

West London Healthy Home and Environment (WellHome) Study: Protocol for a Community-Based Study Investigating Exposures Across the Indoor-Outdoor Air Pollution Continuum in Urban Communities

 , , , , , , , , , ,
, , , , , , , , , ,  , , add
Show full author list
, , add
Show full author list
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Background and Rationale
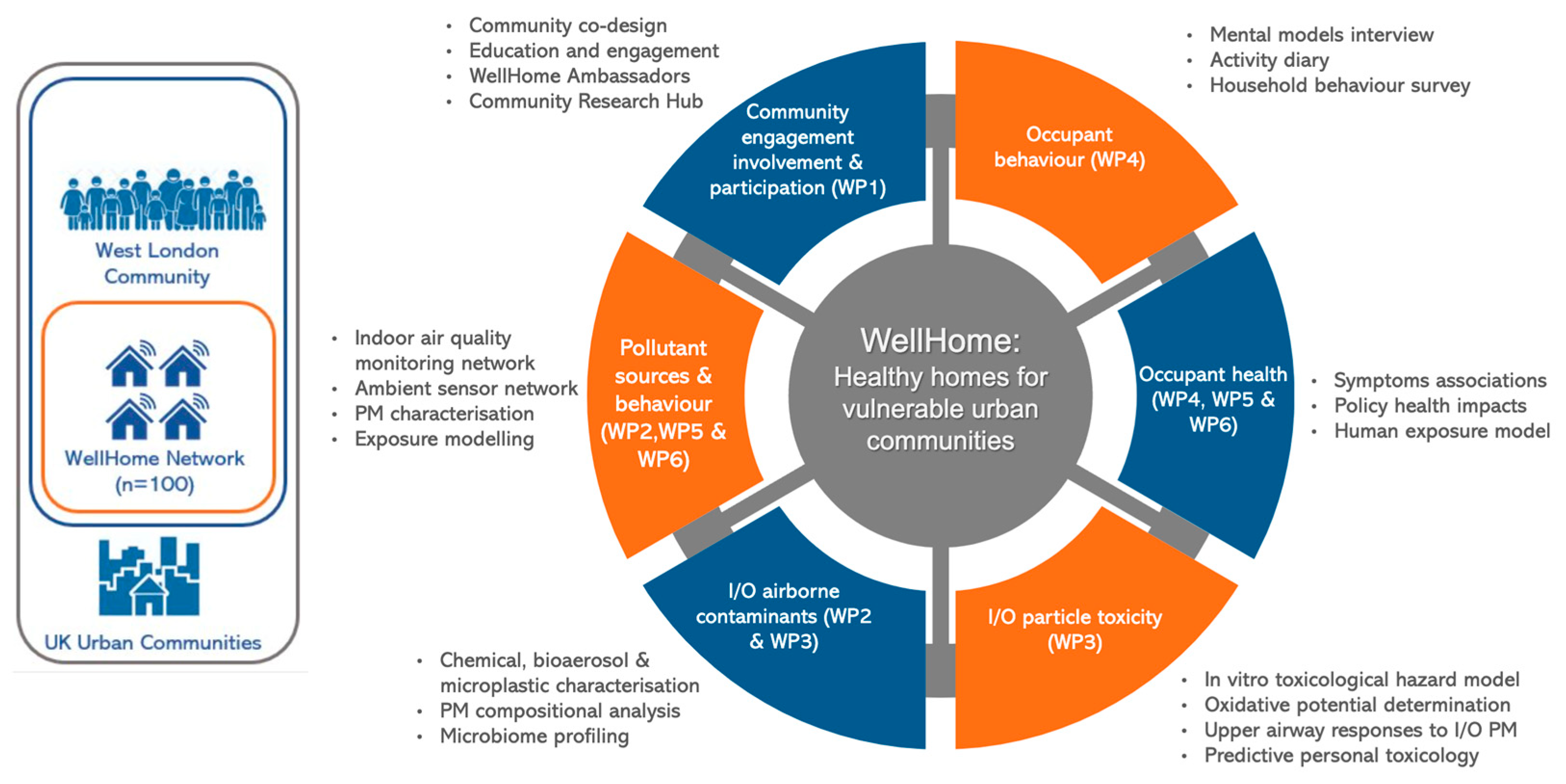
1.2. A Community-Driven Approach to Indoor Air Pollution Research
- At least one child in the household must have a diagnosis of asthma by a health practitioner.
