
Crossing Borders: SRH Challenges Among Immigrant and Minority Adolescents

 , , ,
, , ,  and
and 
{kind=link}
Abstract
1. Introduction
- Key challenges to SRH access, including cultural and systemic challenges;
- Recent advances in community-based, school-based, and digital health interventions;
- Policy and advocacy efforts shaping adolescent SRH outcomes;
- Gaps in research and future directions for improving services and access.
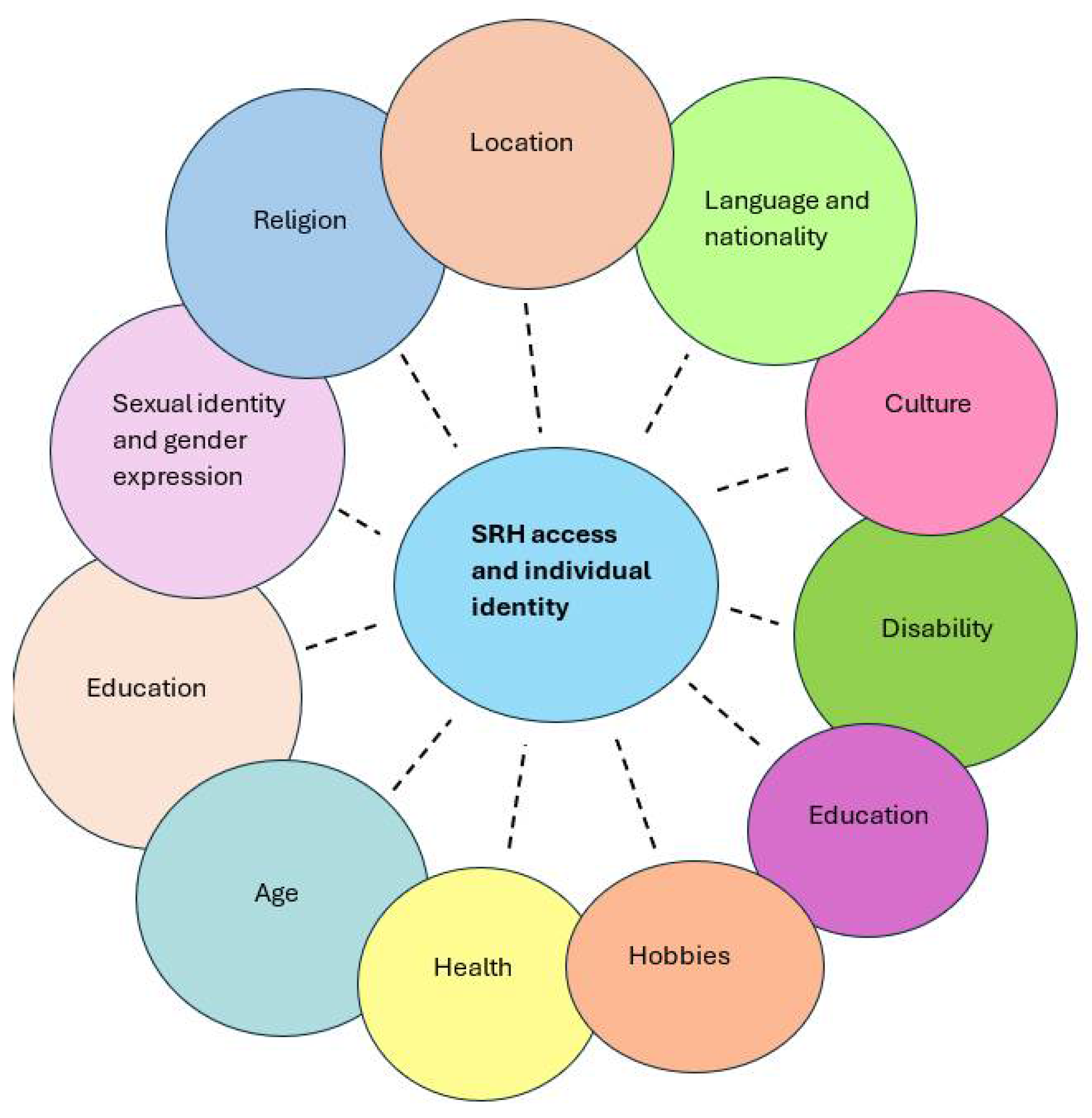
2. Intersectionality: A Critical Lens for Understanding Immigrant Adolescents’ SRH
3. Challenges Faced by Adolescents from Immigrant and Minority Backgrounds
3.1. Systemic Challenges (Limited Healthcare Access and Policy Barriers)
3.2. Individual Barriers (Cultural Barriers and Stigma)
4. Advances in SRH Promotion for Immigrant and Minority Adolescents
4.1. Innovative Interventions
4.1.1. Digital Health
4.1.2. Community-Based Interventions
4.2. Policy Shift
5. Gaps and Future Directions–Research Needs and Policy Recommendations
- 1.
- A Lack of Disaggregated Data
- 2.
