
Assessing Neighborhood Characteristics and Their Association with Prenatal Maternal Stress, Depressive Symptoms, and Well-Being in Eight Culturally Diverse Cities: A Cross-Sectional Study

 , , ,
, , ,
Abstract
1. Introduction
The Current Study
2. Materials and Methods
2.1. Data
2.2. Ethics
2.3. Sample
2.4. Procedure
3. Measures
3.1. Neighborhood Characteristics Scales
3.2. Nomological Net Measures
3.3. Analytical Strategy
3.3.1. Factorial Validity and Measurement Invariance
3.3.2. Nomological Networks
4. Results
4.1. Descriptive Statistics
4.2. Internal Consistency
4.3. Factorial Validity
Factorial Structure
4.4. Cross-Country Invariance
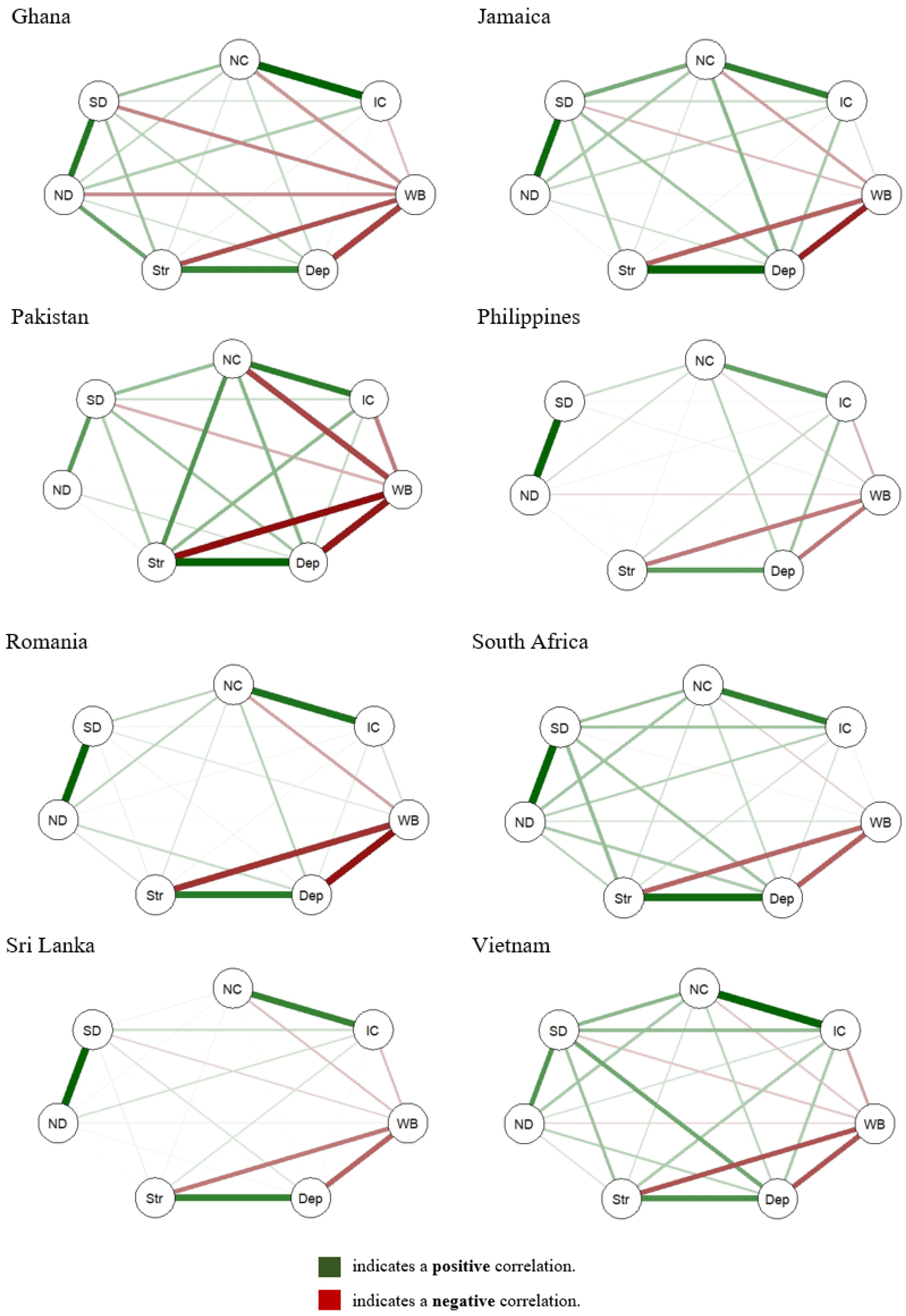
4.5. Nomological Network
5. Discussion
Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barcelona de Mendoza, V.; Harville, E.W.; Savage, J.; Giarratano, G. Experiences of intimate partner and neighborhood violence and their association with mental health in pregnant women. J. Interpers. Violence 2018, 33, 938–959. [Google Scholar]
- Shannon, M.M.; Clougherty, J.E.; McCarthy, C.; Elovitz, M.A.; Nguemeni Tiako, M.J.; Melly, S.J.; Burris, H.H. Neighborhood violent crime and perceived stress in pregnancy. Int. J. Environ. Res. Public Health 2020, 17, 5585. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Kestens, Y.; Dahhou, M.; Daniel, M.; Kramer, M.S. Neighborhood deprivation and maternal psychological distress during pregnancy: A multilevel analysis. Matern. Child Health J. 2015, 19, 1142–1151. [Google Scholar]
- Guildea, Z.; Fone, D.L.; Dunstan, F.; Sibert, J.; Cartlidge, P. Social deprivation and the causes of stillbirth and infant mortality. Arch. Dis. Child. 2001, 84, 307–310. [Google Scholar] [PubMed]
- Kaufman, J.S.; Dole, N.; Savitz, D.A.; Herring, A.H. Modeling community-level effects on preterm birth. Ann. Epidemiol. 2003, 13, 377–384. [Google Scholar] [PubMed]
- Metcalfe, A.; Lail, P.; Ghali, W.A.; Sauve, R.S. The association between neighbourhoods and adverse birth outcomes: A systematic review and meta-analysis of multi-level studies. Paediatr. Perinat. Epidemiol. 2011, 25, 236–245. [Google Scholar]
- Bronfenbrenner, U. Toward an experimental ecology of human development. Am. Psychol. 1977, 32, 513. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Ecological models of human development. Read. Dev. Child. 1994, 2, 37–43. [Google Scholar]
- Marco, M.; Gracia, E.; Tomás, J.M.; López-Quílez, A. Assessing neighborhood disorder: Validation of a three-factor observational scale. Eur. J. Psychol. Appl. Leg. Context 2015, 7, 81–89. [Google Scholar]
- Mujahid, M.S.; Diez Roux, A.V.; Morenoff, J.D.; Raghunathan, T. Assessing the measurement properties of neighborhood scales: From psychometrics to ecometrics. Am. J. Epidemiol. 2007, 165, 858–867. [Google Scholar]
