Abstract
Due to several interpersonal, social, and organizational challenges, dental health has been occasionally compromised in the transgender population. There is a lack of awareness among transgender persons to access affordable trans-competent oral health care. More information is required to identify and assess the oral health condition of this population in order to encourage better access to oral healthcare and effectively influence public health policy and practice. This systematic review aims to provide evidence about the status of oral health and hygiene of the transgender population across the globe. A systematic literature search using keywords and MESH search terms was conducted using PubMed, Medline, Google Scholar, and EBSCO online databases. The references of included journal articles were manually searched and appropriate studies were included, which were then critically appraised using the Joanna Briggs Institute (JBI) tool and the Newcastle–Ottawa protocol for the risk of bias assessment of prevalence studies, with each study assessed by two independent reviewers. Based on the search procedures, a total of 2026 articles were initially screened and, after evaluation, 20 were included in the systematic review. Transgender persons often face stigma and discrimination in dental healthcare settings, which affects their oral health status. A greater prevalence of substance abuse stemming from anxiety, lack of adequate education, and poor socioeconomic status leads to an increased prevalence of oral health diseases in this marginalized population. There is a need for policies and reforms to appraise their oral health and hygiene status and improve access to oral health services in this population.
1. Introduction
Bockting, in the year 1999, first defined transgender persons as “individuals who cross or transcend culturally defined categories of gender.” [1]. Globally, there is outstanding dynamism in dismantling stereotypical barriers concerning the transgender population to create a receptive society in which the ability to express one’s gender is normal and not a privilege. For decades now, this community has been struggling to breach the prejudice they are subjected to in the form of violence, harassment, unacceptability, and denial of human rights, and the sphere of health care services and dental health care is no exception [1].
According to the World Health Organization (WHO), oral health is defined as a state of being free of mouth and facial pain, oral infections and sores, and oral and other diseases that limit an individual’s capacity to bite, chew, smile, and speak, as well as their psychosocial well-being. The importance of oral health in governing an individual’s overall health, well-being, and quality of life is indispensable. Oral diseases commonly comprise dental decay, periodontal disease, tooth loss, and oral cancer, including oral manifestations of HIV infection, which are the commonest of chronic diseases and sustain a significant portion of public health problems because of their prevalence, their repercussions on the comprehensive health of individuals and society, and hefty expenses associated with their treatment [2].
Many obstacles in areas as diverse as social, financial, interpersonal, and health eventually affect how transgender people view getting medical care. At a social level, their unacceptance puts them through emotional instability, shame, fear, and internalized transphobia. Poor health literacy, lack of familiarity with the health care system, facilities, and insurance, as well as financial restrictions, contribute to an increased prevalence of HIV and drug abuse, including alcohol and tobacco use. Transgender individuals face discrimination by health care workers, with inadequate consideration, knowledge, and empathy, verbal and physical harassment, and direct refusal or reluctance to provide treatment [3,4]. Dental care professionals are reported to deny oral health services more likely than physicians, considering their sexual orientation and gender expression with greater apathy [5]. In a study conducted by Heima et al. to assess dental fear among transgender individuals, 14.2% of participants indicated they were “very much” or “extremely” fearful of experiencing maltreatment in a dental clinic [6]. Lack of competent training, decrepit curriculum, and a deficiency of receptive care environments among dental professionals eventually contribute to increased risk of poor oral health.
The transgender population faces significant barriers in accessing equitable healthcare, particularly in oral health, a domain that has received little attention in research and policy discourse. Discrimination, financial instability, and lack of gender-affirming care contribute to significant disparities in oral health outcomes. Despite growing advocacy for transgender rights, there is a persistent knowledge gap regarding their oral health status on a global scale.
As the field of transgender health research continues to expand, there is a growing need for dynamic and adaptive evidence synthesis methods. A promising approach is the concept of ‘living systematic reviews’, which involve periodic updates to integrate new findings in real time. Unlike traditional systematic reviews that provide a snapshot of available evidence at a fixed point in time, living systematic reviews continuously evolve, ensuring that healthcare professionals, researchers, and policymakers have access to the most current data. Implementing this approach for transgender oral health research would allow for a more responsive and up-to-date understanding of disparities, risk factors, and intervention strategies, ultimately fostering more inclusive and equitable healthcare policies.
This living systematic review and meta-analysis aims to fill this gap by synthesizing the available global evidence on the oral health and hygiene status of transgender individuals, such as dental caries, periodontitis, oral lesions, tooth loss, and oral hygiene status.
The central hypothesis guiding this review is that transgender individuals experience significantly poorer oral health outcomes than cisgender populations, driven by a combination of social stigma, economic challenges, and barriers to healthcare access. By systematically evaluating the existing literature, this study seeks to identify patterns, quantify disparities, and highlight areas requiring further research and policy intervention.
2. Materials and Methods
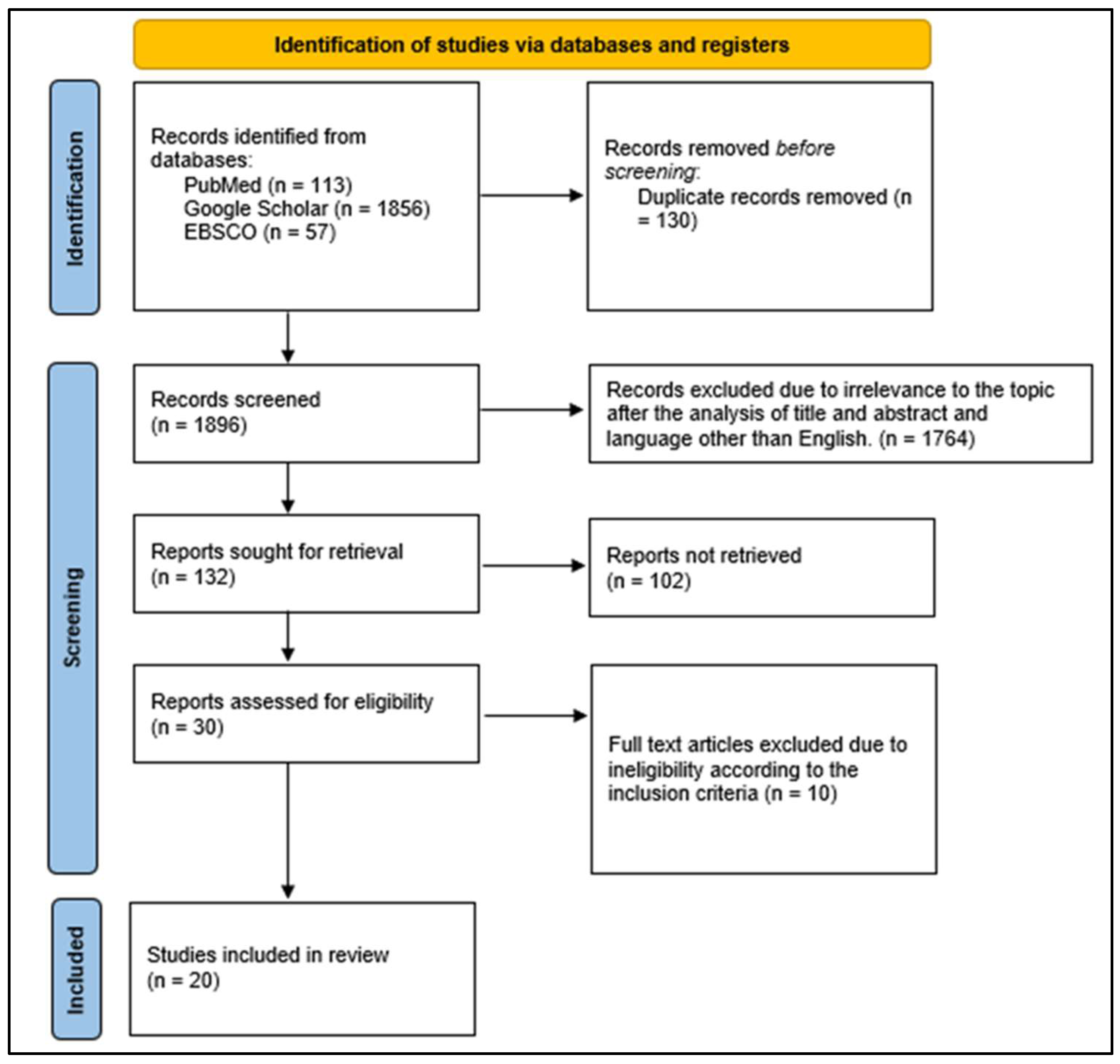
This living systematic review and meta-analysis has been structured in agreement with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-E 2012 checklist and is registered on PROSPERO (International Prospective Register of Systematic Reviews) (protocol number: CRD42021272384) [7]. An ethics review was not mandated since this was a systematic review that was based on the compilation of secondary literature from the articles included in the study (Figure 1).
