

The Relationship Between Food Insecurity and Mental Health Among Syrians and Syrian Refugees Working in Agriculture During COVID-19

 , ,
, ,
Abstract
1. Introduction
Food (In)security and Mental Health

2. Materials and Methods
2.1. Study Design
2.2. Participant Recruitment
2.2.1. Household Survey
2.2.2. Researcher Interviews
2.3. Materials
2.3.1. Household Survey
2.3.2. Researcher Interviews
2.4. Data Analysis
2.4.1. Household Survey
2.4.2. Researcher Interviews
3. Results
3.1. Quantitative Analysis (Household Survey)
3.1.1. Correlation Analysis
3.1.2. Regression Analyses
3.2. Qualitative Analysis (Researcher Interviews)
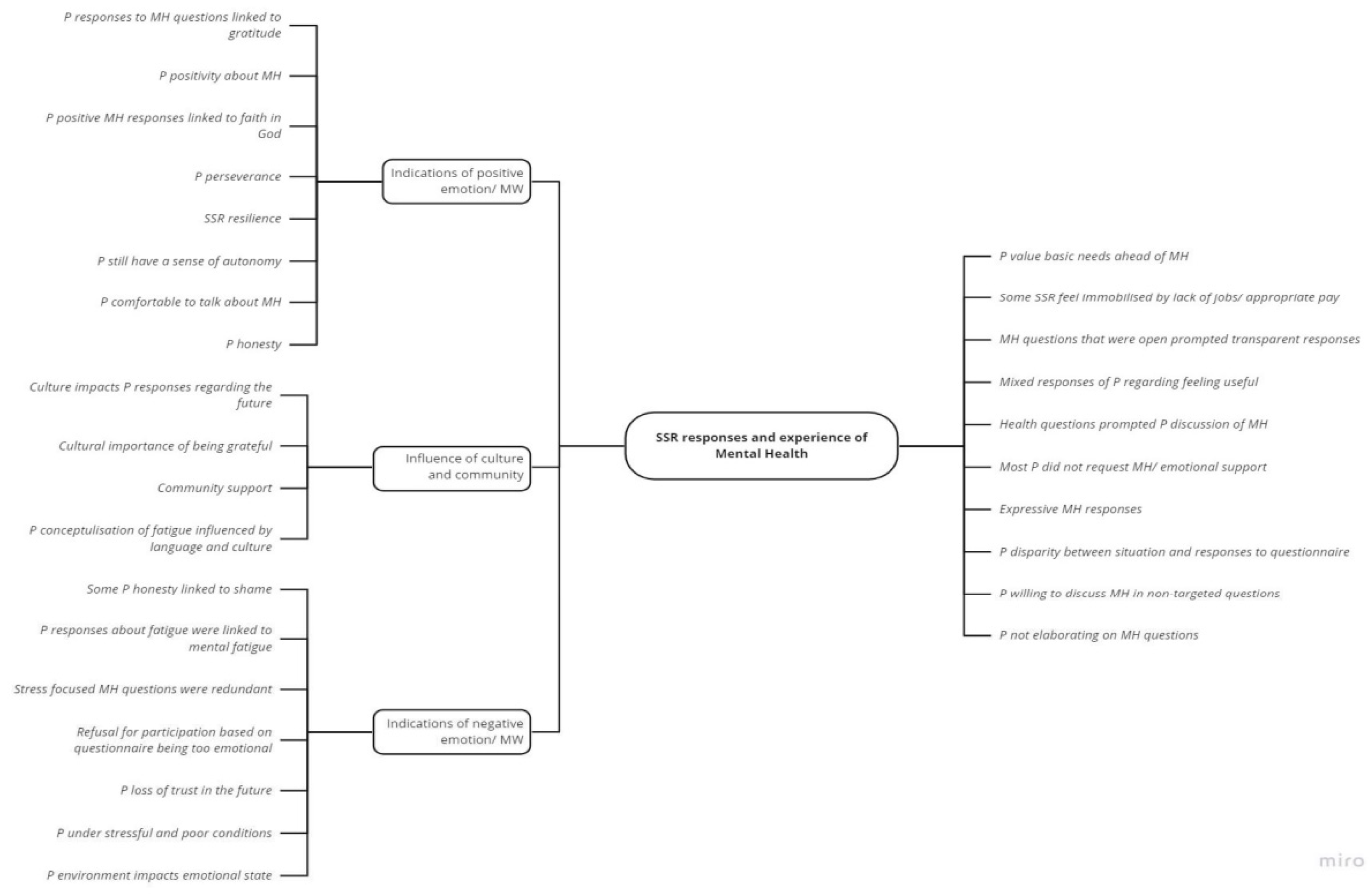
3.2.1. SSR Responses and Experiences of Mental Health
- Indications of positive emotion/well-being: Many SSRs expressed MH in positive terms, often linked to religious beliefs and a sense of resilience. However, there was a noted loss of trust in the future.
- Indications of negative emotion/well-being: Despite the general positive outlook, there were concerns about the future, especially regarding children’s well-being, reflecting the broader societal situations impacting the MH of SSRs. Similar sentiments were reported by long-term displaced Syrian refugees in Lebanon, who experienced anxiety, depression, hopelessness, sadness, and diminished self-worth.
- Influence of culture and community: Cultural and religious beliefs shaped how SSR participants expressed their mental health. A notable influence was the role of religious faith, which fostered a generally positive outlook despite challenges. Many participants emphasised gratitude towards God as a coping mechanism when faced with adversity, exemplified by expressions such as “thank God for what we have” (Interview 1). This perspective reflects the protective role of faith in providing comfort, hope, and meaning during times of hardship.