- Cleveland, H.H.; Crosnoe, R. Individual variation and family-community ties: A behavioral genetic analysis of the intergenerational closure in the lives of adolescents. J. Adolesc. Res. 2004, 19, 174–191. [Google Scholar] [CrossRef]
- Valasik, M.; Barton, M.S. The George Wilson effect: Does intergenerational closure and collective efficacy reduce juvenile delinquency in a neighborhood? Deviant Behav. 2018, 39, 1658–1671. [Google Scholar]
- Dupuis, M.; Studer, J.; Henchoz, Y.; Deline, S.; Baggio, S.; N’Goran, A.; Mohler-Kuo, M.; Gmel, G. Validation of French and German versions of a Perceived Neighborhood Social Cohesion Questionnaire among young Swiss males, and its relationship with substance use. J. Health Psychol. 2016, 21, 171–182. [Google Scholar] [CrossRef]
- Harpham, T.; Grant, E.; Thomas, E. Measuring social capital within health surveys: Key issues. Health Policy Plan. 2002, 17, 106–111. [Google Scholar] [PubMed]
- Méndez, M.L.; Otero, G.; Link, F.; López Morales, E.; Gayo, M. Neighbourhood cohesion as a form of privilege. Urban Stud. 2021, 58, 1691–1711. [Google Scholar]
- Damurski, Ł. Neighbourhood cohesion and territorial cohesion: In search for conceptual integrity. GeoJournal 2022, 87, 4635–4651. [Google Scholar]
- Choi, J.K.; Kelley, M.S.; Wang, D. Neighborhood characteristics, maternal parenting, and health and development of children from socioeconomically disadvantaged families. Am. J. Community Psychol. 2018, 62, 476–491. [Google Scholar]
- Sampson, R.J.; Morenoff, J.D.; Earls, F. Beyond social capital: Spatial dynamics of collective efficacy for children. Am. Sociol. Rev. 1999, 64, 633–660. [Google Scholar]
- Coleman, J.S. The relations between school and social structure. In The Social Organization of Schools: New Conceptualizations of the Learning Process; Springer: Berlin/Heidelberg, Germany, 1987; pp. 177–204. [Google Scholar]
- Windzio, M.; Kaminski, P. The dynamics of intergenerational closure and family networks of social cohesion. Front. Sociol. 2023, 8, 933216. [Google Scholar]
- Michalos, A.C. Encyclopedia of Quality of Life and Well-Being Research; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar]
- Nowak, A.L.; Giurgescu, C.; Templin, T.N.; Dailey, R.K.; Misra, D.P. How Depressive Symptoms among African American Women Relate to Measures of Social Disorder in Her Childhood and Pregnancy Neighborhood. J. Urban Health 2020, 97, 26–36. [Google Scholar]
- Vinikoor-Imler, L.; Messer, L.; Evenson, K.; Laraia, B. Neighborhood conditions are associated with maternal health behaviors and pregnancy outcomes. Soc. Sci. Med. 2011, 73, 1302–1311. [Google Scholar] [PubMed]
