
Rural–Urban Disparities in Perinatal Smoking in the United States: Trends and Determinants


Abstract
1. Introduction
2. Methods
2.1. Study Design and Setting
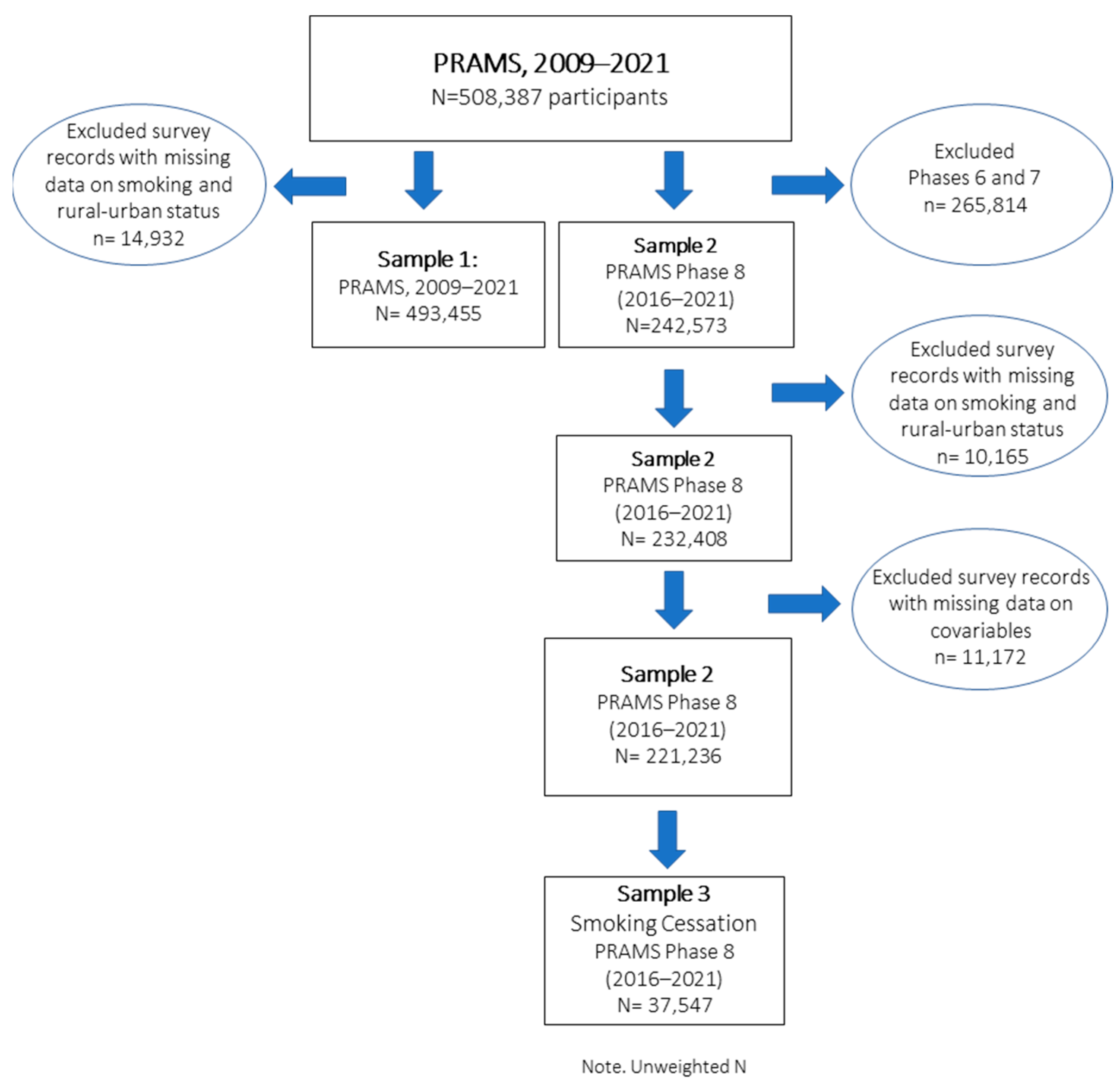
2.2. Sample
2.3. Measures
2.3.1. Cigarette Smoking and Cessation
2.3.2. Rural vs. Urban
2.3.3. Social Determinants of Health (SDOH) Factors
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
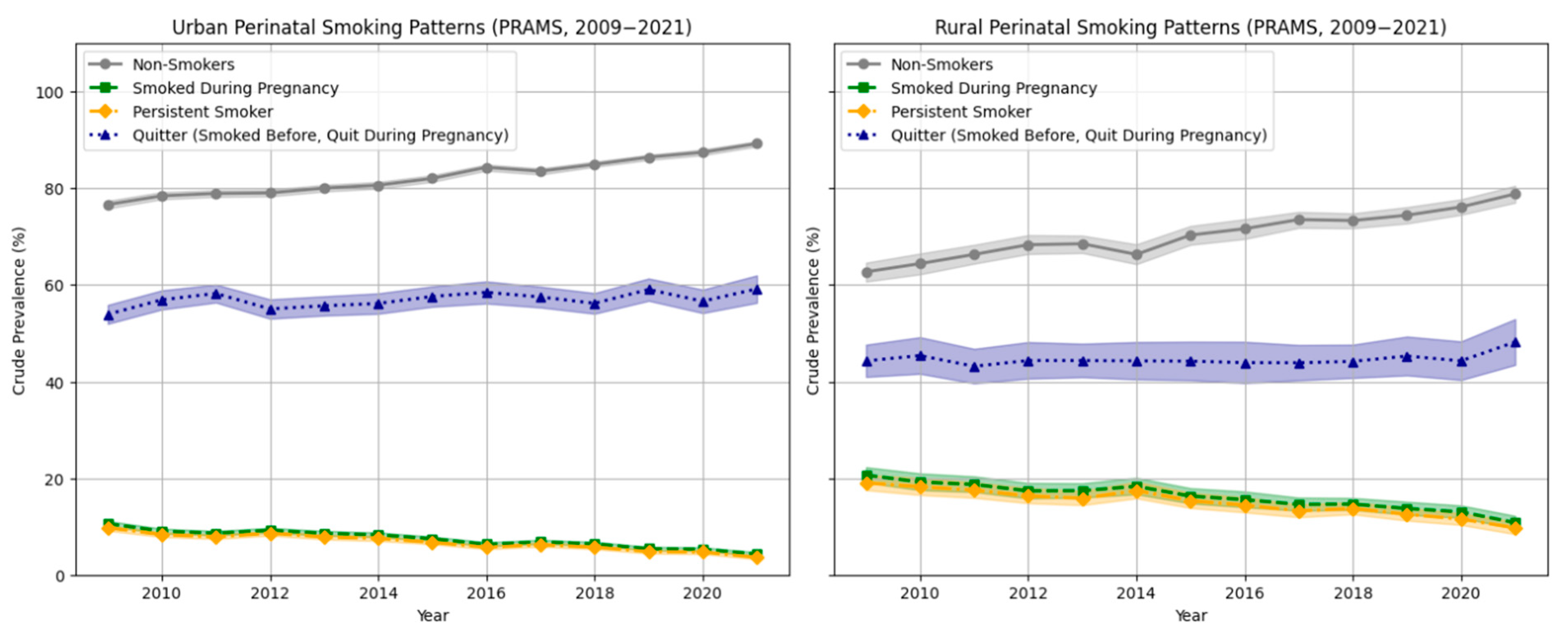
3.2. Trends in the Prevalence of Perinatal Smoking Behavior by Rural–Urban Residence
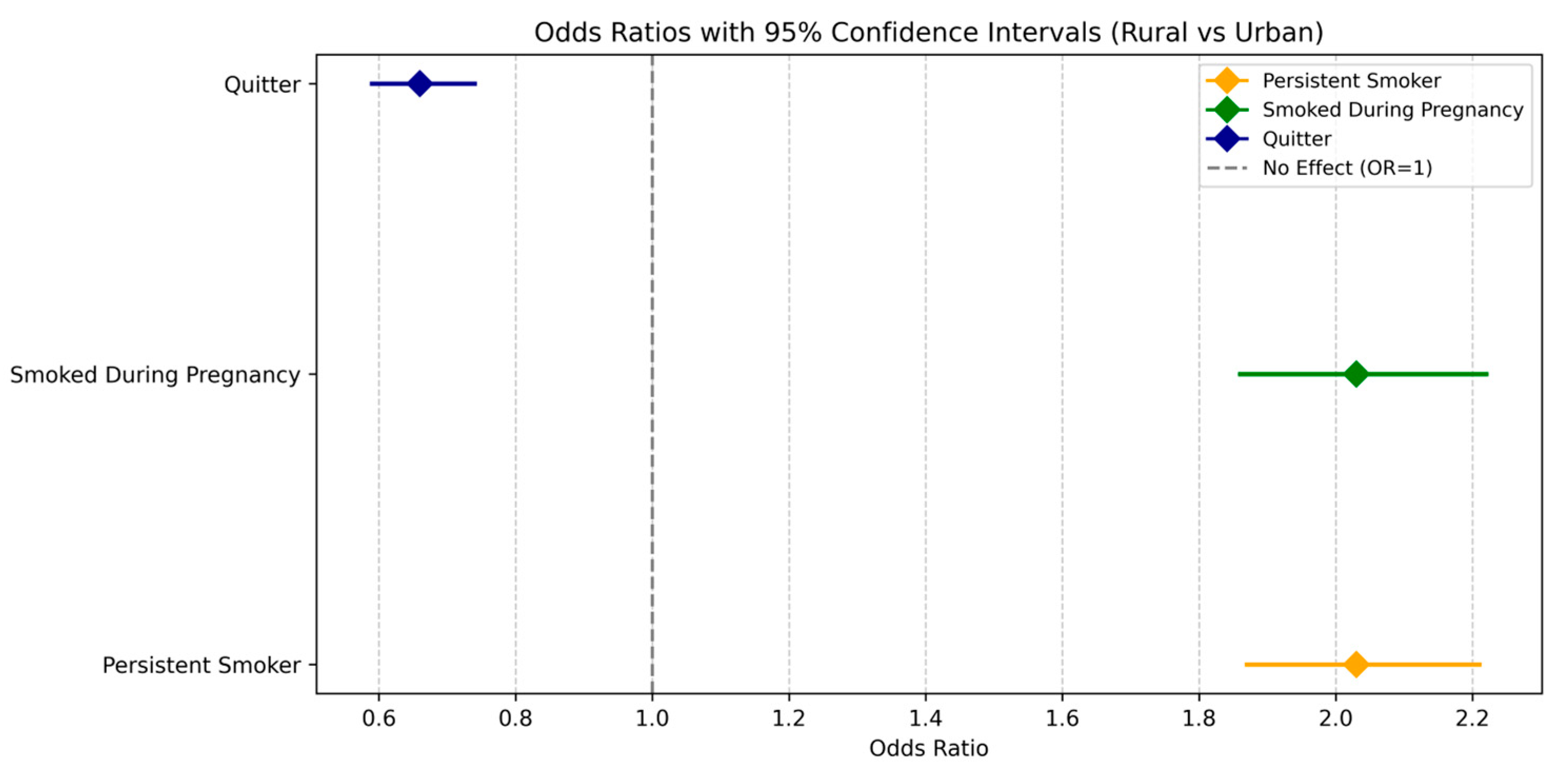
3.3. Explaining the Association Between Perinatal Smoking Behaviors and Rural–Urban Residence
4. Discussion
4.1. Limitations
4.2. Implications and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tarasi, B.; Cornuz, J.; Clair, C.; Baud, D. Cigarette smoking during pregnancy and adverse perinatal outcomes: A cross-sectional study over 10 years. BMC Public Health 2022, 22, 2403. [Google Scholar] [CrossRef] [PubMed]
- Avsar, T.S.; McLeod, H.; Jackson, L. Health outcomes of smoking during pregnancy and the postpartum period: An umbrella review. BMC Pregnancy Childbirth 2021, 21, 254. [Google Scholar] [CrossRef]
- Anderson, T.M.; Lavista Ferres, J.M.; Ren, S.Y.; Moon, R.Y.; Goldstein, R.D.; Ramirez, J.M.; Mitchell, E.A. Maternal Smoking Before and During Pregnancy and the Risk of Sudden Unexpected Infant Death. Pediatrics 2019, 143, e20183325. [Google Scholar] [CrossRef]
- Pereira, P.P.D.S.; Da Mata, F.A.F.; Figueiredo, A.C.G.; De Andrade, K.R.C.; Pereira, M.G. Maternal active smoking during pregnancy and low birth weight in the Americas: A systematic review and meta-analysis. Nicotine Tob. Res. 2017, 19, 497–505. [Google Scholar] [CrossRef]
- Puga, T.B.; Dai, H.D.; Wang, Y.; Theye, E. Maternal tobacco use during pregnancy and child neurocognitive development. JAMA Netw. Open 2024, 7, e2355952. [Google Scholar] [CrossRef] [PubMed]