- Participants should expect to reside at the same address for a minimum of 12 months.
- There must be no smokers in the household.
- Similar to the 100 homes group, participants must reside in West London.
1.3. Study Aim and Objectives
- to identify and explore contrasts in exposure to chemical and biological contaminants within heterogeneous households, considering indoor and outdoor measurements, household characteristics, area level deprivation, seasonality, proximity to traffic sources, and children’s time-activity to estimate personal exposures.
- to understand the potential of these exposures to affect the health of children with asthma and allergies in these households through epidemiological evaluation of symptoms and toxicological assessment of the relative hazard of chemical and biological aerosols.
- to develop behavioural and policy recommendations aimed at reducing the potential health burdens arising from indoor and ingressed outdoor air pollutants.
2. Materials and Methods
2.1. Study Setting and Participants Recruitment
- Households must reside in the area surrounding the Imperial College White City Campus in West London.
- Participants must be over 18 years old and be able to provide informed written consent.
- Participant must be the primary householder.
- We will prioritise the participation of households with children aged 5 to 17 years who have asthma and allergies, with a particular focus on families from minority ethnic backgrounds. This approach aims to ensure a diverse participant group that reflects the community’s diversity.
- Participating children who have asthma or allergies must reside in the participating household.
2.2. Participant Safety and Anonymity
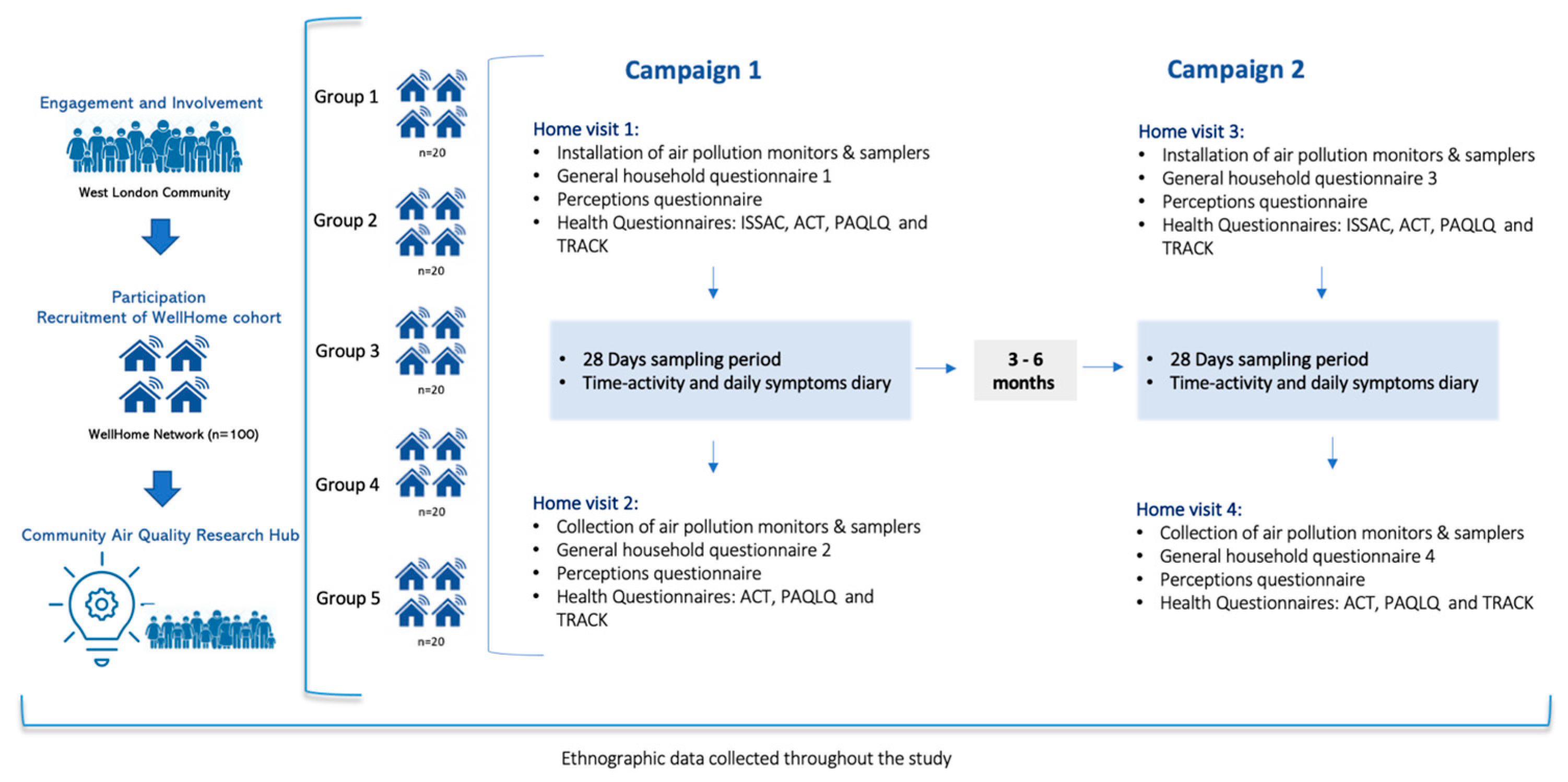
2.3. Study Design
2.4. Engagement and Educational Activities (WP1)
- Face-to-face and online educational sessions for children.
- Workshops with children to learn about the nature of the data we are collecting and how these data will be analysed and interpreted, providing an opportunity for children to actively engage in scientific investigations, improving mathematical literacy, and nurturing their curiosity in science.
- Interactive panel discussions during which residents will have opportunities to meet with WellHome researchers to ask questions about the study.
