Abstract
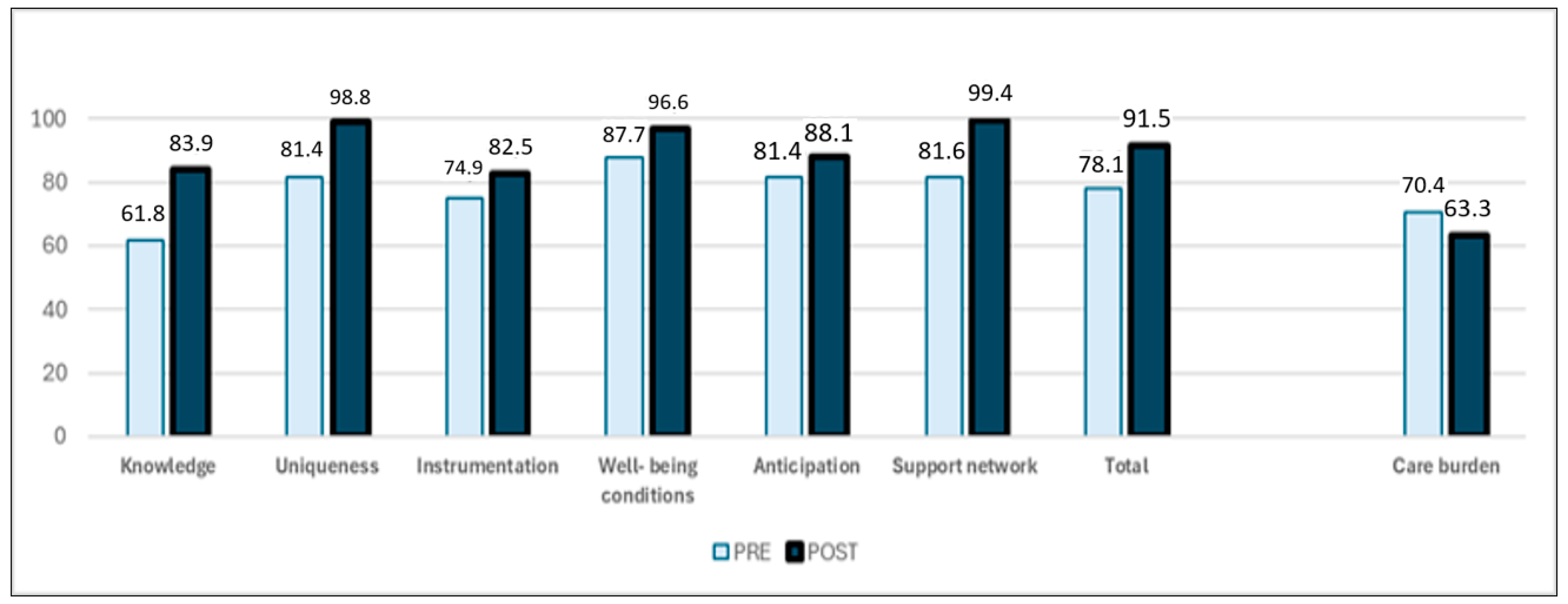
Nutritional health is essential for older people with dementia. Their feeding is a challenge for which caregivers are not always ready, and an intervention that supports them may have a significant social impact. The aim of this project is to design and evaluate the impact of systematic nursing intervention with formal caregivers to promote nutritional health for older people with dementia. This is a “Nursing Methodology Research” study conducted with formal caregivers of older people with dementia in four Colombian nursing homes. It includes three consecutive phases: (1) systematic intervention design under Whittemore and Grey’s parameters, (2) intervention validation with seven international experts, and (3) measurement of intervention impact, which included a quasi-experimental pre-test–post-test design. The “Nurturing Neurons—Formal Caregivers” intervention met the criteria of systematic health interventions. In response to the work and personal requirements of formal caregivers, the intervention used a tele-support modality. Its content validity ratio (CVR) ranged from 0.88 to 0.92; its content validity index (CVI) was 0.90. The experience was positive for the participant caregivers (94.9%) and professional providers (92.5%). The overall caregivers’ caring competence changed from the medium, 78.1, to the high category, 91.5 (p < 0.001). Their perceived burden of care changed from 70.4 to 63.6 (p < 0.001). In conclusion, “Nurturing Neurons—Formal Caregivers” achieved a positive impact, with changes in the structure, processes, and outputs to promote the nutritional health of older people with dementia. It led to a significant improvement in formal caregivers’ caring competence and decreased their perceived care burden. Its cost–benefit was favorable; it generated health equity for a vulnerable population and achieved unexpected benefits in the context.
