

Barriers and Facilitators of Tobacco Cessation Interventions at the Population and Healthcare System Levels: A Systematic Literature Review


Abstract
1. Introduction
2. Materials and Methods
2.1. PICO Framework
2.2. Search Strategy and Database
2.3. Screening Questions
- Is it about tobacco/smoking cessation interventions AND
- Is it conducted in the United States AND
- Is the study outcome tobacco cessation AND
- Are health/healthcare barriers and facilitators explored?
2.4. Data Extraction, Analysis, and Quality Assessment
3. Results
3.1. Population Level Barriers and Facilitators in Tobacco Cessation Interventions
3.1.1. Medical Interventions
3.1.2. Non-Medical Interventions
3.2. Healthcare System Level Barriers and Facilitators in Tobacco Cessation Interventions
3.2.1. Medical Interventions
3.2.2. Non-Medical Interventions
4. Discussion
5. Recommendations for Public Health and Healthcare Systems
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Search Details | Results | Database |
|---|---|---|
| ((“Tobacco Use Cessation”[MeSH Terms] OR “Smoking Cessation”[MeSH Terms] OR “Smoking Reduction”[MeSH Terms] OR (“Tobacco Control”[MeSH Terms] OR “Smoking Reduction”[MeSH Terms]) OR “Nicotine Replacement Therapy”[MeSH Terms]) AND (“outcome assessment, health care”[MeSH Terms] OR “quality assurance, health care”[MeSH Terms] OR “Treatment Outcome”[MeSH Terms] OR “Program Evaluation”[MeSH Terms] OR “Health Services Accessibility”[MeSH Terms]) AND (“Healthcare Disparities”[MeSH Terms] OR “Health Status Disparities”[MeSH Terms] OR “Health Inequities”[MeSH Terms] OR “Socioeconomic Disparities in Health”[MeSH Terms] OR (“Social Determinants of Health”[MeSH Terms] OR “Health Information Management”[MeSH Terms] OR “Health Impact Assessment”[MeSH Terms]) OR “Health Equity”[MeSH Terms] OR “Vulnerable Populations”[MeSH Terms] OR (“Minority Health”[MeSH Terms] OR “Race Factors”[MeSH Terms]))) AND (y_10[Filter]) | 50 | PubMed |
| ((‘tobacco use cessation’/exp OR ‘tobacco use cessation’ OR ‘smoking cessation’/exp OR ‘smoking cessation’ OR ‘tobacco control’/exp OR ‘tobacco control’ OR ‘smoking reduction’/exp OR ‘smoking reduction’ OR ‘nicotine replacement therapy’/exp OR ‘nicotine replacement therapy’) AND [2015,2016,2017,2018,2019,2020,2021,2022,2023,2024,2025]/py) AND ((‘outcome assessment, health care’/exp OR ‘outcome assessment, health care’ OR ‘quality assurance, health care’/exp OR ‘quality assurance, health care’ OR ‘treatment outcome’/exp OR ‘treatment outcome’ OR ‘program evaluation’/exp OR ‘program evaluation’ OR ‘health services accessibility’/exp OR ‘health services accessibility’) AND [2015,2016,2017,2018,2019,2020,2021,2022,2023,2024,2025]/py) AND ((‘healthcare disparities’/exp OR ‘healthcare disparities’ OR ‘health status disparities’/exp OR ‘health status disparities’ OR ‘health inequities’/exp OR ‘health inequities’ OR ‘socioeconomic disparities in health’/exp OR ‘socioeconomic disparities in health’ OR ‘social determinants of health’/exp OR ‘social determinants of health’ OR ‘health information management’/exp OR ‘health information management’ OR ‘health impact assessment’/exp OR ‘health impact assessment’ OR ‘health equity’/exp OR ‘health equity’ OR ‘vulnerable populations’/exp OR ‘vulnerable populations’ OR ‘minority health’/exp OR ‘minority health’ OR ‘race factors’/exp OR ‘race factors’) AND [2015,2016,2017,2018,2019,2020,2021,2022,2023,2024,2025]/py) | 936 | Embase |