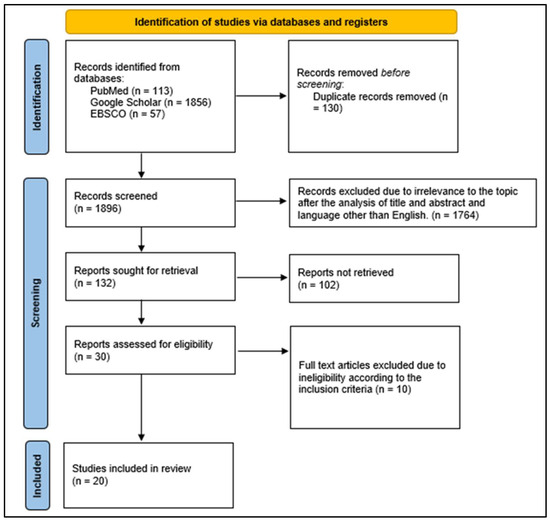
Figure 1.
PRISMA flowchart—identification of studies via databases and registers.
It was conducted with the hypothesis that transgender individuals experience disproportionately poorer oral health outcomes due to structural barriers and social determinants of health. Our study design aimed to identify and quantify disparities in oral health outcomes across different transgender subgroups, assess patterns in healthcare access, and highlight policy gaps. The review was structured to address key research questions, including: (1) What are the primary oral health challenges faced by transgender individuals globally? (2) How do these disparities compare to those observed in cisgender populations? (3) What factors contribute to these disparities, and what policy interventions can mitigate them?
Population (P): Individuals who identify themselves as transgender.
Outcome (O): Evaluating the oral health and dental hygiene status among the transgender population, including their oral hygiene practices; oral hygiene status as measured by the Oral Hygiene Index Simplified (OHI-S); periodontal status as measured by the Calculus Index (CI), Plaque Index (PI), Clinical Attachment Loss (CAL), Community Periodontal Index and Treatment Needs (CPITN), Modified Gingival Index (MGI), Modified Community Periodontal Index (M-CPI), and Probing Pocket Depth (PPD); dental caries as measured by the Decayed-Missing-Filled-Treatment index (DMFT) and any other modes of measurement used; malocclusion; premalignant lesions; and any other relevant oral findings.
Study design (S): The studies which have been considered are observational cross-sectional (descriptive studies) and cohort studies and original research papers.
2.1. Inclusion and Exclusion Criteria
The studies of interest were all descriptive studies conducted among the transgender population to assess their oral health, hygiene, and diseases. The articles were restricted to those published until August 2021 in English and available in full text only. Table 1 illustrates the summary of the included articles.

Table 1.
Characteristics and details of included studies.
The articles without full texts, incomplete information to answer the question of interest, and published in a language other than English where translation into English was not available were excluded. An attempt was made to distinguish any unpublished articles and contact published study authors for additional/missing information. The excluded articles and the reasons for their exclusion are shown in Table 2.
Table 2.
List of excluded studies.
2.2. Search Strategy
Free text words and MeSH terms were utilized, comprising the headings of ((Transgender) OR (transsexual) OR (eunuch) OR (lgbtq) OR (Third gender) OR (Sexual minority)) AND ((Dentition status) OR (Dental caries) OR (Tobacco) OR (periodontal status) OR (Clinical attachment loss) OR (Calculus index) OR (Plaque index) OR (Pocket depth) OR (Oral hygiene habits) OR (Oral hygiene status) OR (Oral cancer) OR (oral mucosal lesions) OR (malocclusion) OR (Dental decay)).
2.3. Studies with Outdated or Inappropriate Terminology Such as ‘Eunuchs’
Excluding studies solely based on outdated terminology would introduce selection bias, potentially leading to an incomplete representation of transgender oral health status in certain regions. Some older studies and studies from specific cultural contexts used terms such as “eunuchs” or other terminology that, while now considered outdated or inappropriate, historically referred to populations within the broader transgender spectrum.
In many countries, particularly in South Asia (e.g., India, Pakistan, and Bangladesh), legally recognized third-gender identities (e.g., Hijra communities) have been studied under various terminologies in both academic and clinical literature. While these terms may not align with modern transgender identity classifications, they represent a significant population group that experiences oral health disparities.
Completely excluding studies based on terminology rather than methodological rigor would result in a significant loss of valuable data, particularly from regions where contemporary transgender health research is limited.
2.4. Mitigation Strategies to Address Terminology Concerns
To ensure inclusivity and accuracy while maintaining methodological rigor, the following steps were undertaken:
- Standardization of Terminology in Data Synthesis: Regardless of the terminology used in the original studies, all extracted data were systematically categorized under standardized, inclusive terminology in our analysis and discussion.
- Transparent Reporting and Acknowledgment: We explicitly acknowledge that certain included studies employed outdated terminology and provided necessary clarifications to avoid misrepresentation or insensitivity.
- Sensitivity Review and Ethical Considerations: The manuscript has undergone a review to ensure that our synthesized findings use affirming and appropriate language in line with contemporary standards in transgender health research.
2.5. Search Databases
An electronic literature search of PubMed, Medline, Google Scholar, and EBSCO online databases was conducted from September 2021 to November 2021.
2.6. Data Extraction
Two reviewers independently assessed the search results based on the title and abstract for initial screening. They then accessed and screened the full texts of the eligible articles. In case of discrepancies in data extraction, both reviewers developed consensus before making a decision. Rayyan QCRI software was used to remove duplicates, and MS Excel 2010 was used to store the data.
The following details were extracted from the included articles: author, year of publication, population characteristics, assessment tool used, outcome measure, and findings. The extracted data were tabulated using MS Excel 2010.
Data were extracted, including four domains:
- Identification of the study (article type; journal type; author; country of the study; language; publication year; host institution of the study);
- Methodological characteristics (study design; study objective; research question; sample characteristics, e.g., sample size, sex; age, statistical analysis);
- Main findings;
- Conclusions.
The authors were approached for any missing data in the studies. The year of publication was used as the year of data collection from the studies, which did not report the year of data collection.
2.7. Quality Assessment
- Risk of Bias
After data extraction, the reviewers independently assessed the possible risk of bias among eligible studies using a specific protocol developed to analyze cross-sectional studies, the Newcastle–Ottawa Scale, which was adapted to the outcomes evaluated in this review along with the Joanna Briggs Institute (JBI) tool for the assessment of prevalence studies. Reviewers scored the papers that adequately fulfilled each methodological criterion and provided a score with a maximum of 9 points in the JBI tool and 10 in the Newcastle–Ottawa Scale, according to the parameters considered. Parameters that did not apply to this revision also received scores and entered the computation of final points as mentioned in Table 3.
Table 3.
Risk of bias assessment for included studies.
2.8. Statistical Analysis
- Assessment of Heterogeneity
Dichotomous data were expressed as risk ratios with 95% confidence intervals. Continuous measurement scales or ordinal data were expressed using the mean and standard deviation. Heterogeneity was evaluated using the I2 test with an alpha of 0.10. Review Manager (Revman V.5.3) was used for data synthesis. Meta-analyses were conducted by considering the prevalence of dental caries and periodontal disease as outcomes. Sensitivity analyses were also performed, with each study excluded sequentially. A Forest plot was used to verify the possible presence of publication bias.
3. Results
A systematic literature search using keywords and MESH search terms was conducted using PubMed (n = 113), Google Scholar (n = 1856), and EBSCO (n = 57) online databases. Of the 20 included studies in the current systematic review, 18 studies [8,10,11,12,13,14,15,16,17,18,19,20,22,23,24,25,26,27] were conducted in India while 1 study [9] was conducted in Malaysia and 1 study [21] was conducted in Iowa City.
Figure 2, Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7 depict the main results of the meta-analyses regarding the prevalence of dental caries, periodontal disease, oral mucosal lesions, and calculus, respectively.
