


Changes in Pain-Related Psychological Distress After Surgery in Patients with Musculoskeletal Injury

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Cohort
2.2. Study Tools
2.3. Statistical Analysis
3. Results
Exploratory Analysis of Those with High Preoperative Distress
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnson, L.L.; Pittsley, A.; Becker, R.; De Young, A. A novel quantitative pain assessment instrument that provides means of comparing patient’s pain magnitude with a measurement of their pain tolerance. J. Clin. Med. Res. 2015, 7, 781. [Google Scholar] [CrossRef] [PubMed]
- Zieliński, J.; Morawska-Kochman, M.; Zatoński, T. Pain assessment and management in children in the postoperative period: A review of the most commonly used postoperative pain assessment tools, new diagnostic methods and the latest guidelines for postoperative pain therapy in children. Adv. Clin. Exp. Med. 2020, 29, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Furie, K.; Park, A.L.; Wong, S.E. Mental health and involuntary retirement from sports post-musculoskeletal injury in adult athletes: A systematic review. Curr. Rev. Musculoskelet. Med. 2023, 16, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Reese, L.M.S.; Pittsinger, R.; Yang, J. Effectiveness of psychological intervention following sport injury. J. Sport Health Sci. 2012, 1, 71–79. [Google Scholar] [CrossRef]
- Weng Hong, C.; Ajit Singh, V.; Amar Singh, A.K. Psychological disorders in patients with orthopaedic oncological diseases and their coping strategies. J. Orthop. Surg. 2022, 30, 10225536221093431. [Google Scholar] [CrossRef]
- Kirven, J.C.; Everhart, J.S.; DiBartola, A.C.; Jones, J.; Flanigan, D.C.; Harrison, R. Interventional efforts to reduce psychological distress after orthopedic trauma: A systematic review. HSS J.® 2020, 16, 250–260. [Google Scholar] [CrossRef]
- Lentz, T.A.; Beneciuk, J.M.; Bialosky, J.E.; Zeppieri, G., Jr.; Dai, Y.; Wu, S.S.; George, S.Z. Development of a yellow flag assessment tool for orthopaedic physical therapists: Results from the Optimal Screening for Prediction of Referral and Outcome (OSPRO) cohort. J. Orthop. Sports Phys. Ther. 2016, 46, 327–343. [Google Scholar] [CrossRef]