- Ad-hoc workshops with participating families aimed at actively gathering their input into the development of the study’s public-facing reports.
- An online community air quality research hub, incorporating live data feeds, advice, participant profiles, and notifications.
2.5. Household Exposure Sampling (WP2)
2.5.1. Air Pollution Monitoring Network
2.5.2. Passive Sampling Network
2.5.3. Questionnaires
2.6. Quantitative Profiling of Social Health Inequalities and Policy Disconnects Using Toxicological Paradigms (WP3)
2.7. Occupant Understanding and Behavioural Factors in Indoor Air Quality (WP4)
2.8. Characterising Sources and Behaviour That Reduce Exposure in the West London Community (WP5)
2.9. Harmonising the Data and Statistical Analysis of Relationships Between Sources Behaviours and Symptoms (WP6)
3. Discussion
Dissemination
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| WCET | White City Engagement Team |
| WP | Work Package |
| PIS | Participant Information Sheet |
| ICREC | Imperial College Research Ethics Committee |
| STEM | Science, Technology, Engineering, and Mathematics |
| PM2.5 | Particulate Matter that are 2.5 microns or less in diameter |
| NO2 | Nitrogen dioxide |
| HCHO | Formaldehyde |
| VOCs | Volatile Organic Compounds |
| tVOCs | total Volatile Organic Compounds |
| CO2 | Carbon dioxide |
| rDNA | ribosomal DNA |
| PCR | Polymerase Chain Reaction |
| BSL | British Sign Language |
| ISSAC | International Study of Asthma and Allergies in Childhood |
| ACT | The Asthma Control Test |
| PAQLQ | The Paediatric Asthma Quality of Life Questionnaire |
| TRACK | The Test for Respiratory and Asthma Control |
| CMAQ | Community Multiscale Air Quality |
| HIA | Health Impact Assessment |
| DAGs | Directed Acyclic Graphs |
References
- Ferguson, L.; Taylor, J.; Davies, M.; Shrubsole, C.; Symonds, P.; Dimitroulopoulou, S. Exposure to indoor air pollution across socio-economic groups in high-income countries: A scoping review of the literature and a modelling methodology. Environ. Int. 2020, 143, 105748. [Google Scholar] [CrossRef] [PubMed]
- Maung, T.Z.; Bishop, J.E.; Holt, E.; Turner, A.M.; Pfrang, C. Indoor Air Pollution and the Health of Vulnerable Groups: A Systematic Review Focused on Particulate Matter (PM), Volatile Organic Compounds (VOCs) and Their Effects on Children and People with Pre-Existing Lung Disease. Int. J. Environ. Res. Public Health 2022, 19, 8752. [Google Scholar] [CrossRef] [PubMed]
