1. Introduction
Significant evidence has accumulated on the association of psychosocial working conditions using the Demand-Control-Support model (DCS) with both health outcomes and positive behavioral outcomes. Much of the evidence is based on measures—namely, task-level demands, control, and support—derived from the Job Content Questionnaire (JCQ 1). Recently published extensions of both the theoretical base, i.e., the Associationalist Demand–Control (ADC) model (see
Appendix A, A.1), and of the corresponding original JCQ to the JCQ 2.0 (see
Appendix A, A.2), suggest that it is important to test whether the previously observed “foundational associations” of the DCS model remain valid when using the revised JCQ 2.0. The JCQ 2.0 substantially updates the instrument, shortening previous scales and adding a considerable number of new scales at multiple levels: task, organization, and external-to-work.
Past research has led to extensive and differentiated literature on the associations between job strain and chronic diseases such as cardiovascular diseases (CVD) [
1,
2,
3,
4] as well as the onset of musculoskeletal disorders [
5] and depressive symptoms [
6,
7,
8]. Likewise, task demands, control, and support are associated with favorable work outcomes [
9], such as job satisfaction (JS) [
10] and active behaviors outside the workplace [
11,
12,
13].
In this paper, we test the implications of the new JCQ 2.0 instrument, examining the associations between the DCS constructs at the task and the organizational levels and the classic demand–control DC hypotheses predicting workplace outcomes, both negative (health deficit, disease) and positive (active, motivational, learning-related), in an integrated manner. Additionally, we test the combinations of demand and control (job strain, i.e., the combination of high demands and low control, and active work, i.e., the combination of high demands and high control) as the DC approach has done before.
One of the important goals for the JCQ 2.0, as proposed by Karasek and colleagues (see
Appendix A, A.1), was to maintain—to the extent possible—the pragmatically and intellectually useful DC narrative. A meta-analysis of 106 studies [
14] clearly demonstrates the utility of the Demand-Control-Support framework, as is confirmed by further work [
9]. Thus, empirically, the first step was to assess the degree to which factors for demand, control, and support at the task and organizational level, based on numerous sub-scales, namely the JCQ 2.0 scales, function as previously hypothesized. Analysis of the structure of the JCQ 2.0 (see
Appendix A, A.3) found sufficient coherence across four pilot studies in four countries and across the two levels to ensure that the DCS constructs are empirically usable at multiple levels, allowing us to apply composite scores for further analyses.
Thus, in this paper, we combine scale scores belonging to the same factors (see
Appendix A, A.3) and analyze the predictive validity of these six composite scores for health and work-related outcomes. The use of such composite scales will substantially simplify testing, presenting, and understanding of the findings—given four pilot studies, two testing levels, up to seventeen scales (in later pilot versions), and six dependent variables. However, analyses of composite scores may overlook important associations for many of the individual JCQ 2.0 scales (see
Appendix A, A.2) that are further examined in an additional paper (see
Appendix A, A.4). We note that using the composite scores—summing over the component scales equally weighted—is not the same as using, for example, the underlying factor scores from a structural equation model.
In this paper, we conduct three different forms of dependent measure tests:
We use the JCQ 2.0 scales, in composite form, to test the association of the JCQ 2.0 dimensions with dependent variables, including worker health and favorable work outcomes.
We review the relative strength of association for JCQ 2.0 composite task and organization level scales with two dependent variables using a simplified path model analysis.
We test the relative improvement that the JCQ 2.0 instrument provides in “predicting” (albeit cross-sectionally) associations over the base JCQ 1 items in both Australia and Germany.
With these tests, we hence aim at showing that (i) the JCQ 2.0 composite scales for demand, control, and stability-support at both the task and the organizational level are related to health and work-related outcomes as hypothesized in the DC and ADC models, and (ii) the JCQ 2.0 explains more variance in health and work-related outcomes than the scales solely from the JCQ 1.
It should be noted that the organizational-level scales only exist in a full, practically relevant set in the two later pilots, Australia and Germany. However, a limited comparative review of task-level associations is provided for Korea and China with regard to the first analyses.