- George, S.Z.; Beneciuk, J.M.; Lentz, T.A.; Wu, S.S.; Dai, Y.; Bialosky, J.E.; Zeppieri, G., Jr. Optimal screening for prediction of referral and outcome (OSPRO) for musculoskeletal pain conditions: Results from the validation cohort. J. Orthop. Sports Phys. Ther. 2018, 48, 460–475. [Google Scholar] [CrossRef]
- Cabell, G.H.; Kwon, N.F.; Sutton, K.F.; Lentz, T.A.; Lewis, B.D.; Olson, S.; Mather, R.C., III. Pain-Associated Psychological Distress Is of High Prevalence in Patients With Hip Pain: Characterizing Psychological Distress and Phenotypes. Arthrosc. Sports Med. Rehabil. 2024, 6, 100846. [Google Scholar] [CrossRef]
- Okafor, C.; Levin, J.M.; Boadi, P.; Cook, C.; George, S.; Klifto, C.; Anakwenze, O. Pain associated psychological distress is more strongly associated with shoulder pain and function than tear severity in patients undergoing rotator cuff repair. JSES Int. 2023, 7, 544–549. [Google Scholar] [CrossRef]
- Levin, J.M.; Baker, R.; Goltz, D.E.; Wickman, J.; Lentz, T.A.; Cook, C.; George, S.Z.; Klifto, C.S.; Anakwenze, O.A. Heterogeneity of pain-related psychological distress in patients seeking care for shoulder pathology. J. Shoulder Elb. Surg. 2022, 31, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Butera, K.A.; George, S.Z.; Lentz, T.A. Psychometric evaluation of the optimal screening for prediction of referral and outcome yellow flag (OSPRO-YF) tool: Factor structure, reliability, and validity. J. Pain 2020, 21, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Khatib, Y.; Jenkin, D.; Naylor, J.M.; Harris, I.A. Psychological Traits in Patients Waiting for Total Knee Arthroplasty. A Cross-sectional Study. J. Arthroplast. 2016, 31, 1661–1666. [Google Scholar] [CrossRef] [PubMed]
- Mariaux, F.; Elfering, A.; Fekete, T.F.; Porchet, F.; Haschtmann, D.; Reitmeir, R.; Loibl, M.; Jeszenszky, D.; Kleinstuck, F.S.; Mannion, A.F. The use of the Core Yellow Flags Index for the assessment of psychosocial distress in patients undergoing surgery of the cervical spine. Eur. Spine J. 2024, 33, 2269–2276. [Google Scholar] [CrossRef]