| ((((TS = (smoking cessation)) OR TS = (Smoking Reduction)) OR TS = (Tobacco Control)) OR TS = (Tobacco Use Cessation)) OR TS = (Nicotine Replacement Therapy) and Preprint Citation Index (Exclude–Database) AND ((((TS = (Health Care Outcome Assessment)) OR TS = (Health Care Quality Assurance)) OR TS = (Treatment Outcome)) OR TS = (Program Evaluation)) OR TS = (Health Services Accessibility) and Preprint Citation Index (Exclude–Database) AND ((((((((((TS = (Healthcare Disparities)) OR TS = (Health Status Disparities)) OR TS = (Health Inequities)) OR TS = (Socioeconomic Disparities in Health)) OR TS = (Social Determinants of Health)) OR TS = (Health Information Management)) OR TS = (Health Impact Assessment)) OR TS = (Health Equity)) OR TS = (Vulnerable Populations)) OR TS = (Minority Health)) OR TS = (Race Factors) Preprint Citation Index (Exclude–Database) and 2015 or 2016 or 2017 or 2018 or 2019 or 2020 or 2021 or 2022 or 2023 or 2024 or 2025 (Publication Years) and Article or Review Article (Document Types) | 1426 | Web of Science |
| Section and Topic | Item # | Checklist Item | Location Where Item Is Reported |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | Line 2–3, Page 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | The abstract section was prepared accordingly. |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | Lines 63–91 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | Lines 91–98 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Lines 101–126 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | Lines 109–115 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Lines 109–115 and Appendix A Table A1 |
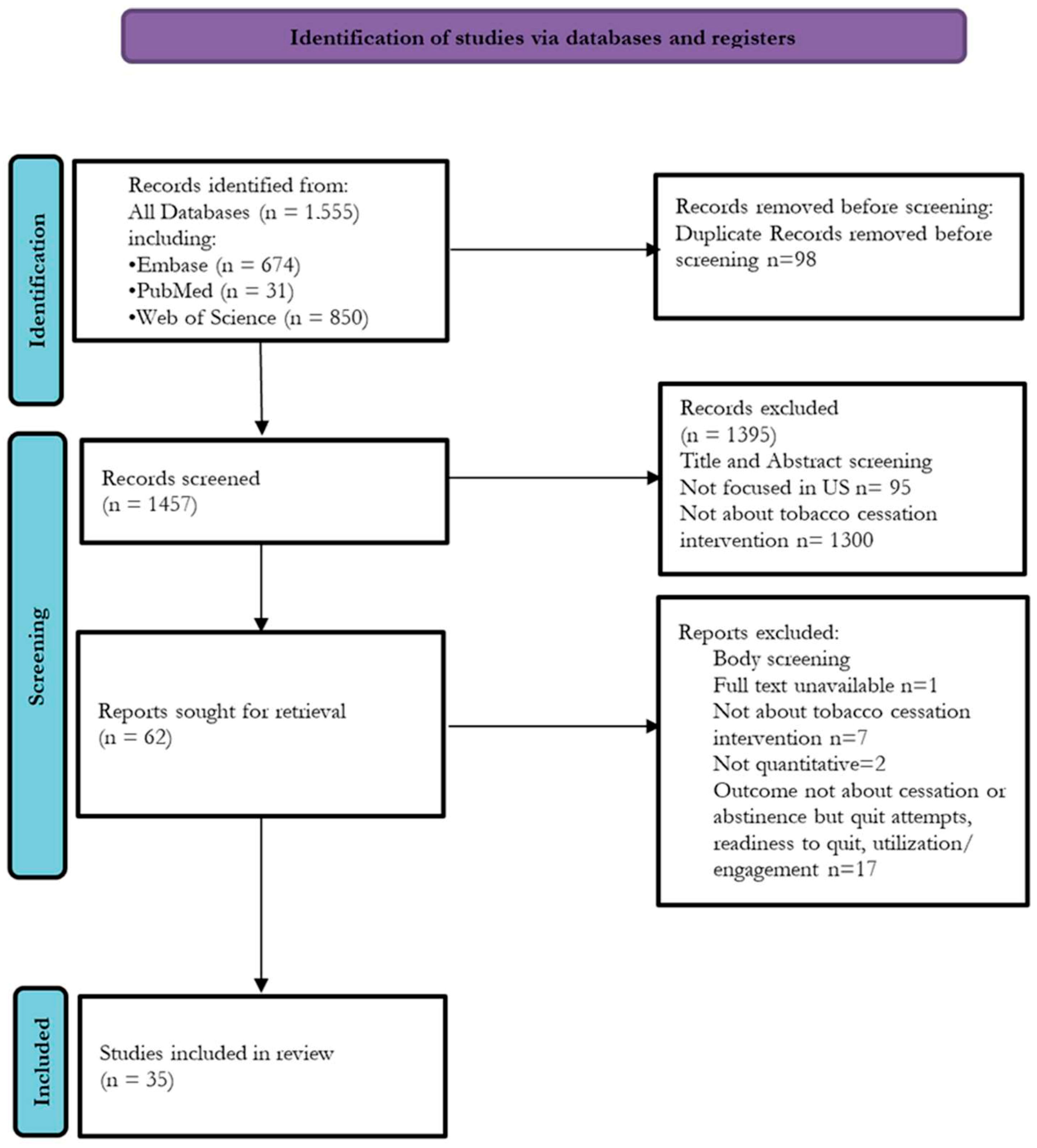
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | Lines 109–126 and Figure 1 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | Lines 109–126 and Figure 1 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | Table 1A and Table 2B |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | Table 1A and Table 2B | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | Lines 127–130 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | Table 1A and Table 2B |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | Lines 117–126 and Figure 1 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | NA | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | Table 1A and Table 2B | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | Lines 133–136 | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | NA | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | NA | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | Lines 133–136 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | NA |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Figure 1 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | Lines 143–147 | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Table 1A and Table 2B |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | Table 1A and Table 2B |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | Table 1A and Table 2B; Figure 1 |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | Table 1A and Table 2B |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | NA | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | Lines 320–344 | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | NA | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | NA |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | NA |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | Lines 377–390 |
| 23b | Discuss any limitations of the evidence included in the review. | Lines 391–399 | |
| 23c | Discuss any limitations of the review processes used. | Lines 391–399 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | Lines 401–411 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | Not registered |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | Not prepared | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | Not registered/not prepared | |
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | NA |
| Competing interests | 26 | Declare any competing interests of review authors. | NA |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | NA |
References
- Tobacco. World Health Organization. 2025. Available online: https://www.who.int/health-topics/tobacco#tab=tab_2 (accessed on 10 February 2025).
