

Maternal Death: Retrospective Autopsy Study in Southwestern Colombia, 2000–2023
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Case Selection
2.3. Data Collection
- Sociodemographic characteristics: Age, provenance (municipality/department), type of health insurance (public, private, uninsured).
- Clinical characteristics: Number of previous pregnancies, gestational age at death, history of abortion, pre-existing pathological conditions (e.g., sickle cell anemia, systemic lupus erythematosus, nutritional disorders, hypertension), type of delivery (vaginal, cesarean, intrauterine fetal death), level of healthcare received (Level 1, 2, 3, 4), duration of hospitalization (days between admission and death).
- Autopsy findings: Macroscopic and microscopic findings relevant to the cause of death.
2.4. Determination of Cause of Death
2.5. Statistical Analysis
- Descriptive statistical analyses were performed using Stata statistical software (Version 2019, accessed on January 2025).
- Quantitative variables were assessed for normality using the Shapiro–Wilk test. Variables with a p-value > 0.05 were considered normally distributed and were summarized using means and standard deviations. Variables that did not meet the assumption of normality (p ≤ 0.05) were presented using medians and interquartile ranges.
- Qualitative variables were described using frequencies and percentages.
- Comparisons between categorical variables were performed using the Chi-square test.
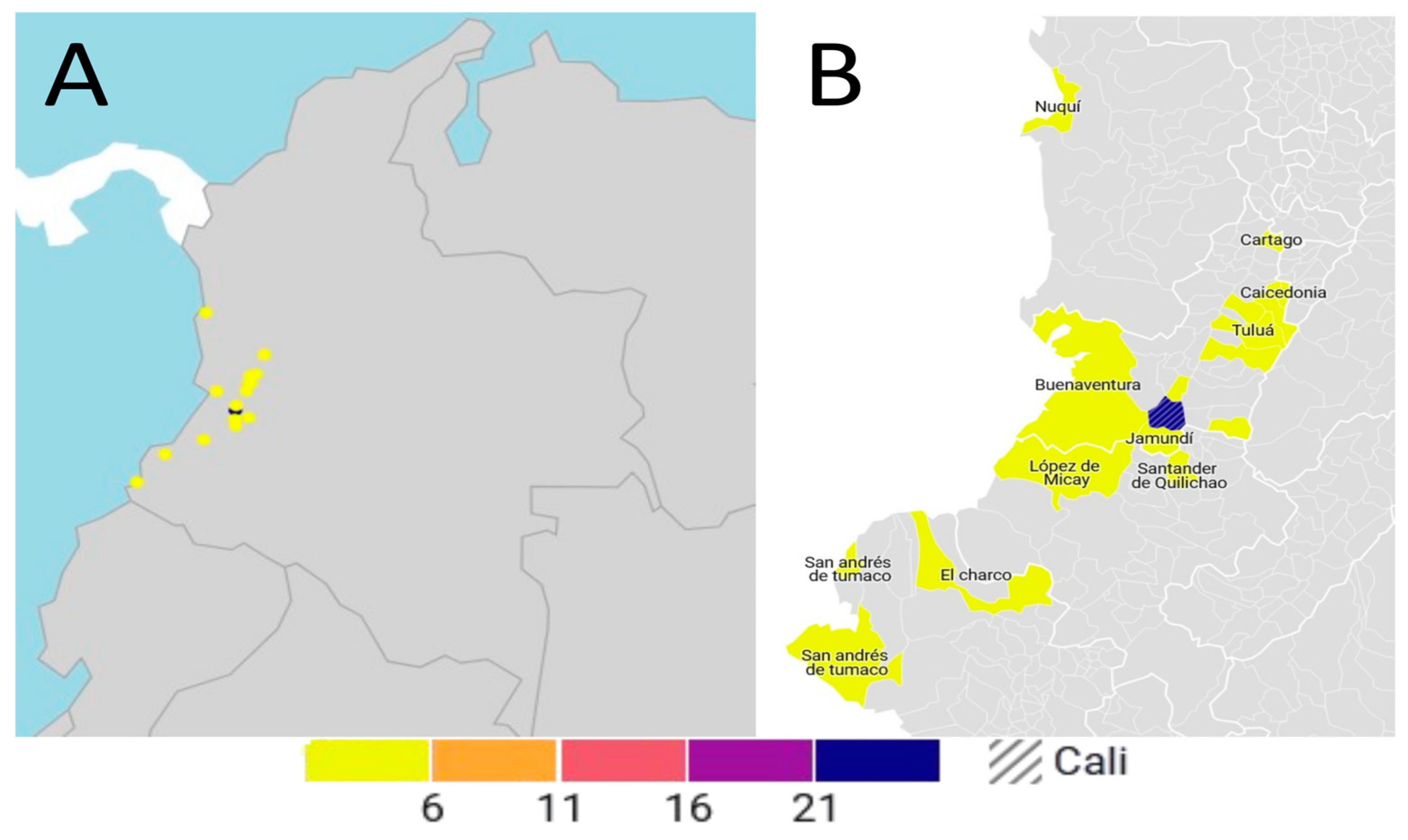
- The geographical distribution of cases by provenance was visualized using a map. A choropleth map was created using the online tool Datawrapper (https://www.datawrapper.de/). The platform was accessed on 20 April 2025.
2.6. Ethical Considerations
3. Results