- Megee, F.; Gough, K.; Frowen, J.; Dixon, B.; Magarey, M.; Wiesenfeld, D.; Ramakrishnan, A. Predictors of distress associated with altered appearance and function in people treated surgically for oral cancers: A cross-sectional study. Int. J. Oral Maxillofac. Surg. 2023, 52, 923–930. [Google Scholar] [CrossRef]
- Trief, P.M.; Grant, W.; Fredrickson, B. A prospective study of psychological predictors of lumbar surgery outcome. Spine 2000, 25, 2616–2621. [Google Scholar] [CrossRef]
- Aaron, R.V.; Rassu, F.S.; Wegener, S.T.; Holley, A.L.; Castillo, R.C.; Osgood, G.M.; Fisher, E. Psychological treatments for the management of pain after musculoskeletal injury: A systematic review and meta-analysis. Pain 2024, 165, 3–17. [Google Scholar] [CrossRef]
- Aabedi, A.; Wang, V.; Fraix, M.P.; Agrawal, D.K. Psychological Treatment in the Management of Pain following Musculoskeletal Injury. J. Orthop. Sports Med. 2025, 7, 162–168. [Google Scholar] [CrossRef]
- Leech, J.B.; MacPherson, K.L.; Klopper, M.; Shumway, J.; Salvatori, R.T.; Rhon, D.I.; Young, J.L. The relationships between pain-associated psychological distress, pain intensity, patient expectations, and physical function in individuals with musculoskeletal pain: A retrospective cohort study. PM R 2023, 15, 1371–1381. [Google Scholar] [CrossRef]
- Morriss, N.J.; Kim, B.I.; Poehlein, E.; Park, C.N.; Lentz, T.A.; Green, C.L.; Lau, B.C. Association between preoperative multidimensional psychological distress and physical function after surgery for sports-related injury. Orthop. J. Sports Med. 2023, 11, 23259671231163854. [Google Scholar] [CrossRef]
- Retzky, J.S.; Baker, M.; Hannan, C.V.; Srikumaran, U. Single Assessment Numeric Evaluation scores correlate positively with American Shoulder and Elbow Surgeons scores postoperatively in patients undergoing rotator cuff repair. J. Shoulder Elb. Surg. 2020, 29, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, M.; Boffa, A.; Pignotti, E.; Andriolo, L.; Zaffagnini, S.; Filardo, G. The minimal clinically important difference changes greatly based on the different calculation methods. Am. J. Sports Med. 2023, 51, 1067–1073. [Google Scholar] [CrossRef] [PubMed]