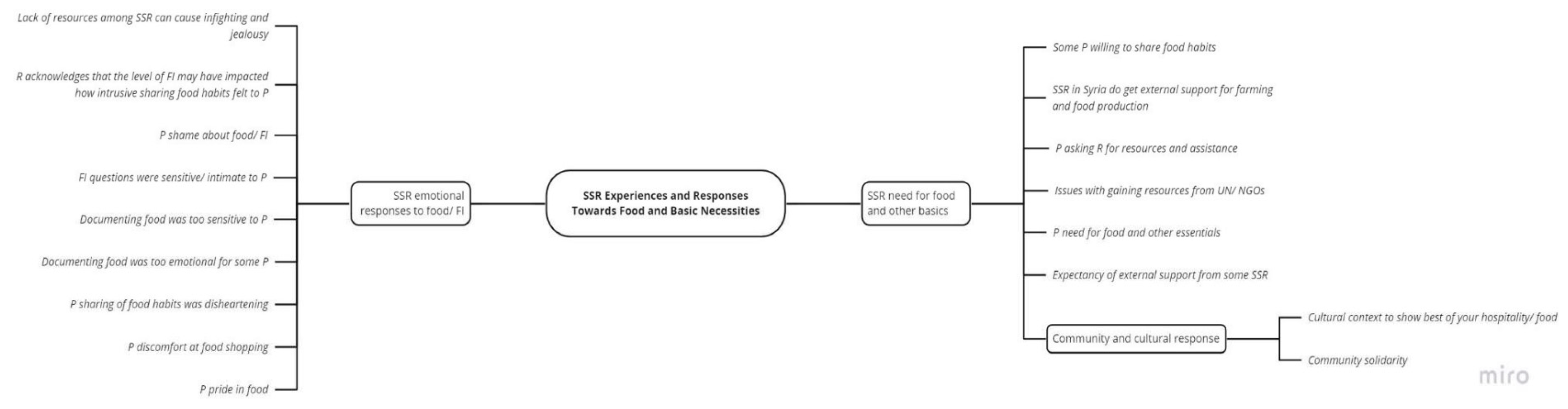
3.2.2. SSR Experiences and Responses Towards Food and Basic Necessities
- Emotional responses to FI/food: SSRs often expressed emotions an emotion-based approach when discussing food habits such as shame or distress. Nevertheless, others expressed pride in the nature of their cooking.
- SSR feed for food and other basics: This sub-theme highlighted the lack of availability of resources and SSR reliance on external bodies for support.
- Community and cultural responses: A sense of solidarity and camaraderie within the community. SSRs relied on community-based food distribution practices, and extended networks to mitigate food insecurity (such as relying on neighbours).
3.2.3. The Impact of COVID-19 and Other Social Issues on SSRs
- COVID-19 and additional economic issues: The impact of the pandemic was often overshadowed by pre-existing economic challenges, such as inflation. The pandemic merely exacerbated these difficulties.
- Work and financial changes: The impact of COVID-19 and the existing economic challenges that COVID-19 exacerbated were keenly observed through changes in work available to SSRs. Many Syrian refugees lost their jobs due to disruptions in agricultural supply chains and pandemic-related restrictions, exacerbating already precarious working conditions shaped by limited labour rights and legal ambiguity. While work was disrupted for many, some displaced people continued working as the beginning of the pandemic coincided with the start of the agricultural season in the Middle East.
- Debt: SSR communities were able to exhibit coping mechanisms, including resource-sharing, informal debt networks or getting a loan from an NGO to counteract the impact of the current economic issue. However, many respondents reported having nothing left to sell and no one to borrow from, indicating that their communities’ ability to cope with shocks had already been eroded before the pandemic.
- Regional differences: Some interviews referred to the current economic crisis in Lebanon as playing a significant role in impacting the lives of SSRs.
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CARA | Council for At-Risk Academics |
| CSI | Coping Strategy Index |
| FI | Food Insecurity |
| LMICs | Lower-/Middle-Income Countries |
| MH | Mental Health |
| MPCA | Multi-Purpose Cash Assistance |
| NGO | Non-Governmental Organisation |
| PPE | Personal Protective Equipment |
| SRs | Syrian Refugees |
| SSRs | Syrians and Syrian Refugees |
| SWEMWBS | Warwick–Edinburgh Mental Wellbeing Scale |
| UNHCR | United Nations High Commissioner for Refugees |
| USDA | The United States Department of Agriculture |
| WHO | World Health Organization |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n | M | SD | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|---|
| 6. MH | 100 | 25.58 | 4.25 | - | |||
| 7. C19p | 100 | 2.44 | 0.69 | −0.16 | - | ||
| 8. C19a | 100 | 8.76 | 2.81 | 0.09 | −0.09 | - | |
| 9. FI | 100 | 18.85 | 4.06 | −0.24 * | 0.29 ** | 0.15 | - |
| Variables | n | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. MH | 100 | 24.58 | 4.25 | - | ||||||||
| 2. C19p | 100 | 2.44 | 0.69 | −0.158 | - | |||||||
| 3. C19a | 100 | 8.76 | 2.81 | 0.086 | −0.092 | - | ||||||
| 4. FI | 100 | 18.85 | 4.06 | −0.237 * | 0.287 ** | 0.146 | - | |||||
| 5. No change | 100 | 1.96 | 0.20 | 0.004 | −0.116 | 0.031 | 0.086 | - | ||||
| 6. Storage of food | 100 | 1.45 | 0.50 | −0.206 * | 0.198 * | 0.028 | 0.208 * | −0.226 * | - | |||
| 7. Having smallerportions | 100 | 1.40 | 0.49 | 0.364 ** | −0.191 | 0.096 | −0.352 ** | −0.250 * | −0.123 | - | ||
| 8. Cleaning more than normal | 100 | 1.18 | 0.39 | −0.077 | 0.213 * | 0.124 | 0.099 | −0.436 ** | 0.361 ** | 0.043 | - | |
| 9. No visiting with family/ friends | 100 | 1.03 | 0.17 | −0.079 | 0.175 | −0.035 | −0.042 | −0.862 ** | 0.194 | 0.215 * | 0.375 ** | - |
| Variables | n | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. MH | 100 | 24.58 | 4.25 | - | |||||||||
| 2. C19p | 100 | 2.44 | 0.69 | −0.158 | - | ||||||||