3.1. Overview of Autopsied Cases
3.2. Sociodemographic and Clinical Characteristics
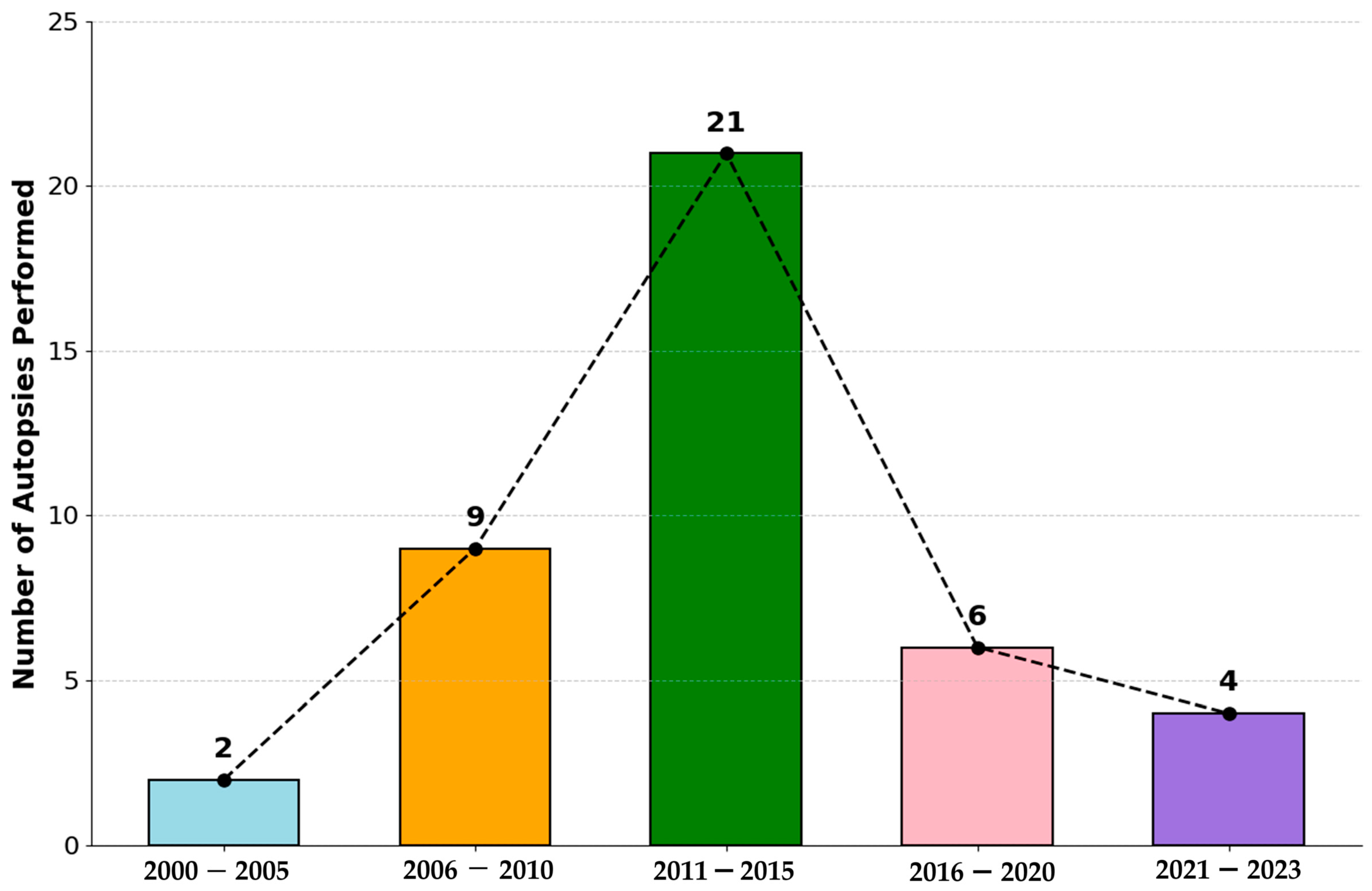
3.3. Temporal Trend of Maternal Mortality
3.4. Causes of Maternal Mortality
3.4.1. Indirect Causes of Death
3.4.2. Direct Causes of Death
3.5. Geographical Distribution
4. Discussion
4.1. Main Findings
4.2. Trend Analysis and National Context
4.3. Comparative Analysis of the Causes of Maternal Death
4.4. Comparative Analysis of Sociodemographic and Clinical Profiles
4.5. Significance of Pathological Findings
4.6. Study Limitations
4.7. Future Recommendations
- Diagnostic Validation: Conduct prospective multicenter studies in Colombia that systematically compare clinical diagnoses of the cause of maternal mortality with autopsy findings to quantify concordance, identify the most frequent discrepancies, and evaluate the real added value of autopsy in epidemiological surveillance.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MM | Maternal Mortality |
| MMR | Maternal Mortality Ratio |
| LB | Live Births |
| WHO | World Health Organization |
| SLE | Systemic Lupus Erythematosus |
| HTN | Hypertension |
| N | Number of Cases |
| SLE | Systemic Lupus Erythematosus |
| PPH | Postpartum Hemorrhage |
| HDP | Hypertensive Disorders in Pregnancy |
| SCA | Sickle Cell Anemia |
| ANC | Antenatal Care |
| SMM | Severe Maternal Morbidity |
| PMR | Proportional Mortality Ratio |
| DANE | National Administrative Department of Statistics |
| SIVIGILA | National Public Health Surveillance System |
References
- García-Tizón Larroca, S.; Amor Valera, F.; Ayuso Herrera, E.; Cueto Hernandez, I.; Cuñarro Lopez, Y.; De Leon-Luis, J. Human Development Index of the Maternal Country of Origin and Its Relationship with Maternal near Miss: A Systematic Review of the Literature. BMC Pregnancy Childbirth 2020, 20, 224. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, E.R.; Klein, T.J.; Beyuo, T.K. Maternal Mortality in Low and Middle-Income Countries. Obstet. Gynecol. Clin. N. Am. 2022, 49, 713–733. [Google Scholar] [CrossRef] [PubMed]