- Filardo, G.; Roffi, A.; Merli, G.; Marcacci, T.; Ceroni, F.B.; Raboni, D.; Bortolotti, B.; De Pasqual, L.; Marcacci, M. Patient kinesiophobia affects both recovery time and final outcome after total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3322–3328. [Google Scholar] [CrossRef]
- Suer, M.; Philips, N.; Kliethermes, S.; Scerpella, T.; Sehgal, N. Baseline kinesiophobia and pain catastrophizing scores predict prolonged postoperative shoulder pain. Pain Physician 2022, 25, E285. [Google Scholar]
- Haugen, E. Athlete mental health & psychological impact of sport injury. Oper. Tech. Sports Med. 2022, 30, 150898. [Google Scholar]
- Hartigan, E.H.; Lynch, A.D.; Logerstedt, D.S.; Chmielewski, T.L.; Snyder-Mackler, L. Kinesiophobia after anterior cruciate ligament rupture and reconstruction: Noncopers versus potential copers. J. Orthop. Sports Phys. Ther. 2013, 43, 821–832. [Google Scholar] [CrossRef]
- Dismore, L.; Van Wersch, A.; Murty, A.N.; Swainston, K. A qualitative study with orthopaedic surgeons on pain catastrophizing and surgical outcomes: Shifting from a medical towards a biopsychosocial model of surgery. Br. J. Pain 2022, 16, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Doménech, J.; Sanchis-Alfonso, V.; Espejo, B. Changes in catastrophizing and kinesiophobia are predictive of changes in disability and pain after treatment in patients with anterior knee pain. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2295–2300. [Google Scholar] [CrossRef]
- Chmielewski, T.L.; George, S.Z. Fear avoidance and self-efficacy at 4 weeks after ACL reconstruction are associated with early impairment resolution and readiness for advanced rehabilitation. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 397–404. [Google Scholar] [CrossRef]
