

Assessment of the Status of Water, Sanitation and Hygiene (WASH) Services at Primary Schools in uMfolozi Local Municipality, Kwa-Zulu Natal, South Africa

 ,
, 
Abstract
1. Introduction
2. Methods and Materials
2.1. Contextualisation of Study Area
2.2. Study Design
2.3. Study Population and Sample Size
2.4. Data Collection
2.5. Data Processing and Analysis
2.6. Ethical Consideration
3. Results
3.1. Descriptive Analysis of Learners in Schools
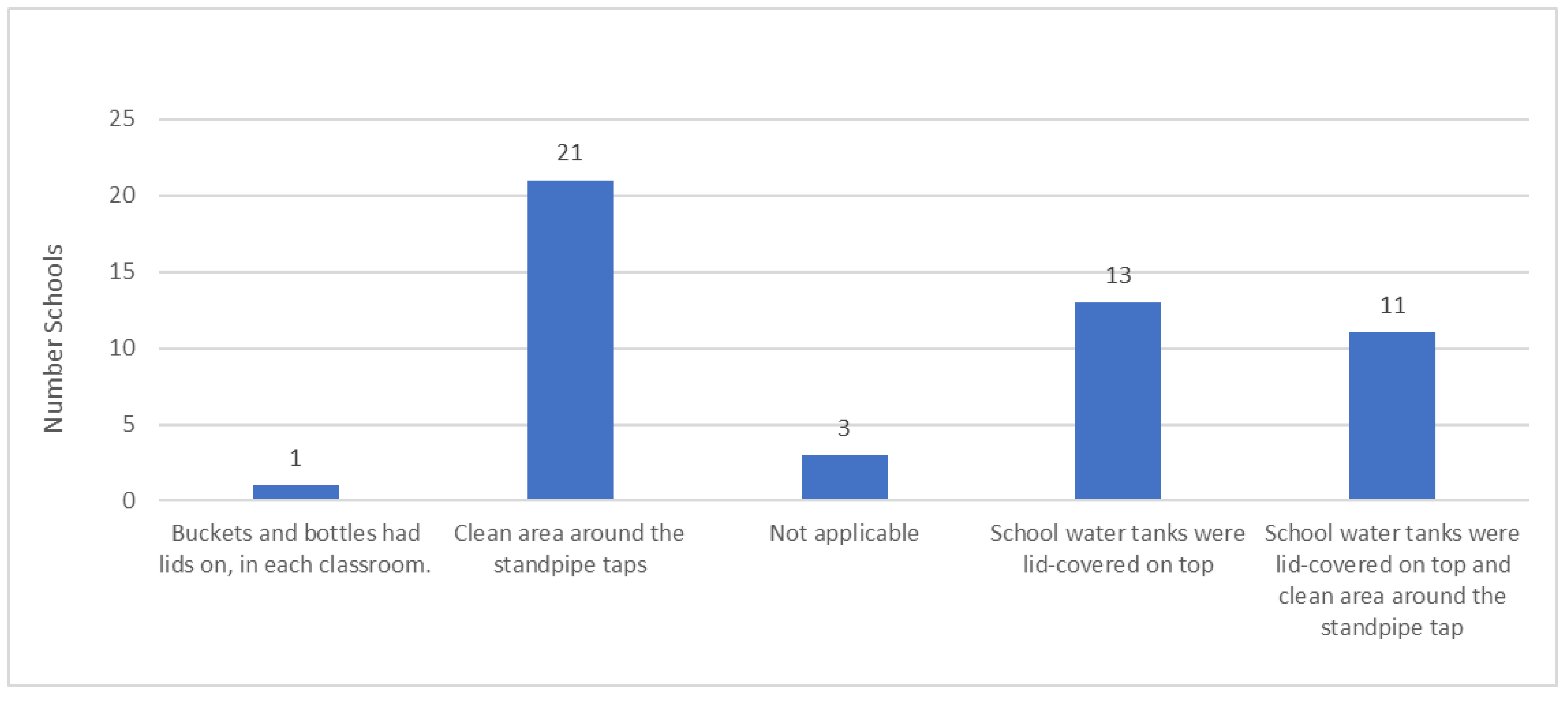
3.2. The Status of Water Availability and Reliability in Primary Schools
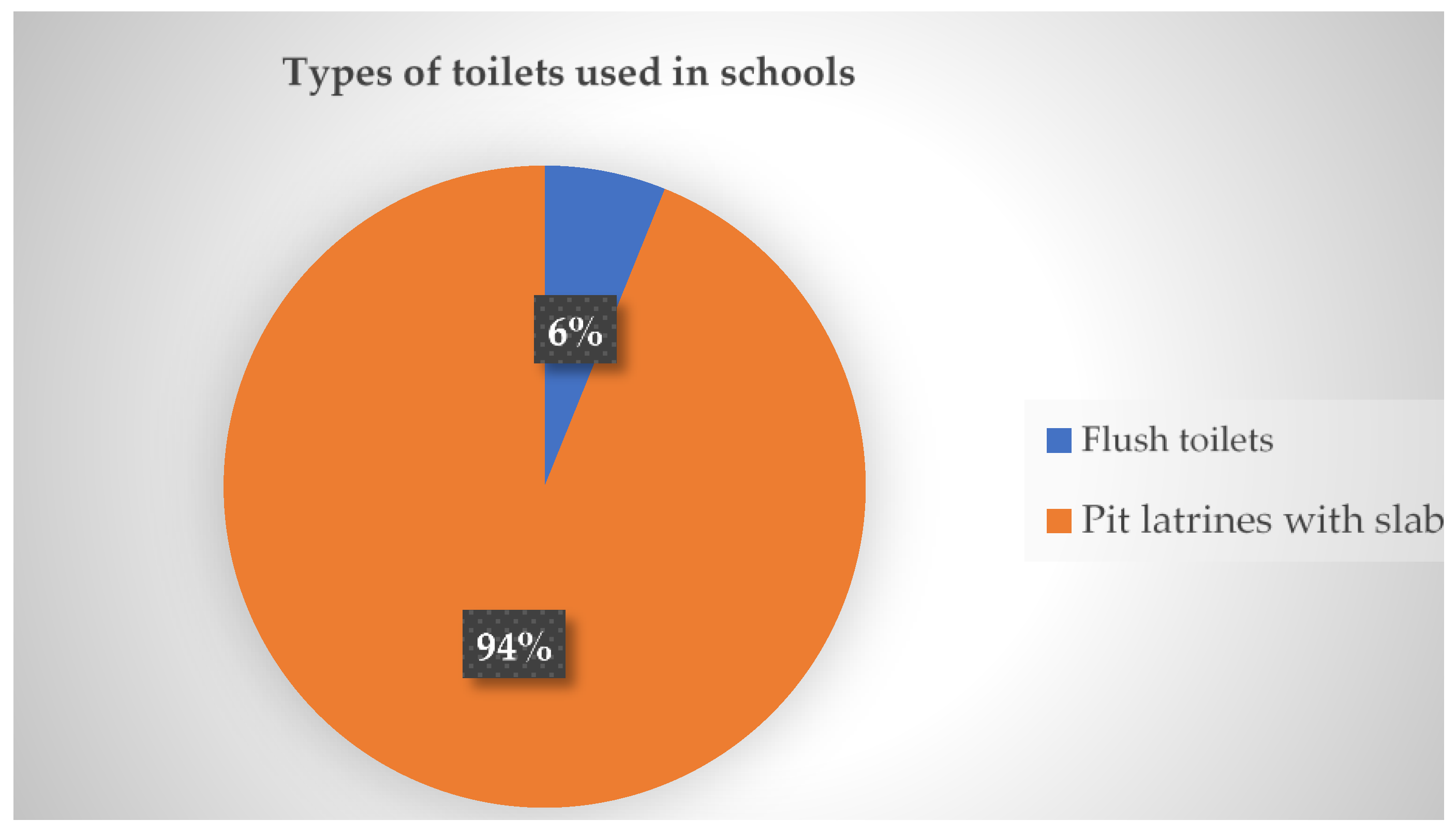
3.3. The Status of Sanitation Facilities in Schools
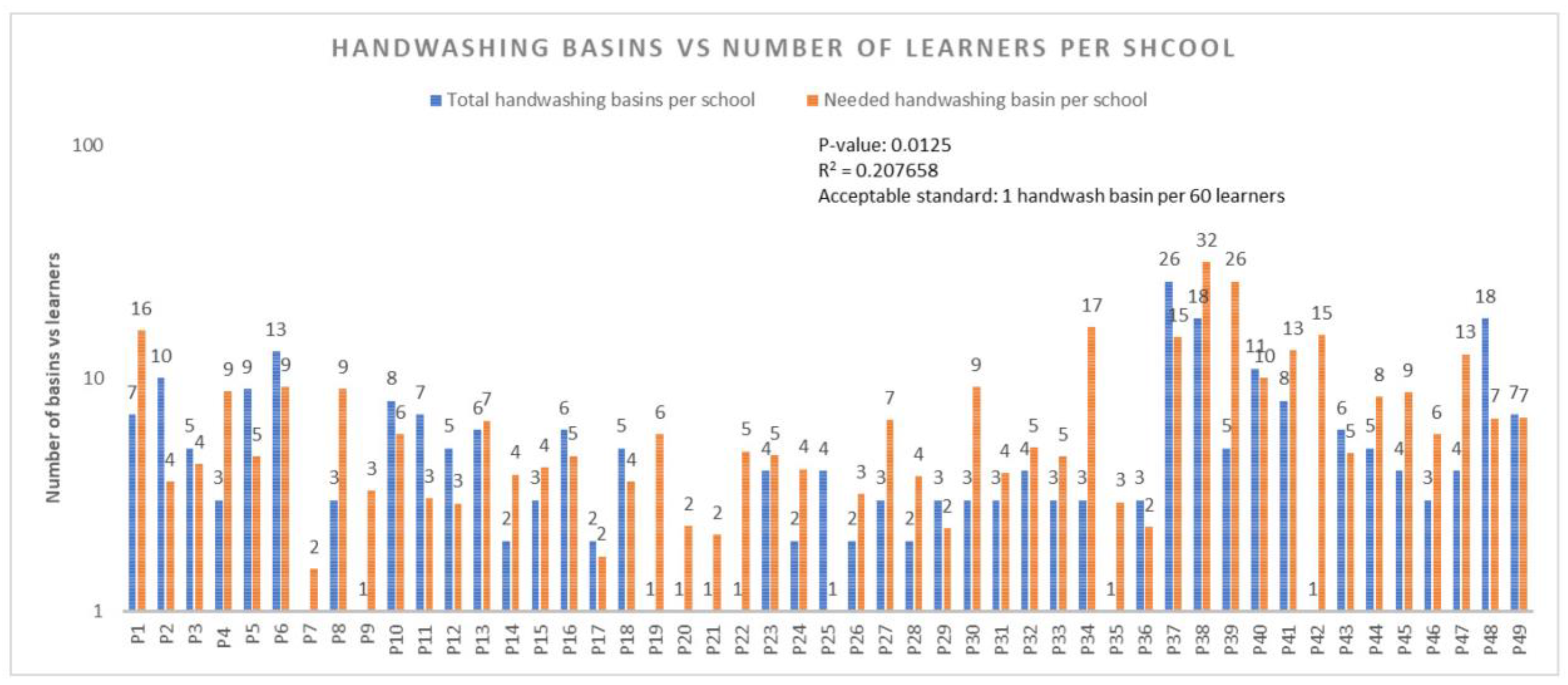
3.4. The Status of Hygiene in Schools
4. Discussion
4.1. Water
4.2. Sanitation
4.3. Hygiene
5. Conclusions
6. Recommendations
- Increase investment in WASH infrastructure: The government should increase investment in WASH infrastructure in uMfolozi primary schools. This includes providing schools with access to reliable sources of clean water, constructing adequate sanitation facilities, and installing hygiene facilities.