- Kurjak, A.; Stanojević, M.; Dudenhausen, J. Why Maternal Mortality in the World Remains Tragedy in Low-Income Countries and Shame for High-Income Ones: Will Sustainable Development Goals (SDG) Help? J. Perinat. Med. 2023, 51, 170–181. [Google Scholar] [CrossRef]
- Birabwa, C.; Banke-Thomas, A.; Waiswa, P.; Semaan, A.; Kananura, R.M.; Van Olmen, J.; Beňová, L. Maternal Health in Cities: Analysis of Institutional Maternal Mortality and Health System Bottlenecks in Kampala City Uganda, 2016–2021. J. Glob. Health Rep. 2024, 8, e2024006. [Google Scholar] [CrossRef]
- Castañeda-Orjuela, C.; Hilarion Gaitan, L.; Diaz-Jimenez, D.; Cotes-Cantillo, K.; Garfield, R. Maternal Mortality in Colombia during the COVID-19 Pandemic: Time Series and Social Inequities. BMJ Open 2023, 13, e064960. [Google Scholar] [CrossRef] [PubMed]
- Escobar, M.F.; Echavarria, M.P.; Gallego, J.C.; Riascos, N.; Vasquez, H.; Nasner, D.; Pabon, S.; Castro, Z.A.; Cardona, D.A.; Castro, A.M.; et al. Effect of a Model Based on Education and Teleassistance for the Management of Obstetric Emergencies in 10 Rural Populations from Colombia. Digit. Health 2022, 8, 205520762211290. [Google Scholar] [CrossRef]
- Ramos Jaraba, S.M.; Quiceno Toro, N.; Ochoa Sierra, M.; Ruiz Sánchez, L.; García Jiménez, M.A.; Salazar-Barrientos, M.Y.; Bedoya Bedoya, E.; Vélez Álvarez, G.A.; Langer, A.; Gausman, J.; et al. Health in Conflict and Post-Conflict Settings: Reproductive, Maternal and Child Health in Colombia. Confl. Health 2020, 14, 33. [Google Scholar] [CrossRef]