| 3. C19a | 100 | 8.76 | 2.81 | 0.086 | −0.092 | - | |||||||
| 4. FI | 100 | 18.85 | 4.06 | −0.237 * | 0.287 ** | 0.146 | - | ||||||
| 5. No change | 100 | 1.97 | 0.17 | −0.088 | 0.015 | 0.046 | 0.152 | - | |||||
| 6. Information distribution | 100 | 1.57 | 0.50 | −0.074 | 0.077 | −0.258 ** | 0.027 | 0.084 | - | ||||
| 7. Organisation of food items | 100 | 1.54 | 0.50 | −0.086 | 0.150 | 0.012 | 0.017 | −0.045 | 0.049 | - | |||
| 8. Staying home | 100 | 1.11 | 0.31 | 0.084 | −0.047 | 0.143 | −0.094 | −0.313 ** | −0.017 | 0.068 | - | ||
| 9. No social gatherings | 100 | 1.08 | 0.27 | 0.066 | −0.070 | 0.024 | −0.070 | −0.164 | 0.033 | 0.198 * | 0.485 ** | - | |
| 10. Mosque announcements | 100 | 1.70 | 0.46 | 0.055 | 0.005 | −0.326 ** | −0.126 | 0.013 | 0.181 | −0.079 | 0.091 | 0.032 | - |

References
- Ayouni, I.; Maatoug, J.; Dhouib, W.; Zammit, N.; Fredj, S.B.; Ghammam, R.; Ghannem, H. Effective public health measures to mitigate the spread of COVID-19: A systematic review. BMC Public Health 2021, 21, 1015. [Google Scholar] [CrossRef]
- Kamalrathne, T.; Jayasinghe, N.; Fernando, N.; Amaratunga, D.; Haigh, R. Managing compound events in the COVID-19 era: A critical analysis of gaps, measures taken, and challenges. Int. J. Disaster Risk Reduct. 2024, 112, 104765. [Google Scholar] [CrossRef]
- Mendenhall, E. The COVID-19 syndemic is not global: Context matters. Lancet 2020, 396, 1731. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Bulled, N.; Ostrach, B.; Mendenhall, E. Syndemics and the biosocial conception of health. Lancet 2017, 389, 941–950. [Google Scholar] [CrossRef]
- Burke, J.; Abdulateef, S.; Boden, L.; Calia, C. Food Security and Mental Health Under the COVID-19 Syndemic. Humanitarian Practice Network. 2020. Available online: https://odihpn.org/blog/food-security-and-mental-health-under-the-covid-19-syndemic/ (accessed on 12 August 2024).
- Huizar, M.I.; Arena, R.; Laddu, D.R. The global food syndemic: The impact of food insecurity, Malnutrition and obesity on the healthspan amid the COVID-19 pandemic. Prog. Cardiovasc. Dis. 2021, 64, 107. [Google Scholar] [CrossRef]
- Nagata, J.M.; Seligman, H.K.; Weiser, S.D. Perspective: The Convergence of Coronavirus Disease 2019 (COVID-19) and Food Insecurity in the United States. Adv. Nutr. 2021, 12, 287–290. [Google Scholar] [CrossRef]
- Rod, M.H.; Rod, N.H. Towards a syndemic public health response to COVID-19 . Scand. J. Public Health 2021, 49, 14–16. [Google Scholar] [CrossRef]
- Yadav, U.N.; Rayamajhee, B.; Mistry, S.K.; Parsekar, S.S.; Mishra, S.K. A Syndemic Perspective on the Management of Non-communicable Diseases Amid the COVID-19 Pandemic in Low- and Middle-Income Countries. Front. Public Health 2020, 8, 508. [Google Scholar] [CrossRef]
- UNHCR. Refugee Statistics. Refugee Data Finder. Available online: https://www.unhcr.org/refugee-statistics/download?url=6CL09p (accessed on 12 August 2024).
- Faleh, H.M.H.; Ahmad, A.-Q.A.S. The impact of Syrian refugee crisis on neighboring countries. RUDN J. Pol. Scie. 2018, 20, 548–554. [Google Scholar]
- Gabiam, N. Humanitarianism, development, and security in the 21st century: Lessons from the Syrian refugee crisis. Int. J. Middle East Stud. 2016, 48, 382–386. [Google Scholar] [CrossRef]
- 3RP. Regional Strategic Overview. 2024. Available online: https://www.3rpsyriacrisis.org/wp-content/uploads/2024/03/3RP_RSO_2024_.pdf (accessed on 10 November 2024).
- UNICEF. Child Food Poverty Report. A Nutrition Crisis in Early Childhood in Lebanon. Available online: https://www.unicef.org/lebanon/reports/child-food-poverty-report (accessed on 12 August 2024).
- UNWFP. Syria—World Food Programm. Available online: https://www.wfp.org/emergencies/syria-emergency#:~:text=The%20country%20remains%20among%20the,risk%20of%20becoming%20food%20insecure (accessed on 12 August 2024).
- Karasapan, O.; Brookings. Syrian Refugees in Jordan: A Decade and Counting. 2022. Available online: https://www.brookings.edu/articles/syrian-refugees-in-jordan-a-decade-and-counting/ (accessed on 20 November 2024).