1. Introduction
According to the World Health Organization [1], the world is experiencing a significant and accelerated increase in longevity. It estimates that between 2015 and 2050, the share of the world’s population over 60 years of age will increase from 12% to 22%, and that in 2050, 80% of older adults will live in low- and middle-income countries like Colombia.
This increase in longevity poses challenges to social and health systems, which require more resources to meet the demands of this population [2]. As society ages, the support of functionality, autonomy, and well-being in older people becomes an important challenge [3,4]. Longevity brings an increase in the number of people with dementia, which leads to higher pressure on health systems and society. There are currently more than fifty-five million people with dementia in the world, a figure that will reach 152 million in 2050 [5]. In response to this situation, the World Health Organization created a global plan that identified the following necessary actions: giving priority to the issue within public health systems; increasing social awareness and inclusive actions; reducing associated risks; strengthening diagnosis, treatment, and care; supporting caregivers; having information systems; and promoting research and innovation in this field. This plan proposes that 75% of countries should develop policies and programs to support and train caregivers of people with dementia by 2025 [6].
Among the actions related to care for older adults with dementia are food and nutrition. Research indicates that good nutrition is associated with a lower level of cognitive decline and that maintaining adequate nutrition is essential to promote a better quality of life in older adults [7,8]. However, one-third of older adults with dementia have malnutrition, and at least half of them are at risk of developing it, especially in long-term care settings, with malnutrition incidence rates reaching 75.6% and malnutrition risks of 90.4% [9]. Malnutrition in older people with dementia is related to changes in eating behaviors, such as altered hunger signals and difficulty feeding themselves [9]. It is also associated with loss of appetite, decreased olfactory and gustatory perception of flavors, forgetting to eat or drink, difficulties in chewing or swallowing, disruptive behaviors, or mealtime-related events [10]. Poor nutritional status in this group is, in turn, related to greater cognitive and functional deterioration, as well as an increase in neuropsychiatric symptoms, like depression and apathy [11]. There is an urgent need to break this vicious cycle and mitigate the risks of malnutrition in older people with dementia through robust detection and intervention strategies, including dietary modifications and caregiver support measures to improve their nutritional status [12].
A recent systematic search analyzed thirty-three studies on interventions to promote nutrition in older adults with dementia published between 1995 and 2023. Its results report interventions with multiple components that achieved positive effects on food intake: support with meals; environmental modifications that transform the mealtime experience; family-style food offerings; proper presentation of dishes; training for caregivers; and Montessori-type stimulation. According to the researchers, the interventions had a positive effect, with greater knowledge, better attitudes from caregivers, and a meal offering according to the reality and needs of each person and institution. Eighteen studies were conducted in North America, five in Europe, one in Australia, and eight in Asia; none were conducted in Latin America. Most focused on older adults’ nutritional health, with only 21% including formal caregivers. No impact measurement was reported [13].
Caregivers’ and professionals’ views on nutritional health care for people with dementia highlight the importance of accounting for specific conditions, behaviors, and malnutrition risks. They recommend using supplements, environmental management, and addressing caregivers’ stress levels, which can lead to poor food choices, affecting both their health and that of the person they care for [14].
A study on caregivers’ experiences with dementia-related feeding and eating difficulties indicated the impact of dementia on the nutritional status of individuals. Caregivers reported increased levels of stress, which correlated with the level of cognitive impairment of the person they were caring for [15].
Despite the advances, these studies do not address issues like the impact of these situations on families or the stress that families create on care personnel, which can cause greater overload. Moreover, the perception of caregiver burden has a direct impact on the quality of care provided by the caregiver [16]. Therefore, it is important to provide and accept technical training on care, psychoeducation, psychological support, and the development of ethical and emotional tools. This will help bridge the gap between formal caregivers and families, as well as lessen the perceived burden of understanding and accepting this aspect of aging. Supports that enhance caregiving can ease the impact of illness and death and help redefine bereavement and better manage stress [17].
The present study aims to design and rigorously evaluate the impact of a systematic nursing intervention specifically targeted to formal caregivers. The intervention objective is to optimize the nutritional health of older adults with dementia and simultaneously mitigate the burden inherent to the caregiving process. This research seeks to respond to current international commitments that advocate for the well-being of the growing population of older adults with dementia, who are at elevated risk of malnutrition. In addition, it seeks to promote the development and implementation of concrete support strategies for caregivers, enabling them to effectively promote the nutritional health of their patients. Finally, this work seeks to contribute to closing the existing knowledge gap in this area by addressing the impact measurement within the Latin American cultural context, thus enriching the global understanding of this complex study phenomenon.