1.1. New Theoretic Base
The new systems-theoretic base for the multilevel demand, control, and stability-support (DCS-S) concept is the ADC theory (see
Appendix A, A.1). The basic building blocks of DCS are here translated to fit a new multilevel framework, which specifies expanded and refined DCS constructs at the task level and new DCS-S elaborations at the organizational level. Karasek et al. (see
Appendix A, A.1) describe how the JCQ 2.0 differs from its predecessor, the JCQ 1, in capturing organizational-level working conditions and how these impact working conditions at the task level. Specifically, they describe the expansion of support at the task level to stability-support at the organizational level (see
Appendix A, A.1). The ADC model involves workers and organizations (a) doing their daily “work” as necessary for their adaptation to their environment and then (b) building “ordering capacity” to restore their capability for further actions necessary for continual existence of healthy wellbeing and growth. The original DC model’s dual hypotheses about workers’ health and wellbeing reflect “energy and order” related working conditions. Utilization of these very general and abstract “energy and order” themes allows for building DC narrative-consistent, broadly generalizable extensions in a multilevel JCQ 2.0 workplace social context. While the JCQ 1 focused on task implications, the focal theoretical innovations for the JCQ 2 represent extensions of “control” as multilevel work-related action pathways. The expanded multilevel demands concept reflects both the worker’s possibility of maintaining a personal equilibrium in daily working life and at the same time the organization’s need to continually bring in new resources of effective adaption and further growth. The dynamic nature of this balance of challenges is reflected in the organizational mid-level concept of Platforms of Dynamic Stability as discussed by Karasek et al. (see
Appendix A, A.1). Overall, ADC theory describes how systems can either organize themselves into higher levels of complexity (extending the Active Work hypothesis and “health” as in the established DC model)—i.e., systems that grow and develop—or, alternatively, how complex systems devolve to lower levels of complexity (extending the Job Strain hypothesis of the DC model), no longer able to sustain their original capability. While empirical testing of the full range of ADC theory’s dynamic hypotheses is beyond the capacities of the current cross-sectional datasets, the test below can verify the new instrument’s capability of meaningfully extending the original DC narrative in our current global economic context and is thus both a feasible and a necessary requirement for meaningful empirical testing of the JCQ 2.0.
1.2. JCQ 2.0 Task-Level Constructs and Associations
Given the modifications to the JCQ 2.0 tool compared to the JCQ 1 [
15], shortening the available scales and adding new scales, it is important to verify the foundational associations of the DCS model using the revised JCQ 2.0 tool. We propose:
Hypothesis 1. High task-level demands will be positively related to poor health (poor self-rated health (SRH), burnout, depression) and negatively related to favorable work outcomes (affective commitment to the organization (AC)/work engagement (WE), JS, and intention to stay (ITS)/intention to leave (ITL)).
Hypothesis 2. High task-level control and support will be negatively related to poor health and positively associated with favorable work outcomes.
It is important to also verify, using the new tool, the foundational strain and active dimensions specified in the DC model at the task level and their associations with health and favorable work outcomes, respectively, that have been found in previous research [
16,
17,
18]. For the revised JCQ 2.0, we propose:
Hypothesis 3. Workers with high job strain at the task level have higher levels of poor health than workers with low job strain.
Hypothesis 4. Workers with high task-level active work have higher levels of favorable work outcomes than workers with passive jobs [
12].
1.3. JCQ 2.0 Organizational-Level Constructs and Associations
Moving to the organizational level framework, the separate components are organizational demands, control, and stability-support. Demands are conceived in terms of organizational disorder and restructuring, assessing organizational processes and change affecting job demands for employees, respectively; for more detailed definitions of all JCQ 2.0 measures, please refer to Karasek et al. (see
Appendix A, A.1).
Control is conceptualized in terms of organizational decision latitude, procedural justice, and conducive communication. Procedural justice refers to fairness in decision making; consistency of application; input from affected parties; and accurate, correctable, and ethical decisions [
19]. Research on organizational justice showed that it was related to coronary heart disease (CHD; [
20]). Specifically, low levels of procedural justice were associated with a higher risk of poor SRH and minor psychiatric disorders as well as sickness absence (women only), even after adjustment for the DCS task level measures (women only; [
19]). Organizational decision latitude refers to control at the organizational level, provided by communication between employees and managers, which relates to subjective wellbeing and organizational commitment [
21]. Conducive communication refers to a skill-enhancing, interactive communication mode engaging workers and customers.