- Strengthen WASH management and capacity building: The government should strengthen WASH management and capacity building at the school level. This includes training school staff on WASH management and providing them with the resources they need to implement effective WASH programmes.
- Promote community participation in WASH: The government should promote community participation in WASH. This includes working with communities to identify WASH needs, develop WASH plans, and implement WASH programmes. A conference paper by [29] revealed that in the provinces of Bam and Sanmatenga in Burkina Faso, three community self-assessments are conducted each year; at the start, middle, and end of the academic year. In order to review indicators for each target and ascertain the degree of success and difficulties, the WASH committee conducts direct observations of the school’s water, sanitation, and hygiene facilities as well as monitoring visits that involve interactive interactions between the various actors of the school community.
7. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ngure, F.M.; Reid, B.M.; Humphrey, J.H.; Mbuya, M.N.; Pelto, G.; Stoltzfus, R.J. Water, sanitation, and hygiene (WASH), environmental enteropathy, nutrition, and early child development: Making the links. Ann. N. Y. Acad. Sci. 2014, 1308, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Kılıç, Z. The importance of water and conscious use of water. Int. J. Hydrol. 2020, 4, 239–241. [Google Scholar] [CrossRef]
- Lesa, M. The Status of Sanitation Facilities in Selected Public Schools in Kabushi Constituency of Ndola Urban; Mulungushi University: Kabwe, Zambia, 2018. [Google Scholar]
- Egbinola, C.N.; Amanambu, A.C. Water supply, sanitation and hygiene education in secondary schools in Ibadan, Nigeria. Bull. Geography. Socio-Econ. Ser. 2015, 29, 31–46. [Google Scholar] [CrossRef]
- Agol, D.; Harvey, P. Gender differences related to WASH in schools and educational efficiency. Water Altern. 2018, 11, 284–296. [Google Scholar]
- Pal, M.; Ayele, Y.; Hadush, M.; Panigrahi, S.; Jadhav, V.J. Public health hazards due to unsafe drinking water. Air Water Borne Dis. 2018, 7, 1000138. [Google Scholar]
- Shah, A.A.; Khan, M.A.; Kanwal, N.; Bernstein, R. Assessment of safety of drinking water in tank district: An empirical study of water-borne diseases in rural Khyber Pakhtunkhwa, Pakistan. Int. J. Environ. Sci. 2016, 6, 418–428. [Google Scholar]
- Zivi, K. Hiding in public or going with the flow: Human rights, human dignity, and the movement for menstrual equity. Hum. Rights Q. 2020, 42, 119–144. [Google Scholar] [CrossRef]
- Unicef. Strategy for Water, Sanitation and Hygiene 2016–2030. 2016. Available online: https://www.unicef.org/documents/unicef-strategy-water-sanitation-and-hygiene-2016-2030 (accessed on 16 January 2025).
- World Health Organization. Oral Health Promotion: An Essential Element of a Health-Promoting School; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- World Health Organization. Making Every School a Health-Promoting School: Country Case Studies; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Anthonj, C.; Githinji, S.; Höser, C.; Stein, A.; Blanford, J.; Grossi, V. Kenyan school book knowledge for water, sanitation, hygiene and health education interventions: Disconnect, integration or opportunities? Int. J. Hyg. Environ. Health 2021, 235, 113756. [Google Scholar] [CrossRef] [PubMed]
- Stats, S.A. Census, Department of Statistics Africa, Republic of South Africa. 2022. Available online: https://census.statssa.gov.za/assets/documents/2022/Provinces_at_a_Glance.pdf (accessed on 16 November 2024).