- Hellstadius, Y.; Lagergren, J.; Zylstra, J.; Gossage, J.; Davies, A.; Hultman, C.M.; Lagergren, P.; Wikman, A. A longitudinal assessment of psychological distress after oesophageal cancer surgery. Acta Oncol. 2017, 56, 746–752. [Google Scholar] [CrossRef]
- Occhipinti, S.; Zajdlewicz, L.; Coughlin, G.D.; Yaxley, J.W.; Dunglison, N.; Gardiner, R.A.; Chambers, S.K. A prospective study of psychological distress after prostate cancer surgery. Psycho-oncology 2019, 28, 2389–2395. [Google Scholar] [CrossRef] [PubMed]
- Malay, M.R.; Lentz, T.A.; O’Donnell, J.; Coles, T.; Mather III, R.C.; Jiranek, W.A. Development of a comprehensive, nonsurgical joint health program for people with osteoarthritis: A case report. Phys. Ther. 2020, 100, 127–135. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Psychological Domain | Example Item (Paraphrased) | Response Range |
|---|---|---|
| Negative Mood | “I am hot-headed” | 1–4 (Almost never–Almost always) |
| Poor Coping | “I can’t stop thinking about my pain” “I refrain from activities that may aggravate my pain” | 0–4 (Not at all–All the time) 0–6 (Completely disagree–Completely agree) |
| Positive Affect | “I live a full life despite chronic pain” “My emotional state does not deter me from performing therapy” | 0–4 (Never true–Always true) 0–10 (I can’t do it–I can do it) |
| Overall | |
|---|---|
| N | 133 |
| Age in years, mean (sd) | 49.0 (17.2) |
| Gender, n (%) | |
| Male | 59 (44.4) |
| Female | 74 (56.6) |
| Race, n (%) | |
| White | 94 (70.7) |
| Black/AA | 28 (21.1) |
| Mixed/Other/Not Reported | 11 (8.3) |
| ASA, mean (sd) | 2.19 (0.62) |
| BMI, mean (sd) | 29.91 (6.71) |
| Current Smoker, n (%) | 5 (3.8) |
| Laterality = Right, n (%) | 61 (45.9) |
| Anatomic Location of Surgery, n (%) | |
| Femur/Knee | 72 (54.1) |
| Foot/Toes | 1 (0.8) |
| Humerus/Elbow | 2 (1.5) |
| Leg/Ankle | 8 (6.0) |
| Other MSK | 4 (3.0) |
| Pelvis/Hip | 1 (0.8) |
| Shoulder | 45 (33.8) |
| CPT Code Category | |
| Femur/Knee Arthroscopy | 61 (45.9) |
| Femur/Knee Excision | 1 (0.8) |
| Femur/Knee Repair/Revision/Reconstruction | 10 (7.5) |
| Foot/Toes Fracture and/or Dislocation | 1 (0.8) |