- Limited Scalability and Integration of Culturally Adapted Interventions
- 3.
- Inadequate Policy Attention to Structural and Intersectional Inequities
- 4.
- Insufficient Youth Engagement in Programme Design and Evaluation
- 5.
- Limited Evidence on the Long-Term Impact of Digital SRH Interventions
- 6.
- Fragmented Funding and Inconsistent Evaluation Frameworks
6. Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Organization for Migration (IOM). Migration and Human Mobility: Key Global Figures. 2025. Available online: https://www.migrationdataportal.org/key-figures (accessed on 25 May 2025).
- International Organization for Migration (IOM). Child and Young Migrants. 2024. Available online: https://www.migrationdataportal.org/themes/child-and-young-migrants (accessed on 25 May 2025).
- Cristóbal-Narváez, P.; Febas Fernandez, M.; Rueda, M.J.; Aparicio Pareja, L. Invisible Youths? Future Health and Social Care Challenges of Unaccompanied Minor Migrants in Spain. In Multidisciplinary Perspectives on Immigrant Health: New Insights from Spain; Stanek, M., Juárez, S.P., Requena, M., Eds.; Springer Nature: Cham, Switzerland, 2025; pp. 91–114. [Google Scholar]
- Kanengoni-Nyatara, B.; Watson, K.; Galindo, C.; Charania, N.A.; Mpofu, C.; Holroyd, E. Barriers to and Recommendations for Equitable Access to Healthcare for Migrants and Refugees in Aotearoa, New Zealand: An Integrative Review. J. Immigr. Minor. Health 2024, 26, 164–180. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Sánchez, M.; Immordino, P.; Romano, G.; Giordano, A.; García-Gil, C.; Morales, F. Access of migrant women to sexual and reproductive health services: A systematic review. Midwifery 2024, 139, 104167. [Google Scholar] [CrossRef]
- Raymundo, G.; Smith-Merry, J.; McNab, J. Experiences of health service literacy and access amongst Australian young adults from migrant backgrounds. Health Promot. J. Aust. 2021, 32, 69–79. [Google Scholar] [CrossRef]
- NSW Centre for the Advancement of Adolescent Health The Children’s Hospital at Westmead. Access to Health Care Among NSW Adolescents, Phase 1 Final Report. 2002. Available online: https://www.health.nsw.gov.au/kidsfamilies/youth/Documents/access-phase-1-report.pdf#:~:text=By%20far%20the%20most%20significant%20of%20young,with%20embarrassment%20and%20shame%20in%20disclosing%20concerns (accessed on 24 May 2025).
- Galloway, C.T.; Duffy, J.L.; Dixon, R.P.; Fuller, T.R. Exploring African-American and Latino Teens’ Perceptions of Contraception and Access to Reproductive Health Care Services. J. Adolesc. Health 2017, 60, S57–S62. [Google Scholar] [CrossRef]
- Decker, M.J.; Atyam, T.V.; Zárate, C.G.; Bayer, A.M.; Bautista, C.; Saphir, M. Adolescents’ perceived barriers to accessing sexual and reproductive health services in California: A cross-sectional survey. BMC Health Serv. Res. 2021, 21, 1263. [Google Scholar] [CrossRef]
- Wang, W.; Wei, C.; Buchholz, M.E.; Martin, M.C.; Smith, B.D.; Huang, Z.J.; Wong, F.Y. Prevalence and risks for sexually transmitted infections among a national sample of migrants versus non-migrants in China. Int. J. STD AIDS 2010, 21, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Chow, E.P.; Zhao, P.; Xu, Y.; Ling, L.; Zhang, L. Rural-to-urban migrants are at high risk of sexually transmitted and viral hepatitis infections in China: A systematic review and meta-analysis. BMC Infect. Dis. 2014, 14, 490. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2016. 2016. Available online: https://www.cdc.gov/std/stats16/CDC_2016_STDS_Report-for508WebSep21_2017_1644.pdf (accessed on 25 May 2025).