Stability-support is conceived in terms of psychosocial safety climate, rewards, and consideration of workers’ interests. Psychosocial safety climate refers to organizational policies, practices, and procedures for the protection of worker psychological health and well-being and predicts psychological distress, emotional exhaustion, and employee engagement [
22].
The inclusion of rewards, specifically the aspects of financial rewards and appreciation, is inspired by research on the effort–reward imbalance (ERI) model [
23]. ERI is associated with depressive symptoms [
24], adverse cardiovascular and other health effects [
25], CVD and depression, Type II diabetes, alcoholism, sleeping problems, and sickness absence [
26]. Both ERI and job strain are related to angina pectoris, depression, and poor SRH [
27]. A systematic review found statistically significant associations between ERI and CVD [
2].
Consideration of workers’ interests refers to fairness to workers in the context of organization change processes (see
Appendix A, A.1).
We propose that the DCS-S constructs and their combinations (e.g., high strain, active work) at the organizational level will relate to health and work outcomes in parallel ways to the DCS constructs and combinations at the task level. We expect:
Hypothesis 5. High organizational level demands will be positively associated with indicators of poor health and negatively associated with favorable work outcomes.
Hypothesis 6. High organizational level control and stability-support will be negatively associated with poor health and positively associated with favorable work outcomes.
Hypothesis 7. Workers with high organizational level job strain have higher levels of poor health than workers who have low strain.
Hypothesis 8. Workers with high organizational level active work have higher levels of favorable work outcomes than those who have passive jobs.
Two separate but related tasks remain: The first is to show that the JCQ 2.0 tool can be used to verify theoretical considerations consistent with causal pathways—albeit only using cross-sectional data—that have important policy implications. The second task is more pragmatic and is to show the utility of using the JCQ 2.0 tool over the JCQ 1 tool.
Organizational context matters and affects work design [
28], implying a hierarchy of causation. Therefore, one needs to consider how the organizational level DCS-S composites affect lower level entities, i.e., DCS at the task level. Since the organizational level is more distal, they are leading and likely to influence downstream task level composites. Demands emanating at the organizational level are likely to filter through to task level demands in addition to their direct effects on outcomes. Organizational level control is likely to affect task control, and stability-support at the organizational level is likely to affect task support, again both in addition to their direct effects on outcomes. For instance, psychosocial safety climate at the organizational level (work unit), reported by one group of nurses, predicted support from supervisors at the task level, reported by different nurses in the same unit 24 months later [
29]. These hierarchical relations imply process paths from organizational DCS-S through task DCS to health and work outcomes. Hence, we propose:
Hypothesis 9. Organizational composites (D, C, and S-S) will correlate with parallel task composites in such a way that organizational composites will affect task composites. Furthermore, task composites will affect health and work outcomes. There will be additional direct effects from organizational composites to health and work-related outcomes, not mediated by task composites.
Given these predicted multilevel associations, organizational composites will explain additional variance in health and work-related outcomes, as implied in the expectation of direct effects. The pragmatic goal here is to show instrument improvement, the added variance of JCQ 2.0 organizational domains over task domains, and vice versa. In addition, the composites at both levels assess working conditions in a far more comprehensive way than the JCQ 1 DCS core scales did. Hence, we aim to show the added variance of the new JCQ 2.0 tool over the established JCQ 1 DCS core, including the most often tested DC model measures: “psychological demands” and “decision latitude”. We expect:
Hypothesis 10. JCQ 2.0 DCS-S composite scores at the organizational level will explain additional variance over and above that explained by the JCQ 2.0 composite scores at the task level and vice versa. Moreover, we expect that the JCQ 2.0 task and organizational composites will explain more variance than the JCQ 1 DC and DCS core scales.
3. Results
3.1. Task Level
Hypothesis 1 proposed that high task demands will be positively associated with indicators of poor health (poor SRH, high levels of burnout, and depression) and negatively associated with favorable work outcomes (AC/WE, JS, and ITL/ITS). This hypothesis was nearly fully supported in Australia (no effect for demand and WE) and fully supported in Germany, as shown in
Table 1; effects were of small to medium magnitude in most instances and large for burnout in Germany.
Hypothesis 2 proposed that high task control and support will be negatively associated with indicators of poor health and positively associated with favorable work outcomes. This hypothesis was nearly fully supported—as shown in
Table 1—in Australia and Germany (no effect for control and burnout in Australia). For Australia, the effects were small to medium. In Germany, effects ranged from small to large.