2. Materials and Methods
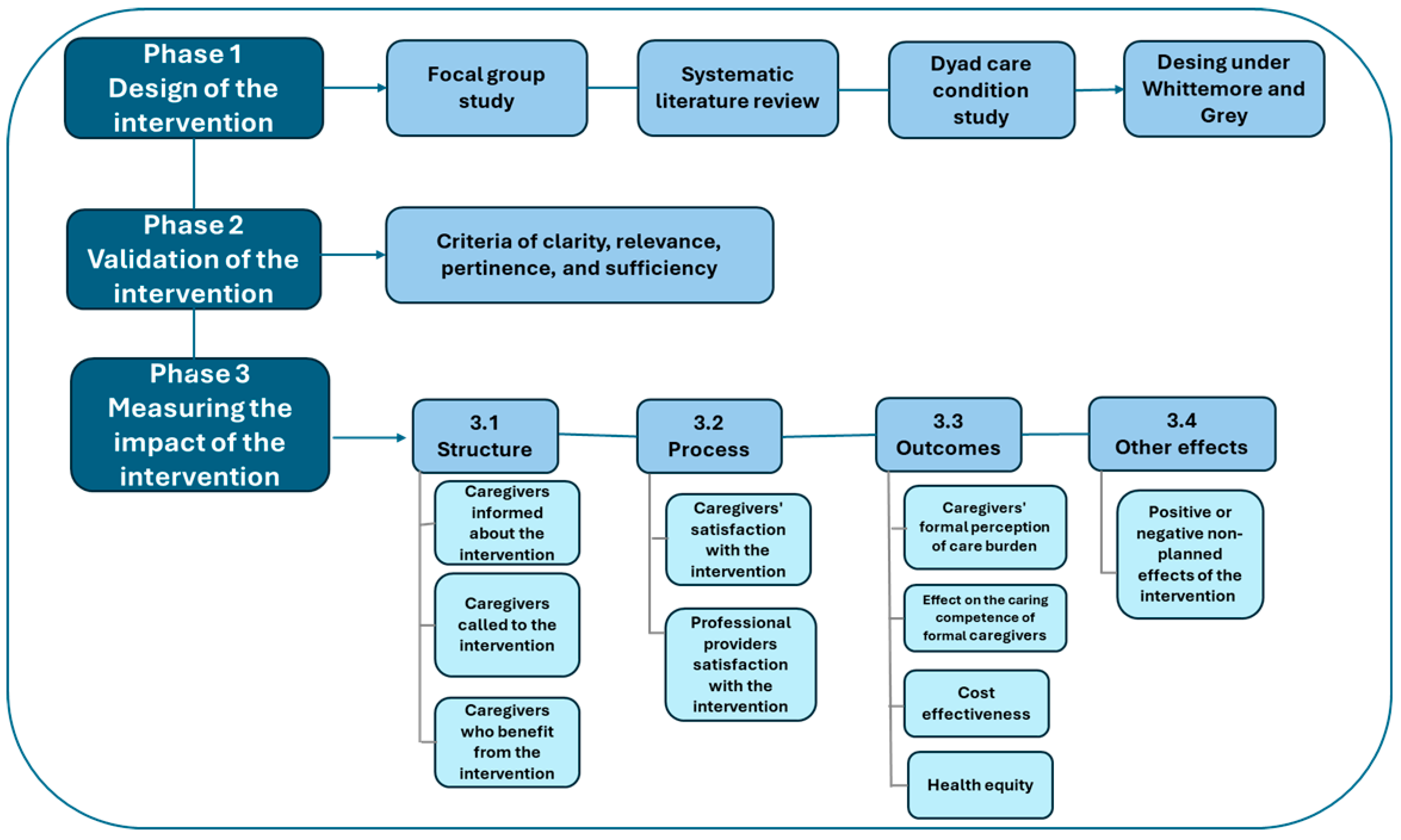
This study is a Nursing Methodology Research study. It is part of the project “Nurturing Neurons” 2022–2025. It includes three consecutive phases (see Figure 1).
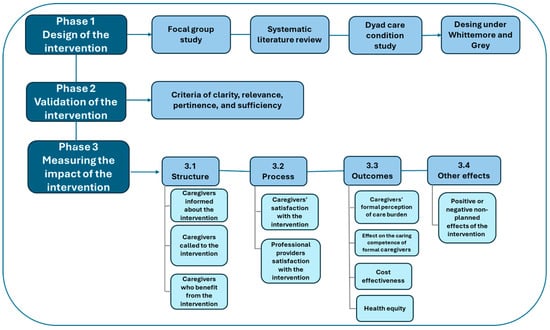
Figure 1.
Study phases. Source: Study data, 2025.
2.1. Phase 1: Intervention Design
The intervention design followed Whittemore and Grey’s guidelines for systematic health interventions. These included finding the problem to be intervened; organizing the content, processes, and conditions for the intervention; and defining its expected effects [18].
