





The Impact of Social Isolation on the Subjective Well-Being of Older People in China: An Empirical Analysis Based on the 2021 China General Social Survey
Abstract
1. Introduction
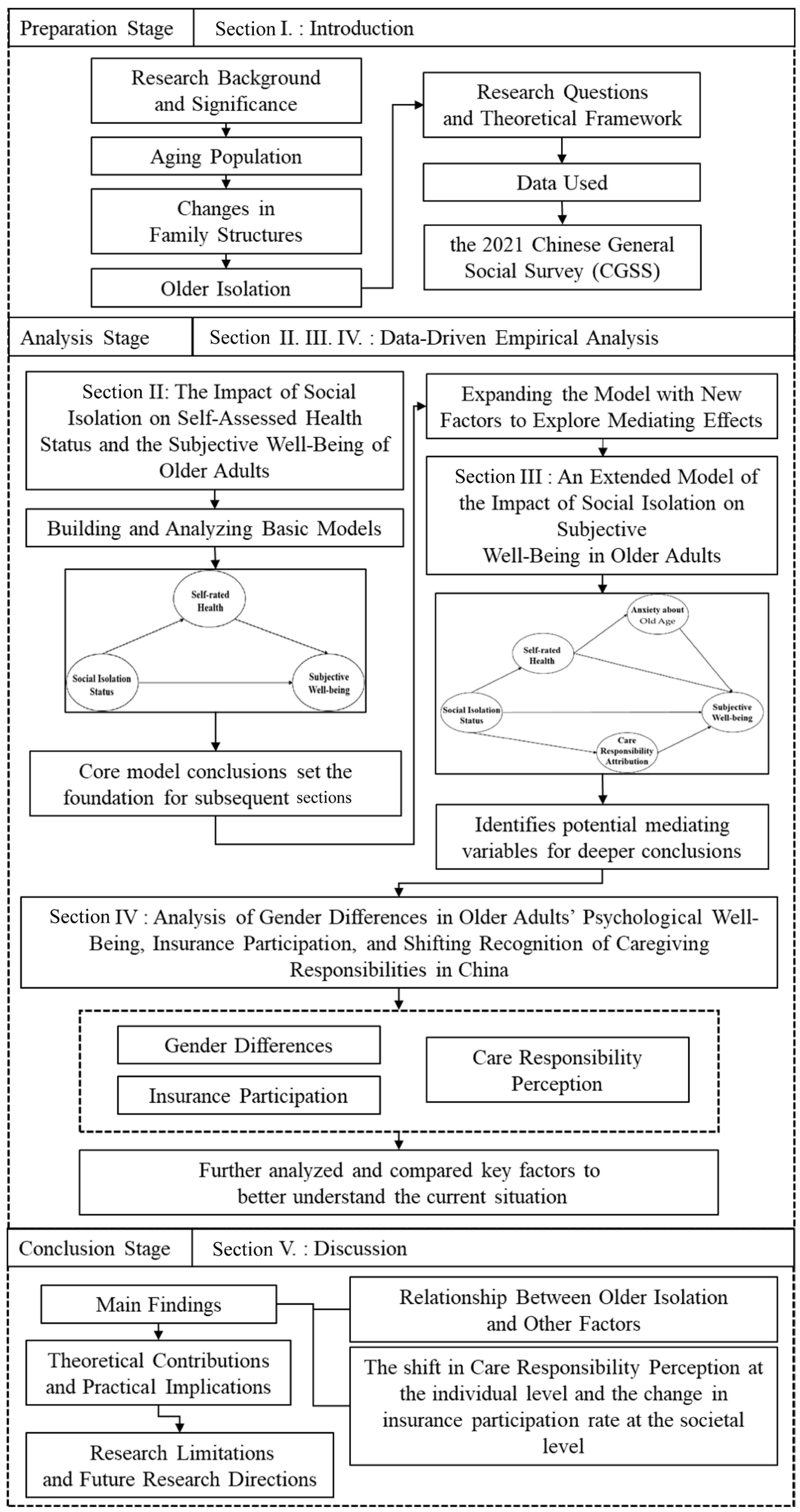
1.1. Structure and Analytical Method of the Study
1.2. Data
2. The Impact of Social Isolation on Self-Assessed Health Status and the Subjective Well-Being of Older Adults
2.1. Prior Research
2.1.1. The Challenges Facing China’s Aging Society
2.1.2. The Impact of Social Isolation on Attitudes Toward Self-Assessed Health and Subjective Well-Being in Older Adults
