
The Longitudinal Relationship Between Physical Functions and Cognitive Functions Among Middle-Aged and Older Adults in Primary Care



Abstract
1. Introduction
2. Materials and Methods
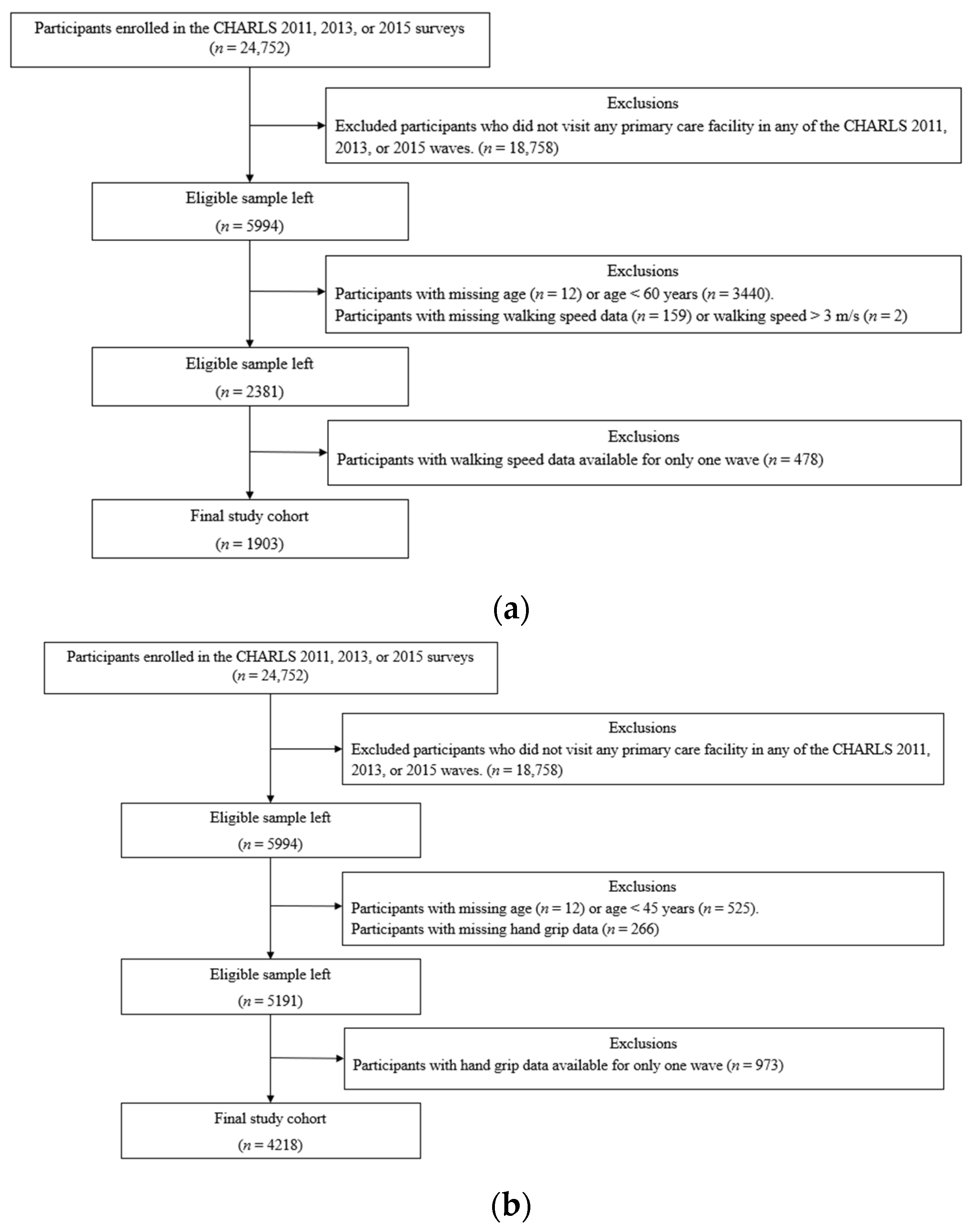
2.1. Data Source and Study Population
2.2. Measurements
2.2.1. Measurement of Cognitive Function
2.2.2. Assessment of GS
2.2.3. Assessment of HGS
2.2.4. Covariates
2.3. Statistical Analysis
2.4. Reporting
3. Results
3.1. Sample Characteristics
3.2. Association Between GS and Cognitive Functions
3.3. Association Between HGS and Cognitive Functions
3.4. Impact of Baseline GS on Temporal Change in Cognitive Functions
3.5. Impact of Baseline HGS on Temporal Changes in Cognitive Functions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CHARLS | China Health and Retirement Longitudinal Study |
| CI | Confidence interval |
| HGS | Hand grip strength |
| GS | Gait speed |
| GLMM | Generalized linear mixed-effects model |
| OCS | Overall cognitive score |
| OR | Odds ratio |
| PA | Physical activity |
References
- Nie, W.; Hu, J. The relationship between grip strength and cognitive impairment: Evidence from NHANES 2011–2014. Brain Behav. 2025, 15, e70381. [Google Scholar] [CrossRef] [PubMed]
- Blazer, D.G. Depression in late life: Review and commentary. J. Gerontol. Ser. A 2003, 58, M249–M265. [Google Scholar] [CrossRef] [PubMed]
- Yarnall, A.J.; Sayer, A.A.; Clegg, A.; Rockwood, K.; Parker, S.; Hindle, J.V. New horizons in multimorbidity in older adults. Age Ageing 2017, 46, 882–888. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Taekema, D.G.; Ling, C.H.Y.; Kurrle, S.E.; Cameron, I.D.; Meskers, C.G.M.; Blauw, G.J.; Westendorp, R.G.J.; de Craen, A.J.M.; Maier, A.B. Temporal relationship between handgrip strength and cognitive performance in oldest old people. Age Ageing 2012, 41, 506–512. [Google Scholar] [CrossRef]
- Liu, Y.; Cui, J.; Luo, X.; Wang, Z.; Shen, Z.; Fang, Y.; Li, C.; Hong, J. Longitudinal association between handgrip strength and depressive symptoms in middle-aged and older Chinese adults: Mediating role of functional limitation. Front. Public Health 2025, 13, 1496641. [Google Scholar] [CrossRef]
- Chai, S.; Zhao, D.; Gao, T.; Wang, X.; Wang, X.; Luo, J.; Li, J.; Zhou, C. The relationship between handgrip strength and cognitive function among older adults in China: Functional limitation plays a mediating role. J. Affect. Disord. 2024, 347, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Abudukelimu, N.; Zhang, P.; Du, J.; Li, M.; Shen, Y.; Mao, Y.; Wang, D.; Zhu, Q. Association of handgrip strength weakness and asymmetry with cognitive impairment and depressive symptoms in older Chinese adults. Sci. Rep. 2025, 15, 9763. [Google Scholar] [CrossRef]
- Huang, J.; Wang, X.; Zhu, H.; Huang, D.; Li, W.; Wang, J.; Liu, Z. Association between grip strength and cognitive impairment in older American adults. Front. Mol. Neurosci. 2022, 15, 973700. [Google Scholar] [CrossRef]
- Chen, K.K.; Lee, S.Y.; Pang, B.W.J.; Lau, L.K.; Jabbar, K.A.; Seah, W.T.; Tou, N.X.; Yap, P.L.K.; Ng, T.P.; Wee, S.-L. Associations of low handgrip strength and hand laterality with cognitive function and functional mobility: The Yishun study. BMC Geriatr. 2022, 22, 677. [Google Scholar] [CrossRef]
- Bohannon, R.W. Grip strength: An indispensable biomarker for older adults. Clin. Interv. Aging 2019, 14, 1681–1691. [Google Scholar] [CrossRef]