Three previous studies from the same research project were inputs for the intervention design: (1) A focus group study with representatives of 14 Colombian gerontological services that described the experience of managers and caregivers concerning feeding and nutrition for older adults with dementia. (2) A systematic literature review that identified the best available evidence on interventions that could improve nutritional nursing care for institutionalized older adults with dementia. (3) An exploratory study that characterized the nutritional care needs of elderly individuals with dementia and their caregivers. Findings from the focus group and characterization studies confirmed the presence of malnutrition or an elevated risk of malnutrition among older adults with dementia. They also reflected a high perceived caregiving burden of formal caregivers, as well as a lack of guidance and skills to address nutritional health problems. Formal caregivers expressed interest in receiving support to develop better caregiving skills, but they perceived a lack of adequate time and space for training in their work environment. However, they indicated frequent use of telephone and computer resources for caregiving support.
2.2. Phase 2: Intervention Validation
Seven experts from Latin America validated the intervention. All of them had postgraduate degrees and more than three years of experience with older people with dementia and nutritional health care. They reviewed the intervention’s facial and content validity based on a previously prepared format that rated levels of clarity, relevance, pertinence, and sufficiency. The evaluation format used a Likert scale ranging from one (does not meet the criteria) to four (fully meets the condition evaluated). Each case included space for observations. The results analysis process used Lawshe’s parameters, modified by Tristan, to determine the content validity ratio (CVR) and content validity index (CVI), accepting results above 0.75 as valid [19].
2.3. Phase 3: Impact Measurement
We developed the intervention in four elderly care institutions. It included 106 adult formal caregivers who cared for older people with dementia, had access to a mobile device, and had a formal technical or 1.5-year degree.
The intervention impact measurements included its structure, processes, and output. It followed Tanahashi’s framework to enable global understanding [20]. It also included indicators that responded to the five goals proposed by the WHO for the supply of health services: service experience for both receivers and offers, service results, cost effectiveness, and health equity [21,22]. Finally, the impact measurement assessed the intervention’s positive or negative effects according to participants [23] (see Table 1).

Table 1.
Impact measurement.
Our research group, based on international experiences [24], accepted values of 80% or more as a positive result for the analysis of the structure and process indicators.
We assessed the perception of the care burden for the output indicators based on the section of perception of burden and support of the survey of characterization for the care of the dyad GCPC-UN-D, validated in Colombia [25]. We used this scale because we detected high care burden perception when it was used in the previous characterization study. We considered the survey to be simple, sufficient, and culturally appropriate. The survey scale evaluated the overload perception on a range from zero (none) to three (intense).
Our team used the abbreviated CUIDAR instrument, validated in Colombia, to measure care competence. It assesses knowledge, uniqueness, instrumentation, welfare conditions, anticipation, and support network. Its Cronbach’s alpha was 0.928 [26]. The instrument’s authors state that caring competence is high when scores are above 81, medium when scores are between 47 and 81, and low when scores are below 47.
To evaluate the intervention’s effect, we performed a quasi-experimental pre-test–post-test design. Our participant selection was intentionally from four geriatric homes characterized as part of the previous studies. We evaluated two hypotheses with respect to the effect of the intervention. H10: There is no statistically significant difference in the perception of the burden of formal caregivers before and after the intervention. H20: There is no statistically significant difference in care competence before and after the intervention. Our rejection value for the related samples t-test was p < 0.05 in both cases.
We avoided study biases of selection, attrition, instrumentation, and measurement. We included participants from institutions with different public and private legal statuses, from different socioeconomic strata, and with both rural and urban locations; we invited all caregivers of the selected institutions to participate in the study. We requested the support of management and institutions to ensure the voluntary participation of formal caregivers in the entire intervention process. We selected standardized and previously defined instruments and measures and asked an external trained professional to collect the measurement data.
To ensure external validity, the results apply only to the Colombian population included but may be potentially beneficial for other groups of a similar nature.
3. Results
3.1. Intervention Design
The following is a summary of the nursing systematic intervention (see Table 2).
Table 2.
Summary of the nursing systematic intervention.
The experts included two nutritionists, four nurses, and a psychologist. Regarding their nationalities, three were Colombians, one was Cuban, one was Chilean, one was Ecuadorian, and one was Venezuelan. The validation results showed a CVR range from 0.88 to 0.98 and a CVI of 0.90 (see the Supplementary Material).
In response to the experts’ suggestions, the researchers included references relevant to the context, activities to strengthen support skills for the caregivers, and clarification of concepts and terms. Our research group also incorporated evaluation details to make it more constructive. Finally, in response to an expert suggestion, the researchers contacted fourteen relatives of these institutionalized elderly patients to inquire about their expectations of care associated with nutritional health and incorporated their suggestions.