2.2. Data Utilization and Analytical Method
2.2.1. Data Utilization
2.2.2. Variable Settings
2.2.3. Model Analysis
2.3. Summary
3. An Extended Model of the Impact of Social Isolation on Subjective Well-Being in Older Adults
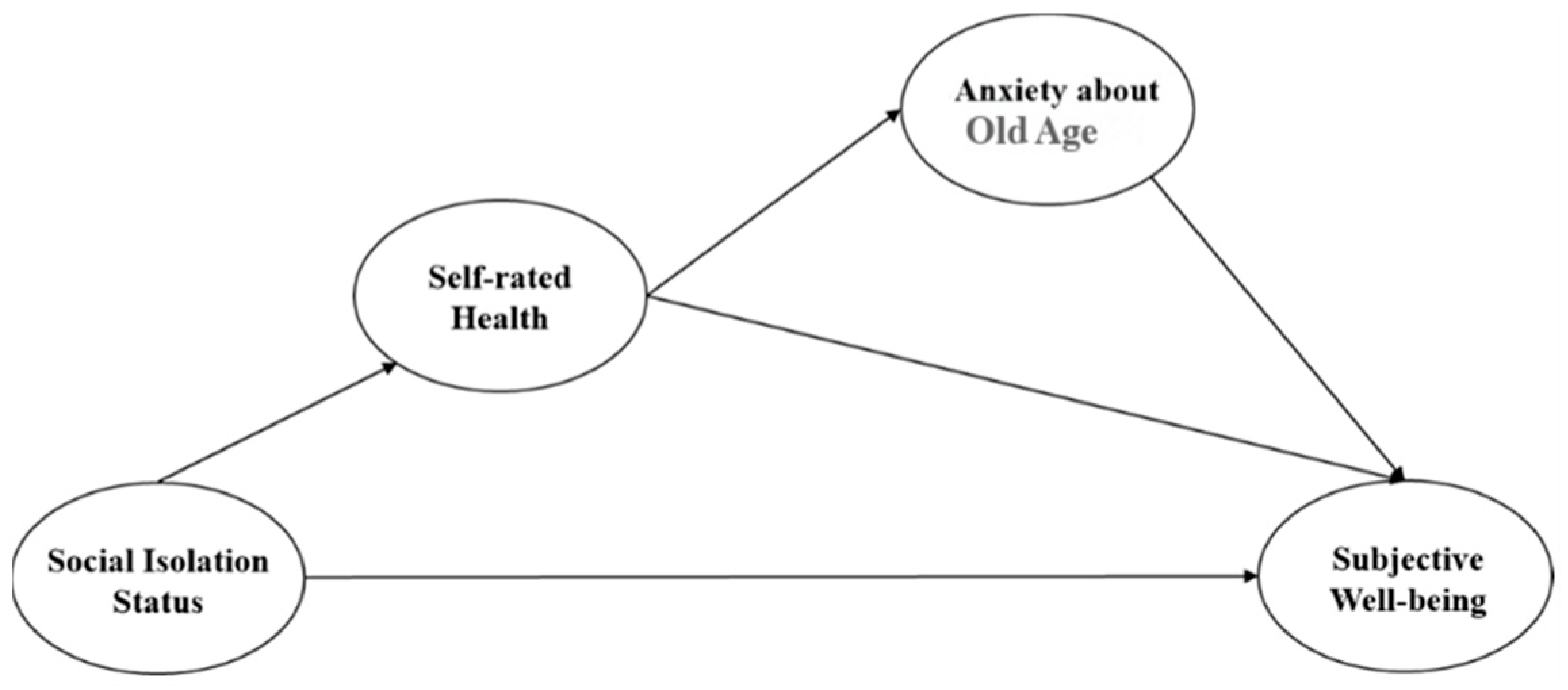
3.1. The Extended Estimation Model
3.2. Analytical Method
- (1)
- Group-based regression analysis: separate analyses were conducted for older and younger groups, with heterogeneity testing performed to identify differences between the models for each group. Based on the results, each factor’s impact on subjective well-being in older adults was then assessed.