- UNICEF. Humanitarian Action for Children. Syrian Refugees. Available online: https://www.unicef.org/media/100936/file/2021-HAC-Syrian-Refugees-May-Update.pdf (accessed on 12 August 2024).
- Nabulsi, D.; Ismail, H.; Hassan, F.A.; Sacca, L.; Honein-AbouHaidar, G.; Jomaa, L. Voices of the vulnerable: Exploring the livelihood strategies, coping mechanisms and their impact on food insecurity, health and access to health care among Syrian refugees in the Beqaa region of Lebanon. PLoS ONE 2020, 15, e0242421. [Google Scholar] [CrossRef]
- Sawaya, T.; Ballouz, T.; Zaraket, H.; Rizk, N. Coronavirus Disease (COVID-19) in the Middle East: A Call for a Unified Response. Front. Public Health 2020, 8, 209. [Google Scholar] [CrossRef]
- Arciniegas Guaneme, I.; Guerisoli, E.; Guyot, L.; Kallergis, A. COVID-19 and Forcibly Displaced People: Addressing the Impacts and Responding to the Challenges. Reference Paper for the 70th Anniversary of the 1951 Refugee Convention. The New School for Social Research. Prepared for UNHCR. 2021. Available online: https://www.unhcr.org/people-forced-to-flee-book/ (accessed on 12 August 2024).
- Lupieri, S. Refugee Health During the COVID-19 Pandemic: A Review of Global Policy Responses. Risk Manag. Healthc. Policy 2021, 14, 1378. [Google Scholar] [CrossRef]
- Klema, M. Precarious Labour Under Lockdown. Available online: https://onehealthfieldnetwork.com/refugee-labour-under-lockdown (accessed on 12 August 2024).
- USDA Economic Research Service. Definitions of Food Security. Available online: https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security (accessed on 12 August 2024).
- Clemens, M.; Huang, C.; Graham, J. The Economic and Fiscal Effects of Granting Refugees Formal Labor Market Access (No. 496). 2018. Available online: www.cgdev.org (accessed on 22 August 2024).
- Marbach, M.; Hainmueller, J.; Hangartner, D. The long-term impact of employment bans on the economic integration of refugees. Sci. Adv. 2018, 4, eaap9519. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Dernini, S.; Berry, E.M. Coping with Food Insecurity Using the Sociotype Ecological Framework. Front. Nutr. 2018, 5, 107. [Google Scholar] [CrossRef]
- Ejiohuo, O.; Onyeaka, H.; Unegbu, K.C.; Chikezie, O.G.; Odeyemi, O.A.; Lawal, A.; Odeyemi, O.A. Nourishing the Mind: How Food Security Influences Mental Wellbeing. Nutrients 2024, 16, 501. [Google Scholar] [CrossRef]
- Smith, J.; Ker, S.; Archer, D.; Gilbody, S.; Peckham, E.; Hardman, C.A. Food insecurity and severe mental illness: Understanding the hidden problem and how to ask about food access during routine healthcare. BJPsych Adv. 2023, 29, 204–212. [Google Scholar] [CrossRef]
- Cantekin, D. Syrian Refugees Living on the Edge: Policy and Practice Implications for Mental Health and Psychosocial Wellbeing. Int. Migr. 2019, 57, 200–220. [Google Scholar] [CrossRef]
- Kamelkova, D. Food Insecurity and Its Association with Mental Health Among Syrian Refugees Resettled in Norway. Master’s Thesis, The University of Bergen, Bergen, Norway, 2021. [Google Scholar]
- Karaman, M.A.; Ricard, R.J. Meeting the mental health needs of Syrian refugees in Turkey. Prof. Couns. 2016, 6, 318. [Google Scholar] [CrossRef]
- M’zah, S.; Lopes Cardozo, B.; Evans, D.P. Mental Health Status and Service Assessment for Adult Syrian Refugees Resettled in Metropolitan Atlanta: A Cross-Sectional Survey. J. Immigr. Minor. Health 2019, 21, 1019–1025. [Google Scholar] [CrossRef]
- Hassan, G.; Ventevogel, P.; Jefee-Bahloul, H.; Barkil-Oteo, A.; Kirmayer, L.J. Mental health and psychosocial wellbeing of Syrians affected by armed conflict. Epidemiol. Psychiatr. Sci. 2016, 25, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Bruening, M.; Dinour, L.M.; Rosales Chavez, J.B. Food insecurity and emotional health in the USA: A systematic narrative review of longitudinal research. Public Health Nutr. 2017, 20, 3200–3208. [Google Scholar] [CrossRef] [PubMed]
- Maynard, M.; Andrade, L.; Packull-McCormick, S.; Perlman, C.M.; Leos-Toro, C.; Kirkpatrick, S.I. Food insecurity and mental health among females in high income countries. Int. J. Environ. Res. Public Health 2018, 15, 1424. [Google Scholar] [CrossRef] [PubMed]
- Narvaez, A.; Goudie, S.; The Food Foundation. Pushed to the Brink: The UK’s Interlinked Mental Health and Food Insecurity Crises. 2024. Available online: https://foodfoundation.org.uk/publication/pushed-brink-link-between-food-insecurity-and-mental-health (accessed on 2 September 2024).