3.2. Impact Measurement
Table 3.
Impact results of the intervention.
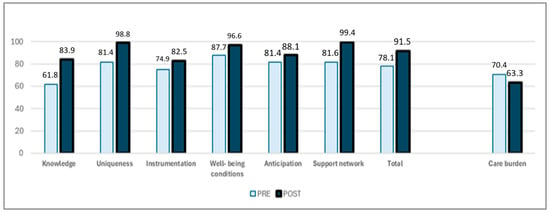
Figure 2.
Care competence and perceived burden of formal caregivers. Source: Study data, 2025.
3.3. Unexpected Effects of the Intervention
This project created a set of interdisciplinary interventions that help individuals and the community. These were the development of innovative programs, the impact on public policies, improvements in quality of life, and the strengthening of academic training and scientific dissemination (see the Supplementary Material).
4. Discussion
This study, which measured the impact of the systematic nursing intervention “Nurturing Neurons—Formal Caregivers”, showed positive changes in structure, processes, and products to promote the nutritional health of older adults with dementia. We found positive changes in the structure of the intervention coverage, programmed service coverage, and acceptability of the intervention. Both caregivers and intervention providers reported satisfaction with the process and results. The results showed a positive effect on reducing the perceived burden of care for formal caregivers, effective coverage, improved caregiving competency among caregivers, achievement of cost–benefit ratios with the intervention, and greater health equity.
This systematic nursing intervention is directed at formal caregivers of institutionalized older adults with dementia to promote their nutritional health. Researchers used the results of earlier studies within the same project to leverage the intervention design. This aligns with third-generation universities’ purpose of creating social value based on the development of knowledge [27].
The intervention validation conducted under the Tristan-adjusted Lawshe’s parameters reflected a consensus among the evaluators on the relevance of each of its components [19]. The proposal met the acceptance threshold with expert suggestions. The inclusion of international Spanish-speaking experts helped unify linguistic expressions to make it possible to replicate it in other contexts.
The intervention demonstrated substantial service coverage and received positive acceptance from the participants. The lower-than-expected contact coverage was due to employment status reasons, such as vacation or temporary leave, resignation or retirement, and role changes for the formal caregiver within the institution. It is crucial to evaluate the impact of these modifications on the individuals receiving care and to implement strategies that facilitate reduced employee turnover [28]. It is also necessary to review whether there is an excessive burden of care, which may be associated with caregiver safety, patient behavior, or the time devoted to the people in their care [28].
The intervention aimed to include users and feature measurable, replicable parameters. Both recipients and providers found the intervention inclusive and satisfactory. Dialogue among participants can yield valuable contributions to society [29].
The study results rejected both null hypotheses: there was a statistically significant decrease in the care burden perceived by formal caregivers and a significant increase in their care competence. This achievement in a brief period of six weeks may be explained by the interest and support of the institutions in strengthening the care competency of the caregivers and the backing they received to participate in the intervention.
We designed the intervention in a tele-support modality to conveniently fit formal caregivers’ schedules and locations. It had a total coverage effectiveness.
This type of intervention makes it easier for caregivers to reconcile work, family life, and personal expectations, and we found that it reduced its cost by more than half. Therefore, this project ratifies the recommendation to deliver interventions in diverse ways to respond to the reality of caregivers of people with dementia [30]. This type of intervention has the potential to help caregivers reduce the malnutrition risk in elderly people with dementia and avoid other complications, including an accelerated cognitive decline [31]. However, we need to continue this research to demonstrate if it helps in such topics.
Our intervention modality shows similar effects to the intervention developed with a telehealth coaching modality, which also found positive effects on caregivers of people with dementia nutrition [32].
The reported interventions to improve the feeding and nutrition of older adults with dementia aimed to improve their participation, compensate for their dysfunction, and increase food intake through nutritional supplementation, assistance, person-centered care, environmental modifications, education, and other multicomponent actions [21]. This study supports the importance of person-centered care and assessments to train and motivate staff to provide this care [33,34]. Our research evaluated the nursing systematic intervention impact, unlike previous studies.
Our findings support previous researchers’ findings that identified ways to optimize formal caregivers’ ability to feed individuals with dementia. They reported that the processes associated with nutrition are complex and that caregiver care competence plays a key role in positively impacting the eating experience of individuals with dementia [35,36]. We also agree with a study on caregivers who experience challenges related to the nutritional health of older adults with dementia in their care. The results emphasize the importance of receiving information and support regarding nutritional care from health professionals to develop management strategies and to reduce the burden of caregiving [37].