- Ross, E.J.; Graham, D.L.; Money, K.M.; Stanwood, G.D. Developmental consequences of fetal exposure to drugs: What we know and what we still must learn. Neuropsychopharmacology 2015, 40, 61–87. [Google Scholar] [CrossRef]
- Can Özalp, E.; Yalçın, S.S. Is maternal cigarette or water pipe use associated with stopping breastfeeding? Evidence from the Jordan population and family health surveys 2012 and 2017–18. Int. Breastfeed J. 2021, 16, 43. [Google Scholar] [CrossRef]
- Lange, S.; Probst, C.; Rehm, J.; Popova, S. National, regional, and global prevalence of smoking during pregnancy in the general population: A systematic review and meta-analysis. Lancet Glob. Health 2018, 6, e769–e776. [Google Scholar] [CrossRef] [PubMed]
- Idris, B.I.; Giskes, K.; Borrell, C.; Benach, J.; Costa, G.; Federico, B.; Helakorpi, S.; Helmert, U.; Lahelma, E.; Moussa, K.M.; et al. Higher smoking prevalence in urban compared to non-urban areas: Time trends in six European countries. Health Place 2007, 13, 702–712. [Google Scholar] [CrossRef]
- Higgins, S.T.; Erath, T.; Chen, F.F. Examining U.S. disparities in smoking among rural versus urban women of reproductive age: 2002–2019. Prev. Med. 2024, 185, 108054. [Google Scholar] [CrossRef]
- Doogan, N.J.; Roberts, M.E.; Wewers, M.E.; Stanton, C.A.; Keith, D.R.; Gaalema, D.E.; Kurti, A.N.; Redner, R.; Cepeda-Benito, A.; Bunn, J.Y.; et al. A growing geographic disparity: Rural and urban cigarette smoking trends in the United States. Prev. Med. 2017, 104, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.A.; Weinberger, A.H.; Eggers, E.M.; Parker, E.S.; Villanti, A.C. Trends in Rural and Urban Cigarette Smoking Quit Ratios in the US From 2010 to 2020. JAMA Netw. Open 2022, 5, e2225326. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Kok, G. The theory of planned behavior: A review of its applications to health-related behaviors. Am. J. Health Promot. 1996, 11, 87–98. [Google Scholar] [CrossRef]