| Humerus/Elbow Repair/Revision/Reconstruction | 2 (1.5) |
| Leg/Ankle Arthroscopy | 2 (1.5) |
| Leg/Ankle Fracture and/or Dislocation | 2 (1.5) |
| Leg/Ankle Incision | 1 (0.8) |
| Leg/Ankle Repair/Revision/Reconstruction | 3 (2.3) |
| Other MSK Intro or Removal | 4 (3.0) |
| Pelvis/Hip Fracture and/or Dislocation | 1 (0.8) |
| Shoulder Arthroscopy | 42 (31.6) |
| Shoulder Fracture and/or Dislocation | 2 (1.5) |
| Shoulder Repair/Revision/Reconstruction | 1 (0.8) |
| Preop | Postop | Mean Difference | T-Statistic | p-Value * | |
|---|---|---|---|---|---|
| N | 133 | 133 | |||
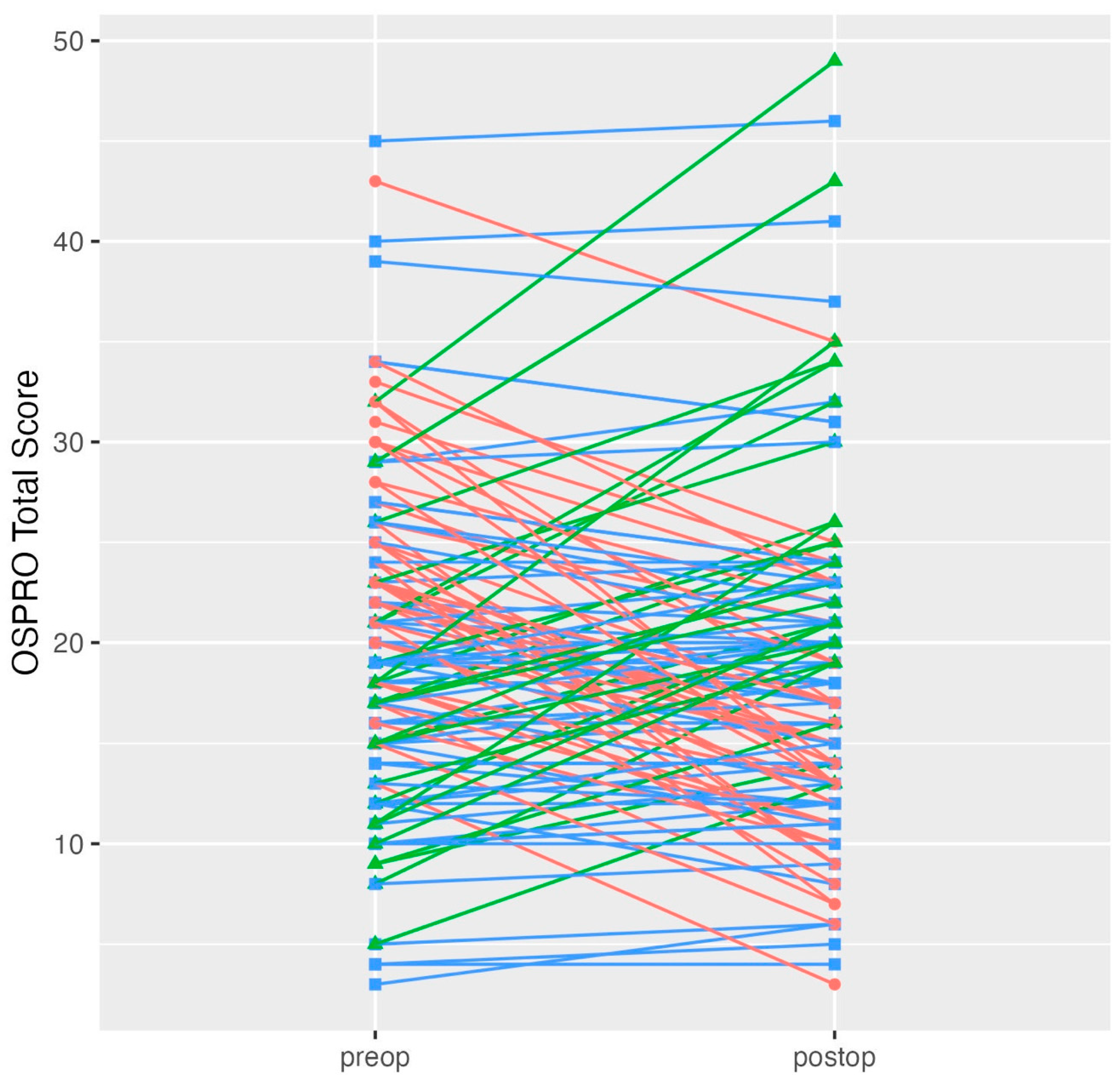
| OSPRO Total Score, mean (sd) | 20.0 (7.9) | 18.5 (8.6) | −1.44 | −2.24 | 0.027 |
| PHQ9, mean (sd) | 5.2 (4.1) | 4.8 (4.6) | −0.33 | −0.86 | 0.390 |
| STAI, mean (sd) | 36.1 (7.9) | 35.7 (8.6) | −0.46 | −0.73 | 0.466 |
| STAXI, mean (sd) | 15.2 (3.3) | 15.0 (3.7) | −0.29 | −1.27 | 0.207 |
| FABQPA, mean (sd) | 16.4 (4.8) | 13.5 (5.0) | −2.89 | −5.33 | <0.001 |
| FABQW, mean (sd) | 16.3 (11.5) | 13.1 (10.7) | −3.22 | −3.09 | 0.002 |
| PCS, mean (sd) | 16.1 (9.5) | 14.7 (10.1) | −1.40 | −1.52 | 0.132 |
| TSK11, mean (sd) | 24.7 (5.8) | 22.8 (6.0) | −1.88 | −3.25 | 0.001 |
| PASS20, mean (sd) | 30.8 (14.9) | 27.8 (15.8) | −3.00 | −2.24 | 0.027 |
| PSEQ, mean (sd) | 35.6 (10.6) | 36.8 (11.5) | 1.12 | 1.21 | 0.230 |
| SER, mean (sd) | 88.9 (19.4) | 87.1 (21.4) | −1.86 | −0.99 | 0.324 |
| CPAQ, mean (sd) | 63.3 (15.5) | 65.0 (16.3) | 1.66 | 1.26 | 0.208 |
| Meaningful Decrease | No Meaningful Change | Meaningful Increase | |
|---|---|---|---|
| Meaningful Change (1.5 × SD) in Questionnaire Score Estimates | |||
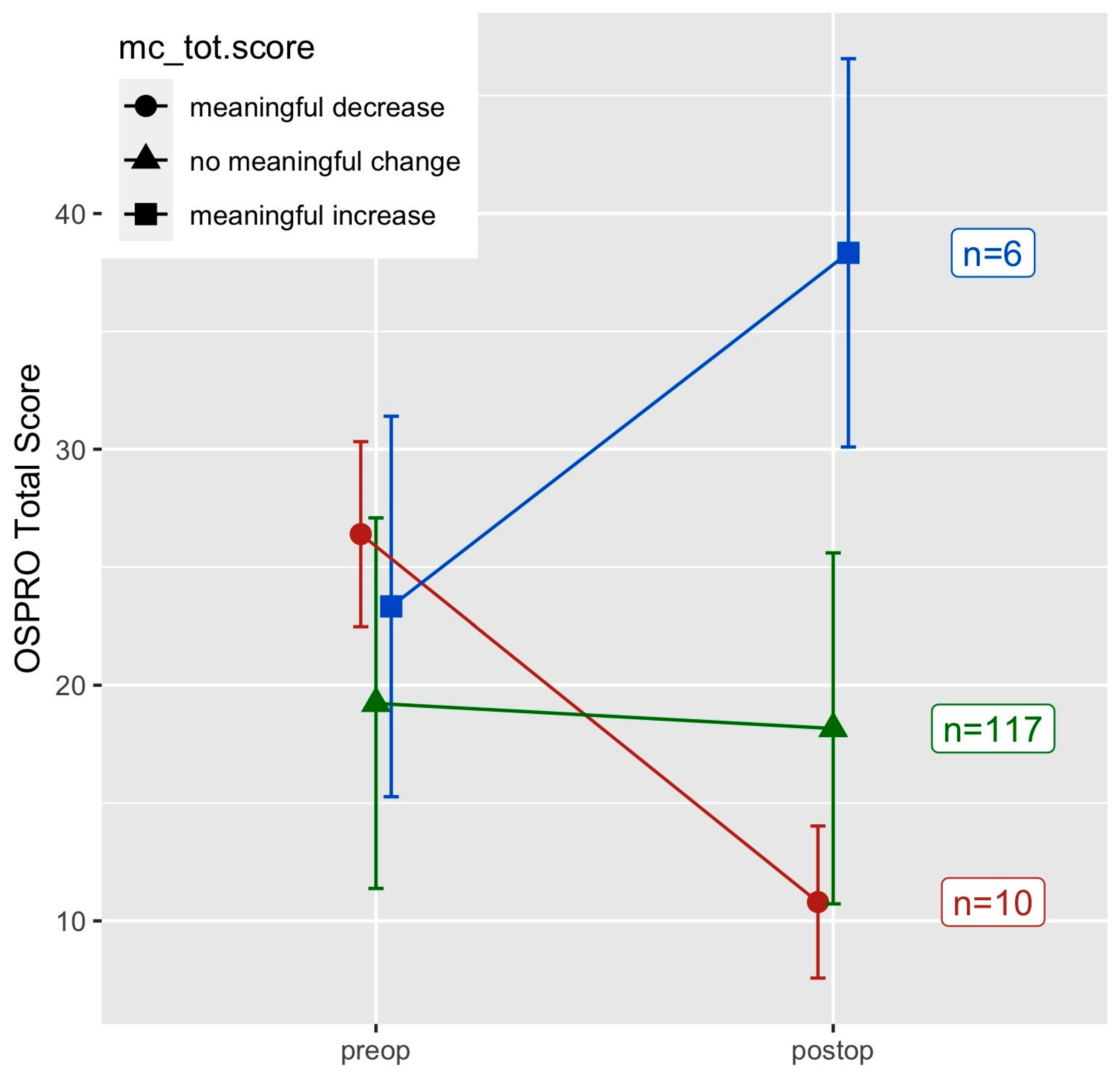
| OSPRO Total Score | 10 (7.5) | 117 (88.0) | 6 (4.5) |
| PHQ9 | 10 (7.5) | 117 (88.0) | 6 (4.5) |
| STAI | 6 (4.5) | 123 (92.5) | 4 (3.0) |
| STAXI | 6 (4.5) | 122 (91.7) | 5 (3.8) |
| FABQPA | 30 (22.6) | 95 (71.4) | 8 (6.0) |
| FABQW | 15 (11.3) | 112 (84.2) | 6 (4.5) |
| PCS | 17 (12.8) | 107 (80.5) | 9 (6.8) |
| TSK11 | 17 (12.8) | 108 (81.2) | 8 (6.0) |
| PASS20 | 15 (11.3) | 111 (83.5) | 7 (5.3) |