- Hensel, D.J.; Nance, J.; Fortenberry, J.D. The Association Between Sexual Health and Physical, Mental, and Social Health in Adolescent Women. J. Adolesc. Health 2016, 59, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M. Positive sexuality and its impact on overall well-being. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013, 56, 208–214. [Google Scholar] [CrossRef]
- Riza, E.; Kalkman, S.; Coritsidis, A.; Koubardas, S.; Vassiliu, S.; Lazarou, D.; Karnaki, P.; Zota, D.; Kantzanou, M.; Psaltopoulou, T.; et al. Community-Based Healthcare for Migrants and Refugees: A Scoping Literature Review of Best Practices. Healthcare 2020, 8, 115. [Google Scholar] [CrossRef]
- Wolff, H.; Epiney, M.; Lourenco, A.P.; Costanza, M.C.; Delieutraz-Marchand, J.; Andreoli, N.; Dubuisson, J.B.; Gaspoz, J.M.; Irion, O. Undocumented migrants lack access to pregnancy care and prevention. BMC Public Health 2008, 8, 93. [Google Scholar] [CrossRef] [PubMed]
- Mengesha, Z.B.; Perz, J.; Dune, T.; Ussher, J. Refugee and migrant women’s engagement with sexual and reproductive health care in Australia: A socio-ecological analysis of health care professional perspectives. PLoS ONE 2017, 12, e0181421. [Google Scholar] [CrossRef] [PubMed]
- Napier-Raman, S.; Hossain, S.Z.; Lee, M.J.; Mpofu, E.; Liamputtong, P.; Dune, T. Migrant and refugee youth perspectives on sexual and reproductive health and rights in Australia: A systematic review. Sex. Health 2023, 20, 35–48. [Google Scholar] [CrossRef]
- Staneva, A.; Chai, A. Migrant well-being in Australia: Does locus of control matter? Econ. Hum. Biol. 2025, 56, 101447. [Google Scholar] [CrossRef] [PubMed]
- Crenshaw, K. Demarginalizing the intersection of race and sex: A black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. In Feminist Legal Theories; Routledge: Abingdon, UK, 1997. [Google Scholar]
- Bauer, G.R. Incorporating intersectionality theory into population health research methodology: Challenges and the potential to advance health equity. Soc. Sci. Med. 2014, 110, 10–17. [Google Scholar] [CrossRef]
- Kelly, C.; Kasperavicius, D.; Duncan, D.; Etherington, C.; Giangregorio, L.; Presseau, J.; Sibley, K.M.; Straus, S. ‘Doing’ or ‘using’ intersectionality? Opportunities and challenges in incorporating intersectionality into knowledge translation theory and practice. Int. J. Equity Health 2021, 20, 187. [Google Scholar] [CrossRef]
- Beck, A.; Corak, M.; Tienda, M. Age at Immigration and the Adult Attainments of Child Migrants to the United States. Ann. Am. Acad. Pol. Soc. Sci. 2012, 643, 134–159. [Google Scholar] [CrossRef]
- Istiko, S.N.; Simeon, R.; Aimable, N.; Valencia, M.M.E.; Vanessa, K.; Olivia, H.; Osborne, R.; Hou, J.Z.; Abell, B.; Mullens, A.B.; et al. Developing critical HIV health literacy: Insights from interviews with priority migrant communities in Queensland, Australia. Cult. Health Sex. 2024, 26, 936–951. [Google Scholar] [CrossRef]
- Development ICoPa. Sexual and Reproductive Health and Rights: An Essential Element of Universal Health Coverage. 2019. Available online: https://www.unfpa.org/sites/default/files/pub-pdf/SRHR_an_essential_element_of_UHC_SupplementAndUniversalAccess_27-online.pdf (accessed on 29 May 2025).
- Darebo, T.D.; Spigt, M.; Teklewold, B.; Badacho, A.S.; Mayer, N.; Teklewold, M. The sexual and reproductive healthcare challenges when dealing with female migrants and refugees in low and middle-income countries (a qualitative evidence synthesis). BMC Public Health 2024, 24, 520. [Google Scholar] [CrossRef]
- Hjelm, T.; Bondas, T.; Høgmo, B.K. Secret Voices are Breaking the Silence: A Meta-Ethnography of Perceptions of Sexual and Reproductive Health Among Resettled Refugee Youth. Glob. Qual. Nurs. Res. 2025, 12, 23333936251330688. [Google Scholar] [CrossRef]
- Maheen, H.; Chalmers, K.; Khaw, S.; McMichael, C. Sexual and reproductive health service utilisation of adolescents and young people from migrant and refugee backgrounds in high-income settings: A qualitative evidence synthesis (QES). Sex. Health 2021, 18, 283–293. [Google Scholar] [CrossRef] [PubMed]
- WHO. Refugee and Migrant Health. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/refugee-and-migrant-health (accessed on 25 May 2025).