- Mujahid, M.S.; Wall-Wieler, E.; Hailu, E.M.; Berkowitz, R.L.; Gao, X.; Morris, C.M.; Abrams, B.; Lyndon, A.; Carmichael, S.L. Neighborhood disinvestment and severe maternal morbidity in the state of California. Am. J. Obstet. Gynecol. MFM 2023, 5, 100916. [Google Scholar]
- Sampson, R.J.; Raudenbush, S.W.; Earls, F. Neighborhoods and violent crime: A multilevel study of collective efficacy. Science 1997, 277, 918–924. [Google Scholar] [PubMed]
- Nadan, Y.; Spilsbury, J.C.; Korbin, J.E. Culture and context in understanding child maltreatment: Contributions of intersectionality and neighborhood-based research. Child Abus. Negl. 2015, 41, 40–48. [Google Scholar]
- Baranyi, G.; Sieber, S.; Cullati, S.; Pearce, J.R.; Dibben, C.J.; Courvoisier, D.S. The longitudinal associations of perceived neighborhood disorder and lack of social cohesion with depression among adults aged 50 years or older: An individual-participant-data meta-analysis from 16 high-income countries. Am. J. Epidemiol. 2020, 189, 343–353. [Google Scholar] [PubMed]
- Tarkiainen, L.; Moustgaard, H.; Korhonen, K.; Noordzij, J.M.; Beenackers, M.A.; Van Lenthe, F.J.; Burstrom, B.; Martikainen, P. Association between neighbourhood characteristics and antidepressant use at older ages: A register-based study of urban areas in three European countries. J. Epidemiol. Community Health 2021, 75, 426–432. [Google Scholar]
- Foley, S.; Hughes, C.; Murray, A.L.; Baban, A.; Fernando, A.D.; Madrid, B.; Osafo, J.; Sikander, S.; Abbasi, F.; Walker, S. Prenatal attachment: Using measurement invariance to test the validity of comparisons across eight culturally diverse countries. Arch. Women’s Ment. Health 2021, 24, 619–625. [Google Scholar]
- Murray, A.L.; Hemady, C.L.; Dunne, M.; Foley, S.; Osafo, J.; Sikander, S.; Madrid, B.; Baban, A.; Taut, D.; Ward, C. Measuring antenatal depressive symptoms across the world: A validation and cross-country invariance analysis of the Patient Health Questionnaire–9 (PHQ-9) in eight diverse low resource settings. Psychol. Assess. 2021, 34, 993. [Google Scholar]
- Valdebenito, S.; Murray, A.; Hughes, C.; Băban, A.; Fernando, A.D.; Madrid, B.J.; Ward, C.; Osafo, J.; Dunne, M.; Sikander, S. Evidence for Better Lives Study: A comparative birth-cohort study on child exposure to violence and other adversities in eight low-and middle-income countries-foundational research (study protocol). BMJ Open 2020, 10, e034986. [Google Scholar]
- Cohen, S. Perceived Stress in a Probability Sample of the United States; American Psychological Association: Washington, DC, USA, 1988. [Google Scholar]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [PubMed]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods Psychol. Res. Online 2003, 8, 23–74. [Google Scholar]