This systematic nursing intervention strengthens the knowledge, attitude, and behavior of formal caregivers of people with dementia at mealtimes. These may include, as reported in previous studies, taking care of their posture and comfort; verbal and nonverbal communication; their physical orientation; food description and respect for preferences; portioning; the variety of foods and beverages offered; ensured schedules; cleanliness of the person and their environment; and manifestations of commitment and closeness to them [35].
This project responds to the needs of caregivers of older people with dementia. It is necessary to consider their own opinion regarding the training they have or require. While it is important to provide them with increased caregiving support, it is also important to ensure that they have the knowledge and skills needed to perform their role [38]. Additionally, the researcher’s selection of the institutions taking part in this research reflected equity in the proposed supply of health services [21].
Our group responded to global demand in the field of nutritional health of people with dementia. Our results have a positive impact on the structure, process, and expected products. In this sense, this field of study requires continued expansion to broaden the scope of this systematic nursing intervention. This impact evaluation study included participants as a fundamental principle to ensure effectiveness and to promote equity and sustainability [23,29]. Despite these findings, this study has the limitation of not having a randomized controlled experimental design that would improve the level of evidence of these results.
5. Conclusions
The nursing systematic and validated tele-support intervention “Nurturing Neurons—Formal Caregivers”, which promotes nutrition in older people with dementia, achieved a positive impact, with changes in the structure, processes, and outputs that promote the nutritional health of older people with dementia.
Its design responded to formal caregivers’ needs and contexts. It reflected good overall coverage and programmed care and was well accepted, as evidenced by its completion by caregivers who kept their work positions.
The intervention led to elevated levels of satisfaction among recipients and providers. It significantly decreased the perceived burden of care for formal caregivers and increased their caring competence, while having effective coverage, a net benefit, and greater health equity for the vulnerable population.
The impact evaluation design revealed unexpected results that positively affected the community involved. This input can be the basis for public policies that respond to international commitments for the care of this population group.
Given the positive impact of this intervention, it will be relevant to advance this research field by strengthening the emotional, bioethical, and educational aspects and involving both formal caregivers and family members to strengthen the nutritional health care of older people with dementia while reducing the care burden for their caregivers.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/ijerph22060849/s1: Supplementary material Table S1: Intervention validation results; Supplementary material Table S2: Unexpected effects of the intervention.
Author Contributions
Conceptualization, P.S.-G., M.E.M.-F. and B.S.-H.; methodology, P.S.-G., M.E.M.-F., A.R.-R., J.A.C.-M., B.R.-P. and B.S.-H.; software, P.S.-G., M.E.M.-F. and B.S.-H.; validation, P.S.-G., M.E.M.-F., A.R.-R., J.A.C.-M., B.R.-P. and B.S.-H.; formal analysis, P.S.-G., M.E.M.-F., A.R.-R., J.A.C.-M., B.R.-P. and B.S.-H.; investigation, P.S.-G., M.E.M.-F., A.R.-R., J.A.C.-M., B.R.-P. and B.S.-H.; resources, P.S.-G., M.E.M.-F., A.R.-R., J.A.C.-M. and B.S.-H.; data curation, P.S.-G., M.E.M.-F., A.R.-R., J.A.C.-M., B.R.-P. and B.S.-H.; writing—original draft preparation, P.S.-G., M.E.M.-F. and B.S.-H.; writing—review and editing, P.S.-G., M.E.M.-F., A.R.-R., J.A.C.-M., B.R.-P. and B.S.-H.; visualization, P.S.-G., M.E.M.-F., A.R.-R., J.A.C.-M., B.R.-P. and B.S.-H.; supervision, P.S.-G., M.E.M.-F., J.A.C.-M., B.R.-P., and B.S.-H.; project administration, P.S.-G., M.E.M.-F. and B.S.-H.; funding acquisition, M.E.M.-F., A.R.-R., J.A.C.-M. and B.S.-H. All authors have read and agreed to the published version of the manuscript.
Funding
Universidad de La Sabana funded this research, under project Nos. ENF 60 2021 and ENF 63 2022. Puravida Fundación and Universidad de Los Andes, Chile, both participated with in-kind contributions.
Institutional Review Board Statement
This study complied with the Declaration of Helsinki and received approval from the Research Ethics Committee of Universidad de La Sabana (Approval Act No. 0080820, Approval Date: 8 August 2020) with modification (Approval Act No. 011 2023, Approval Date: 12 October 2023).
Informed Consent Statement
All subjects or their legal representatives provided informed consent for this study. The research group obtained written informed consent from the participants or their legal representatives to publish this paper.
Data Availability Statement
The data are available on request from the corresponding author. The authors are interested in contacting different organizations that are interested in the same topics.
Acknowledgments
The authors acknowledge all the individual and institutional participants for their commitment to improving the quality of life and nutritional health of older people with dementia.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Aging and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 2 January 2025).