- Ntoumanis, N.; Ng, J.Y.Y.; Prestwich, A.; Quested, E.; Hancox, J.E.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Lonsdale, C.; Williams, G.C. A meta-analysis of self-determination theory-informed intervention studies in the health domain: Effects on motivation, health behavior, physical, and psychological health. Health Psychol. Rev. 2021, 15, 214–244. [Google Scholar] [CrossRef] [PubMed]
- Solar, O.; Irwin, A. A Conceptual Framework for Action on the Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Silveira, M.F.; Matijasevich, A.; Menezes, A.M.B.; Horta, B.L.; Santos, I.S.; Barros, A.J.D.; Barros, F.C.; Victora, C.G. Secular trends in smoking during pregnancy according to income and ethnic group: Four population-based perinatal surveys in a Brazilian city. Br. Med. J. Open 2016, 6, e010127. [Google Scholar] [CrossRef]
- Talbot, J.A.; Williamson, M.E.; Pearson, K.B.; Lenardson, J.D.; Ziller, E.C.; Jimenez, F.; Paluso, N.; Munk, L.; Janis, J. Advancing Tobacco Prevention and Control in Rural America; National Network of Public Health Institutes: Washington, DC, USA, 2019. [Google Scholar]
- Leider, J.P.; Meit, M.; McCullough, J.M.; Resnick, B.; Dekker, D.; Alfonso, Y.N.; Bishai, D. The State of Rural Public Health: Enduring Needs in a New Decade. Am. J. Health 2020, 110, 1283–1290. [Google Scholar] [CrossRef]
- Cheng, D.; Salimi, S.; Terplan, M.; Chisolm, M.S. Intimate partner violence and maternal cigarette smoking before and during pregnancy. Obstet. Gynaecol. 2015, 125, 356–362. [Google Scholar] [CrossRef]
- Hutcheson, T.D.; Greiner, K.A.; Ellerbeck, E.F.; Jeffries, S.K.; Mussulman, L.M.; Casey, G.N. Understanding smoking cessation in rural communities. J. Rural. Health. 2008, 24, 116–124. [Google Scholar] [CrossRef]