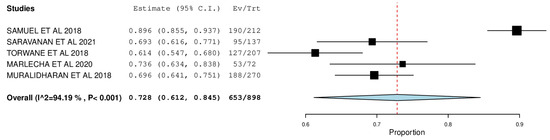
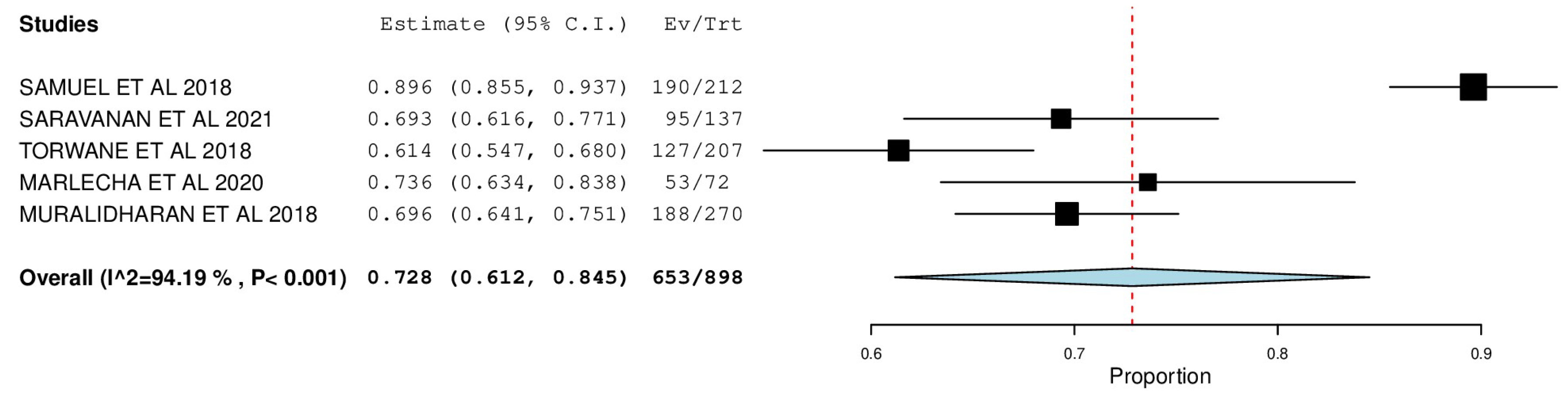
Figure 2.
Forest plot depicting the prevalence of decayed teeth.
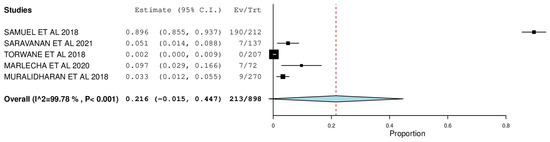
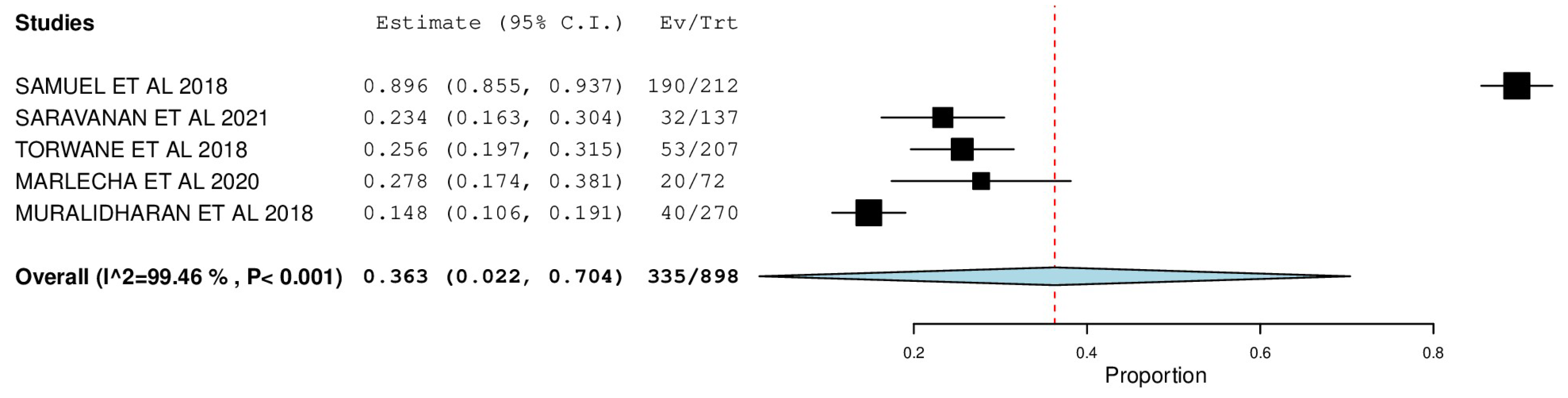
Figure 3.
Forest plot depicting the prevalence of filled teeth.
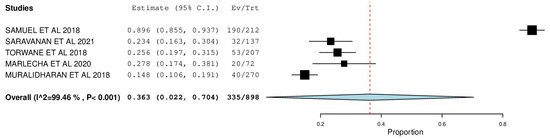
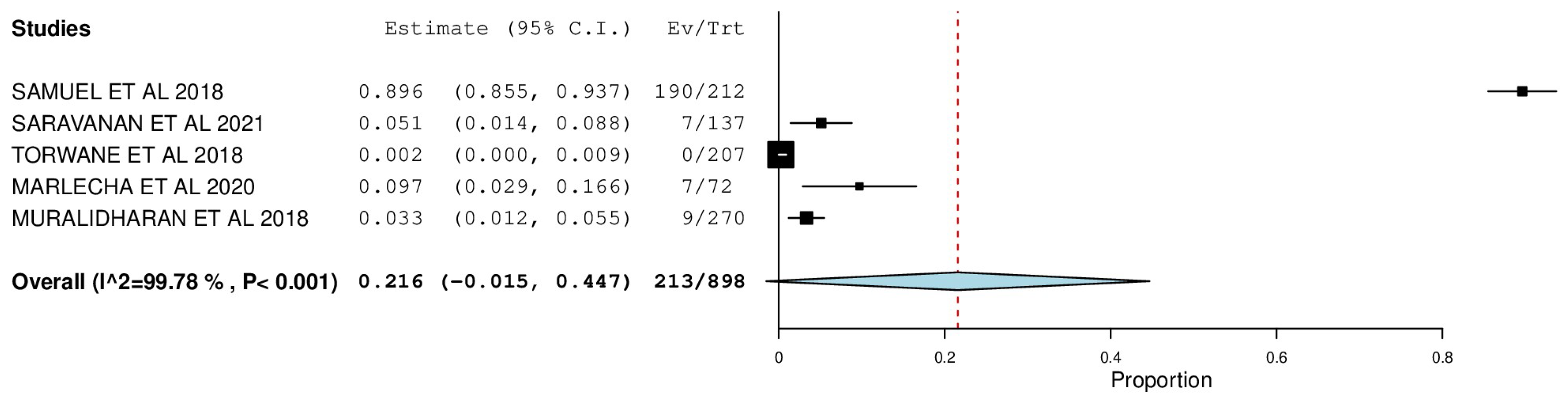
Figure 4.
Forest plot depicting the prevalence of missing teeth.
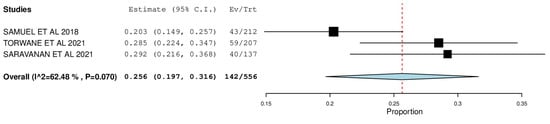
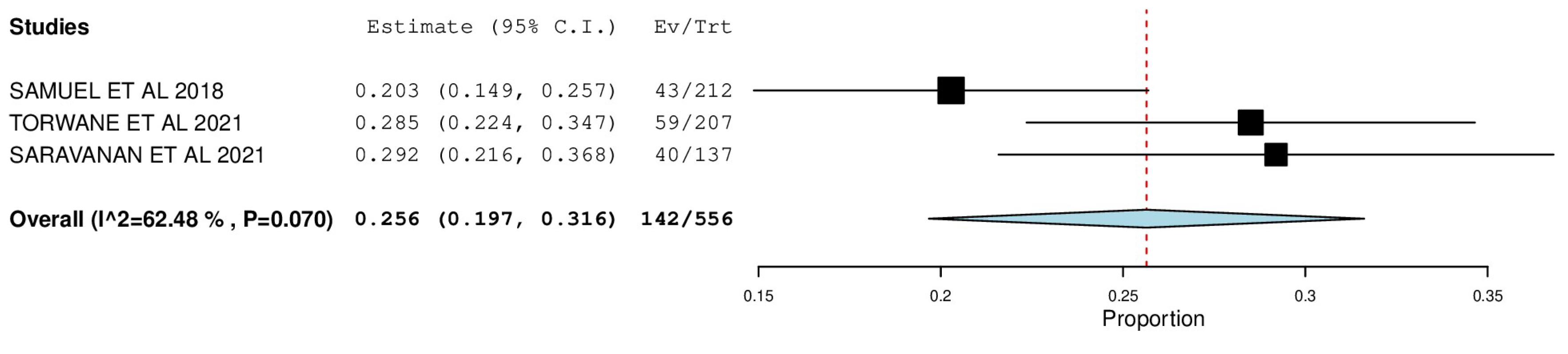
Figure 5.