- Githaiga, J.N.; Noll, S.; Olivier, J.; Amponsah-Dacosta, E. What’s in a name?—How migrant populations are classified and why these matters for (in)equitable access to routine childhood and adolescent immunisation services: A scoping review. Vaccine 2025, 49, 126784. [Google Scholar] [PubMed]
- Iwami, M.; Bouaddi, O.; Razai, M.S.; Mansour, R.; Morais, B.; Ali, N.M.; Crawsha, A.F.; Bojang, S.; Seedat, F.; Deal, A.; et al. Defining drivers of human papillomavirus (HPV) vaccine uptake in migrant populations globally and strategies and interventions to improve coverage: A systematic review. medRxiv, 2025; medRxiv:2025.01.31.25321303. [Google Scholar]
- Brewer, S.E.; Alsharea, E.; Wah, L.S. ‘I don’t know exactly what that means to do check-ups’: Understanding and experiences of primary care among resettled young adult refugees. Health Educ. Res. 2023, 39, 143–158. [Google Scholar] [CrossRef]
- D’Alonzo, K.T.; Greene, L. Strategies to establish and maintain trust when working in immigrant communities. Public Health Nurs. 2020, 37, 764–768. [Google Scholar] [CrossRef] [PubMed]
- Moezzi, S.M.I.; Etemadi, M.; Lankarani, K.B.; Behzadifar, M.; Katebzada, H.; Shahabi, S. Barriers and facilitators to primary healthcare utilization among immigrants and refugees of low and middle-income countries: A scoping review. Glob. Health 2024, 20, 75. [Google Scholar] [CrossRef]
- Sherif, B.; Awaisu, A.; Kheir, N. Refugee healthcare needs and barriers to accessing healthcare services in New Zealand: A qualitative phenomenological approach. BMC Health Serv. Res. 2022, 22, 1310. [Google Scholar] [CrossRef]
- Meherali, S.; Ismail, R.A.; Mariam, A.; Samar, K.; Piper, S.F.; Paula, P.-H.; Khan, Z.; Flicker, S.; Okeke-Ihejirika, P.; Salami, B.; et al. Between cultures and traditions: A qualitative investigation of sexual and reproductive health experiences of immigrant adolescents in Canada. Cult. Health Sex. 2024, 1, 1–17. [Google Scholar] [CrossRef]
- Aibangbee, M.; Micheal, S.; Mapedzahama, V.; Liamputtong, P.; Pithavadian, R.; Hossain, Z.; Mpofu, E.; Dune, T. Migrant and Refugee Youth’s Sexual and Reproductive Health and Rights: A Scoping Review to Inform Policies and Programs. Int. J. Public Health 2023, 68, 1605801. [Google Scholar] [CrossRef]
- Aibangbee, M.; Micheal, S.; Liamputtong, P.; Pithavadian, R.; Hossain, S.Z.; Mpofu, E.; Dune, T. Socioecologies in shaping migrants and refugee youths’ sexual and reproductive health and rights: A participatory action research study. Reprod. Health 2024, 21, 134. [Google Scholar] [CrossRef]
- Aibangbee, M.; Micheal, S.; Liamputtong, P.; Pithavadian, R.; Hossain, S.Z.; Mpofu, E.; Dune, T.M. Barriers to Sexual and Reproductive Health and Rights of Migrant and Refugee Youth: An Exploratory Socioecological Qualitative Analysis. Youth 2024, 4, 1538–1566. [Google Scholar] [CrossRef]
- Kohlenberger, J.; Buber-Ennser, I.; Rengs, B.; Leitner, S.; Landesmann, M. Barriers to health care access and service utilization of refugees in Austria: Evidence from a cross-sectional survey. Health Policy 2019, 123, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Wilson, F.A.; Stimpson, J.P. Federal and State Policies Affecting Immigrant Access to Health Care. JAMA Health Forum 2020, 1, e200271. [Google Scholar] [CrossRef]
- Heeren, M.; Wittmann, L.; Ehlert, U.; Schnyder, U.; Maier, T.; Müller, J. Psychopathology and resident status—Comparing asylum seekers, refugees, illegal migrants, labor migrants, and residents. Compr. Psychiatry 2014, 55, 818–825. [Google Scholar] [CrossRef]
- Konstantinou, E.; Murto, T.; Bacatum, C.; Félix, T.; Häsänen, M.; Oliveira, M.; Prapas, C.; Jogi, O.; Koutavelis, E.; Lähteenmäki, E.; et al. Migrants’ Perceptions and Needs in Sexual Health Education: A Focus Group Study. Sex. Cult. 2025, 29, 943–962. [Google Scholar] [CrossRef]
- Meherali, S.; Salami, B.; Okeke-Ihejirika, P.; Vallianatos, H.; Stevens, G. Barriers to and facilitators of South Asian immigrant adolescents’ access to sexual and reproductive health services in Canada: A qualitative study. Can. J. Hum. Sex. 2021, 30, e20200056. [Google Scholar] [CrossRef]
- Rawson, H.A.; Liamputtong, P. Culture and sex education: The acquisition of sexual knowledge for a group of Vietnamese Australian young women. Ethn. Health 2010, 15, 343–364. [Google Scholar] [CrossRef]
- Valdez, E.S.; Chan, J.; Donis, A.; Collins-Lovell, C.; Dixon, S.; Beatriz, E.; Gubrium, A. Structural Racism and Its Influence On Sexual and Reproductive Health Inequities Among Immigrant Youth. J. Immigr. Minor. Health 2023, 25, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Ezer, P.; Fisher, C.M.; Jones, T.; Power, J. Changes in Sexuality Education Teacher Training Since the Release of the Australian Curriculum. Sex. Res. Soc. Policy 2022, 19, 12–21. [Google Scholar] [CrossRef]
- WHO. Six Actions to Improve Adolescent Health. 2024. Available online: https://www.who.int/news-room/spotlight/six-actions-to-improve-adolescent-health (accessed on 27 May 2025).
