manual. When recruiting facilitators, there were no preferences with regard to age, gender, ethnicity, or cultural background. In the “Baby Ubuntu” groups, the gender of the facilitators largely depended on the context, with female facilitators being observed to feel more comfortable in supporting the emotional needs of caregivers, and male facilitators having a key role in changing community perspectives. | “Baby Ubuntu” facilitators are required to have enough literacy to be able to read the manual either in English or their local language. |
| Facilitators’ training in intervention delivery | Facilitators will receive training from a master trainer in “Baby Ubuntu”, which covers both the intervention content, the delivery methods and group facilitation skills. The training manual was adapted with the support of one of the developers of the “Baby Ubuntu” and the subsequent facilitator training manual (RL). Both the parent facilitators and healthcare professional facilitators will be trained together to ensure that power is shared from the beginning. The training is practical and includes group discussions and opportunities to role-play, facilitating activities from the different modules. | The same |
| Facilitators’ training in group facilitation | See above. | The same |
| Facilitators’ materials (Item 3 on TIDieR checklist) | Facilitators will be provided with a manual, which includes module 0 that assists them in their preparation for the groups. They will also have materials such as posters and objects to assist with demonstrations and practice during the groups. | The same |
| Intended facilitation style | The “Encompass” groups, like all previous “Ubuntu” groups, are run with a participatory approach using principles from adult learning theory. The group participants’ experiences are acknowledged as being important knowledge within the group and are built upon during the sessions, along with problem-solving discussions relevant to their own situations. The facilitator imparts their knowledge within this context, but the relationship is more horizontal than vertical. | The same |
| “Encompass” Module | Overview of Module | The Same or Different to the “Baby Ubuntu” Module *? | Adaptations and Rationale |
|---|---|---|---|
| Module 0: Before you begin | Helps facilitators to plan the groups, follow the manual, top tips, common mistakes, how to refer to if there is an issue, and how to monitor and evaluate. | The same | No major changes |
| Module 1: Let us get started | About the programme, sharing information about complex neurodisability, and personal story sharing. | The same | No major changes |
| Module 2: Know your child | Explores what their child can do, and what they would like their child to progress to (setting achievable goals) without reinforcing ‘typical developmental milestones’. Exploring different healthcare services. | The same | Although the module has largely stayed the same, parent partners for the project emphasised the need not to reinforce ‘typical developmental milestones’, as this is something that they come across often in medical appointments and interacting with other children in their lives. They felt that this does not need to be reinforced, but rather children should be celebrated for what they can do, and to understand that development will happen differently for all of the children in “Encompass”. |
| Module 3: Positioning, carrying and learning to move | How to position children who need assistance, and how to assist children to learn to move. | Combined two of the “Baby Ubuntu” modules into one (module 3, positioning and carrying, and module 5, learning to move) | Caregivers as well as healthcare professionals from the qualitative study referenced in Figure 1 agreed that learning to position and carry their child with a complex neurodisability would be an essential component of the “Encompass” programme. Parts of this module would need to be adapted as caregivers may require information about specialist equipment, such as standing frames or seating, which were not as freely available in Uganda for “Baby Ubuntu”. “I just went by experience and with my son, for example, now I’m struggling because he’s getting quite tall, but it would have helped if I knew how to carry him properly when he was bit younger because I’m having a lot of back pain in general now even when I’m not carrying him and I know that’s because I was carrying him incorrectly” C16 “Often parents break their back because of wrong lifting technique and the implication is not on them alone. Even the child that they’re carrying. If they leave the child you know in the wrong position, it could affect so many things”. H3 |
| Module 4: Eating and drinking | Feeding challenges, practical skills to address these feeding challenges, exploring topics of diet, positioning for feeding, utensils, textures, and kind and sensitive feeding methods. | The same | This module was deemed to be equally relevant to caregivers in London as it was to the participants of “Baby Ubuntu” groups in Uganda. This may include supporting caregivers in knowing when to seek support and acknowledging the stress that accompanies feeding difficulties, as illustrated in the quote below: “I needed help because every time I had to feed him, we had a lot of problems and I had to keep asking doctors to help me what to do because he was very skinny and he ate a little and even if I wanted, I couldn’t give him you know nutrition. So, I think it should be like that [caregivers] can look for help if [needed].” C11 Additional advice was sought from a local specialist speech and language therapist who provided suggestions for this module, including the introduction of the International Dysphagia Diet Standardisation Initiative (IDDSI) framework [58] to help caregivers understand different textures and thicknesses if their child has swallowing difficulties. |
| Module 5: Communicating | Explores the importance of communication, how the family can support communication, e.g., engaging, taking turns, making choices, and using alternative forms of communication, and practising communication. | The same | No major changes |