3.2. Task-Level Job Combinations—Job Strain and Active Work
As shown in
Table 2, for both Australia and Germany, Hypothesis 3—workers with high task-level job strain have higher levels of poor SRH, burnout, and depression compared to low-strain workers—was supported with small to large effects in Australia and large effects in Germany. Health among workers in high-strain jobs was significantly worse compared to those in low-strain jobs.
For Hypothesis 4—workers with high task-level active work have more favorable work outcomes than workers who have passive jobs—there was only support from the Australian data in relation to one out of three outcome measures, with a moderate effect for WE (
Table 2). The German sample showed a negligible effect for ITL, a small effect for JS, and a moderate effect for AC (see
Table 2).
3.3. Organizational Level
Hypothesis 5 proposed that high organizational demands are positively associated with indicators of poor health and negatively associated with favorable work outcomes. This hypothesis was supported in Germany and only partly supported in Australia, particularly in relation to favorable work outcomes (see
Table 1). Organizational demands were related to health and work outcomes in Australia with small effects for burnout, depression, and JS (for poor SRH, WE, and ITS, the effect was negligible) and as expected, in Germany with small to moderate effects, with a large effect for JS.
Hypothesis 6 proposed that high organizational control and stability-support are negatively associated with indicators of poor health and positively associated with favorable work outcomes. Organizational-level control and stability-support were related to health and work outcomes as expected with small to medium effects in Australia and with small to large effects in Germany (see
Table 1). Thus, this hypothesis was well supported.
3.4. Organizational-Level Job Combinations—Job Strain and Active Work
In Hypothesis 7, it was expected that workers with high organizational-level job strain have higher levels of poor health than workers who have low strain. This hypothesis was fully supported in Australia and Germany (see
Table 2). In Australia, the effect was small for SRH and depression and large for burnout; for Germany, the results were even stronger (mainly large effects). In each case, workers’ health in organizational-level high-strain jobs was significantly worse compared to workers’ health in low-strain jobs.
Hypothesis 8 proposed that workers with high active work at the organizational level have higher levels of favorable work outcomes than those in passive work. This hypothesis was supported in Australia and Germany with small to moderate effects (see
Table 2).
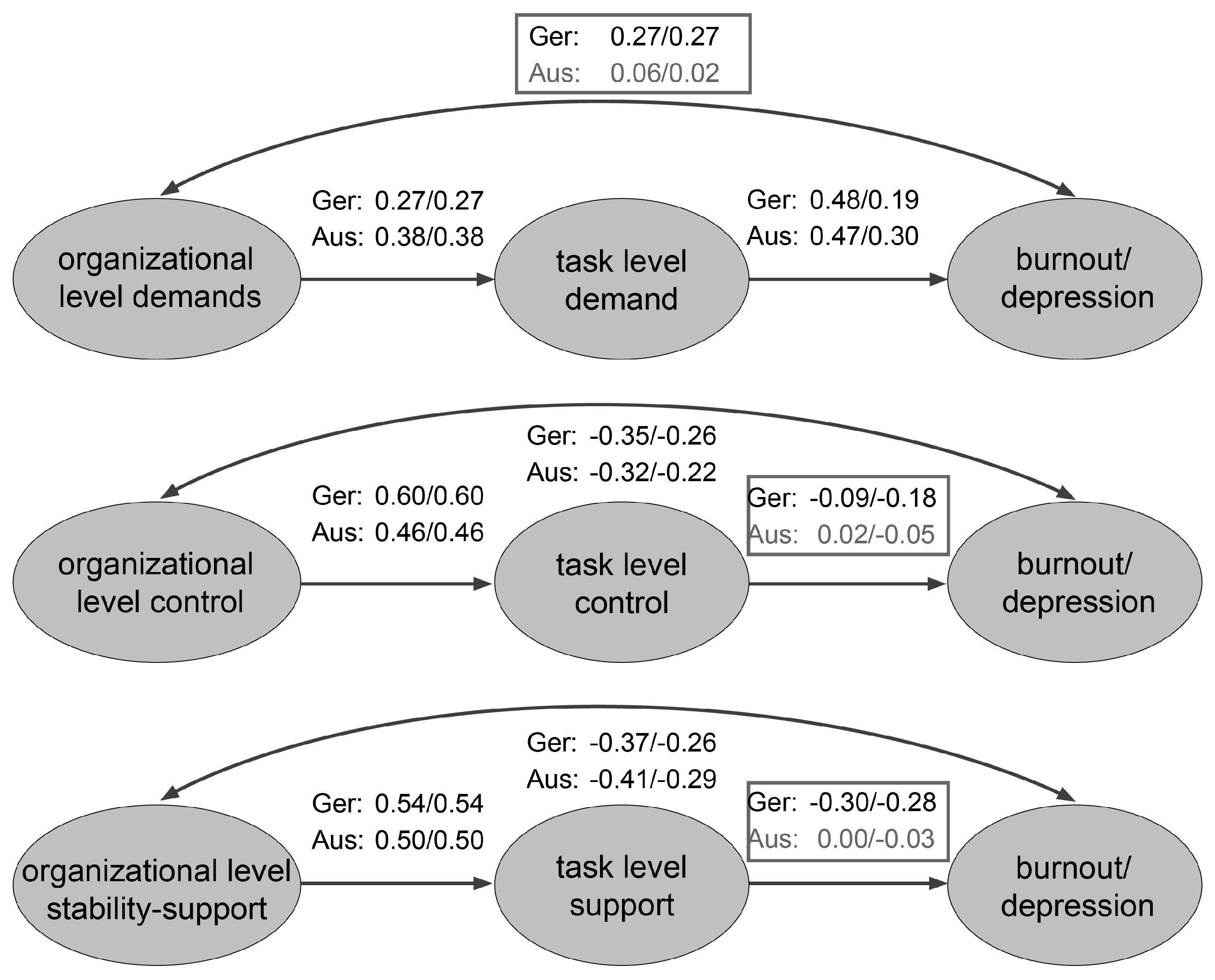
3.5. Path Analysis
In the path models, organizational composites (D, C, and S-S) were modeled as antecedents to parallel task composites (see
Figure 1). Effect sizes were small to large, linking the parallel composites across Australian and German data.