- Burden of Cigarette Use in the U.S. Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention. 2024. Available online: https://www.cdc.gov/tobacco/campaign/tips/resources/data/cigarette-smoking-in-united-states.html (accessed on 10 February 2025).
- Improving Tobacco-Related Health Disparities. National Center for Chronic Disease Prevention and Health Promotion; Office on Smoking and Health. Available online: https://www.cdc.gov/tobacco/tobacco-features/health-equity.html (accessed on 10 February 2025).
- Simmons, V.N.; Piñeiro, B.; Hooper, M.W.; Gray, J.E.; Brandon, T.H. Tobacco-Related Health Disparities Across the Cancer Care Continuum. Cancer Control 2016, 23, 434. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC5972388/ (accessed on 10 February 2025). [CrossRef] [PubMed]
- Marbin, J.; Balk, S.J.; Gribben, V.; Groner, J. Health disparities in tobacco use and exposure: A structural competency approach. Pediatrics 2021, 147, e2020040253. Available online: https://publications.aap.org/pediatrics/article/147/1/e2020040253/33415/Health-Disparities-in-Tobacco-Use-and-Exposure-A (accessed on 10 February 2025). [CrossRef] [PubMed]
- United States Public Health Service Office of the Surgeon General; National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health, Washington (DC). Interventions for Smoking Cessation and Treatments for Nicotine Dependence—Smoking Cessation—NCBI Bookshelf. In Smoking Cessation: A Report of the Surgeon General; US Department of Health and Human Services: Washington, DC, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK555596/ (accessed on 10 February 2025).
- Benefits of Quitting Smoking. National Center for Chronic Disease Prevention and Health Promotion; Office on Smoking and Health. Available online: https://www.cdc.gov/tobacco/about/benefits-of-quitting.html (accessed on 10 February 2025).
- Brooks, D.R.; Burtner, J.L.; Borrelli, B.; Heeren, T.C.; Evans, T.; Davine, J.A.; Greenbaum, J.; Scarpaci, M.; Kane, J.; Rees, V.W.; et al. Twelve-month outcomes of a group-randomized community health advocate-led smoking cessation intervention in public housing. Nicotine Tob. Res. 2018, 20, 1434–1441. [Google Scholar] [CrossRef] [PubMed]
- Chen Lyu, J.; Meacham, M.C.; Nguyen, N.; Ramo, D.; Ling, P.M. Factors Associated with Abstinence Among Young Adult Smokers Enrolled in a Real-world Social Media Smoking Cessation Program. Nicotine Tob. Res. 2024, 26, S27–S35. [Google Scholar]
- Hickman, N.J.; Delucchi, K.L.; Prochaska, J.J. Treating tobacco dependence at the intersection of diversity, poverty, and mental illness: A randomized feasibility and replication trial. Nicotine Tob. Res. 2015, 17, 1012–1021. [Google Scholar] [CrossRef]
- Kurti, A.N.; Tang, K.; Bolivar, H.A.; Evemy, C.; Medina, N.; Skelly, J.; Nighbor, T.; Higgins, S.T. Smartphone-based financial incentives to promote smoking cessation during pregnancy: A pilot study. Prev. Med. 2020, 140, 106201. [Google Scholar] [CrossRef]
- Bailey, S.R.; Marino, M.; Ezekiel-Herrera, D.; Schmidt, T.; Angier, H.; Hoopes, M.J.; DeVoe, J.E.; Heintzman, J.; Huguet, N. Tobacco Cessation in Affordable Care Act Medicaid Expansion States Versus Non-expansion States. Nicotine Tob. Res. 2020, 22, 1016–1022. Available online: https://academic.oup.com/ntr/article/22/6/1016/5498071 (accessed on 10 February 2025). [CrossRef] [PubMed]
- Thrul, J.; Meacham, M.C.; Tice, C.; Kelly, O.; Ramo, D.E. Live counselor contact in a facebook intervention predicts smoking cessation outcomes. Psychol. Addict. Behav. 2020, 34, 360–369. [Google Scholar] [CrossRef]
- Kreuter, M.W.; Garg, R.; Fu, Q.; Caburnay, C.; Thompson, T.; Roberts, C.; Sandheinricha, D.; Javeda, I.; Wolffa, J.M.; Butler, T.; et al. Helping low-income smokers quit: Findings from a randomized controlled trial comparing specialized quitline services with and without social needs navigation. Lancet Reg. Health–Am. 2023, 23, 100529. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L2025307733&from=export (accessed on 10 February 2025). [CrossRef]