- Rural Health Information Hub. Substance Use and Misuse in Rural Areas; Rural Health Information Hub: Grand Forks, ND, USA. Available online: https://www.ruralhealthinfo.org/topics/substance-use (accessed on 25 January 2024).
- Higgins, S.T. Behavior change, health, and health disparities 2024: Smoking and other tobacco use among women and girls. Prev. Med. 2024, 188, 108155. [Google Scholar] [CrossRef]
- Shulman, H.B.; D’Angelo, D.V.; Harrison, L.; Smith, R.A.; Warner, L. The Pregnancy Risk Assessment Monitoring System (PRAMS): Overview of Design and Methodology. Am. J. Public Health 2018, 108, 1305–1313. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. NCHS Urban-Rural Classification Scheme for Counties; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2023. [Google Scholar]
- Matthews, K.A.; Croft, J.B.; Liu, Y.; Lu, H.; Kanny, D.; Wheaton, A.G.; Cunningham, T.J.; Khan, L.K.; Caraballo, R.S.; Holt, J.B.; et al. Health-Related Behaviors by Urban-Rural County Classification—United States, 2013. MMWR Morb. Mortal. Wkly. Rep. Surveill. Summ. 2017, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Meit, M.; Knudson, A.; Gilbert, T.; Yu, A.T.-C.; Tanenbaum, E.; Ormson, E.; Popat, S. The 2014 Update of the Rural-Urban Chartbook; Rural Health Reform Policy Research Center: Bethesda, MD, USA, 2014; Volume 10. [Google Scholar]
- Preventing Tobacco Addiction Foundation. Tobacco Twenty-One: Tobacco 21 Grade Cards. 2025. Available online: https://tobacco21.org/state-grades/ (accessed on 15 May 2025).
- IBM Corp. IBM SPSS Statistics for Windows, Version 29.0; IBM Corp: Armonk, NY, USA, 2022. [Google Scholar]
- Office of Disease Prevention and Health Promotion. Healthy People 2030. Available online: https://odphp.health.gov/healthypeople (accessed on 20 March 2024).