- Sudhinaraset, M.; To, T.M.; Ling, I.; Melo, J.; Chavarin, J. The Influence of Deferred Action for Childhood Arrivals on Undocumented Asian and Pacific Islander Young Adults: Through a Social Determinants of Health Lens. J. Adolesc. Health 2017, 60, 741–746. [Google Scholar] [CrossRef]
- Raymond-Flesch, M.; Siemons, R.; Pourat, N.; Jacobs, K.; Brindis, C. There is No Help Out There and if There is, It’s Really Hard to Find: A Qualitative Study of the Healthcare Access and Concerns of Latino Dreamers. J. Adolesc. Health 2014, 54, S18–S19. [Google Scholar] [CrossRef]
- Suphanchaimat, R.; Kantamaturapoj, K.; Putthasri, W.; Prakongsai, P. Challenges in the provision of healthcare services for migrants: A systematic review through providers’ lens. BMC Health Serv. Res. 2015, 15, 390. [Google Scholar] [CrossRef] [PubMed]
- Asif, Z.; Kienzler, H. Structural barriers to refugee, asylum seeker and undocumented migrant healthcare access. Perceptions of Doctors of the World caseworkers in the UK. SSM Ment. Health 2022, 2, 100088. [Google Scholar] [CrossRef]
- Page, K.R.; Spiegel, P.B.; Cuneo, C.N. Detained at the doctor’s office: US immigration policy endangers health. BMJ 2025, 388, r304. [Google Scholar] [CrossRef]
- Juárez, S.P.; Honkaniemi, H.; Dunlavy, A.C.; Aldridge, R.W.; Barreto, M.L.; Katikireddi, S.V.; Rostila, M. Effects of non-health-targeted policies on migrant health: A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, e420–e435. [Google Scholar] [CrossRef] [PubMed]
- Metusela, C.; Ussher, J.; Perz, J.; Hawkey, A.; Morrow, M.; Narchal, R.; Estoesta, J.; Monteiro, M. In My Culture, We Don’t Know Anything About That: Sexual and Reproductive Health of Migrant and Refugee Women. Int. J. Behav. Med. 2017, 24, 836–845. [Google Scholar] [CrossRef]
- El Ansari, W.; Kareem, E.-A.; Arafa, M. Breaking the silence—systematic review of the socio-cultural underpinnings of men’s sexual and reproductive health in Middle East and North Africa (MENA): A handful of taboos? Arab. J. Urol. 2025, 23, 16–32. [Google Scholar] [CrossRef]
- Okeke, S. How perceived Australian sexual norms shape sexual practices of East Asian and sub-Saharan African international students in Sydney. BMC Public Health 2021, 21, 395. [Google Scholar] [CrossRef]
- Kiridaran, V.; Mehar, C.; Bailey, J.V. Views, attitudes and experiences of South Asian women concerning sexual health services in the UK: A qualitative study. Eur. J. Contracept. Reprod. Health Care 2022, 27, 418–423. [Google Scholar] [CrossRef]
- Mohd Tohit, N.F.; Haque, M. Forbidden Conversations: A Comprehensive Exploration of Taboos in Sexual and Reproductive Health. Cureus 2024, 16, e66723. [Google Scholar] [CrossRef]
- Betancourt, J.R.; Green, A.R.; Carrillo, J.E. Cultural Competence in Health Care: Emerging Frameworks and Practical Approaches. 2022. Available online: https://www.commonwealthfund.org/sites/default/files/documents/___media_files_publications_fund_report_2002_oct_cultural_competence_in_health_care__emerging_frameworks_and_practical_approaches_betancourt_culturalcompetence_576_pdf.pdf (accessed on 27 May 2025).
- Dong, Y.; Zhang, L.; Lam, C.; Huang, Z. Counteracting sexual and reproductive health misperceptions: Investigating the roles of stigma, misinformation exposure, and information overload. Patient Educ. Couns. 2024, 120, 108098. [Google Scholar] [CrossRef]
- Lirios, A.; Mullens, A.B.; Daken, K.; Moran, C.; Gu, Z.; Assefa, Y.; Dean, J.A. Sexual and reproductive health literacy of culturally and linguistically diverse young people in Australia: A systematic review. Cult. Health Sex. 2024, 26, 790–807. [Google Scholar] [CrossRef] [PubMed]
- Napier-Raman, S.; Bidewell, J.; Hossain, S.Z.; Mpofu, E.; Lee, M.J.; Liamputtong, P.; Dune, T. Migrant and Refugee Youth’s Sexual and Reproductive Health and Rights: A Gender Comparison of Knowledge, Behaviour, and Experiences. Sex. Cult. 2025, 29, 734–760. [Google Scholar] [CrossRef]
- Botfield, J.R.; Zwi, A.B.; Rutherford, A.; Newman, C.E. Learning about sex and relationships among migrant and refugee young people in Sydney, Australia: ‘I never got the talk about the birds and the bees’. Sex Educ. 2018, 18, 705–720. [Google Scholar] [CrossRef]
- Crankshaw, T.L.; Freedman, J.; Mutambara, V.M.; Rajah, Y. “I still don’t know how someone gets pregnant”: Determinants of poor reproductive health among young female refugees in South Africa. BMC Womens Health 2024, 24, 10. [Google Scholar] [CrossRef]
- Herzig van Wees, S.; Fried, S.; Larsson, E.C. Arabic speaking migrant parents’ perceptions of sex education in Sweden: A qualitative study. Sex. Reprod. Healthc. 2021, 28, 100596. [Google Scholar] [CrossRef] [PubMed]
- Tirado, V.; Engberg, S.; Holmblad, I.S.; Strömdahl, S.; Ekström, A.M.; Hurtig, A.K. “One-time interventions, it doesn’t lead to much”—healthcare provider views to improving sexual and reproductive health services for young migrants in Sweden. BMC Health Serv. Res. 2022, 22, 668. [Google Scholar] [CrossRef] [PubMed]
- Meherali, S.; Bhaumik, S.; Idrees, S.; Kennedy, M.; Lassi, Z.S. Digital knowledge translation tools for sexual and reproductive health information to adolescents: An evidence gap-map. Ther. Adv. Reprod. Health 2024, 18, 26334941241307881. [Google Scholar] [CrossRef]
- Brook Young People. Language and Cultural Barriers to Accessing Sexual Health Services. 2022. Available online: https://www.brook.org.uk/blog/language-and-cultural-barriers-to-accessing-sexual-health-services-2/ (accessed on 28 May 2025).