Forest plot depicting the prevalence of oral mucosal lesions.
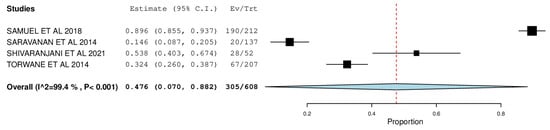
Figure 6.
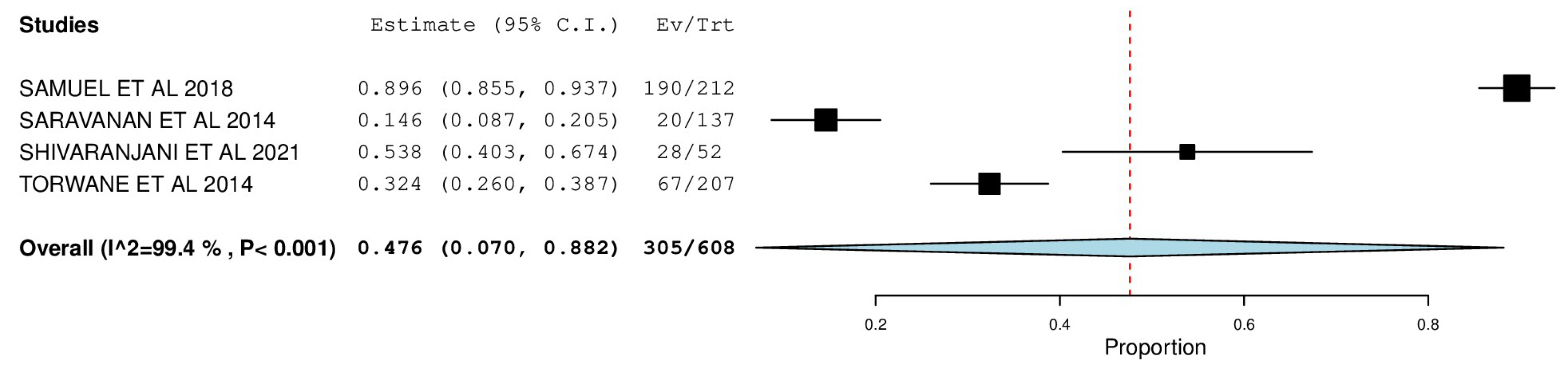
Forest plot depicting the prevalence of periodontal status as measured by pocket probing depth.
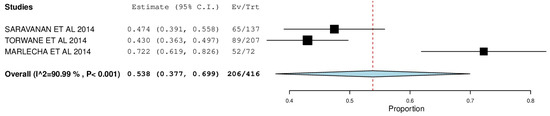
Figure 7.
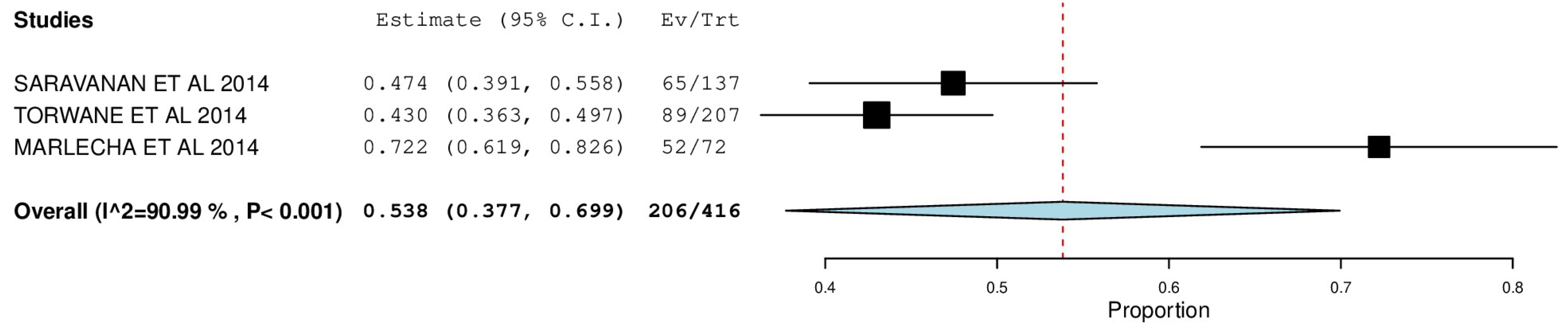
Forest plot depicting the prevalence of oral hygiene status as measured by the presence of calculus.
The overall mean difference for decayed teeth was reported in 5 studies, which was 0.72, having a precision of 0.63 to 0.84. The results obtained were statistically significant (p-value < 0.05) (Figure 2).
The overall mean difference for filled teeth was reported in 5 studies, which was 0.36, having a precision of 0.02 to 0.70. The results obtained were statistically significant (p-value < 0.05) (Figure 3).
The overall mean difference for missing teeth was reported in 5 studies, which was 0.22, having a precision of −0.01 to 0.44. The results obtained were statistically significant (p-value < 0.05) (Figure 4).
The overall mean difference for oral mucosal lesions was reported in 3 studies, which was 0.25, having a precision of 0.19 to 0.31. The results obtained were not statistically significant (p-value > 0.05) (Figure 5).
The overall mean difference for periodontal status was reported in 4 studies, which was 0.47, having a precision of 0.07 to 0.89. The results obtained were statistically significant (p-value < 0.05) (Figure 6).
The overall mean difference for oral hygiene status was reported in 3 studies, which was 0.53, having a precision of 0.37 to 0.69. The results obtained were statistically significant (p-value < 0.05) (Figure 7).
Heterogeneity among the included studies was observed in both analyses (p < 0.001), and the analyses were considered to have high heterogeneity based on the I2 test (prevalence of decayed teeth—I2 = 94.19%; prevalence of missing teeth—I2 = 99.46%; prevalence of filled teeth—I2 = 99.78%; prevalence of periodontal disease—I2 = 99.4%; prevalence of oral mucosal lesions—I2 = 62.48%; prevalence of calculus—I2 = 90.99%.
3.1. Oral Mucosal Lesions
In the analysis of the included studies, the pooled prevalence of oral mucosal lesions was 25.6% (95% CI: 0.197, 0.316). The forest plot depicting the proportion of prevalence of the lesions in each study indicated that the study by Saravanan et al. had the highest prevalence—29.2% (95% CI: 0.216, 0.368), and that by Samuel et al. had the lowest—20.3% (95% CI: 0.149, 0.257). According to Samuel et al. [22], a more significant proportion of the population was affected with leukoplakia (26%), which was similar to findings put forth by Torwane et al. [25] (28.90%), with leukoplakia being the major lesion (7.7%). However, while Saravanan et al. [17] depicted an overall occurrence close to that reported by Torwane et al. (29.2%), his target population was significantly affected by candidiasis (13.9%).
3.2. Periodontal Status
Five studies were included in studying periodontal status via a forest plot with a pooled prevalence of 47.6% (95% CI: 0.070, 0.882). Samuel et al. reported the highest prevalence—89.6% (95% CI: 0.855, 0.937), and Saravanan et al. reported the lowest—14.6% (95% CI: 0.087, 0.205). The Calculus Index measured the presence of the calculus to estimate the target population’s oral hygiene status. A forest plot was designed with a pooled prevalence of 53.8% (95% CI: 0.377, 0.699). Torwane et al. reported the lowest prevalence—43% (95% CI: 0.363, 0.497), and Marlecha et al. reported the highest—72.2% (95% CI: 0.619, 0.826). Kalyan et al. [10] reported a significant prevalence of gingivitis (98.9%) and periodontitis (94.27%) among transgender persons, which was in congruence with findings by Torwane et al. [8] (92.8%) and Saravanan et al. [17] (83%).
3.3. Dental Caries
The percent DMF among the included studies was meta-analyzed to study the caries experience among the transgender population. In congruence with the forest plot, the highest prevalence was reported by Samuel et al.—D: 89.6% (95% CI: 0.855, 0.937), M: 89.6% (95% CI:0.855, 0.937), F: 89.6% (95% CI: 0.855, 0.937) and the lowest prevalence was reported by Torwane et al.—D: 61.4% (95% CI: 0.547, 0.680), M: 25.6% (95% CI: 0.197, 0.315), F: 00.2% (95% CI: 0.000, 0.009), with the pooled prevalence of D, M, and F being 72.8% (95% CI: 0.612, 0.845), 36.3% (95% CI: 0.022, 0.704), and 21.6% (95% CI: −0.015, 0.447), respectfully. A noteworthy conclusion one can draw from this forest plot is that while the treatment needs of this population seem high, the proportion of filled teeth is comparatively very low, which indicates poor utilization of dental services and inadequate knowledge regarding oral health diseases, leading to accumulated oral health problems that are majorly left untreated.