- Yang, J.; Deng, Y.; Yan, H.; Li, B.; Wang, Z.; Liao, J.; Cai, X.; Zhou, L.; Tan, W.; Rong, S. Association between grip strength and cognitive function in US older adults of NHANES 2011–2014. J. Alzheimer’s Dis. 2022, 89, 427–436. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, H.Y. Nomogram for predicting changes in cognitive function in community-dwelling older adults with mild cognitive impairment: A retrospective study. J. Korean Acad. Nurs. 2025, 55, 50–63. [Google Scholar] [CrossRef]
- Prokopidis, K.; Giannos, P.; Ispoglou, T.; Kirk, B.; Witard, O.C.; Dionyssiotis, Y.; Scott, D.; Macpherson, H.; Duque, G.; Isanejad, M. Handgrip strength is associated with learning and verbal fluency in older men without dementia: Insights from the NHANES. Geroscience 2023, 45, 1049–1058. [Google Scholar] [CrossRef]
- Rasmussen, L.J.H.; Caspi, A.; Ambler, A.; Broadbent, J.M.; Cohen, H.J.; D’arbeloff, T.; Elliott, M.; Hancox, R.J.; Harrington, H.; Hogan, S.; et al. Association of neurocognitive and physical function with gait speed in midlife. JAMA Netw. Open 2019, 2, e1913123. [Google Scholar] [CrossRef]
- Sui, S.X.; Williams, L.J.; Holloway-Kew, K.L.; Hyde, N.K.; Pasco, J.A. Skeletal muscle health and cognitive function: A narrative review. Int. J. Mol. Sci. 2021, 22, 255. [Google Scholar] [CrossRef]
- Ali, P.; Renaud, P.; Montero-Odasso, M.; Gautier, J.; Dinomais, M.; Annweiler, C. Gait performance in older adults across the cognitive spectrum: Results from the GAIT cohort. J. Am. Geriatr. Soc. 2024, 72, 3437–3447. [Google Scholar] [CrossRef]
- Peel, N.M.; Alapatt, L.J.; Jones, L.V.; Hubbard, R.E. The association between gait speed and cognitive status in community-dwelling older people: A systematic review. J. Am. Geriatr. Soc. 2019, 67, 776–783. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, H.; Chen, Y.; Cai, M.; Guo, C.; Chen, P. Association between walking speed and cognitive domain functions in Chinese suburban-dwelling older adults. Front. Aging Neurosci. 2022, 14, 935291. [Google Scholar] [CrossRef]
- Peel, N.M.; Kuys, S.S.; Klein, K. Gait speed as a measure in geriatric assessment in clinical settings: A systematic review. J. Gerontol. Ser. A 2013, 68, 39–46. [Google Scholar] [CrossRef]
- Tian, Q.; Montero-Odasso, M.; Buchman, A.S.; Mielke, M.M.; Espinoza, S.; DeCarli, C.S.; Newman, A.B.; Kritchevsky, S.B.; Rebok, G.W.; Resnick, S.M.; et al. Dual cognitive and mobility impairments and future dementia: Setting a research agenda. Alzheimer’s Dement. 2023, 19, 1579–1586. [Google Scholar] [CrossRef]
- Hao, W.; Zhao, W.; Kimura, T.; Ukawa, S.; Kadoya, K.; Kondo, K.; Tamakoshi, A. Association of gait with global cognitive function and cognitive domains detected by MoCA-J among community-dwelling older adults: A cross-sectional study. BMC Geriatr. 2021, 21, 523. [Google Scholar] [CrossRef]
- Su, Y.-H.; Chiou, J.-M.; Shiu, C.; Chen, J.-H.; Chen, Y.-C. Longitudinal, bidirectional association between gait speed and cognitive function in community-dwelling older adults without dementia. J. Am. Med. Dir. Assoc. 2025, 26, 105544. [Google Scholar] [CrossRef]
- Windham, B.G.; Parker, S.B.; Zhu, X.; Gabriel, K.P.; Palta, P.; Sullivan, K.J.; Parker, K.G.; Knopman, D.S.; Gottesman, R.F.; Griswold, M.E.; et al. Endurance and gait speed relationships with mild cognitive impairment and dementia. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2022, 14, e12281. [Google Scholar] [CrossRef]