- Alipour, J.; Payandeh, A.; Karimi, A. Prevalence of Maternal Mortality Causes Based on ICD-MM: A Systematic Review and Meta-Analysis. BMC Pregnancy Childbirth 2023, 23, 821. [Google Scholar] [CrossRef]
- Shiferaw, M.A.; Bekele, D.; Surur, F.; Dereje, B.; Tolu, L.B. Maternal Death Review at a Tertiary Hospital in Ethiopia. Ethiop. J. Health Sci. 2021, 31, 35–42. [Google Scholar] [CrossRef]
- Namagembe, I.; Kiwanuka, N.; Byamugisha, J.K.; Ononge, S.; Beyeza-Kashesya, J.; Kaye, D.K.; Moffett, A.; Aiken, C.E.; Nakimuli, A. Why Mothers Die at a Busy Tertiary Urban Hospital in Kampala, Uganda: A Comprehensive Review of Maternal Deaths 2016-2018 and Implications for Quality Improvement to Reduce Deaths. Afr. Health Sci. 2022, 22, 489–499. [Google Scholar] [CrossRef]
- Samuel, O.; Zewotir, T.; North, D. Decomposing the Urban–Rural Inequalities in the Utilisation of Maternal Health Care Services: Evidence from 27 Selected Countries in Sub-Saharan Africa. Reprod. Health 2021, 18, 216. [Google Scholar] [CrossRef] [PubMed]
- Ávila Mellizo, G.A.; Rubiano, H. Protocolo de Vigilancia en Salud Pública. Mortalidad Materna; Instituto Nacional de Salud—Dirección de Vigilancia y Análisis del Riesgo en Salud Pública: Colombia, 2024. Available online: https://www.ins.gov.co/buscador-eventos/Lineamientos/Pro_mortalidad%20materna%202024.pdf (accessed on 3 May 2025).
- Ruíz, L.A.V.; Sandoval-Martínez, D.K.; Mantilla-Hernández, J. C Estudio de las biopsias de muertes maternas en un hospital universitario de alta complejidad en Santander, Colombia. Rev. Cubana Obstet. Ginecol. 2019, 45. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0138-600X2019000200005&lng=es (accessed on 3 May 2025).
- ICD-10 Version: 2010. Available online: https://icd.who.int/browse10/2010/en (accessed on 3 May 2025).