- Tiotiu, A.I.; Novakova, P.; Nedeva, D.; Chong-Neto, H.J.; Novakova, S.; Steiropoulos, P.; Kowal, K. Impact of Air Pollution on Asthma Outcomes. Int. J. Environ. Res. Public Health 2020, 17, 6212. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, P.E.; Mudway, I.S.; Grigg, J. Air Pollution and Asthma: Mechanisms of Harm and Considerations for Clinical Interventions. Chest 2021, 159, 1346–1355. [Google Scholar] [CrossRef]
- Maestre-Batlle, D.; Nygaard, U.C.; Huff, R.D.; Alexis, N.E.; Tebbutt, S.J.; Turvey, S.E.; Carlsten, C.; Bølling, A.K. Dibutyl phthalate exposure alters T-cell subsets in blood from allergen-sensitized volunteers. Indoor Air 2022, 32, e13026. [Google Scholar] [CrossRef]
- Carlsten, C. Synergistic Environmental Exposures and the Airways Capturing Complexity in Humans: An Underappreciated World of Complex Exposures. Chest 2018, 154, 918–924. [Google Scholar] [CrossRef]
- Maestre-Batlle, D.; Huff, R.D.; Schwartz, C.; Alexis, N.E.; Tebbutt, S.J.; Turvey, S.; Bølling, A.K.; Carlsten, C. Dibutyl Phthalate Augments Allergen-induced Lung Function Decline and Alters Human Airway Immunology. A Randomized Crossover Study. Am. J. Respir. Crit. Care Med. 2020, 202, 672–680. [Google Scholar] [CrossRef]
- Holgate, S. Every Breath We Take: The Lifelong Impact of Air Pollution; Report of a working party; Royal College of Physicians: London, UK, 2016. [Google Scholar]
- Whitty, C. Chief Medical Officer’s Annual Report 2022, Air Pollution; UK Government: London, UK. Available online: https://www.gov.uk/government/publications/chief-medical-officers-annual-report-2022-air-pollution (accessed on 10 December 2022).
- Ferguson, L.; Taylor, J.; Zhou, K.; Shrubsole, C.; Symonds, P.; Davies, M.; Dimitroulopoulou, S. Systemic inequalities in indoor air pollution exposure in London, UK. Build. Cities 2021, 2, 425–448. [Google Scholar] [CrossRef]
- Thurston, G.D.; Kipen, H.; Annesi-Maesano, I.; Balmes, J.; Brook, R.D.; Cromar, K.; De Matteis, S.; Forastiere, F.; Forsberg, B.; Frampton, M.W.; et al. A joint ERS/ATS policy statement: What constitutes an adverse health effect of air pollution? An analytical framework. Eur. Respir. J. 2017, 49, 1600419. [Google Scholar] [CrossRef]
- Barratt, B. My House, My Rules: Co-Designing Residential Air Pollution Research; BBSRC BB/T018895/12020; BBSRC: Swindon, UK, 2023.