- Chou, M.-Y.; Nishita, Y.; Nakagawa, T.; Tange, C.; Tomida, M.; Shimokata, H.; Otsuka, R.; Chen, L.-K.; Arai, H. Role of gait speed and grip strength in predicting 10-year cognitive decline among community-dwelling older people. BMC Geriatr. 2019, 19, 186. [Google Scholar] [CrossRef]
- Gunnarsson, D.V.; Miskowiak, K.W.; Pedersen, J.K.; Hansen, H.; Podlekareva, D.; Johnsen, S.; Dall, C.H. Physical function and association with cognitive function in patients in a post-COVID-19 clinic: A cross-sectional study. Int. J. Environ. Res. Public Health 2023, 20, 5866. [Google Scholar] [CrossRef]
- Zhao, Y.; Hu, Y.; Smith, J.P.; Strauss, J.; Yang, G. Cohort profile: The China Health and Retirement Longitudinal Study (CHARLS). Int. J. Epidemiol. 2014, 43, 61–68. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Wang, T.-Y.; Chen, W.-M.; Chen, K.-H.; Yang, Y.-H.; Chen, P.-C.; Chen, V.C.-H. Physical performance and risk of hip fracture in community-dwelling elderly people in China: A 4-year longitudinal cohort study. Maturitas 2021, 146, 26–33. [Google Scholar] [CrossRef]
- Huang, W.; Zhou, Y. Effects of education on cognition at older ages: Evidence from China’s Great Famine. Soc. Sci. Med. 2013, 98, 54–62. [Google Scholar] [CrossRef]
- Kanne, G.E.; McConnell, E.S.; Disco, M.E.; Black, M.C.; Upchurch, G.; Matters, L.M.; Halpern, D.J.; White, H.K.; Heflin, M.T. Association between bidirectional intergenerational support and successful aging in China: Evidence from CHARLS 2018. Geriatr. Nurs. 2023, 49, 81–88. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Lipton, R.B.; Katz, M.J.; Kuslansky, G.; Sliwinski, M.J.; Stewart, W.F.; Verghese, J.; Crystal, H.A.; Buschke, H. Screening for dementia by telephone using the memory impairment screen. J. Am. Geriatr. Soc. 2003, 51, 1382–1390. [Google Scholar] [CrossRef]
- Fong, T.G.; Fearing, M.A.; Jones, R.N.; Shi, P.; Marcantonio, E.R.; Rudolph, J.L.; Yang, F.M.; Kiely, K.D.; Inouye, S.K. Telephone interview for cognitive status: Creating a crosswalk with the Mini-Mental State Examination. Alzheimer’s Dement. 2009, 5, 492–497. [Google Scholar] [CrossRef]
- Zhang, K.; Zhang, W. Adverse childhood experiences and mild cognitive impairment in later life: Exploring rural/urban and gender differences using CHARLS. J. Appl. Gerontol. 2022, 41, 1454–1464. [Google Scholar] [CrossRef]
- Rong, H.; Lai, X.; Mahmoudi, E.; Fang, H. Early-life exposure to the Chinese famine and risk of cognitive decline. J. Clin. Med. 2019, 8, 484. [Google Scholar] [CrossRef]
- Liu, J.; Cui, K.; Chen, Q.; Li, Z.; Fu, J.; Gong, X.; Xu, H. Association of walking speed with cognitive function in Chinese older adults: A nationally representative cohort study. Front. Aging Neurosci. 2022, 14, 1003896. [Google Scholar] [CrossRef]
- Lin, L.; Sun, W.; Lu, C.; Chen, W.; Guo, V.Y. Adverse childhood experiences and handgrip strength among middle-aged and older adults: A cross-sectional study in China. BMC Geriatr. 2022, 22, 118. [Google Scholar] [CrossRef]
- Chen, Z.; Ho, M.; Chau, P.H. Handgrip strength asymmetry is associated with the risk of neurodegenerative disorders among Chinese older adults. J. Cachexia Sarcopenia Muscle 2022, 13, 1013–1023. [Google Scholar] [CrossRef]