- Nighbor, T.D.; Doogan, N.J.; Roberts, M.E.; Cepeda-Benito, A.; Kurti, A.N.; Priest, J.S.; Johnson, H.K.; Lopez, A.A.; Stanton, C.A.; Gaalema, D.E.; et al. Smoking prevalence and trends among a U.S. national sample of women of reproductive age in rural versus urban settings. PLoS ONE 2018, 13, e0207818. [Google Scholar] [CrossRef] [PubMed]
- Hartley, D. Rural health disparities, population health, and rural culture. Am. J. Public Health 2004, 94, 1675–1678. [Google Scholar] [CrossRef]
- Zaganjor, I.; Kramer, R.D.; Kofie, J.N.; Sawdey, M.D.; Cullen, K.A. Trends in Smoking Before, During, and After Pregnancy in the United States from 2000 to 2020: Pregnancy Risk Assessment Monitoring System. J. Women’s Health 2024, 33, 283–293. [Google Scholar] [CrossRef]
- Stillman, F.A.; Tanenbaum, E.; Wewers, M.E.; Chelluri, D.; Mumford, E.A.; Groesbeck, K.; Doogan, N.; Roberts, M. Variations in support for secondhand smoke restrictions across diverse rural regions of the United States. Prev. Med. 2018, 116, 157–165. [Google Scholar] [CrossRef]
- Salmasi, G.; Grady, R.; Jones, J.; McDonald, S.D.; Knowledge Synthesis Group. Environmental tobacco smoke exposure and perinatal outcomes: A systematic review and meta-analyses. Acta Obstet. Et Gynecol. Scand. 2010, 89, 423–441. [Google Scholar] [CrossRef]
- Harmer, C.; Memon, A. Factors associated with smoking relapse in the postpartum period: An analysis of the child health surveillance system data in Southeast England. Nicotine Tob. Res. 2013, 15, 904–909. [Google Scholar] [CrossRef]
- Shoff, C.; Yang, T.C. Understanding maternal smoking during pregnancy: Does residential context matter? Soc. Sci. Med. 2013, 78, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Buettner-Schmidt, K.; Miller, D.R.; Maack, B. Disparities in Rural Tobacco Use, Smoke-Free Policies, and Tobacco Taxes. West. J. Nurs. Res. 2019, 41, 1184–1202. [Google Scholar] [CrossRef]
- Mac McCullough, J.; Leider, J.P.; Riley, W.J. Local fiscal allocation for public health departments. Am. J. Prev. Med. 2015, 49, 921–929. [Google Scholar] [CrossRef]
- Campbell, K.A.; Cooper, S.; Fahy, S.J.; Bowker, K.; Leonardi-Bee, J.; McEwen, A.; Whitemore, R.; Coleman, T. ‘Opt-out’ referrals after identifying pregnant smokers using exhaled air carbon monoxide: Impact on engagement with smoking cessation support. Tob. Control 2017, 26, 300–306. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Smoking Cessation a Report of the Surgeon General. 2020. Available online: https://www.hhs.gov/sites/default/files/2020-cessation-sgr-full-report.pdf (accessed on 21 June 2024).
- US Preventive Services Task Force. Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Persons: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Florescu, A.; Ferrence, R.; Einarson, T.; Selby, P.; Soldin, O.; Koren, G. Methods for quantification of exposure to cigarette smoking and environmental tobacco smoke: Focus on developmental toxicology. Ther. Drug Monit. 2009, 31, 14–30. [Google Scholar] [CrossRef]
- Hall, S.A.; Kaufman, J.S.; Ricketts, T.C. Defining urban and rural areas in US epidemiologic studies. J. Urban Health 2006, 83, 162–175. [Google Scholar] [CrossRef]