- Women’s Health Victoria. Refugees + Asylum Seekers. 2024. Available online: https://refugeehealthnetwork.org.au/ (accessed on 28 May 2025).
- Radu, I.; Scheermesser, M.; Spiess, M.R.; Schulze, C.; Händler-Schuster, D.; Pehlke-Milde, J. Digital Health for Migrants, Ethnic and Cultural Minorities and the Role of Participatory Development: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 6962. [Google Scholar] [CrossRef]
- Malloy, J.; Partridge, S.R.; Kemper, J.A.; Braakhuis, A.; Roy, R. Co-design of digital health interventions with young people: A scoping review. Digital Health 2023, 9, 20552076231219117. [Google Scholar] [CrossRef]
- Meherali, S.; Munro, S.; Puinean, G.; Salami, B.; Wong, J.P.H.; Vandermorris, A.; Scott, S.D. Co-designing a Sexual Health App With Immigrant Adolescents: Protocol for a Qualitative Community-Based Participatory Action Research Study. JMIR Res. Protoc. 2023, 12, e45389. [Google Scholar] [CrossRef]
- Castleton, P.; Meherali, S.; Memon, Z.; Lassi, Z.S. Understanding the contents and gaps in sexual and reproductive health toolkits designed for adolescence and young adults: A scoping review. Sex. Med. Rev. 2024, 12, 387–400. [Google Scholar] [CrossRef]
- Whitehead, L.; Talevski, J.; Fatehi, F.; Beauchamp, A. Barriers to and Facilitators of Digital Health Among Culturally and Linguistically Diverse Populations: Qualitative Systematic Review. J. Med. Internet Res. 2023, 25, e42719. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Fossey, E.; Palmer, V.J. A scoping review of the use of co-design methods with culturally and linguistically diverse communities to improve or adapt mental health services. Health Soc. Care Commun. 2021, 29, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Inthavong, A.B.; Pourmarzi, D. Characteristics of Sexual Health Programs for Migrants, Refugees, and Asylum Seekers: A Scoping Review. Int. J. Environ. Res. Public Health 2024, 21, 961. [Google Scholar] [CrossRef] [PubMed]
- Health MCFWs. Health in My Language. 2023. Available online: https://www.mcwh.com.au/project/health-in-my-language/ (accessed on 28 May 2025).
- Lang Leve de Liefde. English—Long Live Love. 2025. Available online: https://www.langlevedeliefde.nl/docenten/english (accessed on 28 May 2025).
- Schutte, L.; Meertens, R.M.; Mevissen, F.E.; Schaalma, H.; Meijer, S.; Kok, G. Long Live Love. The implementation of a school-based sex-education program in The Netherlands. Health Educ. Res. 2014, 29, 583–597. [Google Scholar] [CrossRef]
- Durbeej, N.; McDiarmid, S.; Sarkadi, A.; Feldman, I.; Punamäki, R.L.; Kankaanpää, R.; Osman, F. Evaluation of a school-based intervention to promote mental health of refugee youth in Sweden (The RefugeesWellSchool Trial): Study protocol for a cluster randomized controlled trial. Trials 2021, 22, 98. [Google Scholar] [CrossRef]
- Aidoo-Frimpong, G.; Nayem, J.; Adekunle, T.; Thomas, S.; Adekunle, T.; Asfaw, S.; Durado, A.; Williams, E.R.; Martinez, O.; Memiah, P.; et al. Exploring interactive stories for sexual health education among young adults in the USA. Health Promot. Int. 2025, 40, daaf031. [Google Scholar] [CrossRef]
- Huxtable, L.; Atcheson, A. Experiences of Delivering Comprehensive Relationships and Sexuality Education to Young People from Migrant and Refugee Backgrounds in Australia. Youth 2025, 5, 31. [Google Scholar] [CrossRef]
- Australian Council for Educational Research. EveryBODY Education Program. 2025. Available online: https://wellbeingguide.acer.org/program/sexual-health-victoria-everybody (accessed on 2 June 2025).