- Chen, F.F. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct. Equ. Model. A Multidiscip. J. 2007, 14, 464–504. [Google Scholar]
- Muthén, L.; Muthén, B. The Comprehensive Modelling Program for Applied Researchers: User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 2012. [Google Scholar]
- Epskamp, S.; Cramer, A.; Waldorp, L.; Schmittmann, V.; Borsboom, D. Network visualizations of relationships in psychometric data and structural equation models. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar]
- Katus, L.; Foley, S.; Murray, A.L.; Luong-Thanh, B.-Y.; Taut, D.; Baban, A.; Madrid, B.; Fernando, A.D.; Sikander, S.; Ward, C.L. Perceived stress during the prenatal period: Assessing measurement invariance of the Perceived Stress Scale (PSS-10) across cultures and birth parity. Arch. Women’s Ment. Health 2022, 25, 633–640. [Google Scholar]
- Nguyen, T.; Chang, P.P.; Loh, J.M. The psychology of Vietnamese tiger mothers: Qualitative insights into the parenting beliefs and practices of Vietnamese-Australian mothers. J. Fam. Stud. 2014, 20, 48–65. [Google Scholar]
- Tran, N.K.; Van Berkel, S.R.; van IJzendoorn, M.H.; Alink, L.R. Child and family factors associated with child maltreatment in Vietnam. J. Interpers. Violence 2021, 36, NP2931–NP2953. [Google Scholar]
- Jones, E. The courtesy bias in South-East Asian surveys. In Social Research in Developing Countries; Psychology Press: Hove, UK, 1993; pp. 253–259. [Google Scholar]
- Edwards, L.M.; Le, H.-N.; Garnier-Villarreal, M. A systematic review and meta-analysis of risk factors for postpartum depression among Latinas. Matern. Child Health J. 2021, 25, 554–564. [Google Scholar]
- Westland, H.; Vervoort, S.; Kars, M.; Jaarsma, T. Interviewing people on sensitive topics: Challenges and strategies. Eur. J. Cardiovasc. Nurs. 2024, 2, 128. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.S.; Langhout, R.D. “A community with diversity of culture, wealth, resources, and living experiences”: Defining neighborhood in an unincorporated community. Am. J. Community Psychol. 2014, 53, 122–133. [Google Scholar] [PubMed]
- Bhui, K.; Mohamud, S.; Warfa, N.; Craig, T.J.; Stansfeld, S.A. Cultural adaptation of mental health measures: Improving the quality of clinical practice and research. Br. J. Psychiatry 2003, 183, 184–186. [Google Scholar]
- Adebayo, Y.O.; Adesiyan, R.E.; Amadi, C.S.; Ipede, O.; Karakitie, L.O.; Adebayo, K.T. Cross-cultural perspectives on mental health: Understanding variations and promoting cultural competence. World J. Adv. Res. Rev. 2024, 23, 432–439. [Google Scholar] [CrossRef]
- National Collaborating Centre for Mental Health, and National Institute for Health and Clinical Excellence. Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance; British Psychological Society and Gaskell: London, UK, 2020. [Google Scholar]