- Pourmotabbed, A.; Moradi, S.; Babaei, A.; Ghavami, A.; Mohammadi, H.; Jalili, C.; Symonds, M.E.; Miraghajani, M. Food insecurity and mental health: A systematic review and meta-analysis. Public Health Nutr. 2020, 23, 1778–1790. [Google Scholar] [CrossRef]
- Cai, J.; Parker, M.; Tekwe, C.; Bidulescu, A. Food insecurity and mental health among US adults during the COVID-19 pandemic: Results from National Health Interview Survey, 2020–2021. J. Affect. Disord. 2024, 356, 707–714. [Google Scholar] [CrossRef]
- Talham, C.J.; Williams, F. Household food insecurity during the COVID-19 pandemic is associated with anxiety and depression among US- and foreign-born adults: Findings from a nationwide survey. J. Affect. Disord. 2023, 336, 126–132. [Google Scholar] [CrossRef]
- Fang, D.; Thomsen, M.R.; Nayga, R.M., Jr. The association between food insecurity and mental health during the COVID-19 pandemic. BMC Public Health 2021, 21, 607. [Google Scholar] [CrossRef]
- Elgar, F.J.; Pickett, W.; Pförtner, T.-K.; Gariépy, G.; Gordon, D.; Georgiades, K.; Davison, C.; Hammami, N.; MacNeil, A.; Da Silva, M.A.; et al. Relative food insecurity, mental health and wellbeing in 160 countries. Soc. Sci. Med. 2020, 268, 113556. [Google Scholar] [CrossRef]
- Calia, C.; Chakrabarti, A.; Sarabwe, E.; Chiumento, A. Maximising impactful and locally relevant mental health research: Ethical considerations. Wellcome Open Res. 2022, 7, 240. [Google Scholar] [CrossRef]
- Zuntz, A.; Klema, M.; Abdullateef, S.; Mazeri, S.; Alnabolsim, S.; Alfadel, A.; Abi-habib, J.; Azar, M.; Calia, C.; Burke, J.; et al. Syrian refugee labour and food insecurity in Middle Eastern agriculture during the early COVID-19 pandemic. Int. Labour Rev. 2021, 161, 245–266. [Google Scholar] [CrossRef]
- Drysdale, R.E.; Moshabela, M.; Bob, U. Adapting the Coping Strategies Index to measure food insecurity in the rural district of iLembe, South Africa. Food Cult. Soc. 2018, 22, 95–110. [Google Scholar] [CrossRef]
- Fat, L.N.; Scholes, S.; Boniface, S.; Mindell, J.; Stewart-Brown, S. Evaluating and establishing national norms for mental wellbeing using the short Warwick-Edinburgh Mental Well-being Scale (SWEMWBS): Findings from the Health Survey for England. Qual. Life Res. 2017, 26, 1129–1144. [Google Scholar] [CrossRef]
- Maxwell, D.; Caldwell, R. The Coping Strategies Index Field Methods Manual, 2nd ed.; WFP, CARE, Eds.; Cooperative for Assistance and Relief Everywhere, Inc. (CARE): Atlanta, GA, USA, 2008; Available online: https://documents.wfp.org/stellent/groups/public/documents/manual_guide_proced/wfp211058.pdf (accessed on 18 September 2024).
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [PubMed]
- Dhakal, K. NVivo. JMLA 2022, 110, 270–272. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Couns. Psychother. Res. 2021, 21, 37–47. [Google Scholar] [CrossRef]
- Pringle, J.; Drummond, J.; McLafferty, E.; Hendry, C. Interpretative phenomenological analysis: A discussion and critique. Nurse Res. 2011, 18, 20–24. [Google Scholar] [CrossRef]
- Koenig, H.G. Research on religion, spirituality, and mental health: A review. Can. J. Psychiatry. Rev. Can. Psychiatr. 2009, 54, 283–291. [Google Scholar] [CrossRef]
- Levin, J. Religion and mental health: Theory and research. Int. J. Appl. Psychoanal. Stud. 2010, 7, 102–115. [Google Scholar] [CrossRef]
- Papaleontiou-Louca, E. Effects of Religion and Faith on Mental Health. New Ideas Psychol. 2021, 60, 100833. [Google Scholar] [CrossRef]
- Sandage, S.; Hill, P.; Vaubel, D. Generativity, relational spirituality, gratitude, and mental health: Relationships and pathways. Int. J. Psychol. Relig. 2011, 21, 1–16. [Google Scholar] [CrossRef]
- Aghababaei, N.; Tabik, M.T. Gratitude and mental health: Differences between religious and general gratitude in a Muslim context. Ment. Health Relig. Cult. 2013, 16, 761–766. [Google Scholar] [CrossRef]
- Syam, H.; Venables, E.; Sousse, B.; Severy, N.; Saavedra, L.; Kazour, F. With every passing day I feel like a candle, melting little by little. experiences of long-term displacement amongst Syrian refugees in Shatila, Lebanon. Confl. Health 2019, 13, 45. [Google Scholar] [CrossRef] [PubMed]
- Umer, M.; Lazarte Elliot, D. Being Hopeful: Exploring the Dynamics of Posttraumatic Growth and Hope in Refugees. J. Refug. Stud. 2019, 34, 953–975. [Google Scholar] [CrossRef]
- Pasha, S. Developmental Humanitarianism, Resilience and (Dis)Empowerment In A Syrian Refugee Camp. J. Int. Dev. 2019, 32, 244–259. [Google Scholar] [CrossRef]
- Fratzke, S.; Migration Policy Institute Europe. Engaging Communities in Refugee Protection: The Potential of Private Sponsorship in Europe. 2017. Issue No. 9. Available online: https://www.migrationpolicy.org/sites/default/files/publications/PrivateSponsorshipEurope-Fratzke_FINALWEB.pdf (accessed on 25 August 2024).