- Roberts, M.E.; Doogan, N.J.; Tanenbaum, E.; Stillman, F.A.; Mumford, E.A.; Chelluri, D.; Wewers, M.E. How should we define “rural” when investigating rural tobacco use in the United States? Subst. Abus. 2021, 42, 788–795. [Google Scholar] [CrossRef] [PubMed]
- Fouladi, N.; Tchangalova, N.; Ajayi, D.; Millwee, E.; Lovett, C.; Del Sordi, A.; Liggett, S.; De Silva, M.; Bonilla, L.; Nkwonta, A.; et al. COVID-19 Public Health Measures and Patient and Public Involvement in Health and Social Care Research: An Umbrella Review. Int. J. Environ. Res. Public Health 2023, 20, 4887. [Google Scholar] [CrossRef]
- Siddiqi, K.; Mdege, N. A global perspective on smoking during pregnancy. Lancet Glob. Health 2018, 6, e708–e709. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Unweighted N | Overall % a (95% CI) | Urban % a (95% CI) | Rural % a (95% CI) |
|---|---|---|---|---|---|
| Smoking status | |||||
| Before pregnancy | Yes | 39,441 | 15.5 (15.2–15.7) | 13.7 (13.5–14.0) | 24.9 (24.2–25.6) |
| During pregnancy | Yes | 19,280 | 7.1 (6.9–7.3) | 5.9 (5.7–6.0) | 13.8 (13.2–14.4) |
| After pregnancy | Yes | 26,358 | 10.0 (9.8–10.2) | 8.6 (8.4–8.8) | 17.6 (17.0–18.3) |
| Persistent | Yes | 17,367 | 6.4 (6.2–6.5) | 5.2 (5.1–5.4) | 12.6 (12.1–13.1) |
| Cessation | Yes | 20,326 | 54.6 (53.7–55.4) | 57.8 (56.8–58.7) | 44.9 (43.2–46.5) |
| Maternal age (yrs.) | <20 | 10,330 | 4.2 (4.1–4.3) | 3.8 (3.7–4.0) | 6.3 (6.0–6.7) |
| 20–24 | 41,169 | 18.0 (17.8–18.3) | 16.6 (16.4–16.9) | 25.7 (25.0–26.4) | |
| 25–29 | 66,363 | 28.7 (28.4–29.0) | 28.0 (27.7–28.4) | 32.6 (31.9–33.4) | |
| 30–34 | 69,641 | 30.0 (29.8–30.3) | 31.3 (30.9–31.6) | 23.3 (22.7–24.0) | |
| ≥35 | 44,896 | 19.0 (18.7–19.2) | 20.3 (20.0–20.5) | 12.1 (11.6–12.5) | |
| Missing | 9 | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | |
| Race/Ethnicity | White | 104,681 | 56.7 (56.4–57.0) | 53.6 (53.3–53.9) | 73.9 (73.2–74.5) |
| Black | 41,396 | 15.0 (14.8–15.2) | 16.2 (16.0–16.5) | 8.1 (7.6–8.5) | |
| Hispanic | 40,954 | 18.0 (17.8–18.2) | 19.4 (19.1–19.7) | 10.3 (9.9–10.8) | |
| Other b | 39,179 | 9.4 (9.3–9.6) | 10.0 (9.8–10.2) | 6.5 (6.1–6.7) | |
| Missing | 6198 | 0.9 (0.8–0.9) | 0.8 (0.7–0.8) | 1.3 (1.3–1.4) | |
| Marital status | Married | 139,066 | 61.7 (61.4–62.0) | 62.5 (62.2–62.8) | 57.2 (56.4–58.0) |
| other | 93,156 | 38.3 (38.0–38.6) | 37.4 (37.1–37.8) | 42.7 (41.9–43.5) | |
| Missing | 186 | 0.1 (0.0–0.1) | 0.0 (0.0–0.1) | 0.1 (0.1–0.2) | |
| Education (yrs) | <12 | 27,944 | 11.6 (11.4–11.8) | 11.1 (10.9–11.3) | 14.1 (13.6–14.7) |
| 12 | 55,825 | 24.6 (24.3–24.9) | 23.4 (23.0–23.7) | 31.6 (30.9–32.4) | |
| >12 | 146,638 | 63.0 (62.7–63.3) | 64.7 (64.3–65.0) | 53.8 (53.0–54.6) | |
| Missing | 2001 | 0.8 (0.8–0.9) | 0.9 (0.8–0.9) | 0.5 (0.4–0.6) | |
| Household income (US$) | ≤$24,000 | 70,727 | 28.4 (28.1–28.7) | 27.0 (26.7–27.4) | 35.7 (35.0–36.5) |
| $24,001–60,000 | 60,649 | 25.6 (25.3–25.9) | 24.6 (24.3–24.9) | 31.0 (30.3–31.7) | |
| >$60,001 | 79,183 | 37.0 (36.6–37.2) | 39.0 (38.7–39.4) | 25.4 (24.7–26.0) | |
| Missing | 21,849 | 9.1 (8.9–9.3) | 9.3 (9.1–9.5) | 7.9 (7.5–8.4) | |
| Received WIC | Yes | 83,337 | 33.6 (33.3–33.9) | 31.9 (31.5–32.2) | 43.4 (42.6–44.1) |
| No | 145,727 | 65.0 (64.7–65.3) | 66.7 (66.4–67.1) | 55.7 (54.9–56.5) | |