- Morin, G.; Marwah, S. Engaging in emotional and cultural work: Migrant mothers’ experiences of school-based sexuality education. Health Educ. J. 2024, 83, 917–931. [Google Scholar] [CrossRef]
- Feldstein Ewing, S.W.; Wray, A.M.; Mead, H.K.; Adams, S.K. Two approaches to tailoring treatment for cultural minority adolescents. J. Subst. Abuse Treat. 2012, 43, 190–203. [Google Scholar] [CrossRef]
- Munyai, H.S.; Makhado, L.; Ramathuba, D.U.; Lebese, R.T. Challenges regarding sexual health communication with secondary school learners in Limpopo Province: Parents views. Curationis 2023, 46, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Putri, Y.H.S.; Maryati, I.; Solehati, T. Interventions to Improve Sexual and Reproductive Health Related Knowledge and Attitudes Among the Adolescents: Scoping Review. Risk Manag. Healthc. Policy 2025, 18, 105–116. [Google Scholar] [CrossRef]
- Fleming, T.; Crengle, S.; Peiris-John, R.; Ball, J.; Fortune, S.; Yao, E.S.; Latimer, C.L.; Veukiso-Ulugia, A.; Clark, T.C. Priority actions for improving population youth mental health: An equity framework for Aotearoa New Zealand. Ment. Health Prev. 2024, 34, 200340. [Google Scholar] [CrossRef]
- Schaaf, M.; Arnott, G.; Chilufya, K.M.; Khanna, R.; Khanal, R.C.; Monga, T.; Otema, C.; Wegs, C. Social accountability as a strategy to promote sexual and reproductive health entitlements for stigmatized issues and populations. Int. J. Equity Health. 2022, 21 (Suppl. S1), 19. [Google Scholar] [CrossRef]
- Schoneveld, G.C. Sustainable business models for inclusive growth: Towards a conceptual foundation of inclusive business. J. Clean. Prod. 2020, 277, 124062. [Google Scholar] [CrossRef]
- Government of South Australia. Youth Action Plan 2024–2027. 2023. Available online: https://dhs.sa.gov.au/__data/assets/pdf_file/0017/157121/Youth-Action-Plan-Consultation-Report-2023.pdf (accessed on 2 June 2025).
- Association, A.M. Refugee and Asylum Seeker Health and Wellbeing. 2023. Available online: https://www.ama.com.au/sites/default/files/2024-02/AMA%20Refugee%20and%20Asylum%20Seeker%20Health%20Position%20Statement%202023.pdf (accessed on 2 June 2025).
- US Centers for Disease Control and Prevention. Sexual and Reproductive Health: Refugee Health Domestic Guidance. 2025. Available online: https://www.cdc.gov/immigrant-refugee-health/hcp/domestic-guidance/sexual-and-reproductive-health.html (accessed on 2 June 2025).
- WHO. Closing Data Gaps in Gender. 2019. Available online: https://www.who.int/activities/closing-data-gaps-in-gender (accessed on 1 May 2025).
- Mosler Vidal, E. Leave No Migrant Behind: The 2030 Agenda and Data Disaggregation; International Organisation for Migration (IOM): Geneva, Switzerland, 2021. [Google Scholar]
- Kesterton, A.J.; Cabral de Mello, M. Generating demand and community support for sexual and reproductive health services for young people: A review of the Literature and Programs. Reprod. Health 2010, 7, 25. [Google Scholar] [CrossRef] [PubMed]
- WHO. Generating Demand and Community Support for Sexual and Reproductive Health Services for Young People. 2009. Available online: https://www.who.int/publications/i/item/9789241598484 (accessed on 29 May 2025).
- Lisa Roberts. Culturally and Linguistically Diverse Children and Young People: A Literature Review. 2014. Available online: https://ccyp.wa.gov.au/media/zukjulha/literature-review-culturally-and-linguistically-diverse-children-and-young-people-october-2014.pdf?utm_source=chatgpt.com (accessed on 29 May 2025).
- WHO. WHO Community Engagement Framework for Quality, People-Centred and Resilient Health Services. 2017. Available online: https://iris.who.int/bitstream/handle/10665/259280/WHO-HIS-SDS-2017.15-eng.pdf?sequence=1 (accessed on 29 May 2025).