{kind=link}
| Ghana | Jamaica | Pakistan | Philippines | Romania | South Africa | Sri Lanka | Vietnam | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | |
| 2.12 | (1.09) | 2.67 | (1.10) | 1.99 | (1.13) | 1.93 | (0.85) | 1.93 | (0.53) | 2.19 | (1.08) | 1.57 | (0.63) | 1.59 | (0.69) |
| 2.12 | (1.05) | 2.56 | (1.02) | 2.00 | (1.12) | 1.80 | (0.88) | 1.79 | (0.59) | 1.97 | (1.03) | 1.66 | (0.67) | 1.57 | (0.68) |
| 1.74 | (0.89) | 2.81 | (1.09) | 1.58 | (0.81) | 1.80 | (0.85) | 1.75 | (0.57) | 2.11 | (1.06) | 1.67 | (0.64) | 1.63 | (0.68) |
| 2.63 | (1.14) | 3.08 | (0.99) | 1.97 | (1.01) | 2.15 | (0.97) | 1.87 | (0.55) | 2.51 | (1.12) | 2.16 | (0.84) | 1.88 | (0.81) |
| 1.59 | (0.90) | 3.04 | (0.97) | 2.92 | (1.15) | 2.10 | (0.94) | 2.17 | (0.63) | 2.71 | (1.11) | 2.17 | (0.81) | 2.14 | (0.75) |
| 1.73 | (0.99) | 1.79 | (0.91) | 2.72 | (1.21) | 1.80 | (0.89) | 1.75 | (0.58) | 1.93 | (1.07) | 1.79 | (0.65) | 1.84 | (0.75) |
| 1.89 | (1.07) | 1.92 | (0.97) | 2.74 | (1.27) | 1.52 | (0.71) | 1.93 | (0.70) | 1.70 | (0.94) | 2.08 | (0.89) | 2.31 | (1.04) |
| 1.96 | (0.98) | 2.14 | (1.0) | 1.90 | (0.98) | 1.51 | (0.80) | 1.82 | (0.63) | 1.65 | (0.93) | 1.95 | (0.71) | 2.09 | (0.95) |
| 1.77 | (0.91) | 1.56 | (0.78) | 1.54 | (0.79) | 1.43 | (0.67) | 1.78 | (0.67) | 1.47 | (0.80) | 1.74 | (0.61) | 1.53 | (0.69) |
| 1.81 | (1.08) | 2.27 | (1.17) | 2.26 | (1.32) | 2.60 | (1.17) | 1.82 | (0.98) | 2.48 | (1.23) | 2.50 | (1.26) | 1.75 | (0.82) |
| 1.73 | (1.05) | 2.16 | (1.21) | 2.14 | (1.32) | 2.47 | (1.25) | 1.81 | (1.03) | 2.28 | (1.25) | 2.26 | (1.29) | 1.48 | (0.79) |
| 2.10 | (1.13) | 2.03 | (1.11) | 1.75 | (1.13) | 2.17 | (1.17) | 1.78 | (0.97) | 2.23 | (1.20) | 1.93 | (1.07) | 1.71 | (0.92) |
| 1.93 | (1.11) | 1.98 | (1.08) | 1.99 | (1.18) | 2.13 | (1.24) | 2.05 | (1.04) | 2.25 | (1.16) | 2.10 | (1.17) | 1.45 | (0.78) |
| 1.84 | (1.11) | 1.66 | (0.97) | 1.39 | (0.89) | 2.30 | (1.26) | 1.38 | (0.82) | 2.16 | (1.23) | 1.95 | (1.19) | 1.41 | (0.70) |
| 1.97 | (1.11) | 1.76 | (0.97) | 1.43 | (0.87) | 2.40 | (1.23) | 1.65 | (0.93) | 2.75 | (1.23) | 2.24 | (1.22) | 1.53 | (0.75) |
| 1.86 | (1.10) | 2.45 | (1.25) | 1.32 | (0.82) | 1.91 | (1.25) | 1.45 | (0.82) | 2.99 | (1.29) | 2.08 | (1.28) | 1.41 | (0.73) |
| 1.95 | (1.12) | 2.66 | (1.14) | 1.54 | (0.94) | 2.10 | (1.19) | 1.30 | (0.73) | 2.83 | (1.23) | 2.01 | (1.16) | 1.57 | (0.78) |
| 2.26 | (1.29) | 2.20 | (1.28) | 1.86 | (1.12) | 1.96 | (1.17) | 1.29 | (0.70) | 2.93 | (1.28) | 1.76 | (1.16) | 1.33 | (0.70) |
| Ghana | Jamaica | Pakistan | Philippines | Romania | South Africa | Sri Lanka | Vietnam | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | M | (SD) | |
| Perceived stress | ||||||||||||||||