- Mellizo, G.A.Á. Informe de Mortalidad Materna, Colombia, 2022; Instituto Nacional de Salud: Colombia, 2022. Available online: https://www.ins.gov.co/buscador-eventos/Informesdeevento/MORTALIDAD%20MATERNA%20INFORME%202022.pdf (accessed on 3 May 2025).
- Almeida, L.M.; Caldas, J.; Ayres-de-Campos, D.; Salcedo-Barrientos, D.; Dias, S. Maternal Healthcare in Migrants: A Systematic Review. Matern. Child Health J. 2013, 17, 1346–1354. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez Hernández, J.M.; Ariza Ruiz, L.K.; Castro Barbudo, D.; Vivas Sánchez, P.; Matallana Gómez, M.A.; Gómez Hernández, L.J.; Romero Mendoza, L.; Chaparro Narváez, P.E. Analysis of Inequalities and Inequities in Maternal Mortality in Chocó, Colombia. Int. J. Environ. Res. Public Health 2023, 20, 6095. [Google Scholar] [CrossRef]
- Vélez-Maya, M.A.; Grillo-Ardila, C.F.; Higuera-R, I.L.; Molano, D. Caracterización de La Mortalidad Materna Temprana En Bogotá. Estudio de Vigilancia Epidemiológica de Casos Centinela. Ginecol. Obstet. Mex. 2019, 87, 425–435. [Google Scholar]
- Cárdenas-Cardenas, L.M.; Cotes-Cantillo, K.; Chaparro-Narváez, P.E.; Fernández-Niño, J.A.; Paternina-Caicedo, A.; Castañeda-Orjuela, C.; De La Hoz-Restrepo, F. Maternal Mortality in Colombia in 2011: A Two Level Ecological Study. PLoS ONE 2015, 10, e0118944. [Google Scholar] [CrossRef] [PubMed]
- Mosquera Córdoba, M.; Cuesta Caicedo, A.P. Factores biosociales asociados a la mortalidad materna en el departamento de Chocó 2013–2019. Rev. Médica Risaralda 2022, 28, 33–45. [Google Scholar] [CrossRef]
- Bello-Muñoz, C.; Rojas Suarez, J.; Torres Villa, W.; Guardo Roa, M.; Álvarez Castillo, A.; López Camacho, W. Caracterización de la Mortalidad Materna en Bolívar: Estudio de Tres Años. Rev. Cienc. Biomédicas 2013, 4, 247–255. Available online: https://revistas.unicartagena.edu.co/index.php/cbiomedicas/article/view/2816 (accessed on 3 May 2025).
- Vélez Cuervo, S.M.; Rendon Zapata, J.; Caicedo Bolanos, A. Descripción de Los Factores Contribuyentes a Las Muertes Secundarias a Trastornos Hipertensivos Asociados al Embarazo En Antioquia, Colombia (2012–2020). Ginecol. Obstet. Mex. 2024, 92, 127–136. [Google Scholar] [CrossRef]
- Alvarez-Sierra, S.P. Demoras en mortalidad materna en el departamento de Santander 2012 a 2015. Rev. Salud Pública 2018, 20, 699–706. [Google Scholar] [CrossRef]
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.-B.; Daniels, J.; Gülmezoglu, A.M.; Temmerman, M.; Alkema, L. Global Causes of Maternal Death: A WHO Systematic Analysis. Lancet Glob. Health 2014, 2, e323–e333. [Google Scholar] [CrossRef] [PubMed]
- García Bedoya, A. Mortalidad Materna (Período Epidemiológico VI); Instituto Nacional de Salud: Colombia, 2024. Available online: https://www.ins.gov.co/buscador-eventos/Informesdeevento/MORTALIDAD%20MATERNA%20PE%20VI%202024.pdf (accessed on 3 May 2025).