- Ngondwe, P.; Tefera, G.M. Barriers and Facilitators of Access to Healthcare Among Immigrants with Disabilities: A Qualitative Meta-Synthesis. Healthcare 2025, 13, 313. [Google Scholar] [CrossRef]
- Khatri, R.B.; Assefa, Y. Access to health services among culturally and linguistically diverse populations in the Australian universal health care system: Issues and challenges. BMC Public Health 2022, 22, 880. [Google Scholar] [CrossRef]
- Vergani, M.; Mansouri, F.; Weng, E.; Rajkobal, P. The effectiveness of ethno-specific and mainstream health services: An evidence gap map. BMC Health Serv. Res. 2022, 22, 879. [Google Scholar] [CrossRef]
- Andersson Nystedt, T.; Herder, T.; Agardh, A.; Asamoah, B.O. Included and excluded: An intersectionality-based policy analysis of young migrants’ vulnerability to sexual violence in Sweden. Int. J. Equity Health 2025, 24, 86. [Google Scholar] [CrossRef]
- Oumnia, B.; Saad, Z.; Zakaria, B. Interventions to improve migrantsâ access to sexual and reproductive health services: A scoping review. BMJ Glob. Health 2023, 8, e011981. [Google Scholar]
- Szymuś, K.; Manaboriboon, N.; Mohammed, F.E.A.; Hanna, K.F.; Okonkwo, E.H.; Măties, M.; Nasrallah, M.; Shukla, V. Meaningful youth engagement in sexual and reproductive health and rights decision making. Lancet Glob. Health 2024, 12, e20–e21. [Google Scholar] [CrossRef] [PubMed]
- High Impact Practice. Meaningful Adolescent and Youth Engagement and Partnership in Sexual and Reproductive Health Programming: A Strategic Planning Guide. 2022. Available online: https://www.fphighimpactpractices.org/wp-content/uploads/2022/03/HIP-Meaningful-Adolescent-and-Youth-Engagement_SPG.pdf? (accessed on 2 May 2025).
- Sewak, A.; Yousef, M.; Deshpande, S.; Seydel, T.; Hashemi, N. The effectiveness of digital sexual health interventions for young adults: A systematic literature review (2010–2020). Health Promot. Int. 2023, 38, daac104. [Google Scholar] [CrossRef]
- Rabet, R.; Bagree, E.; Salam, Z.; Wahoush, O. Barriers and facilitators to digital primary health care access in immigrant and refugee populations: A scoping review. J. Public Health 2024, 1, e25863. [Google Scholar] [CrossRef]
- Maita, K.C.; Maniaci, M.J.; Haider, C.R.; Avila, F.R.; Torres-Guzman, R.A.; Borna, S.; Lunde, J.J.; Coffey, J.D.; Demaerschalk, B.M.; Forte, A.J. The Impact of Digital Health Solutions on Bridging the Health Care Gap in Rural Areas: A Scoping Review. Perm. J. 2024, 28, 130–143. [Google Scholar] [CrossRef] [PubMed]
- Dear Digital Equity. Cultural Competence Toolkit. 2023. Available online: https://www.deardigitalequity.org/cultural-competence-toolkit (accessed on 27 May 2025).
- Naderbagi, A.; Loblay, V.; Zahed, I.U.M.; Ekambareshwar, M.; Poulsen, A.; Song, Y.J.; Ospina-Pinillos, L.; Krausz, M.; Mamdouh Kamel, M.; Hickie, I.B.; et al. Cultural and contextual adaptation of digital health interventions: Narrative review. J. Med. Internet Res. 2024, 26, e55130. [Google Scholar] [CrossRef]
- YIELD Hub. Sustainable Financing for Youth-Led Organisations: Exploring the Challenges and Possibilities (Action Learning Cycle #6 Priority Brief). 2024. Available online: https://yieldhub.global/wp-content/uploads/2024/02/Cycle-6-Priority-Brief.pdf? (accessed on 2 May 2025).
- Women’s Refugee Commission; United Nations Children’s Fund. Toolkit for Monitoring and Evaluating Adolescent Sexual and Reproductive Health Interventions in Safe Spaces. 2020. Available online: https://www.womensrefugeecommission.org/wp-content/uploads/2020/05/Toolkit-ME-adolescent-sexual-reproductive-health-interventions-safe-spaces-WRC-UNICEF-EN.pdf? (accessed on 2 May 2025).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castleton, P.; Chaudhry, A.S.; Damabi, N.; Meherali, S.; Lassi, Z.S. Crossing Borders: SRH Challenges Among Immigrant and Minority Adolescents. Int. J. Environ. Res. Public Health 2025, 22, 1101. https://doi.org/10.3390/ijerph22071101
Castleton P, Chaudhry AS, Damabi N, Meherali S, Lassi ZS. Crossing Borders: SRH Challenges Among Immigrant and Minority Adolescents. International Journal of Environmental Research and Public Health. 2025; 22(7):1101. https://doi.org/10.3390/ijerph22071101
Chicago/Turabian StyleCastleton, Patience, Ahmed Shabbir Chaudhry, Negin Damabi, Salima Meherali, and Zohra S. Lassi. 2025. "Crossing Borders: SRH Challenges Among Immigrant and Minority Adolescents" International Journal of Environmental Research and Public Health 22, no. 7: 1101. https://doi.org/10.3390/ijerph22071101
APA StyleCastleton, P., Chaudhry, A. S., Damabi, N., Meherali, S., & Lassi, Z. S. (2025). Crossing Borders: SRH Challenges Among Immigrant and Minority Adolescents. International Journal of Environmental Research and Public Health, 22(7), 1101. https://doi.org/10.3390/ijerph22071101