- Nova. Available online: https://novanew.org.uk/ (accessed on 1 February 2021).
- Bubble & Squeak. Available online: https://www.bubblesqueakeat.com/ (accessed on 1 February 2021).
- Indoor Air Quality Working Party. Resources for School Children. Available online: https://theinsidestory.health/worksheets/ (accessed on 1 October 2021).
- Imperial. The Invention Room. Available online: https://www.imperial.ac.uk/white-city-campus/community/the-invention-rooms/ (accessed on 1 February 2021).
- ISO 16000-6:2021; Part 6: Determination of Organic Compounds (VVOC, VOC, SVOC) in Indoor and Test Chamber Air by Active Sampling on Sorbent Tubes, Thermal Desorption and Gas Chromatography Using MS or MS FID. International Organization for Standardization: Geneva, Switzerland, 2021.
- BS 40102-1:2023; Health, Well-Being and Indoor Environmental Quality in Buildings—Part 1: Code of Practice for Indoor Environmental Quality in Occupied Non-Domestic Buildings. British Standards Institution: London, UK, 2023.
- Environmental Research Group at Imperial College. Breathe London, the Community Sensing Network. Available online: https://www.breathelondon.org/ (accessed on 1 October 2021).
- Richardson, A.K.; Irlam, R.C.; Wright, H.R.; Mills, G.A.; Fones, G.R.; Stürzenbaum, S.R.; Cowan, D.A.; Neep, D.J.; Barron, L.P. A miniaturized passive sampling-based workflow for monitoring chemicals of emerging concern in water. Sci. Total Environ. 2022, 839, 156260. [Google Scholar] [CrossRef]
- McEneff, G.L.; Murphy, B.; Webb, T.; Wood, D.; Irlam, R.; Mills, J.; Green, D.; Barron, L.P. Sorbent Film-Coated Passive Samplers for Explosives Vapour Detection Part A: Materials Optimisation and Integration with Analytical Technologies. Sci. Rep. 2018, 8, 5815. [Google Scholar] [CrossRef] [PubMed]
- Shelton, J.M.; Rhodes, J.; Uzzell, C.B.; Hemmings, S.; Brackin, A.P.; Sewell, T.R.; Alghamdi, A.; Dyer, P.S.; Fraser, M.; Borman, A.M.; et al. Citizen science reveals landscape-scale exposures to multiazole-resistant Aspergillus fumigatus bioaerosols. Sci. Adv. 2023, 9, eadh8839. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.I.; Tian, Y.; Taylor, J.W.; Bruns, T.D.; Hyvärinen, A.; Täubel, M. Passive dust collectors for assessing airborne microbial material. Microbiome 2015, 3, 46. [Google Scholar] [CrossRef]
- Wright, S.L.; Gouin, T.; Koelmans, A.A.; Scheuermann, L. Development of screening criteria for microplastic particles in air and atmospheric deposition: Critical review and applicability towards assessing human exposure. Microplastics Nanoplastics 2021, 1, 6. [Google Scholar] [CrossRef]
- Jones, N.; Wendt, J.; Wright, S.; Hartner, E.; Groeger, T. Analysis of Microplastics in Environmental Samples by Pyrolysis/Thermal Desorption-(GC)xGC-TOFMS. Chromatogr. Today 2021, 14, 36–40. [Google Scholar]
- Liu, B.Y.H.; Berglund, R.N.; Agarwal, J.K. Experimental studies of optical particle counters. Atmos. Environ. (1967) 1974, 8, 717–732. [Google Scholar] [CrossRef]
- Jian, C.; Luukkonen, P.; Yki-Järvinen, H.; Salonen, A.; Korpela, K. Quantitative PCR provides a simple and accessible method for quantitative microbiota profiling. PLoS ONE 2020, 15, e0227285. [Google Scholar] [CrossRef]
- Asher, M.; Keil, U.; Anderson, H.; Beasley, R.; Crane, J.; Martinez, F.; Mitchell, E.; Pearce, N.; Sibbald, B.; Stewart, A.; et al. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and methods. Eur. Respir. J. 1995, 8, 483–491. [Google Scholar] [CrossRef]
- GlaxoSmithKline. Asthma Control Test. Available online: https://www.asthmacontroltest.com/en-gb/welcome/ (accessed on 1 February 2022).