- Sierra, F. Geroscience and the challenges of aging societies. Aging Med. 2019, 2, 132. [Google Scholar] [CrossRef] [PubMed]
- Phelan, A.; Ayalon, L. The intersection of ageism and elder abuse. In Advances in Elder Abuse Research: Practice, Legislation, and Policy; Springer: Berlin, Germany, 2020; pp. 11–22. [Google Scholar] [CrossRef]
- Vaupel, J.W.; Villavicencio, F.; Bergeron-Boucher, M.P. Demographic perspectives on the rise of longevity. Proc. Natl. Acad. Sci. USA 2021, 118, e2019536118. [Google Scholar] [CrossRef] [PubMed]
- Hakim, M. Dementia: Guide to diagnosis and management. Bangladesh J. Med. 2023, 35, 138–139. [Google Scholar] [CrossRef]
- Cahill, S. WHO’s global action plan on the public health response to dementia: Some challenges and opportunities. Aging Ment. Health 2020, 24, 197–199. [Google Scholar] [CrossRef]
- Cao, X.P.; Xu, W.; Wang, Z.T.; Tan, L.; Yu, J.T. Dietary Components and Nutritional Strategies for Dementia Prevention in the Elderly. Curr. Alzheimer Res. 2023, 20, 224–243. [Google Scholar] [CrossRef]
- Wu, Y.T.; Beiser, A.S.; Breteler, M.M.; Fratiglioni, L.; Helmer, C.; Hendrie, H.C.; Honda, H.; Ikram, M.A.; Langa, K.M.; Lobo, A.; et al. The changing prevalence and incidence of dementia over time—Current evidence. Nat. Rev. Neurol. 2017, 13, 327–339. [Google Scholar] [CrossRef]
- Arifin, H.; Chen, R.; Banda, K.J.; Kustanti, C.Y.; Chang, C.Y.; Lin, H.C.; Liu, D.; Lee, T.Y.; Chou, K.R. Meta-analysis and moderator analysis of the prevalence of malnutrition and malnutrition risk among older adults with dementia. Int. J. Nurs. Stud. 2024, 150, 104648. [Google Scholar] [CrossRef]
- Murphy, J.L. Improving nutrition and hydration in older people with dementia in care homes. Nurs. Older People 2022, 34, 35–42. [Google Scholar] [CrossRef]
- Kauzor, K.; Drewel, M.; Gonzalez, H.; Rattinger, G.B.; Hammond, A.G.; Wengreen, H.; Lyketsos, C.G.; Tschanz, J.T. Malnutrition, and neuropsychiatric symptoms in dementia: The Cache County dementia progression study. Int. Psychogeriatr. 2023, 35, 653–663. [Google Scholar] [CrossRef]
- Volkert, D. Nutrition and Dementia-Dementia and Nutrition. Ther. Umschau. Rev. Ther. 2023, 80, 217–225. [Google Scholar] [CrossRef]
- Passos, L.; Tavares, J.; Batchelor, M.; Figueiredo, D. Interventions to address mealtime support needs in dementia: A scoping review. PLoS ONE 2024, 19, e0300987. [Google Scholar] [CrossRef] [PubMed]
- Labyak, C.; Sealey-Potts, C.; Wright, L.; Kriek, C.; Dilts, S. Informal caregiver and healthcare professional perspectives on dementia and nutrition. J. Hum. Nutr. Diet. 2024, 37, 1308–1319. [Google Scholar] [CrossRef]
- Sharma, S.; Halim, N.A.A.; Maniam, P. Caregiver experiences with dementia-related feeding/eating difficulties. Healthcare 2024, 12, 133. [Google Scholar] [CrossRef] [PubMed]
- Vicente de Sousa, O.; Mendes, J.; Amaral, T.F. Association between nutritional and functional status indicators with caregivers’ burden in Alzheimer’s disease. Nutr. Diet. 2022, 79, 380–389. [Google Scholar] [CrossRef]
- Gilsenan, J.; Gorman, C.; Shevlin, M. Explaining caregiver burden in a large sample of UK dementia caregivers: The role of contextual factors, behavioural problems, psychological resilience, and anticipatory grief. Aging Ment. Health 2023, 27, 1274–1281. [Google Scholar] [CrossRef]
- Whittemore, R.; Grey, M. The systematic development of nursing interventions. J. Nurs. Scholarsh. 2002, 34, 115–120. [Google Scholar] [CrossRef]
- Tristán-López, A. Modificación al modelo de Lawshe para el dictamen cuantitativo de la validez de contenido de un instrumento objetivo. Av. Medición 2008, 6, 37–48. [Google Scholar]
- Tanahashi, T. Health service coverage and its evaluation. Bull. World Health Organ. 1978, 56, 295. [Google Scholar] [PubMed] [PubMed Central]
- Nundy, S.; Cooper, L.A.; Mate, K.S. The quintuple aim for health care improvement: A new imperative to advance health equity. JAMA 2022, 327, 521–522. [Google Scholar] [CrossRef]
- Gould, K.A. Equity: Introducing the quintuple aim. Dimens. Crit. Care Nurs. 2022, 41, 119–120. [Google Scholar] [CrossRef]
- Libera Bonilla, B.E. Impacto, impacto social y evaluación del impacto. Acimed 2007, 15. Available online: http://scielo.sld.cu/scielo.php?pid=S1024-94352007000300008&script=sci_abstract (accessed on 18 January 2025).