- Zhao, Y.; Strauss, J.; Yang, G.; Giles, J.; Hu, P.; Hu, Y.; Lei, H.Y.; Liu, M.; Park, A.; Smith, J.P.; et al. China Health and Retirement Longitudinal Study–2011–2012 National Baseline Users’ Guide; National School of Development, Peking University: Beijing, China, 2013; Volume 2, pp. 61–68. [Google Scholar]
- Phillips, D.; Green, H.; Petrosyan, S.; Shao, K.; Wilkens, J.; Lee, J. Harmonized CHARLS documentation: Version D (2011–2018). Available online: https://charls.charlsdata.com/pages/Data/harmonized_charls/en.html (accessed on 29 April 2025).
- O’Brien, L.; Forster, J. Physical activity supporting connection to nature, and helping to maintain wellbeing during the COVID-19 restrictions in England. Int. J. Environ. Res. Public Health 2021, 18, 4585. [Google Scholar] [CrossRef]
- Zhou, M.; Kuang, L.; Hu, N. The association between physical activity and intrinsic capacity in Chinese older adults and its connection to primary care: China Health and Retirement Longitudinal Study (CHARLS). Int. J. Environ. Res. Public Health 2023, 20, 5361. [Google Scholar] [CrossRef]
- Yin, W.; Sifre-Acosta, N.; Chamorro, D.; Chowdhury, S.; Hu, N. Impact of physical activity on health behavior change and mental health during the COVID-19 epidemic among Chinese adults: China Health and Retirement Longitudinal Study (CHARLS). Int. J. Environ. Res. Public Health 2025, 22, 201. [Google Scholar] [CrossRef] [PubMed]
- Clouston, S.A.; Brewster, P.; Kuh, D.; Richards, M.; Cooper, R.; Hardy, R.; Rubin, M.S.; Hofer, S.M. The dynamic relationship between physical function and cognition in longitudinal aging cohorts. Epidemiol. Rev. 2013, 35, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.R.; Sun, J.; Han, M.; Nam, C.M.; Park, S. Evaluation of the directional relationship between handgrip strength and cognitive function: The Korean Longitudinal Study of Ageing. Age Ageing 2019, 48, 426–432. [Google Scholar] [CrossRef]
- Li, H.; Zhang, J.; Zou, X.; Jia, X.; Zheng, D.; Guo, X.; Xie, W.; Yang, Q. The bidirectional association between cognitive function and gait speed in Chinese older adults: Longitudinal observational study. JMIR Public Health Surveill. 2023, 9, e44274. [Google Scholar] [CrossRef]
- Rosso, A.L.; Metti, A.L.; Faulkner, K.; Redfern, M.; Yaffe, K.; Launer, L.; Shaaban, C.E.; Nadkarni, N.K.; Rosano, C. Complex walking tasks and risk for cognitive decline in high-functioning older adults. J. Alzheimer’s Dis. 2019, 71 (Suppl. S1), S65–S73. [Google Scholar] [CrossRef]
- Hackett, R.A.; Davies-Kershaw, H.; Cadar, D.; Orrell, M.; Steptoe, A. Walking speed, cognitive function, and dementia risk in the English Longitudinal Study of Ageing. J. Am. Geriatr. Soc. 2018, 66, 1670–1675. [Google Scholar] [CrossRef]
- Best, J.R.; Liu-Ambrose, T.; Boudreau, R.M.; Ayonayon, H.N.; Satterfield, S.; Simonsick, E.M.; Studenski, S.; Yaffe, K.; Newman, A.B.; Rosano, C. An evaluation of the longitudinal, bidirectional associations between gait speed and cognition in older women and men. J. Gerontol. Ser. A 2016, 71, 1616–1623. [Google Scholar] [CrossRef]