- Yohani, S.; Kirova, A.; Georgis, R.; Gokiert, R.; Mejia, T.; Chiu, Y. Cultural Brokering with Syrian Refugee Families with Young Children: An Exploration of Challenges and Best Practices in Psychosocial Adaptation. J. Int. Migr. Integr. 2019, 20, 1181–1202. [Google Scholar] [CrossRef]
- Glanville, L. Resilience and Domination: Resonances of Racial Slavery in Refugee Exclusion. Int. Stud. Q. 2024, 68, sqae116. [Google Scholar] [CrossRef]
- Bargués, P.; Schmidt, J. Resilience and the Rise of Speculative Humanitarianism: Thinking Difference through the Syrian Refugee Crisis. Millennium 2021, 49, 197–223. [Google Scholar] [CrossRef]
- Bahar Özvarış, Ş.; Kayı, İ.; Mardin, D.; Sakarya, S.; Ekzayez, A.; Meagher, K.; Patel, P. COVID-19 barriers and response strategies for refugees and undocumented migrants in Turkey. J. Migr. Health 2020, 1, 100012. [Google Scholar] [CrossRef]
- Hopman, J.; Allegranzi, B.; Mehtar, S. Managing COVID-19 in Low- and Middle-Income Countries. JAMA 2020, 323, 1549–1550. [Google Scholar] [CrossRef]
- Khoury, P.; Azar, E.; Hitti, E. COVID-19 Response in Lebanon: Current Experience and Challenges in a Low-Resource Setting. JAMA 2020, 324, 548–549. [Google Scholar] [CrossRef]
- Nott, D. The COVID-19 response for vulnerable people in places affected by conflict and humanitarian crises. Lancet 2020, 395, 1532–1533. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.; Bherwani, H.; Gulia, S.; Vijay, R.; Kumar, R. Understanding COVID-19 transmission, health impacts and mitigation: Timely social distancing is the key. Environ. Dev. Sustain. 2020, 23, 6681–6697. [Google Scholar] [CrossRef] [PubMed]
- Horton, R. Offline: COVID-19 is not a pandemic. Lancet 2020, 396, 874. [Google Scholar] [CrossRef]
- Reimold, A.E.; Grummon, A.H.; Taillie, L.S.; Brewer, N.T.; Rimm, E.B.; Hall, M.G. Barriers and facilitators to achieving food security during the COVID-19 pandemic. Prev. Med. Rep. 2021, 23, 101500. [Google Scholar] [CrossRef]
- Barrett, C.B. Measuring Food Security. Science 2010, 327, 825–828. [Google Scholar] [CrossRef]
- Davis, A.K.; Barrett, F.S.; Griffiths, R.R. Psychological flexibility mediates the relations between acute psychedelic effects and subjective decreases in depression and anxiety. J. Context. Behav. Sci. 2020, 15, 39–45. [Google Scholar] [CrossRef]
- Erokhin, V.; Gao, T. Impacts of COVID-19 on Trade and Economic Aspects of Food Security: Evidence from 45 Developing Countries. Int. J. Environ. Res. Public Health 2020, 17, 5775. [Google Scholar] [CrossRef]
- Ma, N.L.; Peng, W.; Soon, C.F.; Noor Hassim, M.F.; Misbah, S.; Rahmat, Z.; Yong WT, L.; Sonne, C. COVID-19 pandemic in the lens of food safety and security. Environ. Res. 2021, 193, 110405. [Google Scholar] [CrossRef]
- Allahi, F.; Fateh, A.; Revetria, R.; Cianci, R. The COVID-19 epidemic and evaluating the corresponding responses to crisis management in refugees: A system dynamic approach. J. Humanit. Logist. Supply Chain Manag. 2021, 11, 347–366. [Google Scholar] [CrossRef]
- Dempster, H.; Ginn, T.; Graham, J.; Guerrero Ble, M.; Jayasinghe, D.; Shorey, B. Locked Down and Left Behind: The Impact of COVID-19 on Refugees’ Economic Inclusion. Policy Paper 179. Center for Global Development, Refugees International, and International Rescue Committee. 2020, pp. 1–44. Available online: https://www.cgdev.org/publication/locked-down-and-left-behind-impact-covid-19-refugees-economic-inclusion (accessed on 25 August 2024).
- Sumner, A.; Hoy, C.; Ortiz-Juarez, E. Estimates of the Impact of COVID-19 on Global Poverty. UNU-WIDER. 2020. Available online: https://www.econstor.eu/handle/10419/229267 (accessed on 25 August 2024).
- Woertz, E. COVID-19 in the Middle East and North Africa: Reactions, Vulnerabilities, Prospects 2020. (GIGA Focus Nahost, 2). Hamburg: GIGA German Institute of Global and Area Studies—Leibniz-Institut für Globale und Regionale Studien, Institut für Nahost-Studien. Available online: https://nbn-resolving.org/urn:nbn:de:0168-ssoar-67334-7 (accessed on 25 August 2024).
- El-Khatib, Z.; Al Nsour, M.; Khader, Y.S.; Abu Khudair, M. Mental health support in Jordan for the general population and for the refugees in the Zaatari camp during the period of COVID-19 lockdown. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 514. [Google Scholar] [CrossRef]
- Hagen-Zanker, J.; Both, N. Social Protection Provisions to Refugees During the COVID-19 Pandemic Lessons Learned from Government and Humanitarian Responses 2021, (No. 612). Available online: https://odi.org/en/publications/social-protection-provisions-to-refugees-during-the-covid-19-pandemic-lessons-learned-from-government-and-humanitarian-responses/ (accessed on 28 August 2024).
 ), their emerging sub-themes (
), their emerging sub-themes ( ) and how they interact (- - - - -). The figure depicts how sub-themes relate to larger themes and the potential interaction between themes as well. Note how the theme “SSR Responses and Experiences of Mental Health” is connected to the theme “SSR Experiences and Responses Towards Food and Basic Necessities” through sub-theme “SSR responses to Food/FI”.
), their emerging sub-themes () and how they interact (- - - - -). The figure depicts how sub-themes relate to larger themes and the potential interaction between themes as well. Note how the theme “SSR Responses and Experiences of Mental Health” is connected to the theme “SSR Experiences and Responses Towards Food and Basic Necessities” through sub-theme “SSR responses to Food/FI”.