For both burnout and depression, the direct association between organizational demands and outcomes was close to zero in Australia and small in Germany when all other relations were modeled. The association between task control and task support and the outcomes were close to zero in Australia when all other relations were modeled simultaneously. This was not the case in Germany with the exception of task control and burnout; in all other cases, the associations in the German sample were of a small magnitude.
In Germany, organizational control was directly related to both burnout and depression in a stronger way than task control, whereas associations for task and organizational stability-support were of approximately equal size. For burnout, the relation was stronger for task demand, whereas for depression, it was stronger for organizational demands. In both Germany and Australia, organizational and task control and stability-support were each more strongly related than organizational and task demand.
Because the models are saturated, model fit indices are not available, and model fit could not be assessed. Furthermore, modeling a correlation between the task and the organizational factors and considering both as predictors of burnout or depression, respectively, would give the same values as reported above. However, due to the cross-sectional nature of the data, it is not possible to assess the direction of effects.
Hypothesis 9 that organizational D, C, and S-S affect task composites and task composites affect psychological health, allowing for direct effects of organizational composites on burnout and depression, was nearly fully supported in the German data across all factors. For Australia, this model was not clearly evident: in the demand domain, no association between organizational demand and outcomes remained when task demand was modeled too, which implies a process whereby organizational demands relate to burnout and depression through task demands. By contrast, for control and support, the task composites were not related to the outcomes when the relations with organizational composites were modeled simultaneously.
3.6. Value Added
Hypothesis 10 proposed that the JCQ 2.0 DCS-S organizational composites would explain additional variance over and above that explained by the JCQ 2.0 task composites and vice versa after controlling for gender and age. In addition, the hypothesis proposed that JCQ 2.0 task and organizational domains would explain more variance than the classic JCQ 1 DC and DCS.
For Australia, task and organizational composites added unique variance to each other in the prediction of health and work measures after controlling for gender and age, except for SRH (see
Table 3 first half).
Compared to the baseline classic JCQ 1 DC scales and the JCQ 1 DCS scales, the complete JCQ 2.0 explained more variance in all outcomes (final lines in
Table 3). This indicates merit in the JCQ 2.0 measures over and above those of JCQ 1. Considering both the JCQ 2.0 task and organizational DCS-S scores together explains the largest amount of variance in outcomes.