- (2)
- Pathway-specific analysis: the specific pathways for each hypothesis were analyzed, and a final extended model was proposed based on the resulting findings.
Data Utilization and Explanation of Additional Variables
3.3. Model Regression Analysis
3.3.1. Multicollinearity Testing
3.3.2. Heterogeneity Testing
3.3.3. Mediation Effect Analysis
3.4. Final Extended Model
4. Analysis of Gender Differences in Older Adults’ Psychological Well-Being, Insurance Participation, and Shifting Recognition of Caregiving Responsibilities in China
4.1. Prior Research
4.1.1. Gender Differences in the Psychological State of Older Adults
4.1.2. The Impact of Social Isolation and Insurance Participation on the Elderly's Psychological State
4.1.3. Changes in Social Isolation and Perceptions of Caregiving Responsibility
4.2. Analytical Method
4.3. Data Analysis
4.3.1. Analysis of Insurance Participation
4.3.2. Multinomial Logistic Regression Analysis on the Influence of Social Isolation on Older Adults’ Perceptions of Care Responsibility
4.4. Summary
5. Discussion
5.1. Conclusions
5.2. Contributions to Research and Practice
5.3. Limitations and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, Z. Social Welfare Policy for the Elderly in China; Keio University Press: Tokyo, Japan, 2023; p. 1. [Google Scholar]
- Sohu.com, 160 million Elderly People Living Alone Nationwide, What Are the Challenges and Psychological Crises They Face? Pay Attention to Psychological Factors That Affect Lifespan, 26 June 2024. Available online: https://www.sohu.com/a/788660590_121347929 (accessed on 10 October 2024).
- Shangguan News, 160 million Elderly People Living Alone Nationwide: Over Half Are Aged 80 and Above, How to Provide Appropriate Elderly Care Services? 10 April 2024. Available online: https://m.jfdaily.com/wx/detail.do?id=736482 (accessed on 10 October 2024).
- Kazuhiko, F. What will the advent of a “society with many deaths” mean for Japan? Jpn. Soc. Real Options Real Options Strategy 2018, 10, 36–38. [Google Scholar]
- Matsuura, T.; Ma, X. Living Arrangements and Subjective Well-Being of Older Adults: A Comparison Between Japan and China. J. Happiness Stud. 2022, 23, 903–948. [Google Scholar] [CrossRef]
- She, B. 2003–2008-Report of General Social Survey in China; China Social Sciences Press: Beijing, China, 2009; pp. 1–299. [Google Scholar]
- People’s Daily Online, ’Premature Aging’ Becomes More Prominent, Population Aging Brings New Challenges. Available online: http://finance.people.com.cn/n/2013/0228/c1004-20626099.html (accessed on 10 October 2024).