| Module 6: Play and stimulation | Explores the importance of play for children to develop and learn, early stimulation, using everyday objects in play, inclusion of play in the family and broader community. Siblings were invited to this session. | The same | This module provides an opportunity for caregivers to create simple toys out of everyday objects. In Uganda, toys were made from grasses or plastic bottles during the “Baby Ubuntu” groups. A caregiver in the qualitative study in London made the association that this could still be relevant in their setting. “She showed me how to make something really simple that was really stimulating and he loved it and it was something that we just made things we had in the kitchen. C13 The addition of the word ‘stimulation’ assists caregivers to move away from the idea that play has to involve toys and things, creating a broader understanding that stimulating activities can promote play or playfulness. “And I like early stimulation. I think that’s really important because looking at it, people think of play as almost this specific thing, but it is the early stimulation that you can do leads into play” H4 |
| Module 7: Everyday Routines | How to support children in their everyday routines, for example, sleep, dressing, self-care, and managing travel. | The same (although the module title changed from ‘Everyday Activities’) | The title of ‘Everyday Activities’ was altered slightly to ‘Everyday Routines’ so that the routines of the child could be considered throughout their day and night. With the implementation of “Baby Ubuntu”, this module provided an opportunity to practise many of the skills learnt during previous modules around positioning, eating, drinking, and communicating. Additional self-care activities (e.g., dressing) were noted as important by caregivers in the qualitative study. They also brought up sleep difficulties, including pain, breathing difficulties and leg spasms, which aim to be included in the discussion points. |
| Module 8: Our Community | Identifying ‘our community’. Discussion about common barriers to inclusion and knowing the rights of people with disabilities. | Combined two of the “Baby Ubuntu” modules into one (module 9, togetherness and belonging, and module 10, our community) | Both caregivers and healthcare professionals from the qualitative study highlighted the importance of understanding local charity support in the ‘Our Community’ module. They reported that the “Encompass” groups could be valuable in signposting caregivers to different supports and that the group may be able to learn from each other. “There are various charities out there that help with fund raising for different things like kids shoes. ‘Cause I have to get two different sizes and it’s a nightmare” C13 “There’s always lots of little groups going on that people don’t know about” H4 Although signposting was considered a helpful aspect of the above module, other caregivers emphasised the importance of being proactive and empowering parents to seek out information, as local support offers tend to change. This relates to one of the anticipated outcomes of the programme theory, which is to improve caregivers’ health literacy and activation by improving their skills, confidence, and knowledge in seeking out, accessing, and interacting with various services for their own or their child’s health. |
| Module 9: Going to school | Knowing where to go to seek advice and support for schooling, understanding some of the wording used in schools, e.g., EHCPs, SEND, and sharing experiences and common concerns in sending their children to school. | New module developed for “Encompass” | This module was a new recommendation, which was not included in any previous adaptations of the programme. The additional module within the “Encompass” programme relates more to understanding the policies and systems in the UK that are in place to support the inclusion of children with disabilities within schools. “Education needs to definitely have its own thing because there are changes between nursery school and then there were changes from primary school to secondary school. And funding? One to one? Should your child go to mainstream school? Should the SENCo help you know? What is an EHCP plan? Writing it during your application that took me flipping ages.” C1 “So I sent him to a normal nursery even though we were receiving help from like OT. But the SENCo didn’t know about it till late last year and now I’ve got to move him to a special needs nursery at the end of year. Whereas if I was told from the get-go, none of that would have happened. So now I’ve got uproot him to somewhere he’s been for a year and a half.” C3 |
| Module 10: Next steps | Making plans to continue the group, finding other communities, summarising learnings, and sharing significant changes. | The same | No major changes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prest, K.; Barnicot, K.; Hurt, C.; Badenhorst, F.; Borek, A.; Whyte, M.; Harniess, P.; Jannath, A.; Lassman, R.; Morris, C.; et al. Adapting a Participatory Group Programme for Caregivers of Children with Complex Neurodisability from Low-, Middle-Income Countries to a High-Income Setting: Moving from “Baby Ubuntu” to “Encompass”. Int. J. Environ. Res. Public Health 2025, 22, 1144. https://doi.org/10.3390/ijerph22071144
Prest K, Barnicot K, Hurt C, Badenhorst F, Borek A, Whyte M, Harniess P, Jannath A, Lassman R, Morris C, et al. Adapting a Participatory Group Programme for Caregivers of Children with Complex Neurodisability from Low-, Middle-Income Countries to a High-Income Setting: Moving from “Baby Ubuntu” to “Encompass”. International Journal of Environmental Research and Public Health. 2025; 22(7):1144. https://doi.org/10.3390/ijerph22071144
Chicago/Turabian StylePrest, Kirsten, Kirsten Barnicot, Catherine Hurt, Frances Badenhorst, Aleksandra Borek, Melanie Whyte, Phillip Harniess, Alea Jannath, Rachel Lassman, Christopher Morris, and et al. 2025. "Adapting a Participatory Group Programme for Caregivers of Children with Complex Neurodisability from Low-, Middle-Income Countries to a High-Income Setting: Moving from “Baby Ubuntu” to “Encompass”" International Journal of Environmental Research and Public Health 22, no. 7: 1144. https://doi.org/10.3390/ijerph22071144
APA StylePrest, K., Barnicot, K., Hurt, C., Badenhorst, F., Borek, A., Whyte, M., Harniess, P., Jannath, A., Lassman, R., Morris, C., Osbourne, R., Smythe, T., Tann, C. J., Thomas, K., Wilson, E., Harden, A., & Heys, M. (2025). Adapting a Participatory Group Programme for Caregivers of Children with Complex Neurodisability from Low-, Middle-Income Countries to a High-Income Setting: Moving from “Baby Ubuntu” to “Encompass”. International Journal of Environmental Research and Public Health, 22(7), 1144. https://doi.org/10.3390/ijerph22071144