| 1.66 | (0.84) | 2.24 | (1.01) | 1.74 | (1.00) | 1.83 | (0.90) | 1.44 | (0.50) | 1.99 | (1.07) | 1.70 | (0.62) | 1.43 | (0.52) |
| 1.72 | (0.94) | 2.04 | (1.14) | 1.55 | (0.96) | 1.59 | (0.78) | 1.39 | (0.54) | 1.69 | (0.94) | 1.37 | (0.66) | 1.41 | (0.53) |
| 1.91 | (0.93) | 2.16 | (1.10) | 1.89 | (1.17) | 2.06 | (0.98) | 1.89 | (0.60) | 1.93 | (1.11) | 1.62 | (0.64) | 1.67 | (0.65) |
| 2.75 | (0.86) | 2.38 | (1.04) | 2.16 | (1.16) | 1.97 | (1.12) | 1.72 | (0.86) | 2.32 | (1.25) | 1.94 | (1.20) | 2.29 | (1.10) |
| 2.86 | (0.97) | 2.70 | (1.04) | 2.47 | (1.16) | 2.45 | (1.08) | 1.69 | (0.80) | 2.43 | (1.14) | 2.42 | (1.16) | 2.35 | (1.04) |
| 1.81 | (0.83) | 2.30 | (1.10) | 1.82 | (1.05) | 1.63 | (0.87) | 1.95 | (0.79) | 2.11 | (1.11) | 1.66 | (0.88) | 1.60 | (0.77) |
| 2.88 | (0.92) | 2.58 | (1.01) | 2.46 | (1.11) | 2.52 | (1.10) | 1.78 | (0.92) | 2.52 | (1.20) | 2.35 | (1.19) | 2.01 | (1.07) |
| 2.96 | (1.00) | 2.77 | (1.07) | 3.73 | (0.70) | 2.45 | (1.17) | 1.59 | (0.75) | 2.37 | (1.16) | 2.65 | (1.24) | 1.79 | (0.95) |
| 1.81 | (0.91) | 2.46 | (1.06) | 1.75 | (0.90) | 2.01 | (1.06) | 1.74 | (0.66) | 2.42 | (1.19) | 1.66 | (0.80) | 1.65 | (0.60) |
| 1.63 | (0.90) | 2.13 | (1.14) | 1.86 | (1.15) | 1.83 | (1.04) | 1.27 | (0.49) | 1.91 | (1.14) | 1.64 | (0.91) | 1.33 | (0.59) |
| Well-being | ||||||||||||||||
| 2.56 | (1.69) | 3.28 | (1.46) | 2.66 | (1.85) | 3.34 | (1.66) | 3.86 | (0.79) | 3.04 | (1.57) | 3.50 | (1.52) | 3.43 | (1.44) |
| 2.84 | (1.70) | 2.83 | (1.56) | 2.76 | (1.88) | 3.16 | (1.69) | 3.62 | (1.00) | 3.55 | (1.52) | 3.21 | (1.55) | 3.44 | (1.49) |
| 2.47 | (1.63) | 2.78 | (1.57) | 1.99 | (1.94) | 3.36 | (1.72) | 3.31 | (1.17) | 3.40 | (1.55) | 3.03 | (1.63) | 2.89 | (1.57) |
| 2.39 | (1.65) | 2.56 | (1.67) | 2.63 | (2.04) | 3.25 | (1.74) | 2.91 | (1.35) | 3.23 | (1.64) | 2.99 | (1.69) | 2.92 | (1.62) |
| 2.05 | (1.59) | 2.63 | (1.60) | 2.34 | (2.04) | 3.03 | (1.80) | 3.90 | (0.98) | 3.11 | (1.72) | 3.26 | (1.61) | 3.51 | (1.52) |
| Depressive symptoms | ||||||||||||||||
| 0.89 | (0.94) | 1.32 | (1.07) | 1.10 | (1.19) | 1.07 | (0.97) | 0.65 | (0.59) | 1.19 | (1.14) | 0.70 | (0.75) | 0.65 | (0.61) |
| 0.77 | (0.96) | 1.03 | (1.04) | 0.91 | (1.18) | 0.80 | (0.95) | 0.27 | (0.52) | 0.63 | (1.00) | 0.63 | (0.80) | 0.33 | (0.58) |
| 1.38 | (0.99) | 1.43 | (1.15) | 1.35 | (1.36) | 1.39 | (0.99) | 1.18 | (0.88) | 1.37 | (1.17) | 1.04 | (0.88) | 1.20 | (0.85) |
| 1.39 | (0.89) | 1.67 | (1.05) | 2.05 | (1.16) | 1.22 | (0.93) | 1.18 | (0.76) | 1.08 | (1.13) | 1.04 | (0.87) | 0.99 | (0.77) |
| 1.01 | (0.99) | 1.26 | (1.14) | 1.39 | (1.34) | 0.92 | (1.07) | 0.85 | (0.82) | 1.12 | (1.16) | 0.72 | (0.83) | 0.81 | (0.87) |
| 0.65 | (0.91) | 0.55 | (0.97) | 0.37 | (0.84) | 0.66 | (0.92) | 0.19 | (0.49) | 0.33 | (0.79) | 0.30 | (0.58) | 0.27 | (0.55) |