- Hooghiemstra, A.M.; Ramakers, I.H.G.B.; Sistermans, N.; Pijnenburg, Y.A.L.; Aalten, P.; Hamel, R.E.G.; Melis, R.J.F.; Verhey, F.R.J.; Olde Rikkert, M.G.M.; Scheltens, P.; et al. Gait Speed and Grip Strength Reflect Cognitive Impairment and Are Modestly Related to Incident Cognitive Decline in Memory Clinic Patients With Subjective Cognitive Decline and Mild Cognitive Impairment: Findings From the 4C Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.-M.; Choi, S.; Kim, K.; Kim, S.M.; Kim, S.; Park, S.M. Association among handgrip strength, body mass index, and decline in cognitive function among elderly women. BMC Geriatr. 2018, 18, 91. [Google Scholar] [CrossRef]
- Feng, W.; Chen, Q.; Ma, M.; Xu, J.; Guo, H.; Yuan, W.; Li, R.; Gao, H.; Gu, C.; Ma, Y.; et al. Sex-modified association between grip strength and mild cognitive impairment: A cross-sectional and follow-up study in rural China. BMC Geriatr. 2023, 23, 710. [Google Scholar] [CrossRef]
- Lee, S.; Oh, J.W.; Son, N.H.; Chung, W. Association between handgrip strength and cognitive function in older adults: Korean Longitudinal Study of Aging (2006–2018). Int. J. Environ. Res. Public Health 2022, 19, 1048. [Google Scholar] [CrossRef] [PubMed]
- Haagsma, A.B.; Souza, D.L.B.; Vasconcellos, G.M.; Olandoski, M.; Jerez-Roig, J.; Baena, C.P. Longitudinal relationship between handgrip strength and cognitive function in a European multicentric population older than 50 years. Phys. Ther. 2023, 103, pzad057. [Google Scholar] [CrossRef]
- Bun, S.; Suzuki, K.; Niimura, H.; Shikimoto, R.; Kida, H.; Shibata, M.; Honda, T.; Ohara, T.; Hata, J.; Nakaji, S.; et al. Gender and age influence the association between gait speed and mild cognitive impairment in community-dwelling Japanese older adults: From the Japan Prospective Studies Collaboration for Ageing and Dementia (JPSC-AD). Psychogeriatrics 2023, 23, 918–929. [Google Scholar] [CrossRef]
- Hill, A.B. The environment and disease: Association or causation? Proc. R. Soc. Med. 1965, 58, 295–300. [Google Scholar] [CrossRef]
- Quigley, A.; MacKay-Lyons, M.; Eskes, G. Effects of exercise on cognitive performance in older adults: A narrative review of the evidence, possible biological mechanisms, and recommendations for exercise prescription. J. Aging Res. 2020, 2020, 1407896. [Google Scholar] [CrossRef]
- Valenzuela, P.L.; Saco-Ledo, G.; Morales, J.S.; Gallardo-Gómez, D.; Morales-Palomo, F.; López-Ortiz, S.; Rivas-Baeza, B.; Castillo-García, A.; Jiménez-Pavón, D.; Santos-Lozano, A.; et al. Effects of physical exercise on physical function in older adults in residential care: A systematic review and network meta-analysis of randomised controlled trials. Lancet Healthy Longev. 2023, 4, e247–e256. [Google Scholar] [CrossRef]
- Abo, M.; Hamaguchi, T. Effectiveness of a dual-task intervention involving exercise and vocalized cognitive tasks. J. Clin. Med. 2024, 13, 2962. [Google Scholar] [CrossRef]
- Tan, L.F.; Chan, Y.H.; Seetharaman, S.; Denishkrshna, A.; Au, L.; Kwek, S.C.; Chen, M.Z.; Ng, S.E.; Hui, R.J.Y.; Merchant, R.A. Impact of exercise and cognitive stimulation therapy on physical function, cognition and muscle mass in pre-frail older adults in the primary care setting: A cluster randomized controlled trial. J. Nutr. Health Aging 2023, 27, 438–447. [Google Scholar] [CrossRef]

{kind=link}
| (a) | ||||||||
| Variables | All Subjects (N = 1903) | Baseline GS Status | ||||||
| Low GS (N = 964, 50.66%) | High GS (N = 939, 49.34%) | p1 | ||||||
| N (%) | Mean (SD) | N (%) | Mean (SD) | N (%) | Mean (SD) | |||
| Age at baseline (years) | 67.43 (5.99) | 68.80 (6.47) | 66.03 (5.09) | <0.001 | ||||