- Joubert, D.; Rossouw, S.; Solomon, C.; Meyer, P. Discrepancies between Clinical Diagnoses and Autopsy Findings: A Comparative Study Conducted in South Africa. S. Afr. Med. J. 2022, 879–882. [Google Scholar] [CrossRef] [PubMed]
- Roulson, J.; Benbow, E.W.; Hasleton, P.S. Discrepancies Between Clinical and Autopsy Diagnosis and the Value of Post Mortem Histology; A Meta-Analysis and Review. Histopathology 2005, 47, 551–559. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Clinical and Sociodemographic Characteristics | Descriptor | Measure/Summary | |
|---|---|---|---|
| N () | % | ||
| Age (years) | 15–20 | 10 | 23.8 |
| 21–25 | 7 | 16.7 | |
| 26–30 | 11 | 26.2 | |
| 31–35 | 9 | 21.4 | |
| 36–40 | 5 | 11.9 | |
| Insurance Type | Private | 6 | 14.3 |
| Public | 26 | 61.6 | |
| Uninsured | 1 | 4.1 | |
| No data | 9 | 20 | |
| Number of Pregnancies | 1 | 16 | 38.1 |
| 2–4 | 19 | 5.2 | |
| 5–10 | 5 | 11.9 | |
| More than 10 | 2 | 4.8 | |
| Gestational Weeks | 6–12 | 4 | 9.5 |
| 13–19 | 4 | 9.5 | |
| 20–27 | 10 | 23.8 | |
| 28–36 | 17 | 40.5 | |
| 37–43 | 7 | 16.7 | |
| History of Abortion | Yes | 12 | 28.6 |
| No | 30 | 71.4 | |
| Medical History | Sickle cell anemia | 3 | 7.1 |
| Cirrhosis/atresia | 1 | 2.4 | |
| Malnutrition | 2 | 4.8 | |
| SLE (Systemic Lupus Eryth.) | 3 | 7.1 | |
| HTN (Hypertension) | 3 | 7.1 | |
| Obesity | 1 | 2.4 | |
| Nil of relevance | 29 | 69 | |
| Type of Delivery | Vaginal | 14 | 33.3 |
| Cesarean section | 22 | 52.4 | |
| Not specified | 6 | 14.3 | |
| Level of Care | 1 | 3 | 7.1 |
| 2 | 3 | 7.1 | |
| 3 | 29 | 69 | |
| 4 | 7 | 16.7 | |
| Days between Admission and Death (Mean) | Direct death | 4.2 | |
| Indirect death | 16.5 | ||
| Type of Mortality | Early | 36 | 85.7 |
| Late | 6 | 14.3 | |
| Cause | n |
|---|---|
| Cardiogenic shock | |
| Hypertrophic cardiomyopathy secondary to mitral and aortic stenosis due to rheumatic fever | 1 |
| Severe mitral valve stenosis with left ventricular dilation | 1 |
| Distributive shock | |
| Bilateral basal pulmonary hemorrhage | 1 |
| Toxic hepatopathy | 1 |
| Sickle cell crisis | 1 |
| Metastatic dysgerminoma | 1 |
| Hypovolemic and septic shock | |
| Upper gastrointestinal bleeding, abdominal sepsis due to Escherichia coli | 2 |
| Autoimmune hemolytic anemia | 1 |
| Neurogenic shock | |
| Extensive ischemic cerebrovascular disease | 1 |
| Septic shock | |
| Sepsis—Bacteremia | 4 |
| Massive strongyloidiasis | 2 |
| Viral meningoencephalitis | 1 |
| Bacterial multilobar pneumonia | 4 |
| Cytomegalovirus pneumonia | 1 |
| Miliary tuberculosis | 1 |
| Pulmonary tuberculosis | 1 |
| Cause | n |
|---|---|
| Cardiogenic/Distributive shock | |
| Amniotic fluid embolism | 1 |
| Hypovolemic shock | |
| Uterine hemorrhage | 4 |
| Hypertensive disorders associated with pregnancy | 4 |
| Neurogenic shock | |
| Fulminant hepatic failure secondary to acute fatty liver of pregnancy | 1 |
| Intracerebral hemorrhage due to arteriovenous malformation | 1 |
| Neurogenic and distributive shock | |
| Eclampsia with hemorrhagic stroke | 1 |
| Obstructive shock | |
| Pulmonary thromboembolism | 3 |
| Septic shock | |
| Acute panmetritis and salpingitis | 1 |
| Sepsis due to Acinetobacter baumannii secondary to septic abortion | 1 |
| Reference/ID | Location(s) | Study Period | Design/Type | Key Population/Sample | Reported MMR (Per 100 k LB) | Main Causes | Key Sociodemographic/Risk Factors |