- Zhang, J. The Potential of Community Welfare in Rural China; Minerva Shobo: Tokyo, Japan, 2020; pp. 19–20. [Google Scholar]
- Kotsuji, H. Analysis of Perspectives on Social Isolation of Elderly People. Core Ethics 2011, 7, 109–119. [Google Scholar]
- Zhou, C.; Liu, S.; Mao, J. Family Structure and Parenthood of Rural One-Child Parents Over 50 Years Old: Based on a Survey of 195 Households in Gaochun, Nanjing. J. Nanjing Coll. Popul. Programme Manag. 2011, 27, 5–9+26. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Leary, M.R. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol. Bull. 1995, 117, 497. [Google Scholar] [CrossRef]
- Luo, L.; Wei, L.; Gu, J.; Hu, Y.; Huang, Z.; Li, M. Current situation and risk factors of social isolation among elderly people in Chinese communities: A Meta-analysis. Chin. J. Health Manag. 2024, 30, 1159–1166. [Google Scholar] [CrossRef]
- Saito, M. The Meaning and Problems of the Study Concerning Social Isolation of the Elderly as Social Welfare Research. J. Soc. Welf. Nihon Fukushi Univ. 2009, 121, 29–42. [Google Scholar]
- Naikaku-kanbō. Office for the Promotion of Measures Against Loneliness and Social Isolation Key Findings of the 2023 National Survey on the Situation of Loneliness and Social Isolation (Reiwa 5). Available online: https://www.cao.go.jp/kodoku_koritsu/torikumi/zenkokuchousa/r5/pdf/tyosakekka_point.pdf (accessed on 18 September 2024).
- Okamoto, M. The Direction of Elderly Care Prevention Focused on Subjective Well-Being and Social Interaction. Jpn. Res. Inst. Rev. 2019, 7, 61–92. [Google Scholar]
- Diener, E.; Suh, E.M.; Lucas, R.E.; Smith, H.L. Subjective well-being: Three decades of progress. Psychol. Bull. 1999, 125, 276. [Google Scholar] [CrossRef]
- Wu, Q.; Tan, J.; Liao, X.; Chen, S.; Wang, J. The incidence of social isolation in Chinese elderly population: A meta-analysis. Chin. J. Evid.-Based Med. 2023, 30, 1159–1166. [Google Scholar] [CrossRef]
- Li, Q.; Xu, G.; Zhang, Z. Loneliness and Its Correlates Among the Aged People Living Alone in Urban Areas. J. East China Norm. Univ. (Humanit. Soc. Sci.) 2019, 51, 160–171. [Google Scholar] [CrossRef]
- Wang, Y. Independence and home care for the elderly in rural areas near Chinese cities: Rural Sunan. Mem. Res. Fac. Agric. Hokkaido Univ. 2021, 38, 1–54. [Google Scholar]
- Ochiai, E. The Logic of Global Family Change in Transforming Modernity: Focusing on Asia and Europe. Jpn. Sociol. Rev. Shakaigaku Hyoron 2013, 64, 533–552. [Google Scholar] [CrossRef]
- National Healthcare Security Administration, 2022 Healthcare Security Development Statistical Bulletin [R/OL], 10 March 2023. Available online: https://www.gov.cn/xinwen/2023-03/10/content_5745859.htm?eqid=96caf1a40008eb750000000264619ad3 (accessed on 11 October 2024).