| Missing | 3344 | 1.3 (1.3–1.3) | 1.4 (1.3–1.5) | 0.9 (0.8–1.1) | |
| Parity | 0 | 90,641 | 38.8 (38.5–39.2) | 39.4 (39.0–39.7) | 35.9 (35.2–36.7) |
| 1 | 72,802 | 32.8 (32.5–33.1) | 33.0 (32.7–33.3) | 31.5 (30.8–32.2) | |
| 2 | 38,356 | 16.5 (16.2–16.7) | 16.1 (15.9–16.4) | 18.1 (17.5–18.7) | |
| ≥3 | 30,173 | 11.8 (11.5–12.0) | 11.3 (11.1–11.5) | 14.3 (13.8–14.9) | |
| Missing | 436 | 0.2 (0.2–0.2) | 0.2 (0.2–0.2) | 0.1 (0.1–0.2) | |
| Pregnancy intention | Planned | 99,561 | 44.9 (44.4–44.4) | 44.4 (44.1–44.8) | 42.1 (41.4–42.9) |
| Mistimed | 76,229 | 33.0 (32.7–33.4) | 33.2 (32.9–33.6) | 32.1 (31.3–32.8) | |
| Unsure | 52,934 | 21.3 (21.0–21.6) | 20.8 (20.5–21.0) | 24.4 (23.7–25.1) | |
| Missing | 3684 | 1.6 (1.5–1.7) | 1.6 (1.5–1.7) | 1.4 (1.3–1.6) | |
| Prenatal depression | Yes | 160,357 | 85.2 (85.0–85.4) | 86.0 (85.7–86.2) | 80.8 (80.2–81.5) |
| No | 22,997 | 13.8 (13.6–14.0) | 13.0 (12.8–13.2) | 18.3 (17.7–19.0) | |
| Missing | 2437 | 1.0 (0.9–1.1) | 1.0 (1.0–1.1) | 0.8 (0.7–1.0) | |
| Perinatal stressors c | No | 222,777 | 96.4 (96.3–96.5) | 96.7 (96.5–96.8) | 95.0 (94.6–95.3) |
| Yes | 9631 | 3.6 (3.5–3.7) | 3.3 (3.2–3.5) | 5.0 (4.7–5.4) | |
| Region | Midwest | 59,428 | 25.1 (25.0–25.2) | 23.3 (23.2–23.4) | 35.1 (34.5–35.8) |
| Northeast | 58,871 | 26.2 (26.2–26.3) | 28.9 (28.7–29.0) | 11.8 (11.3–12.4) | |
| South | 55,747 | 32.8 (32.7–32.9) | 31.6 (31.4–31.7) | 36.3 (35.6–37.0) | |
| West | 58,362 | 16.3 (16.3–16.4) | 16.3 (16.2–16.3) | 16.8 (16.4–17.1) | |
| Tobacco 21 Grade | A | 39,168 | 18.9 (18.8–19.0) | 20.8 (20.7–20.9) | 8.5 (8.1–8.9) |
| B | 26,218 | 10.1 (10.1–10.2) | 10.2 (10.1–10.3) | 9.5 (9.0–9.9) | |
| C | 75,271 | 39.0 (38.9–39.1) | 39.9 (39.8–40.1) | 34.0 (33.3–34.7) | |
| F | 65,510 | 21.5 (21.4–21.5) | 19.7 (19.6–19.8) | 31.3 (30.7–31.9) | |
| No policy | 26,241 | 10.5 (10.4–10.5) | 9.3 (9.3–9.4) | 16.7 (16.3–17.2) |
| Variable | Category | Smoking Persistence (N = 221,236) | Smoking Cessation (N = 37,547) | ||
|---|---|---|---|---|---|
| Unadjusted OR (95% CI) | aOR (95% CI) | Unadjusted OR (95% CI) | aOR (95% CI) | ||
| Residency | Rural | 2.61 (2.46–2.77) | 1.45 (1.35–1.56) | 0.59 (0.55–0.64) | 0.74 (0.67–0.80) |
| Urban | ref | ref | ref | ref | |
| Maternal age | <20 | 1.56 (1.35–1.81) | 0.30 (0.25–0.36) | 1.34 (1.13–1.60) | 0.32 (0.27–0.39) |
| 20–24 | 1.95 (1.78–2.13) | 0.59 (0.53–0.67) | 1.08 (0.97–1.21) | 0.64 (0.58–0.72) | |
| 25–29 | 1.70 (1.57–1.85) | 0.91 (0.83–1.01) | 0.92 (0.83–1.02) | 0.99 (0.90–1.08) | |
| 30–34 | 1.15 (1.05–1.25) | 1.02 (0.92–1.13) | 1.02 (0.91–1.14) | 1.08 (0.98–1.19) | |
| ≥35 | ref | ref | ref | ref | |
| Race/ Ethnicity | White | 1.94 (1.77–2.11) | 2.45 (2.21–2.71) | 0.84 (0.75–0.93) | 2.38 (2.16–2.63) |
| Black | 1.26 (1.13–1.40) | 0.58 (0.52–0.66) | 0.96 (0.84–1.10) | 0.57 (0.50–0.64) | |
| Hispanic | 0.41 (0.35–0.47) | 0.22 (0.18–0.25) | 1.89 (1.61–2.20) | 0.24 (0.21–0.28) | |
| Missing | 1.35 (1.08–1.67) | 1.25 (0.97–1.61) | 0.96 (0.71–1.30) | 1.11 (0.88–1.42) | |
| Other | ref | ref | ref | ref | |
| Marital status | Married | ref | ref | ref | ref |
| Other | 4.71 (4.44–4.99) | 2.73 (2.53–2.95) | 2.74 (2.55–2.95) | 2.74 (2.55–2.95) | |