For Germany, the results were similar and of a larger magnitude across all outcomes (see
Table 4). Adding the JCQ 2.0 organizational DCS-S composites in addition to the JCQ 2.0 task DCS composites led to a rise in explained variance. In the same vein, JCQ 2.0 task DCS composites explained additional variance in all outcomes over and above JCQ 2.0 organizational composites. Furthermore, the JCQ 2.0 task and organizational DCS-S composites predicted a larger amount of variance in all outcome measures than the JCQ 1 DC and JCQ 1 DCS scales. Consequently, utilizing the JCQ 2.0 task and organizational DCS-S composites allowed for the greatest explanation of outcome scores.
When considering the relative improvement in explained variance in relation to the classic JCQ 1 psychological demand and decision latitude scales which have been used in many research papers, this improvement varied between 63% for SRH (from Radj2 = 0.08 to Radj2 = 0.13) and 153% for AC (from Radj2 = 0.13 to Radj2 = 0.33) in Germany and between 33% for SRH (from Radj2 = 0.03 to Radj2 = 0.04) and 88% for JS (from Radj2 = 0.17 to Radj2 = 0.32) in Australia. In relation to the JCQ 1 DCS scales, the relative improvement varied between 26% for JS (from Radj2 = 0.50 to Radj2 = 0.63) and 47% for depression (from Radj2 = 0.17 to Radj2 = 0.25) in Germany and between 33% for SRH (from Radj2 = 0.03 to Radj2 = 0.04) as well as ITS (from Radj2 = 0.09 to Radj2 = 0.12) and 60% for JS (from Radj2 = 0.20 to Radj2 = 0.32) in Australia.
To summarize, Hypothesis 10 was supported since in both countries, the JCQ 2.0 task and organizational DCS-S composites explained unique variance in all outcomes, and the JCQ 2.0 DCS version explained more variance in all outcomes compared to the classic JCQ 1 DC and DCS versions.
3.7. Summary of Results
Table 5 summarizes the results of all hypotheses tests. The first three hypotheses were also tested in Korea and China; the details of these analyses are beyond the scope of this paper.
4. Discussion
In this paper, we were able to show that JCQ 2.0 task demand, control, and support relate to health and to positive work-related outcomes nearly as expected in Australia and as expected in Germany, nearly and fully confirming Hypotheses 1 and 2. These DCS JCQ 2.0 task composites comprise both the established JCQ 1 core scales as well as newly developed scales which capture working conditions at the task level in a more comprehensive way. Importantly, the meaning of the foundational concepts of demand and control was retained in the revision of the JCQ. In the same vein, task-level job strain relates to health and work-related outcomes in expected ways, confirming Hypothesis 3 and yielding further support for the claim that the revision of the JCQ has not undermined foundational concepts.
The JCQ 2.0 organizational-level scores for demand, control, and stability-support show a pattern of associations with outcomes that is in most cases similar to the one at the task level, thus fully confirming Hypothesis 6 in both samples and Hypotheses 5 in the German sample. In Australia, Hypothesis 5 could only partly be confirmed as there were some non-significant associations in the Australian sample in relation to organizational demands. In addition, associations between organizational-level job strain and health and work-related outcomes are similar to those for task-level strain, confirming Hypothesis 7 and implying similar mechanisms underlying the detrimental effect of poor working conditions at both the task and the organizational level on health.
By contrast, it was not possible to unequivocally confirm Hypothesis 4 regarding the association of task-level active work with positive work-related outcomes. There was only one association in the Australian data with WE; associations in the German data were present for two out of three outcomes (AC and JS). The argument that job satisfaction and job commitment may not be the most appropriate for testing the active work construct [
44] does not hold true in the current study: in both countries, there was support for the association of active work and WE/AC; additionally, the relation to JS was present in the German sample. One possible explanation for the discrepancy between the two countries with regard to JS is that it was only measured with a single item in Australia and with a seven-item scale in Germany. However, since task demand, control, and support were related to JS in the Australian sample, this does not seem to be the reason. The above argument [
44] could be applicable to ITS/ITL as an outcome measure. Another reason could be that we used the five-category version of the DC model [
41], whereas a lot of other studies have used the four-category version as originally presented [
11].