3.4. Risk of Bias Assessment
Of the 20 studies, 4 studies depicted 9/9 (100%) scores [10,18,22,27] having low risk of bias and strong methodological rigor. Nine studies [8,9,14,15,16,19,23,24,25] depicted 8/9 (88.8%) scores showing moderate risk of bias but were still reliable. Six studies had 7/9 (77.7%) scores [11,12,13,17,21,26] having moderate-to-high risk of bias, possibly due to missing methodological elements and only one study with 66.6% [20] showed high risk of bias, indicating concerns about study quality.
- Expected Heterogenous Variability in Global Meta-Analyses
The observed heterogeneity (I2 values above 90%) in this systematic review and meta-analysis reflects the inherent variations in study populations, methodologies, and reported outcomes across the included studies. However, rather than being an indication of methodological flaws, such heterogeneity is expected in a global synthesis of oral health data for transgender individuals, a population that faces diverse socio-cultural, economic, and healthcare-related barriers across different regions.
3.5. Diverse Study Designs and Populations
The included studies span multiple countries, each with different healthcare systems, cultural perceptions of transgender health, and accessibility to oral healthcare services. Such diversity naturally results in variability in reported oral health outcomes, contributing to heterogeneity. However, this is not necessarily a weakness but rather an expected feature of global epidemiological studies. Some studies used clinical examinations by trained professionals, while others relied on self-reported oral health status, introducing variability in outcome assessment.
3.6. Variability in Oral Health Determinants
The transgender population experiences unique challenges such as gender-affirming hormone therapy (GAHT), social determinants of health, and healthcare disparities, which differ significantly across studies. These factors influence oral health outcomes and contribute to heterogeneity.
3.7. Statistical Handling of Heterogeneity
While I2 values above 90% indicated substantial heterogeneity, random-effects models were employed to account for between-study variability, ensuring robust effect size estimates. Furthermore, sensitivity analyses were conducted to assess the impact of individual studies, ensuring that no single study disproportionately influenced the pooled results.
Sensitivity analysis was performed as part of our methodological rigor to assess the stability of the pooled effect sizes by removing high-variance studies. However, the results indicated no significant deviation from the primary meta-analysis outcomes, confirming that the overall findings were robust.
To ensure that the high heterogeneity did not compromise the validity of pooled estimates, the following statistical methodologies were rigorously applied:
Random-Effects Model (DerSimonian and Laird method) was deployed, which assumes that effect sizes vary across studies due to real differences rather than sampling error alone. Removing studies based on variance alone may introduce bias, as heterogeneity in effect sizes is expected due to real-world differences in transgender populations’ oral health across regions.
Leave-One-Out Sensitivity Analysis was performed to assess whether any single study disproportionately influenced the results. The effect sizes remained stable across iterations, confirming robustness. We systematically re-ran analyses by omitting each study individually to test its influence on the overall results. No single study was found to disproportionately impact the pooled estimates. This supports the robustness of our findings, negating the necessity of excluding high-variance studies arbitrarily.
Tau-Squared (τ2) Estimation and Prediction Intervals were calculated to quantify between-study variance beyond I2. This provides a more accurate representation of heterogeneity than I2 alone.
- Reporting Limitations and Data Constraints Regarding Subgroup Analysis
Lack of Stratified Data: Many of the included studies did not provide stratified results based on age, region, or access to oral healthcare, preventing meaningful subgroup analyses. Conducting subgroup analyses on limited sample sizes would introduce small-study bias and reduce statistical power, leading to unreliable conclusions.
Heterogeneous Reporting of Key Covariates: Some studies provided aggregate data for cisgender and transgender individuals combined, limiting our ability to extract transgender-specific subgroup data.
4. Discussion
In light of transgender persons being deliberated as a marginalized population facing extensive stigmatization and discrimination in the field of dental health care with increased frequency of unmet dental needs, the current systematic review maps the oral health and hygiene status of transgender persons.
The results of this systematic review strongly support the hypothesis that transgender individuals face significant oral health disparities due to systemic inequities. Across multiple studies, we observed patterns of poorer oral hygiene, higher rates of untreated dental diseases, and lower utilization of dental services among transgender populations. These findings align with broader public health research indicating that social determinants—such as discrimination, economic marginalization, and limited access to competent healthcare—play a crucial role in shaping health outcomes for transgender individuals.
In relevance to the 20 studies narrowed down to discern the oral health and hygiene status of transgender persons, four studies depicted a significant prevalence of oral mucosal lesions among them, which could be attributed to transgender persons of lower socioeconomic status and comparatively ill-educated being considerably prone to substance abuse in the form of tobacco and alcohol, as stated in the studies conducted by Stronks et al. [38] and Dangi et al. [39]. In a study performed to analyze the relationship between substance abuse and the occurrence of oral mucosal lesions, Mehrotra et al. [40] found that smokers and chewers among their target population were more afflicted than non-users. Samuel et al. stated that around 87.9% to 92.6% of his sample population were slum dwellers and relied on begging as their source of income, while 99% of the sample population of Torwane et al. belonged to a lower socioeconomic class.
Six studies reported that the dental caries experience ranged from 69.3%, as in that by Saravanan et al. [17], which was in congruence with those by Torwane et al. [8] (67.3%) and Muralidharan et al. [16] (69.6%) but was slightly higher in statistics in those by Marlecha et al. [20] (73.6%) and Ovia et al. (87%). Several factors could contribute to this population’s ubiquitous prevalence of dental caries. Increased frequency of sugar intake was standard in the studies by Torwane et al. and Saravanan et al., an essential parameter that should be considered while assessing dental caries. The population groups of these studies reported poor utilization of dental healthcare facilities, lower socioeconomic status, and inadequate knowledge regarding oral healthcare, including poor practices involving materials used to brush their teeth and the frequency of brushing. In accordance with the studies quoted above, a scarce population of only 26.9 to 42.3% preferred visiting a dentist, coupled with a lack of transgender-friendly dental facilities, discrimination in dental settings, and accumulated dental treatment needs due to unaffordability could condone the susceptibility of this population to dental decay. These factors were akin to the studies by Farah et al. [9], Prasanth et al. [13], Kumar et al. [14], and Shivaranjan et al. [18].
A noteworthy finding among all of the studies included in the systematic review was that the majority of them focused on the periodontal status of the transgender population. The presence of bleeding gums and calculus, markers of poor periodontal status, were reported by four studies, with occurrence ranging from 8.8 to 69% for bleeding gums and 43 to 72.2% for calculus. There was a broad difference in results computed for loss of attachment among transgender persons in studies by Saravanan et al. [17] (16.8%) and Marlecha et al. [20] (40.3%), which could be the fact that 60% of Marlecha et al.’s sample population had never visited a dentist before, leading to untreated and accumulated dental needs. Out of all the studies reporting pocket depth, Torwane et al. had the highest prevalence rate (32.4%) when compared to others (Shivaranjani et al.—15%, Saravana et al.—14.6%), which can be associated with greater tobacco use (90.3%) among its sample population. In consideration of the findings from the abovementioned studies, several factors influence a more significant proportion of transgender persons being affected by periodontal diseases, including increased stress-cortisol levels (Shivaranjani et al. [16]), deleterious habits such as tobacco chewing and smoking, which in turn lead to increased levels of periodontal pathogens in shallow and deep periodontal pockets, altered neutrophil chemotaxis, phagocytosis, and oxidative burst, increased TNF–α and PGE2 levels in gingival crevicular fluid (GCF), neutrophil collagenase and elastase in GCF, and production of PGE2 by monocytes [41]. Considering these findings, it is imperative to understand that oral health is linked to overall health and that poor dental health is associated with high levels of inflammation, poor diet quality, and conditions such as disability, diabetes, and increased risk of cardiovascular disease and pneumonia. Various factors like bacteremia, the release of inflammatory mediators, acute phase reactants, and alterations in immune responses could be possible links between the high prevalence of dental diseases and deteriorating overall health [42,43].
Inadequate knowledge regarding oral conditions, reluctance to visit a dentist, and poor oral hygiene further worsen periodontal status, as also reported by L. Ekanayake in a study conducted to assess the correlation between tobacco use and oral hygiene as a risk indicator for periodontitis [44].