| PSEQ | 4 (3.0) | 117 (88.0) | 12 (9.0) |
| SER | 10 (7.5) | 113 (85.0) | 10 (7.5) |
| CPAQ | 5 (3.8) | 116 (87.2) | 12 (9.0) |
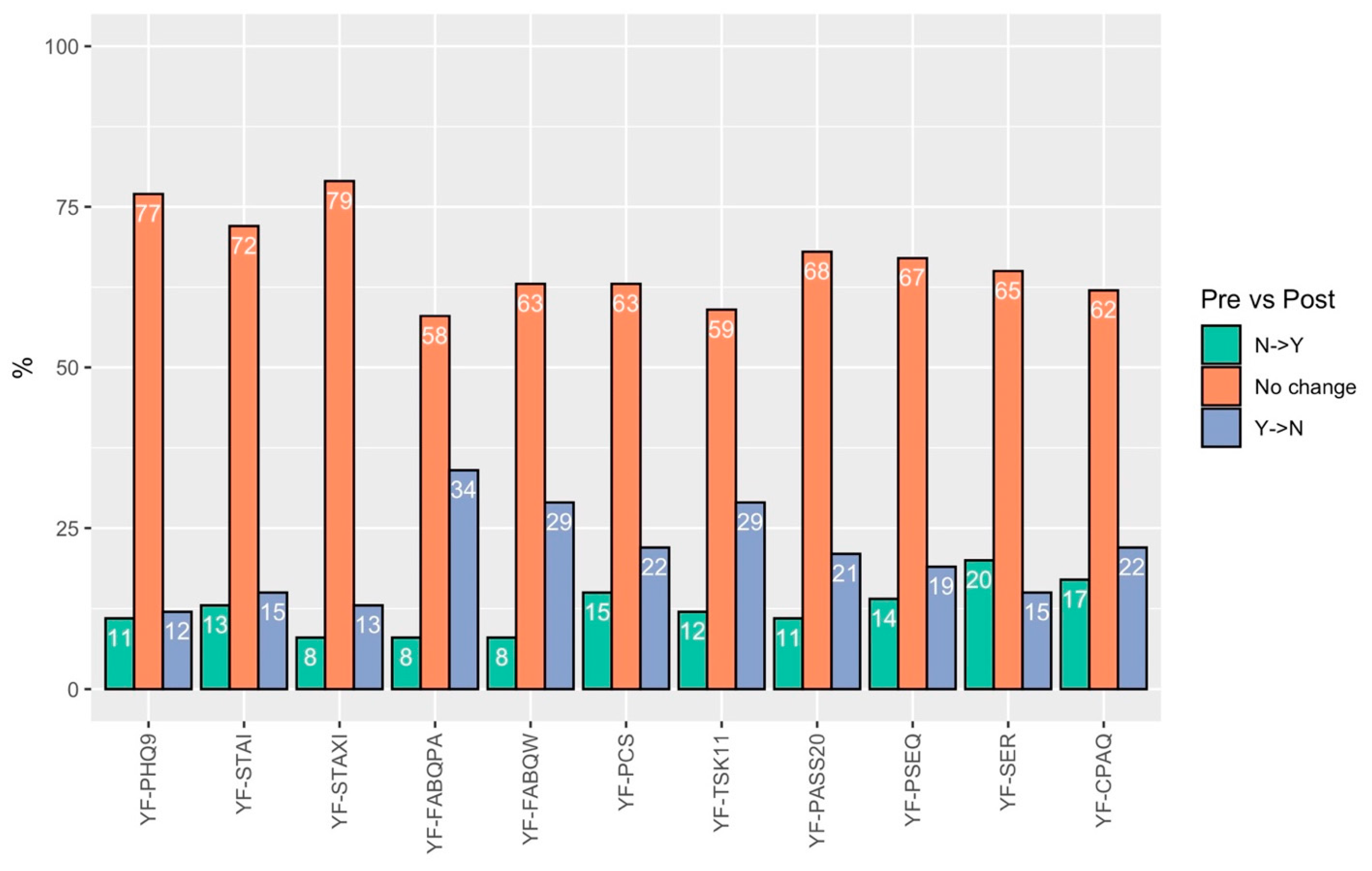
| Meaningful change (1.5 × SD) in patients presenting with YF for each questionnaire | |||
| PHQ9 | 10 (27.8) | 25 (69.4) | 1 (2.8) |
| STAI | 6 (14.6) | 34 (82.9) | 1 (2.4) |
| STAXI | 5 (12.2) | 36 (87.8) | 0 (0.0) |
| FABQPA | 26 (34.7) | 49 (65.3) | 0 (0.0) |
| FABQW | 15 (20.5) | 54 (74.0) | 4 (5.5) |
| PCS | 17 (32.1) | 32 (60.4) | 4 (7.5) |
| TSK11 | 17 (21.0) | 61 (75.3) | 3 (3.7) |
| PASS20 | 14 (22.2) | 46 (73.0) | 3 (4.8) |
| PSEQ | 2 (2.4) | 68 (82.9) | 12 (14.6) |
| SER | 4 (5.6) | 58 (80.6) | 10 (13.9) |
| CPAQ | 4 (5.6) | 56 (77.8) | 12 (16.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabell, G.H.; Kim, B.I.; Wu, K.A.; Luo, E.J.; Bulleit, C.; Morriss, N.J.; Lentz, T.A.; Lau, B.C. Changes in Pain-Related Psychological Distress After Surgery in Patients with Musculoskeletal Injury. Int. J. Environ. Res. Public Health 2025, 22, 857. https://doi.org/10.3390/ijerph22060857
Cabell GH, Kim BI, Wu KA, Luo EJ, Bulleit C, Morriss NJ, Lentz TA, Lau BC. Changes in Pain-Related Psychological Distress After Surgery in Patients with Musculoskeletal Injury. International Journal of Environmental Research and Public Health. 2025; 22(6):857. https://doi.org/10.3390/ijerph22060857
Chicago/Turabian StyleCabell, Grant H., Billy I. Kim, Kevin A. Wu, Emily J. Luo, Clark Bulleit, Nicholas J. Morriss, Trevor A. Lentz, and Brian C. Lau. 2025. "Changes in Pain-Related Psychological Distress After Surgery in Patients with Musculoskeletal Injury" International Journal of Environmental Research and Public Health 22, no. 6: 857. https://doi.org/10.3390/ijerph22060857
APA StyleCabell, G. H., Kim, B. I., Wu, K. A., Luo, E. J., Bulleit, C., Morriss, N. J., Lentz, T. A., & Lau, B. C. (2025). Changes in Pain-Related Psychological Distress After Surgery in Patients with Musculoskeletal Injury. International Journal of Environmental Research and Public Health, 22(6), 857. https://doi.org/10.3390/ijerph22060857