- Hu, J.; Wang, T. Aging Finance in China: Realistic Dilemma, International Experience and Development Strategy. East. Forum—J. Qingdao Univ. (Soc. Sci. Ed.) 2024, 3, 1–11. (In Chinese) [Google Scholar]
- Shi, B. The integrated construction of economic support and service guarantee in the pension insurance system: Japan’s “long-term care insurance” system and its enlightenment. J. China Youth Univ. Political Sci. 2008, 27, 115–121. [Google Scholar] [CrossRef]
- Lyu, H.; Zhang, H. Study on the Influence of Pension Insurance Participation Behavior on the Cognition of Pension Responsibility an Empirical Analysis Based on CGSS2021 Data. J. Insur. Prof. Coll. 2024, 3, 30–36. [Google Scholar]
- Zhang, J.; Peng, J.; Gao, P.; Huang, H.; Cao, Y.; Zheng, L.; Miao, D. Relationship between meaning in life and death anxiety in the elderly: Self-esteem as a mediator. BMC Geriatr. 2019, 19, 308. [Google Scholar] [CrossRef]
- Fan, M. Analysis of Influencing Factors on the Use of Community Elderly Care Services for the Elderly Living Alone. Aging Res. 2023, 10, 1643–1651. [Google Scholar] [CrossRef]
- Tomonaga, M.; Nomura, T.; Sugisawa, H. Possibility of Bias for Evaluation Study on Intervention to Social Isolation of Older Adults. J. Gerontol. Res. 2020, 11, 29–43. [Google Scholar]
- Kawaguchi, Y. The Community Café as a Place-of-Belonging for Elderly People: The Perspectives of Users, Volunteers, and Leaders. Jpn. J. Geriatr. Psychiatry 2018, 31, 291–303. [Google Scholar]
- Wu, S.; Cao, F.; Sun, Y. Visual analysis of the development context and hot trend in healthy aging research in China and abroad. Chinese J. Health Manag. 2024, 18, 609–615. [Google Scholar] [CrossRef]
- Chen, J.; Wang, L.; Ren, J.; Jing, Q.; Sheng, H.; Gao, Q.; Cai, W. Study on the Spatial Distribution and Influencing Factors of Basic Endowment Insurance for Urban and Rural Residents in China Under the Background of Healthy Aging. Chin. Gen. Pract. 2024, 27, 2382–2387. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Social isolation status | Factor extraction conducted through exploratory factor analysis |
| Self-rated health | Overall, how do you feel about your current health status? 1 = Very Poor, 2 = Poor, 3 = Average, 4 = Good, 5 = Very Good |
| Subjective well-being | Overall, do you feel happy with your life? 1 = Very Unhappy, 2 = Unhappy, 3 = Average, 4 = Happy, 5 = Very Happy |
| C Total Effect | a | b | a × b Mediating Effect Value | a × b Boot SE | a × b z Value | a × b p Value | a × b 95% BootCI | c′ Direct Effect |
|---|---|---|---|---|---|---|---|---|
| −0.105 ** | −0.191 ** | 0.135 ** | −0.026 | 0.008 | −3.086 | 0.002 | −0.049~−0.016 | −0.079 ** |
| Variable | Variable Values |
|---|---|
| Gender | Male = 0, Female = 1 |
| Living situation | Living Alone = 0, Living Together = 1 |
| Anxiety about old age | Factors extracted using exploratory factor analysis |
| Care responsibility attribution Who do you think should be primarily responsible for the care of older people with children? (Converted to dummy variables) | Rely primarily on children = 1 Rely primarily on government = 2 Self-responsibility = 3 Responsibility shared by government/children/self = 4 |