The systematic review sought to standardize oral hygiene practices among transgender people since poor oral hygiene is the root cause of declining oral health. Nine out of the twenty included studies mentioned findings about the knowledge, attitude, and practice of transgender persons regarding the importance of oral hygiene. Farah et al. [9], Kumar et al. [14], Hongal et al. [15], and Prasant et al. [13] reported that their target populations were significantly aware of the importance of brushing, and 87.8% brushed their teeth at least once daily. Moreover, 65.3 to 86.1% of them preferred a toothbrush and toothpaste to clean their teeth (Kumar et al., Prasant et al., Saravanan et al., Kalyan et al., and Hongal et al.). Oral hygiene status was further measured with the help of the OHI-S index among four studies, of which Prasanth et al. reported that only 17% of transgender persons had good oral hygiene and 40% of them did not, which was similar to the findings by Kaur et al. in their study to assess the oral hygiene status of mentally and physically challenged individuals [45].
Comparing the oral health status of transgender and non-transgender populations reveals some significant differences. In a study conducted by Luiz et al. assessing the oral health related quality of life in the LGBTIQ+ population, 44.8% of transgender individuals reported frequent or severe oral health issues, whereas only 28.3% of cisgender individuals experienced similar issues. This difference was primarily attributed to transgender individuals with lower educational levels, lower family income, difficulty accessing dental treatment, and suicidal ideation or mental health issues as compared to the cisgender population [46].
Therefore, extensive research has yet to be conducted to decipher the oral health needs of the transgender community, how their oral health requirement varies, and how, as a health care provider, one can assist them adequately since one’s oral hygiene practices do influence one’s vulnerability to oral disease.
Of all of the included studies, only Marlecha et al. assessed malocclusion among transgender persons, with 80.55% of them having class 1 malocclusion and the rest having class 2 and class 3 malocclusion. Scarce data on such findings may be due to the fact that aesthetic considerations are seldom a priority among this community and that the collected data may be insignificant compared to other populations. Another unique study assessed the palatal rugae pattern among the transgender population. Palatoscopy is used in forensic sciences to determine a person’s identification, as it mirrors a person’s genetic makeup. The findings revealed that the rugae length was lesser and wavier, was more forwardly and backwardly directed, and had diverging rugae compared to the male and female control populations. This may serve as a step ahead in studying the genetic makeup and ethnic and racial differences of this community.
One of the inherent challenges of regular systematic reviews is the necessity of a fixed search period to ensure methodological rigor and reproducibility. In this study, our literature search was conducted until November 2021, meaning that any research published after this period was not included in our current analysis. Given the rapidly evolving nature of transgender health research, we acknowledge that more recent studies may offer additional insights that could further enrich our current findings. However, adhering to a pre-specified search window was critical to prevent selective reporting bias and maintain transparency in evidence synthesis. Since this is a living systematic review, newly published data in real time would be periodically updated and published (biennially or triennially, depending on the incidence of fresh publications), ensuring that emerging evidence continues to inform clinical practice and policy development.
Quite a few of the included studies did end up using the incorrect terminology and gender insensitive and no-inclusive discriminatory verbiage for the target population [17,22,25].
While we recognize the importance of distinguishing between different transgender subgroups (e.g., transgender women, transgender men, non-binary individuals, gender-diverse populations), many of the included studies did not stratify their data accordingly. This limitation prevented a statistically meaningful subgroup analysis without introducing significant bias due to small sample sizes within subgroups.
Given that oral health disparities among transgender individuals are largely influenced by systemic healthcare access issues rather than gender identity subcategories alone, aggregating the data into a single transgender category was deemed to be the most methodologically sound approach.
While attempts have been made in isolation to ascertain the oral health needs of the transgender population, most of them end up being thesis or research-oriented, offering minimal translational service for their treatment needs.
4.1. Oral Health Disparities Between Transgender and Cisgender Populations
Oral health disparities exist within all marginalized populations, but transgender individuals face unique structural, social, and medical challenges that exacerbate these disparities. To better understand these inequities, it is important to contrast transgender-specific factors with those affecting the broader cisgender population. This living systematic review helps bridge the knowledge gap between cisgender and transgender oral health disparities and lays the groundwork for future research that can quantitatively compare these populations in a matched-study format.
- Prevalence and General Trends
Studies on cisgender populations indicate that oral health disparities are largely driven by socioeconomic factors, healthcare access, education, and behavioral habits [46]. By contrast, transgender populations experience these same disparities in addition to gender identity-related stressors, such as discrimination in healthcare settings, stigma, and lack of culturally competent providers [35]. Several population-based studies indicate that cisgender individuals have greater access to preventive dental care, lower rates of untreated oral disease, and better oral health literacy than transgender individuals, particularly in countries where transgender-inclusive healthcare policies are lacking [3].
- Social Determinants of Health (SDOH) and Their Role in Oral Health Disparities
Healthcare Access: Cisgender individuals generally experience fewer barriers to healthcare compared to transgender individuals, who often report denial of treatment, lack of gender-affirming care, and fear of discrimination from dental professionals.
Economic Stability: Transgender populations are disproportionately affected by unemployment and economic instability, limiting their ability to afford dental services, whereas cisgender individuals have higher rates of employment-linked dental insurance coverage.
Psychosocial Stress and Behavioral Differences: The minority stress theory suggests that transgender individuals are at higher risk for engaging in adverse health behaviors (e.g., smoking, substance use) due to social marginalization, which contributes to increased periodontal disease and caries prevalence. These behavioral patterns differ significantly from those of cisgender individuals, who do not experience gender-related stressors at the same intensity.
- Inclusion of Contextual Data from Existing Literature
Although this living systematic review did not perform a direct comparative analysis between transgender and cisgender populations due to data limitations, we integrated existing evidence on cisgender oral health trends to better contextualize the findings.
Caries and periodontal disease prevalence in cisgender populations studies on global oral health indicate that dental caries and periodontal disease remain prevalent among cisgender individuals, particularly among lower-income groups. Population-based studies in high-income countries suggest that cisgender adults report lower rates of untreated caries than transgender individuals, likely due to greater access to routine dental care. By contrast, transgender individuals often experience higher levels of untreated oral diseases due to financial constraints and discrimination in dental settings.
4.1.1. Comparison of Dental Visit Frequency and Preventive Care Utilization
Cisgender individuals are more likely to undergo regular dental checkups and receive preventive treatments, such as fluoride application and professional cleaning. Among transgender populations, studies indicate a significantly lower frequency of dental visits, often due to fear of being misgendered or receiving inadequate care from uninformed dental professionals. The inclusion of studies from lower-income countries suggests that oral health disparities among cisgender individuals are often linked to economic barriers, whereas transgender individuals face both economic barriers and additional gender-related healthcare discrimination.
There is a need for a targeted and focused comprehensive program ranging from care to cure to meet and explore the oral health needs of the transgender population. Translational and implementation steps should be adopted to carry forward this research data and fabricate the desired treatment needs that these sections of the population need. Incorporating culturally competent didactic and clinical learning experiences into the education of future oral health professionals may enhance the delivery of relevant and high-quality health care to the minority transgender population [47].
A recent study [48] contributed valuable insights into the oral health challenges faced by transgender populations. While this study was published around the same time as our search period, its findings align with the broader trends identified in our review, reinforcing the systemic disparities affecting this community. Although it was not included in our current meta-analysis due to predefined search parameters, its relevance highlights the importance of ongoing research in this domain. Since this is a living systematic review, further studies will be updated to this metaset periodically.
4.1.2. Specific Recommendations to Improve the Field
Need for Comparative Studies—Future studies should be designed to include both transgender and cisgender populations in the same analysis while controlling for key confounding variables such as socioeconomic status, insurance coverage, access to healthcare services, and comorbid health conditions (e.g., HIV, diabetes, smoking status). Studies that fail to account for these confounders risk over- or underestimating the true disparities between transgender and cisgender populations.
Need for Matched-Control Studies—To obtain statistically valid and generalizable comparisons, future research should implement matched-control study designs, in which transgender and cisgender individuals are matched on relevant demographic and socioeconomic factors to ensure comparability. Stratified analyses by gender identity (transgender women, transgender men, non-binary individuals) should be conducted to explore subgroup-specific disparities. Large-scale population-based cohort studies are needed to assess long-term oral health trends among transgender individuals in comparison to their cisgender counterparts.