- Pacek, L.R.; Joseph McClernon, F.; Bosworth, H.B. Adherence to pharmacological smoking cessation interventions: A literature review and synthesis of correlates and barriers. Nicotine Tob. Res. 2018, 20, 1163–1172. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L624465157&from=export (accessed on 10 February 2025). [CrossRef]
- Register, S.J.; Harrington, K.F.; Agne, A.A.; Cherrington, A.L. Effectiveness of Non-Primary Care-Based Smoking Cessation Interventions for Adults with Diabetes: A Systematic Literature Review. Curr. Diab. Rep. 2016, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kock, L.; Brown, J.; Hiscock, R.; Tattan-Birch, H.; Smith, C.; Shahab, L. Individual-level behavioural smoking cessation interventions tailored for disadvantaged socioeconomic position: A systematic review and meta-regression. Lancet Public Health 2019, 4, e628–e644. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L2004927263&from=export (accessed on 10 February 2025). [CrossRef] [PubMed]
- Patel, N.; Karimi, S.M.; Little, B.; Egger, M.; Antimisiaris, D. Applying Evidence Synthesis for Constructing Directed Acyclic Graphs to Identify Causal Pathways Affecting U.S. Early-Stage Non-Small Cell Lung Cancer Treatment Receipt and Overall Survival. Therapeutics 2024, 1, 64–94. [Google Scholar] [CrossRef]
- Dijk, S.W.; Caulley, L.M.; Hunink, M.; Labrecque, J. From complexity to clarity: How directed acyclic graphs enhance the study design of systematic reviews and meta-analyses. Eur. J. Epidemiol. 2024, 39, 27–33. Available online: https://link.springer.com/article/10.1007/s10654-023-01042-z. (accessed on 10 February 2025). [CrossRef]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC6148624/ (accessed on 10 February 2025). [CrossRef]
- Connected Papers. Available online: https://www.connectedpapers.com/ (accessed on 12 February 2025).
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC1756728/ (accessed on 10 February 2025). [CrossRef]
- Baggett, T.P.; Chang, Y.; Yaqubi, A.; McGlave, C.; Higgins, S.T.; Rigotti, N.A. Financial incentives for smoking abstinence in homeless smokers: A pilot randomized controlled trial. Nicotine Tob. Res. 2018, 20, 1442–1450. [Google Scholar] [CrossRef]
- Chen, C.; Anderson, C.M.; Babb, S.D.; Frank, R.; Wong, S.; Kuiper, N.M.; Zhu, S.H. Evaluation of the Asian Smokers’ Quitline: A Centralized Service for a Dispersed Population. Am. J. Prev. Med. 2021, 60, S154–S162. [Google Scholar] [CrossRef]
- Higgins, S.T.; Plucinski, S.; Orr, E.; Nighbor, T.D.; Coleman, S.R.M.; Skelly, J.; DeSarno, M.; Bunn, J. Randomized clinical trial examining financial incentives for smoking cessation among mothers of young children and possible impacts on child secondhand smoke exposure. Prev. Med. 2023, 176, 107651. [Google Scholar] [CrossRef]
- Hooper, M.W.; Miller, D.B.; Saldivar, E.; Mitchell, C.; Johnson, L.; Burns, M.; Huang, M.C. Randomized Controlled Trial Testing a Video-Text Tobacco Cessation Intervention Among Economically Disadvantaged African American Adults. Psychol. Addict. Behav. 2021, 35, 769–777. [Google Scholar] [CrossRef]
- Halpern, S.D.; French, B.; Small, D.S.; Saulsgiver, K.; Harhay, M.O.; Audrain-McGovern, J.; Loewenstein, G.; Brennan, T.A.; Asch, D.A.; Volpp, K.G.; et al. Randomized Trial of Four Financial-Incentive Programs for Smoking Cessation. N. Engl. J. Med. 2015, 372, 2108–2117. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L604555159&from=export (accessed on 10 February 2025). [CrossRef] [PubMed]
- Kendzor, D.E.; Businelle, M.S.; Frank-Pearce, S.G.; Waring, J.J.C.; Chen, S.; Hébert, E.T.; Swartz, M.D.; Alexander, A.C.; Sifat, M.S.; Boozary, L.K.; et al. Financial Incentives for Smoking Cessation among Socioeconomically Disadvantaged Adults: A Randomized Clinical Trial. JAMA Netw. Open. 2024, 7, e2418821. [Google Scholar] [CrossRef] [PubMed]