| Insurance enrollment status | Urban/Rural Basic Medical Insurance, Participating = 1, Not Participating = 2 Urban/Rural Basic Pension Insurance, Participating = 1, Not Participating = 2 Private Medical Insurance, Participating = 1, Not Participating = 2 Private Pension Insurance, Participating = 1, Not Participating = 2 |
| Overall | Older | Younger (Comparison Group) | |
|---|---|---|---|
| Constant | 3.433 ** (26.143) | 3.393 ** (11.527) | 3.347 ** (22.634) |
| Living alone | −0.024 (−1.565) | −0.010 (−0.457) | −0.076 ** (−3.701) |
| Level of social isolation | −0.068 ** (−4.309) | −0.080 ** (−3.101) | −0.088 ** (−4.356) |
| Participation in private insurance | −0.049 (−1.695) | 0.006 (0.088) | −0.098 ** (−3.173) |
| Anxiety about old age | 0.103 ** (6.363) | 0.116 ** (4.412) | 0.078 ** (3.838) |
| Self-rated health | 0.133 ** (9.025) | 0.112 ** (4.598) | 0.198 ** (10.369) |
| Sample Size | 2717 | 1010 | 1707 |
| R2 | 0.071 | 0.064 | 0.115 |
| Adjusted R2 | 0.069 | 0.059 | 0.112 |
| F value | F (5, 2711) = 41.430, p = 0.000 | F (5, 1004) = 13.716, p = 0.000 | F (5, 1701) = 44.240, p = 0.000 |
| Group 1 | Group 2 | Regression Coefficient b1 | Regression Coefficient b2 | Difference | t Value | p Value | |
|---|---|---|---|---|---|---|---|
| Living situation | Older | Younger | −0.010 | −0.076 | 0.066 | 2.166 | 0.030 * |
| Level of social isolation | Older | Younger | −0.080 | −0.088 | 0.008 | 0.260 | 0.795 |
| Anxiety about old age | Older | Younger | 0.116 | 0.078 | 0.037 | 1.167 | 0.243 |
| Self-rated health | Older | Younger | 0.112 | 0.198 | −0.085 | −2.927 | 0.003 ** |
| Participation in private insurance | Older | Younger | 0.006 | −0.098 | 0.104 | 1.422 | 0.155 |
| C Total Effect | a | B | a × b Mediation Effect Value | a × b Boot SE | a × b z Value | a × b p Value | a × b 95% BootCI | c′ Direct Effect | |
|---|---|---|---|---|---|---|---|---|---|
| 0.107 ** | 0.066 ** | 0.097 ** | 0.006 | 0.003 | 2.167 | 0.030 | 0.004–0.018 | 0.100 ** | |
| C Total Effect | a | b | a × b Mediation Effect Value | a × b Boot SE | a × b z Value | a × b p Value | a × b 95% BootCI | c′ Direct Effect |
|---|---|---|---|---|---|---|---|---|
| −0.105 ** | −0.146 ** | 0.004 | −0.001 | 0.004 | −0.141 | 0.888 | −0.008–0.008 | −0.104 ** |
| C Total Effect | a | b | a × b Mediation Effect Value | a × b Boot SE | a × b z Value | a × b p Value | a × b 95% BootCI | c′ Direct Effect |
|---|---|---|---|---|---|---|---|---|
| −0.036 | −0.191 ** | 0.195 ** | −0.037 | 0.008 | −4.386 | 0.000 | −0.055–−0.022 | 0.001 |
| Living Alone (Mean ± Standard Deviation) | Urban/Rural Basic Medical Insurance Enrollment | Urban/Rural Basic Pension Insurance Enrollment | Private Medical Insurance Enrollment | Private Pension Insurance Enrollment |
|---|---|---|---|---|
| −2.31 (n = 462) | 0.09 ± 0.28 | 0.22 ± 0.41 | 0.96 ± 0.20 | 0.96 ± 0.20 |
| 0.43 (n = 2467) | 0.06 ± 0.24 | 0.20 ± 0.40 | 0.94 ± 0.23 | 0.96 ± 0.19 |
| F | 4.329 | 1.291 | 1.292 | 0.139 |
| p | 0.038 * | 0.256 | 0.256 | 0.709 |
| Theme | Response | Older or Younger (%) | Total (%) | χ2 | p Value | |
|---|---|---|---|---|---|---|
| Older (%) | Younger (%) | |||||
| Urban/rural basic medical insurance | Participating | 2724 (93.00) | 4889 (93.68) | 7613 (93.43) | 1.397 | 0.237 |
| Not Participating | 205 (7.00) | 330 (6.32) | 535 (6.57) | |||
| Urban/rural basic pension insurance | Participating | 2319 (79.17) | 3477 (66.62) | 5796 (71.13) | 143.948 | 0.000 ** |