Call for Culturally Competent Oral Health Interventions—Public health programs, such as the Kartavya model by Kumar et al. [3], should incorporate targeted outreach and education to address the oral health disparities in transgender communities, ensuring equitable access to preventive and restorative dental care and proper salutations without pre-emptive misgendering or using culturally inappropriate terminologies. Dental health professionals should receive gender-affirming training to improve the oral healthcare experience for transgender individuals Dental professionals and policymakers must work collaboratively to create gender-affirming oral health initiatives that address the unique needs of transgender individuals.
One limitation of this systematic review is the variability in diagnostic criteria used across studies to define oral diseases such as periodontitis. Some studies relied on standardized guidelines (e.g., CDC/AAP case definitions), while others used broader or unspecified clinical assessments. Such discrepancies can lead to differences in reported prevalence and contribute to heterogeneity in our findings. To account for this, we conducted heterogeneity assessments (I2 statistics) and, where applicable, sensitivity analyses to evaluate the impact of diagnostic variations on pooled estimates. Despite these methodological differences, the overall trends in oral health disparities among transgender individuals remain consistent across studies, emphasizing the need for standardized diagnostic protocols in future research.
To improve the comparability of findings in future research, there is a pressing need for standardized diagnostic criteria for oral diseases, particularly in marginalized populations such as transgender individuals. Future studies should aim to adopt uniform case definitions (e.g., CDC/AAP for periodontitis) and ensure examiner calibration to minimize inter-study variability. Additionally, the implementation of globally recognized oral health assessment protocols, as outlined by the WHO, could enhance data consistency across different geographic regions and healthcare settings. Establishing these standards will allow for more precise cross-cultural comparisons and facilitate evidence-based policymaking to address oral health disparities.
5. Conclusions
This living systematic review and meta-analysis underscores the indigent oral health and hygiene status of the global transgender population, reinforcing the growing body of evidence on transgender health disparities. By adopting a dynamic and evolving approach, this review enables real-time tracking of trends, advancements in dental care, and the impact of shifting healthcare policies, ensuring that transgender oral health remains a continuously updated research priority.
Our findings validate the disproportionately poorer oral health outcomes experienced by transgender individuals, largely driven by systemic inequalities. These disparities highlight an urgent need for targeted research, policy reforms, and structural interventions to achieve equitable access to oral healthcare worldwide.
As authors, we believe that there is an urgent need to develop preventive and curative modules that aim at their inclusivity and acceptability in healthcare facilities, thereby appraising their oral health-related quality of life. This will not only enhance their overall health and tenacity but also instill in them positive dental health behavior, overarching the equitable ethos of establishing affirmative, accessible, acceptable, and affordable oral healthcare.
Author Contributions
Conceptualization, V.K. and A.R.; methodology, V.K., J.T. and Z.D.B.; software, N.B.; validation, V.K., A.R. and J.T.; formal analysis, V.K. and N.B.; investigation, V.K. and J.T.; resources, V.K.; data curation, V.K. and N.B.; writing—original draft preparation, V.K. and J.T.; writing—A.R. and Z.D.B.; visualization, N.B.; supervision, V.K. and A.R.; project administration, Z.D.B.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Bockting, W.O.; Miner, M.H.; Swinburne Romine, R.E.; Hamilton, A.; Coleman, E. Stigma, Mental Health, and Resilience in an Online Sample of the US Transgender Population. Am. J. Public Health 2013, 103, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A. Oral Health, General Health and Quality of Life. Bull. World Health Organ. 2005, 83, 644. [Google Scholar] [PubMed]
- Kumar, V.; Jain, R.; Singh, S. Kartavya: An Innovative Model to Deliver Oral Health Services to the Transgender Community in India. Spec. Care Dentist 2021, 41, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Pandya, A.K.; Redcay, A. Access to Health Services: Barriers Faced by the Transgender Population in India. J. Gay Lesbian Ment. Health 2021, 25, 132–154. [Google Scholar] [CrossRef]
- Kass, N.E.; Faden, R.R.; Fox, R.; Dudley, J. Homosexual and Bisexual Men’s Perceptions of Discrimination in Health Services. Am. J. Public Health 1992, 82, 1277–1279. [Google Scholar] [CrossRef]
- Heima, M.; Heaton, L.J.; Ng, H.H.; Roccoforte, E.C. Dental Fear Among Transgender Individuals—A Cross-Sectional Survey. Spec. Care Dentist 2017, 37, 212–222. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Arjun, T.N.; Dayma, A.; Joshi, K.R.; Mishra, M.; Singh, V.R.; Khanal, L.R. Assessment of Dentition Status and Treatment Needs Among Eunuchs Residing in Bhopal City, Madhya Pradesh, India: A Cross-Sectional Survey. Int. J. Prev. Clin. Dent. Res. 2018, 5, S28–S34. [Google Scholar]
- Mohd, F.N.; Said, A.H.; Ali, A.; Draman, W.L.; Aznan, M.; Aris, M. Oral Health-Related Quality of Life Among Transgender Women in Malaysia. Alcohol 2022, 47, 47–55. [Google Scholar]
- Kalyan, P.; Dave, B.; Deshpande, N.; Panchal, D. A Study to Assess the Periodontal Status of Eunuchs Residing in Central Gujarat, India: A Cross-Sectional Study. Adv. Hum. Biol. 2020, 10, 162. [Google Scholar] [CrossRef]
- Saravanan, N.; Thiruneervannan, R.; Christopher, P. A Study to Assess the Periodontal Status of Transgender in Chennai City. Biosci. Biotech. Res. 2014, 11, 1673–1677. [Google Scholar] [CrossRef]
- Peeran, S.W.; Thiruneervannan, M.; Kumar, N.; Almarshoudi, S.; Ahmed, F.M. Oral Hygiene and Periodontal Status Among Eunuchs in Chennai, India. EC Dent. Sci. 2017, 15, 123–126. [Google Scholar]
- Prasanth, B.K.; Mahalakshmi, K.; Umadevi, R.; Kalpana, S.; Anantha, V.M. Knowledge on Oral Hygiene Practices and Assessment of Oral Health Status Among Transgender Community Residing in Chennai Metropolitan City—A Descriptive Cross-Sectional Study. Eur. J. Mol. Clin. Med. 2020, 7, 2020. [Google Scholar]
- Kumar, G.; Sethi, A.K.; Bagchi, A.; Rai, S.; Tamilselvan, P. Knowledge, Attitudes and Behaviour Towards Oral Hygiene of Transgenders in Bhubaneswar During COVID-19. J. Fam. Med. Prim. Care 2021, 10, 1353. [Google Scholar] [CrossRef] [PubMed]
- Hongal, S.; Torwane, N.A.; Goel, P.; Byarakele, C.; Mishra, P.; Jain, S. Oral Health-Related Knowledge, Attitude and Practices Among Eunuchs (Hijras) Residing in Bhopal City, Madhya Pradesh, India: A Cross-Sectional Questionnaire Survey. J. Indian Soc. Periodontol. 2014, 18, 624. [Google Scholar]
- Muralidharan, S.; Acharya, A.; Koshy, A.V.; Koshy, J.A.; Yogesh, T.L.; Khire, B. Dentition Status and Treatment Needs and Its Correlation with Oral Health-Related Quality of Life Among Men Having Sex with Men and Transgenders in Pune City: A Cross-Sectional Study. J. Oral Maxillofac. Pathol. 2018, 22, 443. [Google Scholar] [CrossRef]