|---|---|---|---|---|---|---|---|
| Current Study | Cali | 2000–2023 | Descriptive, observational, retrospective | 42 autopsied maternal deaths | Not applicable (case-based, not population-based) | Indirect (57.1%) > Direct (42.9%). Main indirect: Septic shock (65.2%). Main direct: Hypovolemic shock due to postpartum hemorrhage (50%). | Public/Uninsured (65.7%). Age 26–30 (26.2%). From Cauca, Buenaventura, Nariño, Chocó (20% with migration history to Cali). Sickle cell anemia, SLE, nutritional disorders noted; 85.7% early deaths. Most received Level-3 or -4 care. |
| (Álvarez-Sierra, S.P., 2018) [23] | Santander | 2012–2015 | Descriptive, retrospective, cross-sectional | 49 maternal deaths | Not specified in text | Hypertensive disorders, hemorrhagic complications, non-obstetric sepsis, obstetric sepsis, respiratory infections (per 2010–2012 data). | Mostly subsidized regime (57.1%), aged 22–35 (57.1%), mostly postpartum deaths (84%). |
| (Cárdenas-Cárdenas et al., 2015) [19] | Colombia (Municipal & Departmental) | 2011 | Ecological, analytical (two-level) | 1094 municipalities (97.5% coverage) | 69.3 (national) | Not detailed (focus on socioeconomic association). | Multidimensional poverty (municipal/departmental), low insurance (marginal), transparency index (departmental). Higher MMR in poorer departments. |
| (Ruíz et al., 2019) [13] | Santander (University Hospital) | 2005–2018 | Retrospective autopsy series | 31 maternal deaths with autopsy | Not applicable | Indirect (67.8%) > Direct (32.2%). Infectious main among indirect (14 cases). Dengue most frequent (5 cases). | Average age 26.7, basic education, 67.8% died from indirect causes, 45.2% from infection. |
| (Bello-Muñoz et al., 2013) [21] | Bolívar | 2010–2012 | Descriptive retrospective (vital stats, SIVIGILA) | 46 maternal deaths | 46.6 | Direct (62.7%) > Indirect (37.3%). Obstetric hemorrhage leading (MMR 11.1). Infections (MMR 9.12). Preeclampsia complications (MMR 8.1). | Mean age 28.1; 84.7% subsidized regime. Delay types I (73.9%) and IV (82.6%) common; 89.1% preventable deaths. Majority postpartum (58.6%). |
| (Vélez-Maya et al., 2019) [18] | Bogotá | 2010–2012 and 2013–2015 | Observational, retrospective, cross-sectional, analytical (sentinel cases) | 225 early maternal deaths and 630,017 LB | 39 (2010–2012) → 32 (2013–2015) | Direct (49.8%) > Indirect. Leading direct: Hypertensive disorders (16.8%), hemorrhage (13%), other obstetric complications (11%). Rise in infections and suicides (self-inflicted injuries). | Mostly postpartum. Age 25–29 highest proportion. Low education (basic), cohabiting; 96.4% not from special ethnic group. Subsidized and uninsured had higher mortality. |
| (Rodríguez Hernández et al., 2023) [17] | Chocó | 2010–2018 | Mixed (Ecological Analytical & Phenomenological) | 131 deceased women, 58,352 LB | 224 | Causes not detailed; focus on system deficiencies and barriers. | Strong association with Multidimensional Poverty Index (MPI). Weak health infrastructure, geographical barriers, conflict, ethnicity, poverty. Role of traditional midwifery. |