| Gender | Male | 880 (46.24) | 377 (39.11) | 503 (53.57) | <0.001 | |||
| Female | 1023 (53.76) | 587 (60.89) | 436 (46.43) | |||||
| Education Level | Less than lower secondary | 1842 (96.79) | 949 (98.44) | 893 (95.10) | <0.001 | |||
| Upper secondary and vocational training or above | 61 (3.21) | 15 (1.56) | 46 (4.90) | |||||
| BMI | Underweight | 218 (11.46) | 118 (12.24) | 100 (10.65) | 0.499 | |||
| Normal weight | 853 (44.82) | 427 (44.29) | 426 (45.37) | |||||
| Overweight | 355 (18.65) | 173 (17.95) | 182 (19.38) | |||||
| Obesity | 457 (24.01) | 23 (24.17) | 224 (23.86) | |||||
| Missing | 20 (1.05) | 13 (1.35) | 7 (0.75) | |||||
| Household Income | Low | 727 (38.20) | 408 (42.32) | 319 (33.97) | <0.001 | |||
| High | 726 (38.15) | 342 (35.48) | 384 (40.89) | |||||
| Missing | 450 (23.65) | 214 (22.20) | 236 (25.13) | |||||
| Able to Draw Assigned Picture | No | 912 (47.92) | 520 (53.94) | 392 (41.75) | <0.001 | |||
| Yes | 928 (48.77) | 400 (41.49) | 528 (56.23) | |||||
| Missing | 63 (3.31) | 44 (4.56) | 19 (2.02) | |||||
| TICS-10 | Low | 915 (48.08) | 536 (55.60) | 379 (40.36) | <0.001 | |||
| High | 904 (47.50) | 370 (38.38) | 534 (56.87) | |||||
| Missing | 84 (4.41) | 58 (6.02) | 26 (2.77) | |||||
| Word Recall | Low | 311 (16.34) | 195 (20.23) | 116 (12.35) | <0.001 | |||
| High | 1508 (79.24) | 711 (73.76) | 797 (84.88) | |||||
| Missing | 84 (4.41) | 58 (6.02) | 26 (2.77) | |||||
| Overall Cognition Score (N = 1859) | 10.02 (4.55) | 8.96 (4.54) | 11.09 (4.30) | <0.001 | ||||
| (b) | ||||||||
| Variables | All Subjects (N = 4218) | By Baseline HGS Status | ||||||
| Low HGS (N = 2186, 51.83%) | High HGS (N = 2032, 48.17%) | p 1 | ||||||
| N (%) | Mean (SD) | N (%) | Mean (SD) | N (%) | Mean (SD) | |||
| Age at Baseline (years) | 59.38(9.22) | 61.23 (9.55) | 57.40 (8.42) | <0.001 | ||||
| Gender | Male | 1756 (41.63) | 325 (14.87) | 1431 (70.42) | <0.001 | |||
| Female | 2462 (58.37) | 1861(85.13) | 601 (29.58) | |||||
| Education Level | Less than lower secondary | 3928 (93.12) | 2109 (96.48) | 1819 (89.52) | <0.001 | |||
| Upper secondary and vocational training or above | 290 (6.88) | 77 (3.52) | 213 (10.48) | |||||
| BMI | Underweight | 337 (7.99) | 224 (10.25) | 113 (5.56) | <0.001 | |||
| Normal weight | 1710 (40.54) | 861 (39.39) | 849 (41.78) | |||||
| Overweight | 817 (19.37) | 396 (18.12) | 421 (20.72) | |||||
| Obesity | 1301 (30.84) | 673 (30.79) | 628 (30.91) | |||||
| Missing | 53 (1.26) | 32 (1.46) | 21 (1.03) | |||||
| Household Income | Low | 1383 (32.79) | 780 (35.68) | 603 (29.68) | <0.001 | |||
| High | 1382 (32.76) | 705 (32.25) | 677 (33.32) | |||||
| Missing | 1453 (34.45) | 701 (32.07) | 752 (37.01) | |||||
| Able to Draw Assigned Picture | No | 1724 (40.87) | 1133 (51.83) | 591 (29.08) | <0.001 | |||
| Yes | 2386 (56.57) | 981 (44.88) | 1405 (69.14) | |||||
| Missing | 108 (2.56) | 72 (3.29) | 36 (1.77) | |||||
| TICS-10 | Low | 2252 (53.39) | 1388 (63.49) | 864 (42.52) | <0.001 | |||
| High | 1833 (43.46) | 703 (32.16) | 1130 (55.61) | |||||
| Missing | 133 (3.15) | 95 (4.35) | 38 (1.87) | |||||
| Word Recall | Low | 512 (12.14) | 394 (18.02) | 118 (5.81) | <0.001 | |||
| High | 3573 (84.71) | 1697 (77.63) | 1876 (92.32) | |||||
| Missing | 133 (3.15) | 95 (4.35) | 38 (1.87) | |||||