- Meernik, C.; McCullough, A.; Ranney, L.; Walsh, B.; Goldstein, A.O. Evaluation of Community-Based Cessation Programs: How Do Smokers with Behavioral Health Conditions Fare? Community Ment. Health J. 2018, 54, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Vidrine, D.J.; Frank-Pearce, S.G.; Vidrine, J.I.; Tahay, P.D.; Marani, S.K.; Chen, S.; Yuan, Y.; Cantor, S.B.; Prokhorov, A.V. Efficacy of Mobile Phone-Delivered Smoking Cessation Interventions for Socioeconomically Disadvantaged Individuals: A Randomized Clinical Trial. JAMA Intern. Med. 2019, 179, 167–174. [Google Scholar] [CrossRef]
- Bricker, J.B.; Santiago-Torres, M.; Mull, K.E.; Sullivan, B.M.; David, S.P.; Schmitz, J.; Stotts, A.; Rigotti, N.A. Do medications increase the efficacy of digital interventions for smoking cessation? Secondary results from the iCanQuit randomized trial. Addiction 2024, 119, 664–676. [Google Scholar] [CrossRef]
- Villanti, A.C.; Peasley-Miklus, C.; Cha, S.; Schulz, J.; Klemperer, E.M.; LePine, S.E.; West, J.C.; Mays, D.; Mermelstein, R.; Higgins, S.T.; et al. Tailored text message and web intervention for smoking cessation in U.S. socioeconomically-disadvantaged young adults: A randomized controlled trial. Prev. Med. 2022, 165, 107209. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L2019908359&from=export (accessed on 10 February 2025). [CrossRef]
- Heffner, J.L.; Mull, K.E.; Watson, N.L.; McClure, J.B.; Bricker, J.B. Long-Term smoking cessation outcomes for sexual minority versus nonminority smokers in a large randomized controlled trial of two web-based interventions. Nicotine Tob. Res. 2020, 22, 1596–1604. [Google Scholar] [CrossRef]
- Mays, D.; Johnson, A.C.; Phan, L.; Sanders, C.; Shoben, A.; Tercyak, K.P.; Wagener, T.L.; Brinkman, M.C.; Lipkus, I.M. Tailored Mobile Messaging Intervention for Waterpipe Tobacco Cessation in Young Adults: A Randomized Trial. Am. J. Public Health 2021, 111, 1685–1695. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L636002421&from=export (accessed on 10 February 2025). [CrossRef]
- Lee, M.; Miller, S.M.; Wen, K.Y.; Hui, S.K.A.; Roussi, P.; Hernandez, E. Cognitive-behavioral intervention to promote smoking cessation for pregnant and postpartum inner city women. J. Behav. Med. 2015, 38, 932–943. [Google Scholar] [CrossRef]
- Christiansen, B.A.; Reeder, K.M.; Terbeek, E.G.; Fiore, M.C.; Baker, T.B. Motivating low socioeconomic status smokers to accept evidence-based smoking cessation treatment: A brief intervention for the community agency setting. Nicotine Tob. Res. 2015, 17, 1002–1011. [Google Scholar] [CrossRef]
- Collins, B.N.; Nair, U.S.; Davis, S.M.; Rodriguez, D. Increasing home smoking restrictions boosts underserved MOMs’ bioverified quit success. Am. J. Health Behav. 2019, 43, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Graham, A.L.; Amato, M.S.; Cha, S.; Jacobs, M.A.; Bottcher, M.M.; Papandonatos, G.D. Effectiveness of a Vaping Cessation Text Message Program among Young Adult e-Cigarette Users: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 923–930. [Google Scholar] [CrossRef]
- Kamke, K.; Grenen, E.; Robinson, C.; El-Toukhy, S. Dropout and abstinence outcomes in a national text messaging smoking cessation intervention for pregnant women, smokefreemom: Observational study. JMIR mHealth uHealth 2019, 7, e14699. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L629551580&from=export (accessed on 10 February 2025). [CrossRef]
- Dahne, J.; Wahlquist, A.E.; Smith, T.T.; Carpenter, M.J. The differential impact of nicotine replacement therapy sampling on cessation outcomes across established tobacco disparities groups. Prev. Med. 2020, 136, 106096. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0091743520301201 (accessed on 10 February 2025). [CrossRef] [PubMed]
- Fu, S.S.; Van Ryn, M.; Nelson, D.; Burgess, D.J.; Thomas, J.L.; Saul, J.; Clothier, B.; Nyman, J.A.; Hammett, P.; Joseph, A.M. Proactive tobacco treatment offering free nicotine replacement therapy and telephone counselling for socioeconomically disadvantaged smokers: A randomised clinical trial. Thorax 2016, 71, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Galiatsatos, P.; Soybel, A.; Jassal, M.; Cruz, S.A.P.; Spartin, C.; Shaw, K.; Cunningham, J.; Kanarek, N.F. Tobacco treatment clinics in urban public housing: Feasibility and outcomes of a hands-on tobacco dependence service in the community. BMC Public Health. 2021, 21, 1514. [Google Scholar] [CrossRef]