- Juniper, E.F. Measurement of Health-Related Quality of Life & Asthma Control. Available online: https://www.qoltech.co.uk/paqlq.html (accessed on 1 February 2022).
- Murphy, K.R.; Zeiger, R.S.; Kosinski, M.; Chipps, B.; Mellon, M.; Schatz, M.; Lampl, K.; Hanlon, J.T.; Ramachandran, S. Test for Respiratory and Asthma Control in Kids (TRACK): A caregiver-completed questionnaire for preschool-aged children. J. Allergy Clin. Immunol. 2009, 123, 833–839.e9. [Google Scholar] [CrossRef]
- Samoli, E.; Dimakopoulou, K.; Evangelopoulos, D.; Rodopoulou, S.; Karakatsani, A.; Veneti, L.; Sionidou, M.; Tsolakoglou, I.; Krasanaki, I.; Grivas, G.; et al. Is daily exposure to ozone associated with respiratory morbidity and lung function in a representative sample of schoolchildren? Results from a panel study in Greece. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 346–351. [Google Scholar] [CrossRef]
- Atkinson, P. Handbook of Ethnography; Sage: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- Rosenstock, I.M. Health Belief Model. In Encyclopedia of Psychology; American Psychological Association: Washington, DC, USA, 2000; Volume 4, pp. 78–80. [Google Scholar]
- Vu, T.V.; Stewart, G.B.; Kitwiroon, N.; Lim, S.; Barratt, B.; Kelly, F.J.; Thompson, R.; Smith, R.B.; Toledano, M.B.; Beevers, S.D. Assessing the contributions of outdoor and indoor sources to air quality in London homes of the SCAMP cohort. Build. Environ. 2022, 222, 109359. [Google Scholar] [CrossRef]
- Dols, W.S.; Milando, C.W.; Ng, L.; Emmerich, S.J.; Teo, J. On the Benefits of Whole-building IAQ, Ventilation, Infiltration, and Energy Analysis Using Co-simulation between CONTAM and EnergyPlus. In Proceedings of the IBPC 2021, Copenhagen, Denmark, 25–27 August 2021. [Google Scholar]
- Beevers, S.; Assareh, N.; Beddows, A.; Stewart, G.; Holland, M.; Fecht, D.; Liu, Y.; Goodman, A.; Walton, H.; Brand, C.; et al. Climate change policies reduce air pollution and increase physical activity: Benefits, costs, inequalities, and indoor exposures. Environ. Int. 2024, 195, 109164. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Effects of Transport-Related Air Pollution; Krzyzanowski, M., Kuna-Dibbert, B., Schneider, J., Eds.; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2005. [Google Scholar]
- Forastiere, F.; Spadaro, J.V.; Ancona, C.; Andersen, Z.J.; Cozzi, I.; Gumy, S.; Loncar, D.; Mudu, P.; Medina, S.; Velasco, R.P.; et al. Choices of morbidity outcomes and concentration–response functions for health risk assessment of long-term exposure to air pollution. Environ. Epidemiol. 2024, 8, e314. [Google Scholar] [CrossRef]
- Evangelopoulos, D.; Katsouyanni, K.; Keogh, R.H.; Samoli, E.; Schwartz, J.; Barratt, B.; Zhang, H.; Walton, H. PM2.5 and NO2 exposure errors using proxy measures, including derived personal exposure from outdoor sources: A systematic review and meta-analysis. Environ. Int. 2020, 137, 105500. [Google Scholar] [CrossRef]
- Hasselblad, V.; Eddy, D.M.; Kotchmar, D.J. Synthesis of environmental evidence: Nitrogen dioxide epidemiology studies. J. Air Waste Manag. Assoc. 1992, 42, 662–671. [Google Scholar] [CrossRef]