The active work hypothesis has been confirmed previously when additional outcomes were considered. A study with over 3000 employees in 76 northern Belgium companies provided support for the active work hypothesis with a new measure of innovative work behavior that comprises behaviors such as “finding original solutions” and “developing innovative ideas” [
45]. This measure was also positively associated with work demands (i.e., work pressure), as hypothesized for demands in the DC model [
11] and in the concept of “flow” according to Csikszentmihalyi [
46]. The active work hypothesis has also been confirmed in relation to outside-work behaviors [
12] and post-retirement social engagement [
47].
In addition, it must be noted that practitioners have used the active work construct for observing real behavioral change. Social policy initiatives like the European Workplace Innovation Network EUWIN (
https://workplaceinnovation.eu/this-is-workplace-innovation/, accessed on 13 March 2025) consider the active work construct, as do intervention projects like the “Tzatziki Work Organization Simulation Game” (
http://www.oresundsynergy.com/tzatziki-game/, accessed on 13 March 2025). Much of this research has been “case study-based” in dynamically changing company environments, with the result of little direct questionnaire research and limited quantitative precision [
48].
Nevertheless, further explanations seem to exist for the only partially supporting results regarding Hypothesis 4 because Hypothesis 8 on the association of organizational-level active work and positive work-related outcomes was fully confirmed, supporting the theoretical meaning of the active work hypothesis at the organizational level. Thus, the diverging results might be attributable to differences in organizational culture and/or occupational regulations and/or national labor policies, and/or their implementation between Germany and Australia at the time of the study that stimulate varying strategies at the organizational level. Consequently, these results call for further research on the active work hypothesis at both the task and the organizational level in relation to a wide range of outcomes that relate to learning behavior as proposed in the DC model [
11], for which the JCQ 2.0 could prove to be a valuable tool.
For Hypothesis 9, results differed between Germany and Australia. The German data nearly fully confirmed the hypothesis that there are both direct as well as indirect effects of the organizational composites demand, control, and stability-support on burnout and depression, with the indirect effects modeled by the intermediate task composites. However, in Australia, no such evidence could be found, and either the direct effects (for demands) or the indirect effects (for control and stability-support) were zero or close to zero. It is possible that these diverging results are due to the fact that fewer scales were available in the Australian data compared to the German data, rendering the composite demand, control, and stability-support scores at both levels less comprehensive and stable in the Australian data. It is hence worthwhile to put this hypothesis to another test in Australia, applying the complete JCQ 2.0 with all researcher scales. Nevertheless, the direct effects of the organizational control and support measures in Australia show their importance above task-level effects and justify their measurement. The differences could also reflect a cultural difference whereby Australian workers find support and control from the top to be most comforting for their health and wellbeing.
In relation to demands, for both countries, results were consistent with the multilevel theorization that organizational demands are distal to psychological health (burnout and depression), and their detrimental effects on psychological health operate via their influence on task demands. This multilevel process was also observed in Germany for stability-support and control (for the latter, only for depression). In sum, in seven out of twelve tests, there was support for a multilevel mediation process whereby the more distal organizational composites were related to proximal task composites that affected burnout and depression.
Both task and organizational composites explained unique variance in accordance with Hypothesis 10, confirming that they are important for both health and work-related outcomes. With the exception of JS in Australia and AC in Germany, for all other outcomes, the unique variance explained by the task composites was slightly higher than the unique variance explained by the organizational composites. One likely explanation is the greater proximity of the task-level characteristics for workers.
Table 3 and
Table 4 final regressions showed that there is substantial improvement in variance explained (indicated via
Radj2) for each dependent variable with the use of the full JCQ 2.0 DCS-S composite scales with their broad theoretical coverage compared to the JCQ 1 DC and DCS scores. Further additional variance could possibly be explained when considering the JCQ 2.0 external-to-work scales (see
Appendix A, A.5). The absolute magnitude of baseline and increase varied widely because the outcome measures differed in how proximal vs. distal they are to the work environment: whereas JS is clearly work-related, SRH is influenced by many other factors than solely the work environment.