- Lee, J.; Contrera Avila, J.; Ahluwalia, J.S. Differences in cessation attempts and cessation methods by race/ethnicity among US adult smokers, 2016–2018. Addict. Behav. 2023, 137, 107523. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L2020808761&from=export (accessed on 10 February 2025). [CrossRef]
- Kerkvliet, J.L.; Wey, H.; Fahrenwald, N.L. Cessation among state quitline participants with a mental health condition. Nicotine Tob. Res. 2015, 17, 735–741. [Google Scholar] [CrossRef]
- Wewers, M.E.; Shoben, A.; Conroy, S.; Curry, E.; Ferketich, A.K.; Murray, D.M.; Nemeth, J.; Wermert, A. Effectiveness of Two Community Health Worker Models of Tobacco Dependence Treatment Among Community Residents of Ohio Appalachia. Nicotine Tob. Res. 2017, 19, 1499–1507. [Google Scholar] [CrossRef]
- Hooper, M.W.; Calixte-Civil, P.; Verzijl, C.; Brandon, K.O.; Asfar, T.; Koru-Sengul, T.; Antoni, M.H.; Lee, D.J.; Simmons, V.N.; Brandon, T.H. Associations between perceived racial discrimination and tobacco cessation among diverse treatment seekers. Ethn. Dis. 2020, 30, 411–420. [Google Scholar] [CrossRef]
- McCarthy, D.E.; Baker, T.B.; Zehner, M.E.; Adsit, R.T.; Kim, N.; Zwaga, D.; Coates, K.; Wallenkamp, H.; Nolan, M.; Steiner, M.; et al. A comprehensive electronic health record-enabled smoking treatment program: Evaluating reach and effectiveness in primary care in a multiple baseline design. Prev. Med. 2022, 165, 107101. Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L2018636055&from=export (accessed on 10 February 2025). [CrossRef] [PubMed]
- Santiago-Torres, M.; Mull, K.E.; Sullivan, B.M.; Ferketich, A.K.; Bricker, J.B. Efficacy of an acceptance and commitment therapy-based smartphone application for helping rural populations quit smoking: Results from the iCanQuit randomized trial. Prev. Med. 2022, 157, 107008. [Google Scholar] [CrossRef] [PubMed]
- Santiago-Torres, M.; Mull, K.E.; Sullivan, B.M.; Kwon, D.M.; Nez Henderson, P.; Nelson, L.A.; Patten, C.A.; Bricker, J.B. Efficacy and Utilization of Smartphone Applications for Smoking Cessation among American Indians and Alaska Natives: Results from the iCanQuit Trial. Nicotine Tob. Res. 2022, 24, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Webb Hooper, M.; Kolar, S.K. Distress, race/ethnicity and smoking cessation in treatment-seekers: Implications for disparity elimination. Addiction 2015, 110, 1495–1504. [Google Scholar] [CrossRef]
| (A) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Author | Study Design | Intervention | Study Population | Sample Size | Identified Barriers | Identified Facilitators | Cessation Outcomes (Effect, 95% CI) | Quality Rating |
| Baggett et al. [23] | RCT | Financial Incentives with nicotine patch and counseling | Homeless smokers | 50 | Homelessness | Financial incentive | OR = 8.08 (95% CI: 3.35–19.5) | High |
| Brooks et al. [8] | RCT | Community advocate-led cessation | Public housing residents | 250 | Socioeconomically disadvantaged | Peer motivation and social support | OR = 2.98 (95% CI: 1.56–5.68) | High |
| Chen et al. [24] | Cohort | Asian language behavioral counseling+ NRT | Asian immigrants | 14,073 | Language barriers | Multilingual quitline services+ NRT/e-cigs | OR = 0.40 (95% CI: 0.36–0.45) | Moderate |
| Hickman et al. [10] | RCT | Transtheoretical model (TTM)-tailored, computer assisted intervention | Uninsured low SES smokers with mental illness | 100 | Financial constraints, mental illness | Tailored therapy | OR = 1.80 (95% CI: 0.74–4.38) | High |
| Higgins et al. [25] | RCT | Best practice + financial incentives + NRT | Mothers of children < 12 yrs old | 198 | Socioeconomically disadvantaged | NRT+ Incentive | OR = 5.88 (95% CI: 1.87–18.48) | High |
| Hooper, M.W. et al. [26] | RCT | Culturally adapted video–text tobacco cessation intervention+ NRT | Economically disadvantaged and African Americans | 119 | Digital inequities | High motivation, NRT | OR = 3.02 (95% CI: 0.53–7.37) | High |