| (Castañeda-Orjuela et al., 2023) [5] | Colombia (Municipal) | 2019–2020 | Time series, ecological | 6342 deaths (2008–2020); subsample: 1055 (2019–2020) | 80 (2019), 87 (2020) | Causes not detailed; focus on COVID-19 excess mortality and inequality. | Higher mortality in lowest socioeconomic-quintile municipalities (almost 3× higher). Inequality worsened in 2020. Barriers to essential service access. |
| (Mellizo, 2022) [15] | Colombia (National) | 2022 | Surveillance data analysis (SIVIGILA) | 472 maternal deaths of residents | 42.9 (Early maternal mortality) | Direct (60.9%) > Indirect (38.3%). Main direct: Hypertensive disorders (23.8%), hemorrhage (19.5%), pregnancy-related sepsis (7.7%). Main indirect: Other causes (13.4%). | Higher risk: >40 yrs (MMR 119.8). Subsidized (RR 1.90), Uninsured (RR 1.57). Indigenous (RR 4.93), Afro-Colombian (RR 3.34). Rural-dispersed (Ratio 72.0). |
| (Mosquera Córdoba & Cuesta Caicedo, 2022) [20] | Chocó | 2013–2019 | Descriptive retrospective (SIVIGILA forms) | 96 reported maternal deaths | Increased from 108.8 (2009) to 152.2 (2019); peak 317.41 (2017) | Main cause: Hypertensive pregnancy disorders. 94% (68) direct obstetric causes vs. 6% (4) indirect. | Age groups 30–34 (17) and 20–24 (14) contributed most. 90% in SGSSS, 10% uninsured; 94% homemakers. Poor prenatal care by doctors (72.2%). Affected: Afro and Indigenous, rural. |
| (Vélez Cuervo et al., 2024) [22] | Antioquia | 2012–2020 | Descriptive retrospective | 38 deaths from hypertensive pregnancy disorders | Not applicable (focused on hypertensive disorders) | THAE (eclampsia, HELLP, intracerebral hemorrhage, premature placental abruption). | Suboptimal care in 37/38 cases. Delayed detection, poor treatment (Mg sulfate, antihypertensives), lack of resources, administrative issues. |
| INS/SDS Bulletin 2024 [12] | Colombia (National) | 2024 (PE VI preview) | Surveillance data analysis (SIVIGILA) | 90 reported cases (PE VI 2024 preview) | 45.0 (PE VI 2024 preview) | Direct (58%) > Indirect (33.3%) (Grouped causes). Main direct: Obstetric hemorrhage (12.2%), hypertensive disorders (18.9%). | Highest MMR in: Indigenous ethnicity (214.4), Small town residence (94.2), Uninsured (58.9), Age 10–14 (69.3) and >40 (138.0). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cruz-Barbosa, J.S.; Valencia-Cardona, A.F.; Cortés-Buelvas, A.D.; Liscano, Y. Maternal Death: Retrospective Autopsy Study in Southwestern Colombia, 2000–2023. Int. J. Environ. Res. Public Health 2025, 22, 1105. https://doi.org/10.3390/ijerph22071105
Cruz-Barbosa JS, Valencia-Cardona AF, Cortés-Buelvas AD, Liscano Y. Maternal Death: Retrospective Autopsy Study in Southwestern Colombia, 2000–2023. International Journal of Environmental Research and Public Health. 2025; 22(7):1105. https://doi.org/10.3390/ijerph22071105
Chicago/Turabian StyleCruz-Barbosa, Jhoan Sebastian, Andrés Felipe Valencia-Cardona, Armando Daniel Cortés-Buelvas, and Yamil Liscano. 2025. "Maternal Death: Retrospective Autopsy Study in Southwestern Colombia, 2000–2023" International Journal of Environmental Research and Public Health 22, no. 7: 1105. https://doi.org/10.3390/ijerph22071105
APA StyleCruz-Barbosa, J. S., Valencia-Cardona, A. F., Cortés-Buelvas, A. D., & Liscano, Y. (2025). Maternal Death: Retrospective Autopsy Study in Southwestern Colombia, 2000–2023. International Journal of Environmental Research and Public Health, 22(7), 1105. https://doi.org/10.3390/ijerph22071105