Consistent with results of path analyses, the associations in the German data were of a larger magnitude than associations in the Australian data, possibly because the higher number of JCQ 2.0 scales available in the German data rendered the composite scores more stable. The full ADC theory’s relevant set of scales with substantial extensions in the three areas of demand, control, and stability-support was present only in the German scale set. Together with the greater clarity of the multilevel path model testing in Germany in comparison to Australia, the case is also made for the explanation that the full ADC theory, with its relevant dimensions, must be assessed by the JCQ 2.0 for it to reach both its full explanatory power and its ability to distinguish appropriately between the task and the organizational level. Further research is needed to confirm this latter interpretation.
Summarizing, Hypothesis 10 is confirmed: substantially more variance is explained in almost all outcome measures due to the JCQ 2.0 compared to the classic JCQ 1 DC and DCS core scales, which underlines the ability of the revised JCQ 2.0 to provide significantly more precise prediction of relevant outcomes compared to the earlier instrument.
Strengths and Limitations of the Study
There are several strengths of the paper. The first is that the research hypotheses were largely confirmed in two different countries, Germany and Australia, with different cultures. Moreover, the study samples were large and from multiple occupations, allowing us to cover a wide spectrum of working conditions. Also, the revised JCQ 2.0 used in the study was systematically developed, allowing for a stepwise inclusion of more scales from the first study in Korea to the final study in Germany for greater domain coverage. Revisions were based on theoretical considerations as well as experiences in practical use, rendering the JCQ 2.0 suitable for use in practical contexts. Further, the outcome measures applied in the study in many cases stemmed from validated and established instruments. Finally, multiple imputation was applied to missing data instead of restricting analyses to complete cases, thereby avoiding over- or underestimation. As is described by Formazin et al. (see
Appendix A, A.4) with regard to the German data, results from complete case analyses would have led to higher estimates, i.e., overestimation, compared to analyses with imputed data.
There are some limitations that need to be mentioned. This study is based on cross-sectional data; hence, it is not possible to address temporal association or causal interpretation of associations. It should be noted that our aim was rather to demonstrate the utility of the revised and enhanced JCQ 2.0 by illustrating how well it relates to health and work-related outcomes in comparison to established associations with the original JCQ 1. While the ADC model attempts to provide hypotheses about how changes in psychosocial working conditions could affect health and wellbeing outcomes, the restriction to cross-sectional data in this paper makes it impossible to fully test more dynamic aspects of the ADC hypotheses presented. Certainly, dynamic testing of the full ADC model is thus a necessary empirical next step for the future.
The German sample considered in the study was compared with available register information on the working population living in the city where the study took place (“Mikrozensus”;
https://www.destatis.de/DE/ZahlenFakten/GesellschaftStaat/Bevoelkerung/Mikrozensus.html, accessed on 15 January 2013), indicating lower response among three groups of people: male workers, younger employees, and those with lower levels of education. At the same time, response was higher among the following: those older than 45, women, and those with a higher education level (see also
Appendix A, A.4). As a limitation, one hence has to state that associations might be elevated due to unevenly distributed non-response. As a strength, participants stemmed from very different occupations.
McLinton [
49] assessed the demographics in the randomly selected Australian data against Australian Bureau of Statistics data and found the data to be representative of the national working population sample and job characteristics, supporting the generalizability of the findings.
Since both working conditions and outcomes were self-reported, a common method explanation of the relationships cannot be ruled out. It can hence not be ruled out that associations between working conditions and outcomes are somewhat inflated. However, due to the way the study was designed, it was not possible to assess the working conditions or the health and work-related outcomes via a different method, e.g., through experts.
The iterative JCQ 2.0 development process, allowing for additional scales and items at later stages, led to data in four countries that cannot be compared easily nor analyzed simultaneously for direct comparisons. This is especially true for organizational-level constructs assessed in a limited way in the first two pilots (Korea and China) and therefore not included in this paper. Furthermore, this prevented us from testing the predictive models in these two countries, which would have been an additional strength otherwise. In addition, different health and work-related outcomes were used in the four pilots, and no positive outcomes (e.g., WE, JS) were assessed in the first two pilots, rendering direct comparisons between countries impossible. Further, the measures applied were not the most appropriate ones to test the active work hypothesis (which was only partially confirmed). Therefore, we call for further tests applying more suitable measures that directly assess learning behavior as suggested by DC theory [
11]. Finally, future longitudinal research should pay attention to operationalizing the concepts at the correct level, for instance, sampling data across organizations and assessing organizational concepts at the organizational level through aggregation.


 ,
, 



{kind=link}