| Halpern [27] | RCT | Financial incentive programs+ usual care + pharmacotherapy | General smokers | 2538 | Not identified | Incentives for abstinence | (OR = 2.27, 95% CI: 1.24–4.17) | High |
| Kendzor et al. [28] | RCT | Financial incentives for low-income adults+ usual care and medication | Socioeconomically disadvantaged smokers | 320 | Socioeconomic barriers | Financial rewards | OR = 3.18 (95% CI: 1.70–5.95) | High |
| Meernik et al. [29] | Cohort | Community-based cessation program + NRT/other medication | Smokers with behavioral health conditions | 974 | Mental health barriers | Integrated treatment services | OR = 1.15 (95% CI: 1.08–1.21) | Low |
| Vidrine et al. [30] | RCT | Mobile phone-delivered Cessation+ NRT | Socioeconomically disadvantaged smokers | 624 | Low motivation, socioeconomic barriers | NRT+ Text+ Call | RR = 2.11 (95% CI 1.00–4.48) | High |
| (B) | ||||||||
| Author | Study Design | Intervention | Study Population | Sample Size | Identified Barriers | Identified Facilitators | Cessation Outcomes (Effect, 95% CI) | Quality Rating |
| Bricker [31] | RCT | ACT-based smartphone app vs. standard app | General adult smokers | 2088 | Digital access, motivation variability | Self-paced engagement, behavioral support | (RR = 1.72, 95% CI: 1.45–2.05) | High |
| Villanti [32] | RCT | Tailored text message and web intervention | Socioeconomically disadvantaged young adults | 437 | Digital literacy barriers | Personalized messaging, motivational support | (RR = 1.09, 95% CI: 1.04–1.15) | High |
| Heffner [33] | RCT | Web+text-based cessation interventions | Sexual minority vs. nonminority smokers | 2637 | Minority stress, stigma | Not identified | (OR = 0.91, 95% CI: 0.65–1.28) | High |
| Mays et al. [34] | RCT | Tailored mobile messaging for waterpipe cessation | Young adult waterpipe smokers | 349 | Low motivation | Personalized SMS support | OR = 1.9 (95% CI: 1.1–3.3) | High |
| Lee, M. et al. [35] | RCT | Cognitive behavioral counseling Cessation | Pregnant and postpartum women | 277 | Psychological stress | CBC intervention | OR = 2.53 (95% CI: 1.21–5.28) | High |
| Christiansen et al. [36] | RCT | brief intervention in Wisconsin Salvation Army sites | Low SES smokers | 522 | Low motivation to quit | Community support | No significant difference between control and intervention | High |
| Collins et al. [37] | RCT | Behavioral counseling | Mother of young children < 4 years old | 300 | Household smoking exposure | Stricter indoor smoking restrictions | OR = 11.0 (95% CI: 6.3–19.2) | High |
| Graham et al. [38] | RCT | Vaping cessation interactive text messaging | Young adult e-cig smokers age 18–24 | 2588 | Low motivation | Mobile-based intervention | OR = 1.39 (95% CI: 1.15–1.68) | High |
| Kamke et al. [39] | Cohort | Text-based smoking cessation for pregnant women | Pregnant smokers | 1288 | Race, less than high school education, daily smokers | No racial significant difference | OR = 1.01 (95% CI: 0.57–1.78) | Moderate |
| (A) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Author | Study Design | Intervention | Study Population | Sample Size | Identified Barriers | Identified Facilitators | Cessation Outcomes Effect, 95% CI | Quality Rating |
| Dahne [40] | RCT | Nicotine replacement therapy sampling | General smokers | 1245 | Access barriers, race, income, rurality, education | Free provision, proactive encouragement | OR = 1.59 (95% CI: 0.97–2.59) | High |
| Fu et al. [41] | RCT | Proactive outreach tobacco treatment | Low-income smokers covered by Medicaid or MinnesotaCare | 2406 | Cost, low awareness, access, psychosocial | Free access, comprehensive treatment, e.g., NRT, behavioral counseling | OR = 1.47 (95% CI: 1.12–1.93) | High |
| Galiatsatos et al. [42] | Cohort | Tobacco clinics in public housing+ medication | Disadvantaged Public housing resident smokers | 47 | Stress, socioeconomic status | Community-based clinic support | 94.4% | Low |
| Lee, J. et al. [43] | Cohort | Cessation advice receipt | U.S. adult smokers | 6742 | Lack of provider engagement | Not identified | OR = 0.99 (95% CI: 0.95–1.00) | Low |