| Not Participating | 610 (20.83) | 1742 (33.38) | 2352 (28.87) | |||
| Private medical insurance | Participating | 154 (5.26) | 962 (18.43) | 1116 (13.70) | 275.491 | 0.000 ** |
| Not Participating | 2775 (94.74) | 4257 (81.57) | 7032 (86.30) | |||
| Private pension insurance | Participating | 107 (3.65) | 454 (8.70) | 561 (6.89) | 74.507 | 0.000 ** |
| Not Participating | 2822 (96.35) | 4765 (91.30) | 7587(93.11) | |||
| Gender (Mean ± Standard Deviation) | Anxiety About Old Age | Self-Rated Health | Subjective Well-Being |
|---|---|---|---|
| Male (n = 1426) | 2.74 ± 1.04 | 3.17 ± 1.11 | 4.11 ± 0.81 |
| Female (n = 1503) | 2.58 ± 1.00 | 2.98 ± 1.13 | 4.01 ± 0.90 |
| T | 2.423 | 4.626 | 2.651 |
| p value | 0.016 * | 0.000 ** | 0.008 ** |
| Rely on Government | Regression Coefficient | Standard Error | z Value | Wald χ2 Value | p Value | OR | OR 95% CI |
|---|---|---|---|---|---|---|---|
| Social isolation | −0.095 | 0.095 | −0.998 | 0.997 | 0.318 | 0.909 | 0.755–1.096 |
| Intercept | −1.341 | 0.101 | −13.224 | 174.876 | 0.000 | 0.262 | 0.215–0.319 |
| Self-responsibility | Regression Coefficient | Standard Error | z value | Wald χ2 Value | p value | OR | OR 95% CI |
| Social isolation | 0.063 | 0.102 | 0.621 | 0.386 | 0.534 | 1.065 | 0.872–1.301 |
| Intercept | −1.492 | 0.110 | −13.562 | 183.939 | 0.000 | 0.225 | 0.181–0.279 |
| Shared responsibility | Regression Coefficient | Standard Error | z value | Wald χ2 Value | p value | OR | OR 95% CI |
| Social isolation | −0.333 | 0.075 | −4.413 | 19.477 | 0.000 | 0.717 | 0.618–0.831 |
| Intercept | −0.718 | 0.080 | −8.983 | 80.700 | 0.000 | 0.488 | 0.417–0.570 |
| Care Responsibility Attribution (Mean ± Standard Deviation) | Subjective Well-Being |
|---|---|
| Rely primarily on children (n = 1453) | 4.04 ± 0.71 |
| Rely primarily on government (n = 380) | 3.95 ± 0.79 |
| Self-responsibility (n = 382) | 4.10 ± 0.65 |
| Responsibility shared among government/children/older adults (n = 714) | 4.05 ± 0.68 |
| F value | 3.249 |
| p value | 0.021 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, K.; Chen, Z. The Impact of Social Isolation on the Subjective Well-Being of Older People in China: An Empirical Analysis Based on the 2021 China General Social Survey. Int. J. Environ. Res. Public Health 2025, 22, 501. https://doi.org/10.3390/ijerph22040501
Ryu K, Chen Z. The Impact of Social Isolation on the Subjective Well-Being of Older People in China: An Empirical Analysis Based on the 2021 China General Social Survey. International Journal of Environmental Research and Public Health. 2025; 22(4):501. https://doi.org/10.3390/ijerph22040501
Chicago/Turabian StyleRyu, Keikoh, and Zaiqing Chen. 2025. "The Impact of Social Isolation on the Subjective Well-Being of Older People in China: An Empirical Analysis Based on the 2021 China General Social Survey" International Journal of Environmental Research and Public Health 22, no. 4: 501. https://doi.org/10.3390/ijerph22040501
APA StyleRyu, K., & Chen, Z. (2025). The Impact of Social Isolation on the Subjective Well-Being of Older People in China: An Empirical Analysis Based on the 2021 China General Social Survey. International Journal of Environmental Research and Public Health, 22(4), 501. https://doi.org/10.3390/ijerph22040501