| Education (yrs) | <12 | 4.23 (3.93–4.54) | 2.97 (2.69–3.27) | 0.35 (0.31–0.38) | 2.92 (2.66–3.20) |
| 12 | 3.42 (3.22–3.64) | 1.81 (1.68–1.96) | 0.55 (0.51–0.60) | 1.84 (1.71–1.97) | |
| >12 | ref | ref | ref | ref | |
| Household income (US$) | ≤$24,000 | 12.87 (11.63–14.24) | 5.38 (4.70–6.16) | 0.21 (0.19–0.24) | 0.32 (0.27–0.39) |
| $24,001–$60,000 | 4.90 (4.39–5.46) | 2.94 (2.60–3.33) | 0.39 (0.35–0.44) | 0.49 (0.43–0.57) | |
| Missing | 4.35 (3.79–4.98) | 2.90 (2.46–3.41) | 0.30 (0.26–0.35) | 0.40 (0.33–0.49) | |
| >$60,001 | ref | ref | ref | ref | |
| Received WIC | Yes | 3.08 (2.92–3.26) | 1.30 (1.21–1.39) | 0.55 (0.51–0.58) | 0.82 (0.76–0.89) |
| No | ref | ref | ref | ref | |
| Zero | ref | ref | ref | ||
| Parity | 1 | 1.39 (1.30–1.49) | 1.43 (1.32–1.55) | 0.61 (0.56–0.66) | 0.65 (0.59–0.71) |
| 2 | 2.00 (1.85–2.16) | 1.66 (1.51–1.83) | 0.45 (0.41–0.50) | 0.56 (0.50–0.62) | |
| 3+ | 2.86 (2.65–3.10) | 1.91 (1.72–2.12) | 0.28 (0.26–0.32) | 0.40 (0.35–0.45) | |
| Pregnancy intention | Planned | ref | ref | ref | ref |
| Mistimed | 1.49 (1.39–1.60) | 1.21 (1.11–1.30) | 0.88 (0.81–0.96) | 0.90 (0.82–0.99) | |
| Unsure | 3.58 (3.36–3.83) | 1.75 (1.62–1.89) | 0.55 (0.51–0.60) | 0.75 (0.68–0.83) | |
| Prenatal Depression | Yes | 5.13 (4.70–5.60) | 2.08 (1.94–2.23) | 0.56 (0.52–0.60) | 0.71 (0.66–0.78) |
| No | ref | ref | ref | ref | |
| Perinatal stressors | Yes | 2.02 (1.81–2.26) | 2.02 (1.81–2.26) | 0.52 (0.46–0.58) | 0.69 (0.61–0.79) |
| No | ref | ref | ref | ref | |
| Region | Midwest | 1.58 (1.47–1.69) | 1.25 (1.15–1.36) | 0.76 (0.69–0.82) | 0.83 (0.75–0.92) |
| Northeast | 0.98 (0.90–1.07) | 1.19 (1.07–1.33) | 0.97 (0.88–1.07) | 0.86 (0.76–0.98) | |
| South | 1.23 (1.15–1.33) | 1.07 (0.98–1.17) | 0.89 (0.81–0.97) | 0.99 (0.89–1.11) | |
| West | ref | ref | ref | ref | |
| Tobacco 21 Grade | A | ref | ref | ref | ref |
| B | 1.65 (1.48–1.85) | 1.25 (1.11–1.39) | 0.82 (0.71–0.94) | 0.93 (0.79–1.10) | |
| C | 1.51 (1.38–1.65) | 1.24 (1.09–1.41) | 0.77 (0.69–0.86) | 0.87 (0.76–0.99) | |
| F | 1.79 (1.63–1.97) | 1.41 (1.23–1.62) | 0.74 (0.66–0.83) | 0.92 (0.79–1.06) | |
| No policy | 2.21 (1.99–2.44) | 1.25 (1.11–1.39) | 0.61 (0.54–0.69) | 0.79 (0.67–0.92) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Da Rosa, P.; Richter, M. Rural–Urban Disparities in Perinatal Smoking in the United States: Trends and Determinants. Int. J. Environ. Res. Public Health 2025, 22, 895. https://doi.org/10.3390/ijerph22060895
Da Rosa P, Richter M. Rural–Urban Disparities in Perinatal Smoking in the United States: Trends and Determinants. International Journal of Environmental Research and Public Health. 2025; 22(6):895. https://doi.org/10.3390/ijerph22060895
Chicago/Turabian StyleDa Rosa, Patricia, and Matthias Richter. 2025. "Rural–Urban Disparities in Perinatal Smoking in the United States: Trends and Determinants" International Journal of Environmental Research and Public Health 22, no. 6: 895. https://doi.org/10.3390/ijerph22060895
APA StyleDa Rosa, P., & Richter, M. (2025). Rural–Urban Disparities in Perinatal Smoking in the United States: Trends and Determinants. International Journal of Environmental Research and Public Health, 22(6), 895. https://doi.org/10.3390/ijerph22060895