- Leavy, P. Research Design: Quantitative, Qualitative, Mixed Methods, Arts-Based, and Community-Based Participatory Research Approaches; Guilford Publications: New York, NY, USA, 2022. [Google Scholar]
- Cvetković Vega, A.; Maguiña, J.L.; Soto, A.; Lama-Valdivia, J.; Correa López, L.E. Cross-sectional studies. Rev. De La Fac. De Med. Humana 2021, 21, 22. [Google Scholar]
- Wang, X.; Cheng, Z. Cross-sectional studies: Strengths, weaknesses, and recommendations. Chest 2020, 158, S65–S71. [Google Scholar] [CrossRef] [PubMed]
- Fry, M.; Curtis, K.; Considine, J.; Shaban, R.Z. Using observation to collect data in emergency research. Australas. Emerg. Nurs. J. 2017, 20, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Smritirekha. Observation as a Tool for Collecting Data. Int. J. Multidiscip. Educ. Res. 2023, 8, 152–164. [Google Scholar]
- World Health Organization. Improving Health and Learning Through Better Water, Sanitation and Hygiene in Schools: An Information Package for School Staff; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Bhandari, P. How to Calculate Standard Deviation (Guide)|Calculator & Examples. 2024. Available online: https://www.scribbr.com/statistics/standard-deviation/ (accessed on 18 January 2025).
- Fisher, M.B.; Shields, K.F.; Chan, T.U.; Christenson, E.; Cronk, R.D.; Leker, H.; Samani, D.; Apoya, P.; Lutz, A.; Bartram, J. Understanding handpump sustainability: Determinants of rural water source functionality in the Greater Afram Plains region of Ghana. Water Resour. Res. 2015, 51, 8431–8449. [Google Scholar] [CrossRef] [PubMed]
- Bothma, T. School Sanitation Guidelines, Minute: 0010/2009; Western Cape Education Department: Cape Town, South Africa, 2009. [Google Scholar]
- UNICEF. School Readiness: A Conceptual Framework, Education Section, Programme Division, UNICEF/NYHQ2011-2486/Oivier Asselin; UNICEF: New York, NY, USA, 2012. [Google Scholar]
- Department of Water and Sanitation. National Norms and Standards for Domestic Water and Sanitation Services, Version 3-Final. 2017. Available online: https://www.gov.za/sites/default/files/gcis_document/201709/41100gon982.pdf (accessed on 18 November 2024).
- Odeku, O.K. Critical Analysis of School Pit Toilet System as an Impediment to the Right to Access Quality Education in South Africa. Afr. J. Public Aff. 2022, 13, 97–109. [Google Scholar]
- Chigunwe, G.; Tembachako, D. Public School Toilets: A Curse or Blessing for Girls with Physical Impairment. Afr. Educ. Res. J. 2017, 5, 200–206. [Google Scholar]
- Health Promotion Agency for Northern Ireland as Part of the School Food: Top Marks Programme, Water Provision. 2009. Available online: https://www.publichealth.hscni.net/sites/default/files/Water%20Provision%2009_10.pdf (accessed on 4 November 2024).