- World Health Organisation. WHO Guidelines for Indoor Air Quality: Selected Pollutants; WHO: Geneva, Switzerland, 2010; p. 454. [Google Scholar]
- Walton, H.; Dajnak, D.; Holland, M.; Evangelopoulos, D.; Wood, D.; Brand, C.; Assareh, N.; Stewart, G.; Beddows, A.; Lee, S.Y.; et al. Health and associated economic benefits of reduced air pollution and increased physical activity from climate change policies in the UK. Environ. Int. 2025. submitted. [Google Scholar] [CrossRef]
- Dajnak, D.; Kitwiroon, N.; Assareh, N.; Stewart, G.; Evangelopoulos, D.; Wood, D.; Walton, H.; Beevers, S. Pathway to WHO: Achieving Clean Air in the UK; Modelling Air Quality Costs and Benefits; Environmental Research Group—Imperial College London: London, UK, 2022. [Google Scholar]
- World Health Organization, Regional Office for Europe. Health Risks of Air Pollution in Europe—HRAPIE Project: Recommendations for Concentration–Response Functions for Cost–Benefit Analysis of Particulate Matter, Ozone and Nitrogen Dioxide. 2013. Available online: https://iris.who.int/handle/10665/153692 (accessed on 10 February 2022).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varaden, D.; Barratt, B.; Dallman, M.J.; Skillern, A.; Elmi, M.S.; Green, D.C.; Tremper, A.H.; Hedges, M.; Hicks, W.; Priestman, M.; et al. West London Healthy Home and Environment (WellHome) Study: Protocol for a Community-Based Study Investigating Exposures Across the Indoor-Outdoor Air Pollution Continuum in Urban Communities. Int. J. Environ. Res. Public Health 2025, 22, 249. https://doi.org/10.3390/ijerph22020249
Varaden D, Barratt B, Dallman MJ, Skillern A, Elmi MS, Green DC, Tremper AH, Hedges M, Hicks W, Priestman M, et al. West London Healthy Home and Environment (WellHome) Study: Protocol for a Community-Based Study Investigating Exposures Across the Indoor-Outdoor Air Pollution Continuum in Urban Communities. International Journal of Environmental Research and Public Health. 2025; 22(2):249. https://doi.org/10.3390/ijerph22020249
Chicago/Turabian StyleVaraden, Diana, Benjamin Barratt, Margaret J. Dallman, Adam Skillern, Munira S. Elmi, David C. Green, Anja H. Tremper, Michael Hedges, William Hicks, Max Priestman, and et al. 2025. "West London Healthy Home and Environment (WellHome) Study: Protocol for a Community-Based Study Investigating Exposures Across the Indoor-Outdoor Air Pollution Continuum in Urban Communities" International Journal of Environmental Research and Public Health 22, no. 2: 249. https://doi.org/10.3390/ijerph22020249
APA StyleVaraden, D., Barratt, B., Dallman, M. J., Skillern, A., Elmi, M. S., Green, D. C., Tremper, A. H., Hedges, M., Hicks, W., Priestman, M., Barron, L. P., Fitzgerald, S. P., Walder, H. M., Wright, S. L., Mudway, I. S., Fisher, M. C., Hemmings, S. J., Poortinga, W., Tirotto, F., ... Kelly, F. J. (2025). West London Healthy Home and Environment (WellHome) Study: Protocol for a Community-Based Study Investigating Exposures Across the Indoor-Outdoor Air Pollution Continuum in Urban Communities. International Journal of Environmental Research and Public Health, 22(2), 249. https://doi.org/10.3390/ijerph22020249