| Overall Cognition Score (N = 4147) | 10.96(4.39) | 9.71 (4.49) | 12.28 (3.88) | <0.001 | ||||
| (a) | |||||
| Outcome | Statistics | Unadjusted Model | Adjusted Model 1 | ||
| Drawing Ability | OR | 1.89 | 1.33 | ||
| 95% CI | (1.58, 2.27) | (1.07, 1.66) | |||
| p-value | <0.001 | 0.010 | |||
| Word Recall Ability | OR | 1.67 | 2.19 | ||
| 95% CI | (1.17, 2.40) | (1.14, 4.18) | |||
| p-value | 0.005 | 0.018 | |||
| TICS-10 | OR | 2.31 | 1.52 | ||
| 95% CI | (1.85, 2.89) | (1.15, 2.00) | |||
| p-value | <0.001 | 0.003 | |||
| Overall Cognition | Mean Diff. | 0.78 | 0.57 | ||
| 95% CI | (0.57, 0.99) | (0.32, 0.82) | |||
| p-value | <0.001 | <0.001 | |||
| (b) | |||||
| Outcome | Statistics | Adjusted Model A2 | Adjusted Model B3 | ||
| Lagged GS | Current GS | Lagged GS | Current GS | ||
| Drawing Ability | OR | 1.69 | 2.04 | 1.21 | 1.31 |
| 95% CI | 1.37, 2.09 | 1.63, 2.55 | 0.92, 1.60 | 0.99, 1.73 | |
| p-value | <0.001 | <0.001 | 0.162 | 0.063 | |
| Word Recall Ability | OR | 2.76 | 2.53 | 1.48 | 3.60 |
| 95% CI | 1.48, 5.06 | 1.35, 4.76 | 0.50, 4.34 | 1.17, 11.06 | |
| p-value | 0.001 | 0.004 | 0.477 | 0.025 | |
| TICS-10 | OR | 2.52 | 2.62 | 1.36 | 1.48 |
| 95% CI | 1.90, 3.34 | 2.05, 3.70 | 0.95, 1.94 | 1.02, 2.16 | |
| p-value | <0.001 | <0.001 | 0.089 | 0.039 | |
| Overall Cognition | Mean Diff. | 1.40 | 1.30 | 0.73 | 0.79 |
| 95% CI | 1.11, 1.69 | 1.02, 1.58 | 0.37, 1.10) | 0.44, 1.14 | |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | |
| (a) | |||||
| Outcome | Statistics | Unadjusted Model | Adjusted Model 1 | ||
| Drawing Ability | OR | 3.30 | 1.34 | ||
| 95% CI | 2.93, 3.71 | 1.12, 1.60 | |||
| p-value | <0.001 | 0.001 | |||
| Word Recall Ability | OR | 3.08 | 1.42 | ||
| 95% CI | 2.27, 4.19 | 0.78, 2.57 | |||
| p-value | <0.001 | 0.249 | |||
| TICS-10 | OR | 3.80 | 1.37 | ||
| 95% CI | 3.30, 4.37 | 1.11, 1.69 | |||
| p-value | <0.001 | 0.003 | |||
| Overall Cognition | Mean Diff. | 1.36 | 0.50 | ||
| 95% CI | 1.21, 1.52 | 0.27, 0.72 | |||
| p-value | <0.001 | <0.001 | |||
| (b) | |||||
| Outcome | Statistics | Adjusted Model A2 | Adjusted Model B3 | ||
| Lagged HGS | Current HGS | Lagged HGS | Current HGS | ||
| Drawing Ability | OR | 2.09 | 2.46 | 1.13 | 1.38 |
| 95% CI | 1.79, 2.43 | 2.10, 2.89 | 0.90, 1.41 | 1.10, 1.74 | |
| p-value | <0.001 | <0.001 | 0.306 | 0.005 | |
| Word Recall | OR | 2.19 | 2.61 | 2.15 | 1.31 |
| Ability | 95% CI | 1.31, 3.66 | 1.48, 4.61 | 0.52, 9.00 | 0.31, 5.46 |
| p-value | 0.003 | 0.001 | 0.293 | 0.715 | |
| TICS-10 | OR | 2.25 | 3.34 | 1.19 | 1.42 |
| 95% CI | 1.85, 2.72 | 2.76, 4.04 | 0.91, 1.55 | 1.09, 1.86 | |
| p-value | <0.001 | <0.001 | 0.212 | 0.010 | |
| Overall Cognition | Mean Diff. | 1.26 | 1.60 | 0.18 | 0.54 |
| 95% CI | 1.07, 1.46 | 1.49, 1.89 | −0.12, 0.49 | 0.24, 0.85 | |
| p-value | <0.001 | <0.001 | 0.242 | <0.001 | |
| Overall Cognitive Score (All Subjects) | Unadjusted Model | |||
| Slope (95% CI): Low GS | Slope (95% CI): High GS | Diff. in slope (High – Low GS) | p 1 | |
| −0.35 (−0.43, −0.28) | −0.18 (−0.25, −0.13) | 0.17 (0.07, 0.27) | <0.001 | |
| Adjusted Model 2 | ||||
| Slope (95% CI): Low GS | Slope (95% CI): High GS | Diff. in slope (High – Low GS) | p 1 | |
| −0.35 (−0.43, −0.28) | −0.19 (−0.25, −0.13) | 0.16 (0.06, 0.27) | <0.001 | |
| Overall Cognitive Score (Males Only) | Unadjusted Model | |||