- Adams, J.; Bartram, J.; Chartier, Y.; Sims, J. Water, Sanitation and Hygiene Standards for schools in Low-Cost Settings; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Kere, C.; Nikiema, L.Z.; Boutin, M.; Debus, J.P. Increasing local participation in monitoring and learning to improve WASH services in schools. In Proceedings of the 39th WEDC International Conference, Kumasi, Ghana, 11–15 July 2016. [Google Scholar]
- UNICEF. Making Schools Accessible to Children with Disabilities. Retrieved from New Delhi. 2016. Available online: https://www.unicef.org/india/reports/making-schools-accessible-children-disabilities (accessed on 15 January 2025).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Count | Mean | Std Deviation | Min | Max | Con. Level 95% | |
|---|---|---|---|---|---|---|
| Number of learners | 49 | 424 | 216 | 60 | 1898 | 104 |
| Types of Drinking Water Sources | Frequency | % |
|---|---|---|
| Borehole | 15 | 23.1% |
| Rainwater | 25 | 38.5% |
| Schoolyard piped water | 25 | 38.5% |
| Total | 65 | 100% |
| Number of Drinking Water Points | Frequency | % |
|---|---|---|
| Borehole | 31 | 14% |
| Rainwater | 156 | 72% |
| Schoolyard piped water | 29 | 13% |
| Total | 216 | 100% |
| No. of Functional Drinking Water Points | N | % | No. of Non-Functional Drinking Water Points | N | % |
|---|---|---|---|---|---|
| Borehole water | 26 | 16 | Borehole water | 5 | 9 |
| Rainwater | 116 | 71 | Rainwater | 40 | 76 |
| Schoolyard piped water | 21 | 13 | Schoolyard piped water | 8 | 15 |
| Total | 163 | 100 | Total | 53 | 100 |
| N | % | |
|---|---|---|
| Functioning drinking water points | 163 | 76% |
| Non-functioning drinking water points | 53 | 24% |
| Total | 216 | 100% |
| Safety Aspect | N | % |
|---|---|---|
| Water tank covered with tight-fitting lid | 26 | 43% |
| Area around the standpipe tap | 32 | 53% |
| Water storage tank treated regularly with Jik | 2 | 3% |
| Total | 70 | 100% |
| Accessibility to Drinking Water Points | N (Yes) | Percentage (%) |
|---|---|---|
| Is at least one drinking water point accessible to the learners at the school? | 46 | 93% |
| What quality characteristics apply to the drinking water on the premises? Water has no colour, odour, taste and no turbidity | 49 | 100% |
| N (Yes and %) | N (No and %) | |
|---|---|---|
| Are there any posters promoting hygienic use of the toilets? | 2 (4.1%) | 47 (95.9) |
| Is running hot water provided at handwashing facilities? | 1 (2.0%) | 48 (98%) |
| Are handwashing facilities accessible to those with limited mobility? | 0 (0%) | 49 (100%) |
| Are handwashing facilities accessible to the learners in schools? | 45 (91.9%) | 4 (8.1) |
| Is any information about handwashing/hand hygiene visible at the school? | 2 (4.1%) | 47 (95.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radebe, L.C.; Mokgobu, M.I.; Molelekwa, G.F.; Mokoena, M.M. Assessment of the Status of Water, Sanitation and Hygiene (WASH) Services at Primary Schools in uMfolozi Local Municipality, Kwa-Zulu Natal, South Africa. Int. J. Environ. Res. Public Health 2025, 22, 360. https://doi.org/10.3390/ijerph22030360
Radebe LC, Mokgobu MI, Molelekwa GF, Mokoena MM. Assessment of the Status of Water, Sanitation and Hygiene (WASH) Services at Primary Schools in uMfolozi Local Municipality, Kwa-Zulu Natal, South Africa. International Journal of Environmental Research and Public Health. 2025; 22(3):360. https://doi.org/10.3390/ijerph22030360
Chicago/Turabian StyleRadebe, Lindokuhle C., Matlou I. Mokgobu, Gomotsegang F. Molelekwa, and Matodzi M. Mokoena. 2025. "Assessment of the Status of Water, Sanitation and Hygiene (WASH) Services at Primary Schools in uMfolozi Local Municipality, Kwa-Zulu Natal, South Africa" International Journal of Environmental Research and Public Health 22, no. 3: 360. https://doi.org/10.3390/ijerph22030360
APA StyleRadebe, L. C., Mokgobu, M. I., Molelekwa, G. F., & Mokoena, M. M. (2025). Assessment of the Status of Water, Sanitation and Hygiene (WASH) Services at Primary Schools in uMfolozi Local Municipality, Kwa-Zulu Natal, South Africa. International Journal of Environmental Research and Public Health, 22(3), 360. https://doi.org/10.3390/ijerph22030360