| Kerkvliet et al. [44] | Cohort | Quitline service + cessation treatment | Smokers with and without mental health issues | 4935 | Psychological barriers | Not identified | OR = 0.78 (95% CI: 0.68–0.89) | Moderate |
| Wewers et al. [45] | Cohort | Cessation treatment involving community health worker + NRT | Appalachian resident smokers | 707 | Low health resource rural area | Social support | OR = 1.04 (95% CI: 1.01, 1.06) | Low |
| (B) | ||||||||
| Author | Study Design | Intervention | Study Population | Sample Size | Identified Barriers | Identified Facilitators | Cessation Outcomes Effect, 95% CI | Quality Rating |
| Kurti et al. [11] | RCT | Smartphone-based incentives | Pregnant smokers | 30 | Not identified | Smartphone-based incentivized intervention | OR = 9.33 (95% CI: 1.87–46.68) | High |
| Bailey et al. [12] | Cohort | ACA Medicaid expansion cessation | Medicaid-insured smokers | Expansion = 27,670 Non-expansion = 27,670 | Limited access to healthcare due to insurance coverage | Medicaid expansion policies | OR = 1.35 (95% CI: 1.28–1.43) | High |
| Chen Lyu et al. [9] | Cohort | Social media-based cessation | Young adult smokers | 248 | Digital access barriers | Online peer support | OR = 2.6 (95% CI: 1.8–4.2) | High |
| Hooper, M.W. et al. [46] | RCT | Cessation treatment CBT/GHE | Treatment-seekers facing racial barriers | 347 | Racial discrimination | Coping response training | OR = 0.97 (95% CI: 0.94–0.99) | High |
| McCarthy et al. [47] | Cohort | EHR-enabled smoking treatment program | Primary care patients | 6672 | Access barriers | Automated prompts | OR = NP (95% CI: 2.2–10.5) | Moderate |
| Kreuter et al. [14] | RCT | Specialized quitline services with navigation | Low-income smokers | 1137 | Low awareness of NRT, lack of social support, financial | Specialized quitline compared to standard | OR = 0.70 (95% CI = 0.50–0.95) | High |
| Thrul [13] | RCT | Facebook-based live counseling | Young adult smokers aged 18–25 yrs | 251 | Low motivation and social support | Live counseling engagement | OR = 1.10 (95% CI 1.02–1.20) | High |
| Santiago-Torres et al. [48] | RCT | iCanQuit for American Indians and Alaska Natives | Indigenous smokers populations | 169 | Cultural barriers | Increase in acceptance of physical sensations, emotions, and thoughts | OR = 1.97 (95% CI: 0.92–4.25) | High |
| Santiago-Torres et al. [49] | RCT | ACT-based smartphone cessation | Rural smokers populations | 550 | Geographic isolation | Digital intervention | OR = 1.47 (95% CI: 0.96–2.27) | High |
| Webb Hooper et al. [50] | Observational | Cognitive-behavioral therapy (CBT) + 8 weeks nicotine patch (TNP) | Treatment-seeking smokers | 234 | Higher distress (perceived stress and depressive symptoms) | Reduction in distress via behavioral skills | OR = 0.93 (95% CI: 0.89–0.98) | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sultana, S.; Inungu, J.; Jahanfar, S. Barriers and Facilitators of Tobacco Cessation Interventions at the Population and Healthcare System Levels: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2025, 22, 825. https://doi.org/10.3390/ijerph22060825
Sultana S, Inungu J, Jahanfar S. Barriers and Facilitators of Tobacco Cessation Interventions at the Population and Healthcare System Levels: A Systematic Literature Review. International Journal of Environmental Research and Public Health. 2025; 22(6):825. https://doi.org/10.3390/ijerph22060825
Chicago/Turabian StyleSultana, Sanchita, Joseph Inungu, and Shayesteh Jahanfar. 2025. "Barriers and Facilitators of Tobacco Cessation Interventions at the Population and Healthcare System Levels: A Systematic Literature Review" International Journal of Environmental Research and Public Health 22, no. 6: 825. https://doi.org/10.3390/ijerph22060825
APA StyleSultana, S., Inungu, J., & Jahanfar, S. (2025). Barriers and Facilitators of Tobacco Cessation Interventions at the Population and Healthcare System Levels: A Systematic Literature Review. International Journal of Environmental Research and Public Health, 22(6), 825. https://doi.org/10.3390/ijerph22060825