) and how they interact (- - - - -). The figure depicts how sub-themes relate to larger themes and the potential interaction between themes as well. Note how the theme “SSR Responses and Experiences of Mental Health” is connected to the theme “SSR Experiences and Responses Towards Food and Basic Necessities” through sub-theme “SSR responses to Food/FI”.
), their emerging sub-themes () and how they interact (- - - - -). The figure depicts how sub-themes relate to larger themes and the potential interaction between themes as well. Note how the theme “SSR Responses and Experiences of Mental Health” is connected to the theme “SSR Experiences and Responses Towards Food and Basic Necessities” through sub-theme “SSR responses to Food/FI”.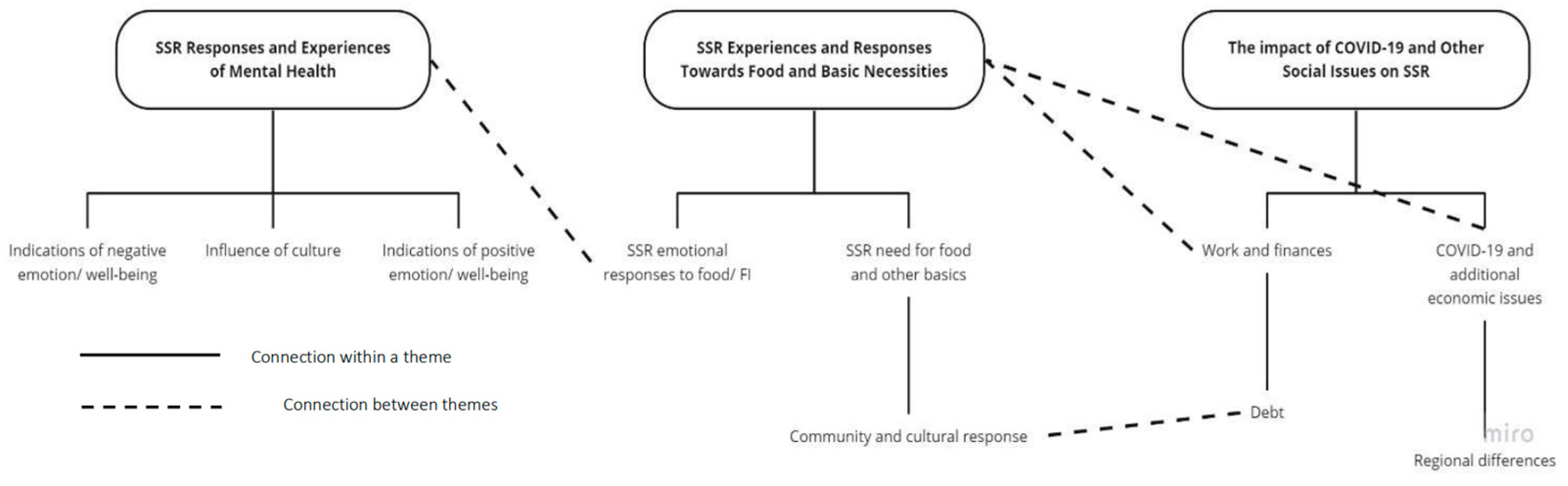
| Variable | B | 95% CI for B | SE B | β | R2 | ∆R2 | |
|---|---|---|---|---|---|---|---|
| LL | UL | ||||||
| Step 1 | 0.09 | 0.092 * | |||||
| Constant | 29.25 *** | 24.38 | 34.12 | 2.45 | |||
| C19p | −1.09 | −2.35 | 0.17 | 0.64 | −0.18 | ||
| C19a | 0.18 | −0.12 | 0.47 | 0.15 | 0.12 | ||
| FI | −0.19 | −0.40 | 0.03 | 0.11 | −0.18 | ||
| Step 2 | 0.09 | 0.001 | |||||
| Constant | 29.39 *** | 24.39 | 34.39 | 2.52 | |||
| C19p | −1.12 | −2.41 | 0.17 | 0.65 | −0.18 | ||
| C19a | 0.17 | −0.13 | 0.47 | 0.15 | 0.11 | ||
| FI | −0.19 | −0.41 | 0.03 | 0.11 | −0.18 | ||
| FI × C19a | 0.11 | −0.71 | 0.93 | 0.42 | 0.03 | ||
| Step 3 | 0.09 | 0.000 | |||||
| Constant | 29.32 *** | 24.14 | 34.49 | 2.61 | |||
| C19p | −1.10 | −2.44 | 0.23 | 0.67 | −0.18 | ||
| C19a | 0.17 | −0.14 | 0.48 | 0.16 | 0.11 | ||
| FI | −0.19 | −0.41 | 0.03 | 0.11 | −0.18 | ||
| FI × C19a | 0.13 | −0.74 | 0.99 | 0.44 | 0.03 | ||
| FI × C19p | −0.05 | −0.91 | 0.81 | 0.43 | −0.01 | ||
| Step 4 | 0.09 | 0.000 | |||||
| Constant | 29.29 *** | 24.07 | 34.51 | 2.63 | |||
| C19p | −1.09 | −2.46 | 0.29 | 0.69 | −0.18 | ||
| C19a | 0.18 | −0.14 | 0.50 | 0.16 | 0.12 | ||
| FI | −0.19 | −0.41 | 0.03 | 0.11 | −0.18 | ||
| FI × C19a | 0.10 | −0.89 | 1.08 | 0.49 | 0.02 | ||
| FI × C19p | −0.07 | −1.02 | 0.88 | 0.48 | −0.02 | ||
| C19a × C19p | 0.06 | −1.01 | 1.13 | 0.54 | 0.01 | ||
| Step 5 | 0.09 | 0.001 | |||||
| Constant | 29.73 *** | 23.74 | 35.72 | 3.02 | |||
| C19p | −1.16 | −2.64 | 0.31 | 0.74 | −0.19 | ||
| C19a | 0.15 | −0.21 | 0.51 | 0.18 | 0.10 | ||
| FI | −0.19 | −0.42 | 0.032 | 0.11 | −0.19 | ||
| FI × C19a | 0.09 | −0.90 | 1.01 | 0.50 | 0.02 | ||
| FI × C19p | −0.10 | −1.08 | 0.88 | 0.49 | −0.03 | ||
| C19a × C19p | −0.03 | −1.25 | 1.19 | 0.62 | −0.01 | ||
| FI × C19a × C19p | 0.14 | −0.77 | 1.05 | 0.46 | 0.05 | ||
| Variable | B | 95% CI for B | SE B | β | R2 | ∆R2 | |
|---|---|---|---|---|---|---|---|
| LL | UL | ||||||
| Step 1 | 0.13 | 0.131 ** | |||||
| Constant | 24.80 *** | 19.08 | 30.51 | 2.88 | |||
| FI | −0.10 | −0.31 | 0.12 | 0.11 | −0.09 | ||
| SP | 2.33 ** | 0.58 | 4.08 | 0.88 | 0.27 | ||
| SF | −1.14 | −2.78 | 0.50 | 0.83 | −0.13 | ||