- Saravanan, N.; Reddy, C.V.; Veeresh, D.J. A Study to Assess the Oral Health Status and Treatment Needs of Eunuchs in Chennai City. J. Indian Assoc. Public Health Dent. 2006, 4, 22. [Google Scholar] [CrossRef]
- Shivaranjani, K.; Pratebha, B.; Muthu, J.; Saravanakumar, R.; Karthikeyan, I. Change in Periodontal Status, Oral Health Knowledge, Attitude, and Practices Following Video-Based Counseling: A Cross-Sectional Study. J. Mahatma Gandhi Inst. Med. Sci. 2021, 26, 36. [Google Scholar] [CrossRef]
- Ovia, M.; Revathi, D.; Ganapathty, D. Oral Hygiene in Transgender of Chennai City. Drug Invent. Today 2019, 11, 235–240. [Google Scholar]
- Marlecha, R.; Mary, V.; An, K.; Christopher, P.; Nagavalli, K.; Salam, H. Oral Health Status, Dental Awareness, and Dental Services Utilization Barriers Among Transgender Population in Chennai. Drug Invent. Today 2020, 14, 1143–1148. [Google Scholar]
- Adekugbe, O.C. Oral Health Status and Dental Service Utilization of Persons Who Identify as Lesbian, Gay, Bisexual, Transgender, and Queer in Iowa City. ProQuest Diss. Publ. 2020, 28030187. [Google Scholar] [CrossRef]
- Samuel, S.R.; Muragaboopathy, V.; Patil, S. Transgender HIV Status, Self-Perceived Dental Care Barriers, and Residents’ Stigma, Willingness to Treat Them in a Community Dental Outreach Program: Cross-Sectional Study. Spec. Care Dentist 2018, 38, 307–312. [Google Scholar] [CrossRef]
- Sivaranjani, K.; Balu, P.; Kumar, R.S.; Muthu, J.; Devi, S.S.; Priyadharshini, V. Correlation of Periodontal Status with Perceived Stress Scale Score and Cortisol Levels Among Transgenders in Puducherry and Cuddalore. SRM J. Res. Dent. Sci. 2020, 11, 52–57. [Google Scholar] [CrossRef]
- Saxena, E.; Chandrashekhar, B.R.; Hongal, S.; Torwane, N.; Goel, P.; Mishra, P. A Study of the Palatal Rugae Pattern Among Male, Female, and Transgender Population of Bhopal City. J. Forensic Dent. Sci. 2015, 7, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Torwane, N.A.; Hongal, S.; Goel, P.; Chandrashekar, B.; Saxena, V. Assessment of Oral Mucosal Lesions Among Eunuchs Residing in Bhopal City, Madhya Pradesh, India: A Cross-Sectional Study. Indian J. Public Health 2015, 59, 24–29. [Google Scholar] [CrossRef]
- Prasanth, B.K.; Mahalakshmi, K.; Umadevi, R.; Kalpana, S.; Anantha Eashwar, V.M. Assessment of Micronuclei in the Exfoliated Buccal Mucosal Cells Based on the Personnel Behavior Among the Transgender Population of Tamil Nadu. Ann. Rom. Soc. Cell Biol. 2021, 25, 4307–4313. [Google Scholar]
- Torwane, N.; Hongal, S.; Saxena, E.; Rana, P.; Jain, S.; Gouraha, A. Assessment of Periodontal Status Among Eunuchs Residing in Bhopal City, Madhya Pradesh, India: A Cross-Sectional Study. Oral Health Dent. Manag. 2014, 13, 628–633. [Google Scholar]
- Żyła, T.; Kawala, B.; Antoszewska-Smith, J.; Kawala, M. Black Stain and Dental Caries: A Review of the Literature. Biomed. Res. Int. 2015, 2015, 469392. [Google Scholar] [CrossRef]
- Roberts, S.J. Health Care of Sexual Minority Women. Nurs. Clin. North Am. 2018, 53, 227–239. [Google Scholar] [CrossRef]
- Gheit, T.; Rollo, F.; Brancaccio, R.N.; Robitaille, A.; Galati, L.; Giuliani, M.; Latini, A.; Pichi, B.; Benevolo, M.; Cuenin, C.; et al. Oral Infection by Mucosal and Cutaneous Human Papillomaviruses in Men Who Have Sex with Men from the OHMAR Study. Viruses 2020, 12, 899. [Google Scholar] [CrossRef]
- Kauth, M.R.; Barrera, T.L.; Denton, F.N.; Latini, D.M. Health Differences Among Lesbian, Gay, and Transgender Veterans by Rural/Small Town and Suburban/Urban Setting. LGBT Health 2017, 4, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Al-Shammari, K.F.; Al-Ansari, J.M.; Al-Khabbaz, A.K.; Dashti, A.; Honkala, E.J. Self-Reported Oral Hygiene Habits and Oral Health Problems of Kuwaiti Adults. Med. Princ. Pract. 2007, 16, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Segal, N.L. Performing Together: Monozygotic Twin Comedians/Twin Research: Mirror-Image Cleft Lip and Palate; Dental Caries; Noninvasive Prenatal Testing; Capgras Syndrome with Folie à Deux/In the News: Athletic Twins; Transgendered Twins; Crib-Sharing; Common Careers. Twin Res. Hum. Genet. 2019, 22, 70–74. [Google Scholar] [CrossRef]
- Macdonald, D.W.; Grossoehme, D.H.; Mazzola, A.; Pestian, T.; Schwartz, S.B. Transgender Youth and Oral Health: A Qualitative Study. J. LGBT Youth 2020, 17, 92–106. [Google Scholar] [CrossRef]
- Russell, S.; More, F. Addressing Health Disparities via Coordination of Care and Interprofessional Education: Lesbian, Gay, Bisexual, and Transgender Health and Oral Health Care. Dent. Clin. North Am. 2016, 60, 891–906. [Google Scholar] [CrossRef]
- Parish, C.L.; Santella, A.J. A Qualitative Study of Rapid HIV Testing and Lesbian, Gay, Bisexual, Transgender, and Queer Competency in the Oral Health Setting: Practices and Attitudes of New York State Dental Directors. Oral Health Prev. Dent. 2018, 16, 343–350. [Google Scholar]
- Coulter, R.W.S.; Kenst, K.S.; Bowen, D.J. Research Funded by the National Institutes of Health on the Health of Lesbian, Gay, Bisexual, and Transgender Populations. Am. J. Public Health 2014, 104, e105–e112. [Google Scholar] [CrossRef]
- Charles, A.; Stronks, K.; Tromp, N.; Bhopal, R.; Zaninotto, P.; Unwin, N.; Nazroo, J.; Kunst, A. A Cross-National Comparative Study of Smoking Prevalence and Cessation Between English and Dutch South Asian and African Origin Populations: The Role of National Context. Nicotine Tob. Res. 2010, 12, 557–566. [Google Scholar] [CrossRef]
- Dangi, J.; Kinnunen, T.H.; Zavras, A.I. Challenges in Global Improvement of Oral Cancer Outcomes: Findings from Rural Northern India. Tob. Induc. Dis. 2012, 10, 5. [Google Scholar] [CrossRef]
- Gupta, K.; Mehrotra, M.; Kumar, P.; Gogia, A.R.; Prasad, A.; Fisher, J.A. Smoke Inhalation Injury: Etiopathogenesis, Diagnosis, and Management. Indian J. Crit. Care Med. 2018, 22, 180. [Google Scholar] [CrossRef]
- Newman, M.G.; Takei, H.; Carranza, F.A. (Eds.) Clinical Periodontology, 9th ed.; WB Saunders Company: Philadelphia, PA, USA, 2002; pp. 245–252. [Google Scholar]
- Kotronia, E.; Brown, H.; Papacosta, A.O.; Lennon, L.T.; Weyant, R.J.; Whincup, P.H.; Wannamethee, S.G.; Ramsay, S.E. Oral Health and All-Cause, Cardiovascular Disease, and Respiratory Mortality in Older People in the UK and USA. Sci. Rep. 2021, 11, 16452. [Google Scholar] [CrossRef] [PubMed]
- Gianos, E.; Jackson, E.A.; Tejpal, A.; Aspry, K.; O’Keefe, J.; Aggarwal, M.; Jain, A.; Itchhaporia, D.; Williams, K.; Batts, T.; et al. Oral Health and Atherosclerotic Cardiovascular Disease: A Review. Am. J. Prev. Cardiol. 2021, 7, 100179. [Google Scholar] [CrossRef]
- Amarasena, N.; Ekanayaka, A.N.; Herath, L.; Miyazaki, H. Tobacco Use and Oral Hygiene as Risk Indicators for Periodontitis. Community Dent. Oral Epidemiol. 2002, 30, 115–123. [Google Scholar] [CrossRef]
- Kaur, S.; Malhotra, R.; Malhotra, R.; Kaur, H.; Battu, V.S.; Kaur, A. Oral Hygiene Status of Mentally and Physically Challenged Individuals Living in a Specialized Institution in Mohali, India. Indian J. Oral Sci. 2013, 4, 17. [Google Scholar] [CrossRef]
- Almeida, L.E.; Almeida, P.F.; Oliveira, V.D.; Mialhe, F.L. Oral Health-Related Quality of Life in the LGBTIQ+ Population: A Cross-Sectional Study. Braz. Oral Res. 2024, 38, e041. [Google Scholar] [CrossRef]
- Dysart-Gale, D. Cultural Sensitivity Beyond Ethnicity: A Universal Precautions Model. Int. J. Allied Health Sci. Pract. 2006, 4, 1. [Google Scholar]
- Manpreet, K.; Ajmal, M.B.; Raheel, S.A.; Saleem, M.C.; Mubeen, K.; Gaballah, K.; Kujan, O. Oral health status among transgender young adults: A cross-sectional study. BMC Oral Health. 2021, 21, 575. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).