| 0.52 | (0.85) | 0.71 | (1.10) | 0.37 | (0.86) | 0.66 | (0.93) | 0.41 | (0.75) | 0.38 | (0.86) | 0.30 | (0.64) | 0.51 | (0.70) |
| 0.48 | (0.75) | 0.73 | (0.99) | 0.59 | (0.93) | 0.56 | (0.86) | 0.35 | (0.58) | 0.47 | (0.91) | 0.47 | (0.73) | 0.40 | (0.61) |
| 0.32 | (0.80) | 0.36 | (0.83) | 0.13 | (0.46) | 0.17 | (0.51) | 0.03 | (0.16) | 0.25 | (0.78) | 0.17 | (0.56) | 0.06 | (0.33) |
| CFI | TLI | SRMR | RMSEA | RMSEA 90% CI | |
|---|---|---|---|---|---|
| Ghana | 0.94 | 0.93 | 0.11 | 0.08 | [0.07, 0.10] |
| Jamaica | 0.96 | 0.95 | 0.07 | 0.05 | [0.03, 0.06] |
| Pakistan | 0.98 | 0.98 | 0.10 | 0.07 | [0.05, 0.08] |
| Philippines | 0.99 | 0.98 | 0.07 | 0.05 | [0.04, 0.07] |
| Romania | 0.98 | 0.98 | 0.08 | 0.06 | [0.04, 0.07] |
| South Africa | 0.98 | 0.97 | 0.07 | 0.06 | [0.04, 0.07] |
| Sri Lanka | 0.99 | 0.99 | 0.07 | 0.05 | [0.02, 0.06] |
| Vietnam | 0.96 | 0.96 | 0.08 | 0.07 | [0.05, 0.08] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campo-Tena, L.; Roman, G.D.; Murray, A.L.; Luong-Thanh, B.Y.; Marlow, M.; Anwer, Y.; Dadzie, A.; Foley, S.; Hernandez, S.S.; Lindsay, C.; et al. Assessing Neighborhood Characteristics and Their Association with Prenatal Maternal Stress, Depressive Symptoms, and Well-Being in Eight Culturally Diverse Cities: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2025, 22, 456. https://doi.org/10.3390/ijerph22030456
Campo-Tena L, Roman GD, Murray AL, Luong-Thanh BY, Marlow M, Anwer Y, Dadzie A, Foley S, Hernandez SS, Lindsay C, et al. Assessing Neighborhood Characteristics and Their Association with Prenatal Maternal Stress, Depressive Symptoms, and Well-Being in Eight Culturally Diverse Cities: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2025; 22(3):456. https://doi.org/10.3390/ijerph22030456
Chicago/Turabian StyleCampo-Tena, Laura, Gabriela Diana Roman, Aja Louise Murray, Bao Yen Luong-Thanh, Marguerite Marlow, Yasmeen Anwer, Awurabena Dadzie, Sarah Foley, Sandra Stuart Hernandez, Carene Lindsay, and et al. 2025. "Assessing Neighborhood Characteristics and Their Association with Prenatal Maternal Stress, Depressive Symptoms, and Well-Being in Eight Culturally Diverse Cities: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 22, no. 3: 456. https://doi.org/10.3390/ijerph22030456
APA StyleCampo-Tena, L., Roman, G. D., Murray, A. L., Luong-Thanh, B. Y., Marlow, M., Anwer, Y., Dadzie, A., Foley, S., Hernandez, S. S., Lindsay, C., Randeny, S., Smith, J. A., Taut, D., & Eisner, M. P. (2025). Assessing Neighborhood Characteristics and Their Association with Prenatal Maternal Stress, Depressive Symptoms, and Well-Being in Eight Culturally Diverse Cities: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 22(3), 456. https://doi.org/10.3390/ijerph22030456