| Step 2 | 0.14 | 0.009 | |||||
| Constant | 25.44 *** | 19.58 | 31.29 | 2.95 | |||
| FI | −0.12 | −0.34 | 0.10 | 0.11 | −0.11 | ||
| SP | 2.12 * | 0.32 | 3.91 | 0.90 | 0.25 | ||
| SF | −1.21 | −2.86 | 0.44 | 0.83 | −0.14 | ||
| FI × SP | −0.47 | −1.40 | 0.46 | 0.47 | −0.10 | ||
| Step 3 | 0.14 | 0.001 | |||||
| Constant | 25.43 *** | 19.55 | 31.31 | 2.96 | |||
| FI | −0.12 | −0.34 | 0.10 | 0.11 | −0.12 | ||
| SP | 2.13 * | 0.32 | 3.93 | 0.91 | 0.25 | ||
| SF | −1.22 | −2.88 | 0.44 | 0.84 | −0.14 | ||
| FI × SP | −0.49 | −1.43 | 0.45 | 0.47 | −0.10 | ||
| FI × SF | 0.13 | −0.71 | 0.97 | 0.42 | 0.3 | ||
| Step 4 | 0.14 | 0.000 | |||||
| Constant | 25.45 *** | 19.52 | 31.39 | 3.00 | |||
| FI | −0.12 | −0.34 | 0.10 | 0.11 | −0.12 | ||
| SP | 2.12 * | 0.30 | 3.94 | 0.917 | 0.25 | ||
| SF | −1.22 | −2.88 | 0.45 | 0.84 | −0.14 | ||
| FI × SP | −0.48 | −1.45 | 0.48 | 0.49 | −0.10 | ||
| FI × SF | 0.11 | −0.80 | 1.03 | 0.46 | 0.03 | ||
| SP × SF | −0.04 | −0.95 | 8.71 | 0.46 | −0.01 | ||
| Step 5 | 0.14 | 0.001 | |||||
| Constant | 25.53 *** | 19.54 | 31.51 | 3.01 | |||
| FI | −0.13 | −0.36 | 0.10 | 0.12 | −0.12 | ||
| SP | 2.06 * | 0.19 | 3.94 | 0.94 | 0.24 | ||
| SF | −1.11 | −2.94 | 0.72 | 0.92 | −0.13 | ||
| FI × SP | −0.50 | −1.48 | 0.47 | 0.49 | −0.10 | ||
| FI × SF | 0.14 | −0.80 | 1.07 | 0.47 | 0.03 | ||
| SP × SF | −0.01 | −0.94 | 0.92 | 0.47 | −0.00 | ||
| FI × SP × SF | 0.14 | −0.82 | 1.11 | 4.9 | 0.03 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calia, C.; El-Gayar, A.; Zuntz, A.-C.; Abdullateef, S.; Almashhor, E.; Grant, L.; Boden, L. The Relationship Between Food Insecurity and Mental Health Among Syrians and Syrian Refugees Working in Agriculture During COVID-19. Int. J. Environ. Res. Public Health 2025, 22, 549. https://doi.org/10.3390/ijerph22040549
Calia C, El-Gayar A, Zuntz A-C, Abdullateef S, Almashhor E, Grant L, Boden L. The Relationship Between Food Insecurity and Mental Health Among Syrians and Syrian Refugees Working in Agriculture During COVID-19. International Journal of Environmental Research and Public Health. 2025; 22(4):549. https://doi.org/10.3390/ijerph22040549
Chicago/Turabian StyleCalia, Clara, Afnan El-Gayar, Ann-Christin Zuntz, Shaher Abdullateef, Esraa Almashhor, Liz Grant, and Lisa Boden. 2025. "The Relationship Between Food Insecurity and Mental Health Among Syrians and Syrian Refugees Working in Agriculture During COVID-19" International Journal of Environmental Research and Public Health 22, no. 4: 549. https://doi.org/10.3390/ijerph22040549
APA StyleCalia, C., El-Gayar, A., Zuntz, A.-C., Abdullateef, S., Almashhor, E., Grant, L., & Boden, L. (2025). The Relationship Between Food Insecurity and Mental Health Among Syrians and Syrian Refugees Working in Agriculture During COVID-19. International Journal of Environmental Research and Public Health, 22(4), 549. https://doi.org/10.3390/ijerph22040549