| Slope (95% CI): Low GS | Slope (95% CI): High GS | Diff. in slope (High – Low GS) | p 1 | |
| −0.35 (−0.48, −0.23) | −0.17 (−0.25, −0.08) | 0.18 (0.03, 0.35) | 0.018 | |
| Adjusted Model2 | ||||
| Slope (95% CI): Low GS | Slope (95% CI): High GS | Diff. in slope (High – Low GS) | p 1 | |
| −0.36 (−0.49, −0.24) | −0.17 (−0.25, −0.08) | 0.19 (0.04, 0.35) | 0.015 | |
| Overall Cognitive Score (Females Only) | Unadjusted Model | |||
| Slope (95% CI): Low GS | Slope (95% CI): High GS | Diff. in slope (High – Low GS) | p 1 | |
| −0.34 (−0.44, −0.24) | −0.21 (−0.30, −0.12) | 0.13 (−0.01, 0.27) | 0.062 | |
| Adjusted Model2 | ||||
| Slope (95% CI): Low GS | Slope (95% CI): High GS | Diff. in slope (High – Low GS) | p 1 | |
| −0.35 (−0.44, −0.25) | −0.22 (−0.31, −0.13) | 0.13 (−0.01, 0.27) | 0.067 | |
| Overall Cognitive Score (All Subjects) | Unadjusted Model | |||
| Slope (95% CI): Low HGS | Slope (95% CI): High HGS | Diff. in slope (High – Low HGS) | p 1 | |
| −0.13 (−0.17, −0.09) | −0.01 (−0.06, 0.03) | 0.12 (0.05, 0.18) | <0.001 | |
| Adjusted Model 2 | ||||
| Slope (95% CI): Low HGS | Slope (95% CI): High HGS | Diff. in slope (High – Low HGS) | p 1 | |
| −0.16 (−0.20, −0.12) | −0.05 (−0.10, −0.01) | 0.11 (0.04, 0.17) | <0.001 | |
| Overall Cognitive Score (Males Only) | Unadjusted Model | |||
| Slope (95% CI): Low HGS | Slope (95% CI): High HGS | Diff. in slope (High – Low HGS) | p 1 | |
| −0.18 (−0.29, −0.08) | −0.06 (−0.11, −0.01) | 0.13 (0.01, 0.25) | 0.039 | |
| Adjusted Model2 | ||||
| Slope (95% CI): Low HGS | Slope (95% CI): High HGS | Diff. in slope (High – Low HGS) | p 1 | |
| −0.20 (−0.31, −0.10) | −0.09 (−0.14, 0.03) | 0.11 (−0.01, 0.24) | 0.059 | |
| Overall Cognitive Score (Females Only) | Unadjusted Model | |||
| Slope (95% CI): Low HGS | Slope (95% CI): High HGS | Diff. in slope (High – Low HGS) | p 1 | |
| −0.13 (−0.18, −0.09) | 0.09 (−0.01, 0.19) | 0.22 (0.11, 0.34) | <0.001 | |
| Adjusted Model2 | ||||
| Slope (95% CI): Low HGS | Slope (95% CI): High HGS | Diff. in slope (High – Low HGS) | p 1 | |
| −0.16 (−0.21, −0.11) | 0.07 (−0.03, 0.16) | 0.23 (0.11, 0.34) | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, N.; Yin, W.; Noon, R.I.; Alabdullatif, N. The Longitudinal Relationship Between Physical Functions and Cognitive Functions Among Middle-Aged and Older Adults in Primary Care. Int. J. Environ. Res. Public Health 2025, 22, 908. https://doi.org/10.3390/ijerph22060908
Hu N, Yin W, Noon RI, Alabdullatif N. The Longitudinal Relationship Between Physical Functions and Cognitive Functions Among Middle-Aged and Older Adults in Primary Care. International Journal of Environmental Research and Public Health. 2025; 22(6):908. https://doi.org/10.3390/ijerph22060908
Chicago/Turabian StyleHu, Nan, Wupeng Yin, Rabeya Illyas Noon, and Noof Alabdullatif. 2025. "The Longitudinal Relationship Between Physical Functions and Cognitive Functions Among Middle-Aged and Older Adults in Primary Care" International Journal of Environmental Research and Public Health 22, no. 6: 908. https://doi.org/10.3390/ijerph22060908
APA StyleHu, N., Yin, W., Noon, R. I., & Alabdullatif, N. (2025). The Longitudinal Relationship Between Physical Functions and Cognitive Functions Among Middle-Aged and Older Adults in Primary Care. International Journal of Environmental Research and Public Health, 22(6), 908. https://doi.org/10.3390/ijerph22060908