- Borrell, C.; Ru, M.; Pasar n, M.I.; Benach, J.; Kunst, A. La medición de las desigualdades en salud. Gac. Sanit. 2000, 14 (Suppl. S3), 20–33. [Google Scholar]
- Chaparro Díaz, L.; Sánchez Herrera, B.; González, G.M. Encuesta de caracterización del cuidado de la diada cuidador familiar-persona con enfermedad crónica. Rev. Cienc. Cuid. 2014, 11, 31–45. [Google Scholar]
- Carrillo González, G.M.; Sánchez Herrara, B.; Vargas, E. Desarrollo y pruebas psicométricas del Instrumento” cuidar”-versión corta para medir la competencia de cuidado en el hogar. Rev. Univ. Ind. Santander. Salud. 2016, 48, 222–231. [Google Scholar] [CrossRef]
- Wissema, J.G. Towards the Third-Generation University: Managing the University in Transition; Edward Elgar Publishing: Cheltenham, UK, 2009. [Google Scholar]
- Allen, A.P.; Buckley, M.M.; Cryan, J.F.; Ní Chorcoráin, A.; Dinan, T.G.; Kearney, P.M.; O’Caoimh, R.; Calnan, M.; Clarke, G.; Molloy, D.W. Informal caregiving for dementia patients: The contribution of patient characteristics and behaviours to caregiver burden. Age Ageing 2020, 49, 52–56. [Google Scholar] [CrossRef]
- Russell, J.; Fudge, N.; Greenhalgh, T. The impact of public involvement in health research: What are we measuring? Why are we measuring it? Should we stop measuring it? Res. Involv. Engagem. 2020, 6, 63. [Google Scholar] [CrossRef]
- Wójcik, D.; Szczechowiak, K.; Konopka, P.; Owczarek, M.; Kuzia, A.; Rydlewska-Liszkowska, I.; Pikala, M. Informal dementia caregivers: Current technology use and acceptance of technology in care. Int. J. Environ. Res. Public Health 2021, 18, 3167. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446, Erratum in Lancet 2023, 402, 10408. [Google Scholar] [CrossRef] [PubMed]
- D’avolio, D.; Gropper, S.S.; Appelbaum, M.; Thiengtham, S.; Holt, J.; Newman, D. The impact of a pilot telehealth coaching intervention to improve caregiver stress and well-being and to increase dietary protein intake of caregivers and their family members with dementia–Interrupted by COVID-19. Dementia 2023, 22, 1241–1258. [Google Scholar] [CrossRef]
- Kul, B.; Tülek, Z. Optimal Care in the Management of Eating Difficulties in Patients with Dementia. Geriatr. Bilim. Derg. 2024, 7, 156–166. [Google Scholar] [CrossRef]
- Blake, D.; Berry, K.; Brown, L.J. A systematic review of the impact of person-centred care interventions on the behaviour of staff working in dementia care. J. Adv. Nurs. 2020, 76, 426–444. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Kim, S.; Alessio, H. Mealtime caregiving knowledge, attitudes, and behaviors for people living with dementia: A systematic review of psychometric properties of instruments. Int. J. Nurs. Stud. 2021, 114, 103824. [Google Scholar] [CrossRef] [PubMed]
- Faraday, J.; Abley, C.; Beyer, F.; Exley, C.; Moynihan, P.; Patterson, J.M. How do we provide good mealtime care for people with dementia living in care homes? A systematic review of carer–resident interactions. Dementia 2021, 20, 3006–3031. [Google Scholar] [CrossRef] [PubMed]
- Ball, L.; Jansen, S.; Desbrow, B.; Morgan, K.; Moyle, W.; Hughes, R. Nutrition support in dementia care. Nutr. Diet. 2015, 72, 22–29. [Google Scholar] [CrossRef]
- Mueller, A.; Thao, L.; Condon, O.; Liebzeit, D.; Fields, B. A systematic review of the needs of dementia caregivers across care settings. Home Health Care Manag. Pract. 2022, 34, 133–147. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).