

Where Do Professional Sports Clubs and Organisations Sit Within a Local Health Promotion System? A Social Network Analysis Study


Abstract
:1. Introduction
Context
- (i)
- Who identifies PSCOs as a key partner in the delivery of HP projects?
- (ii)
- With whom do PSCOs share information, knowledge, and resources?
- (iii)
- What is the perceived importance of PSCOs to the system from other organisations in it?
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Data Analysis
2.4. Ethics
3. Results
3.1. Descriptive Statistics
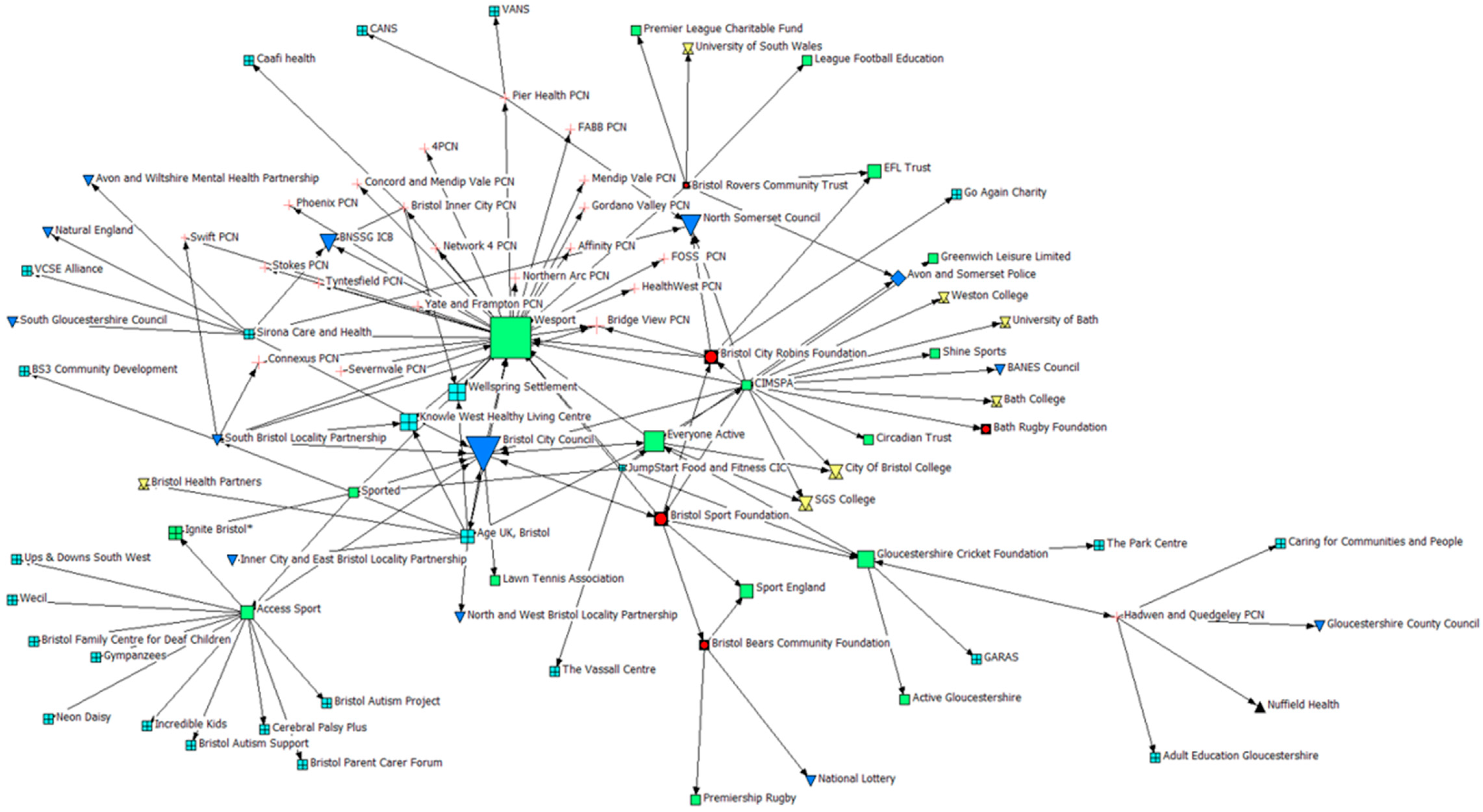
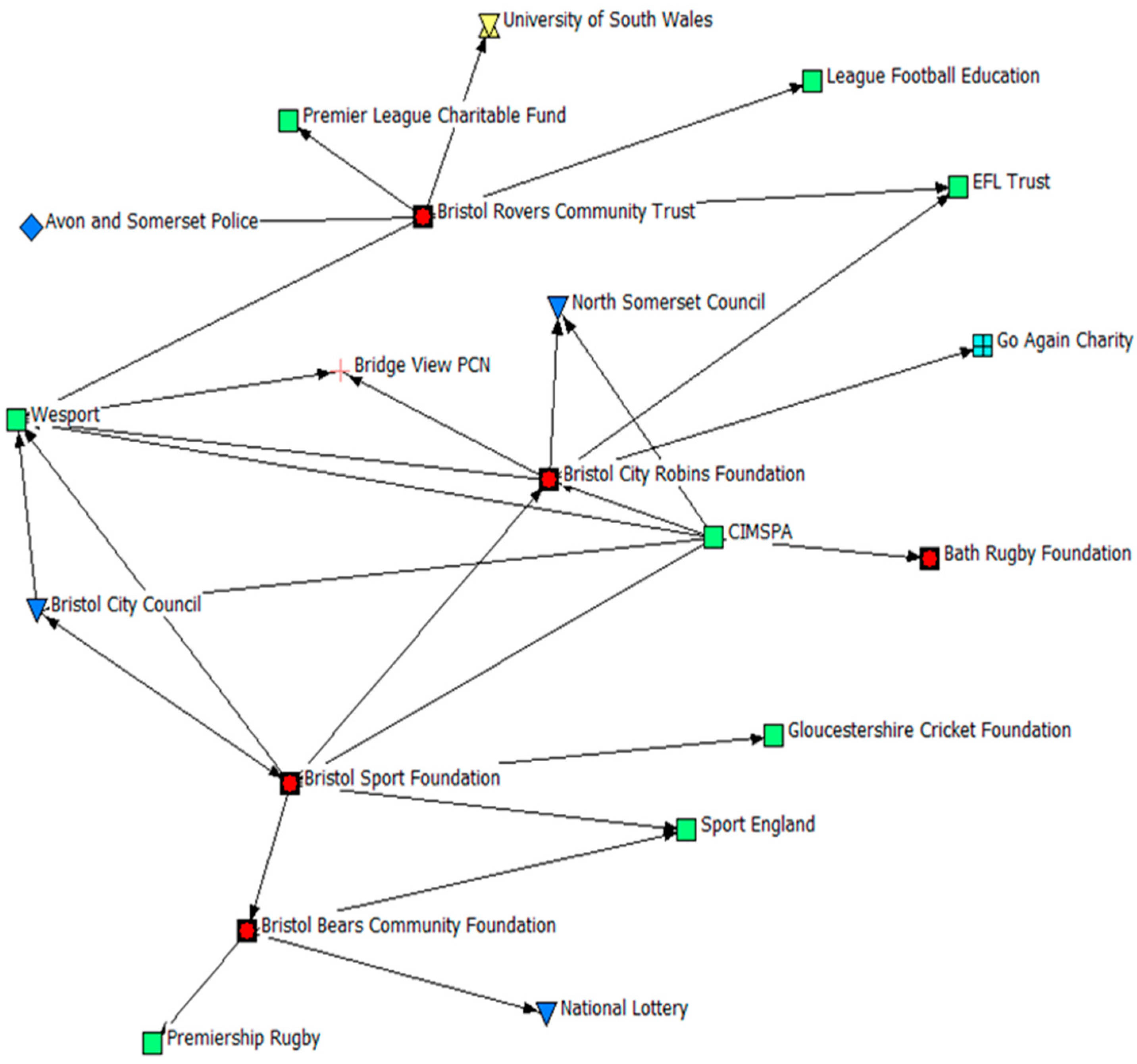
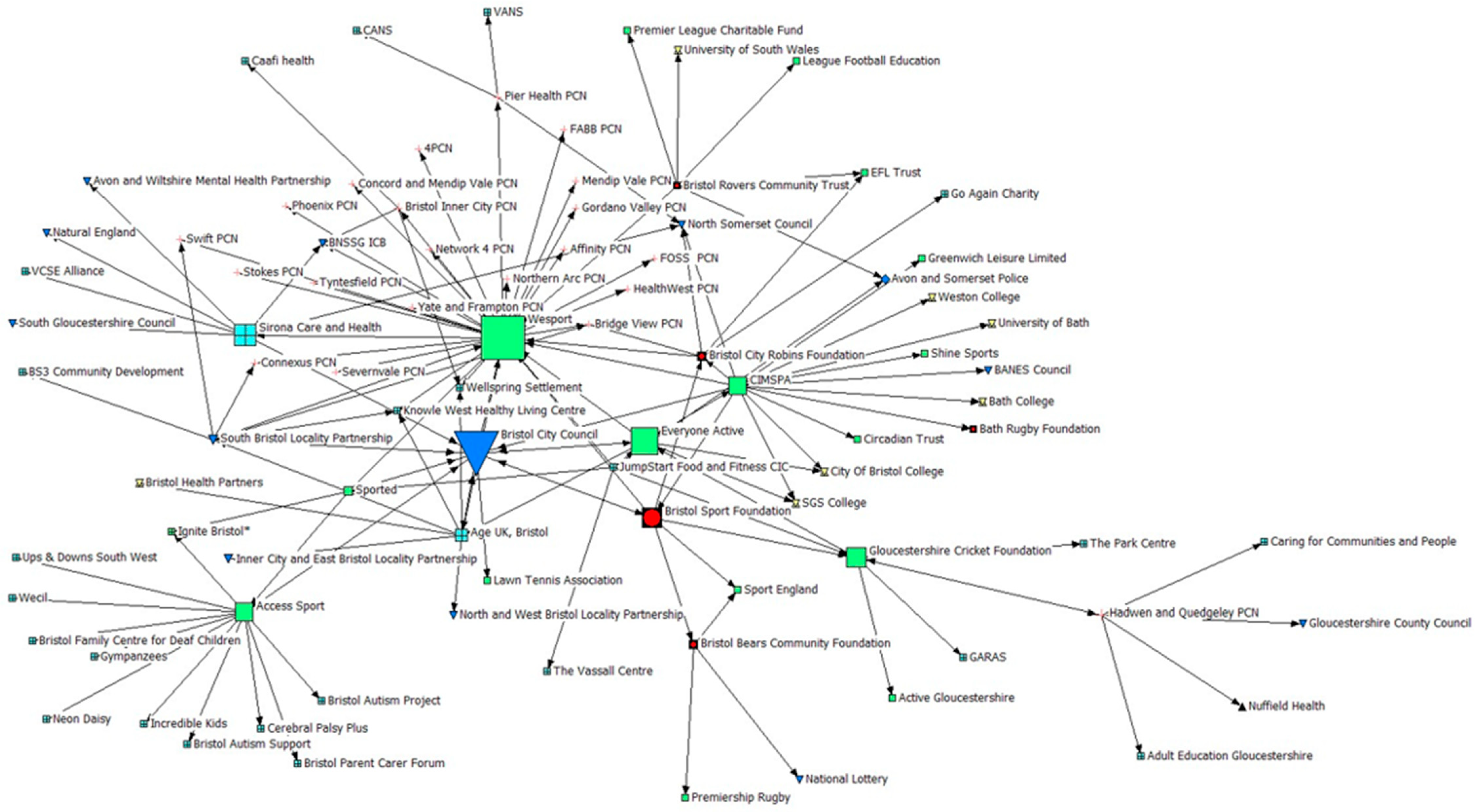
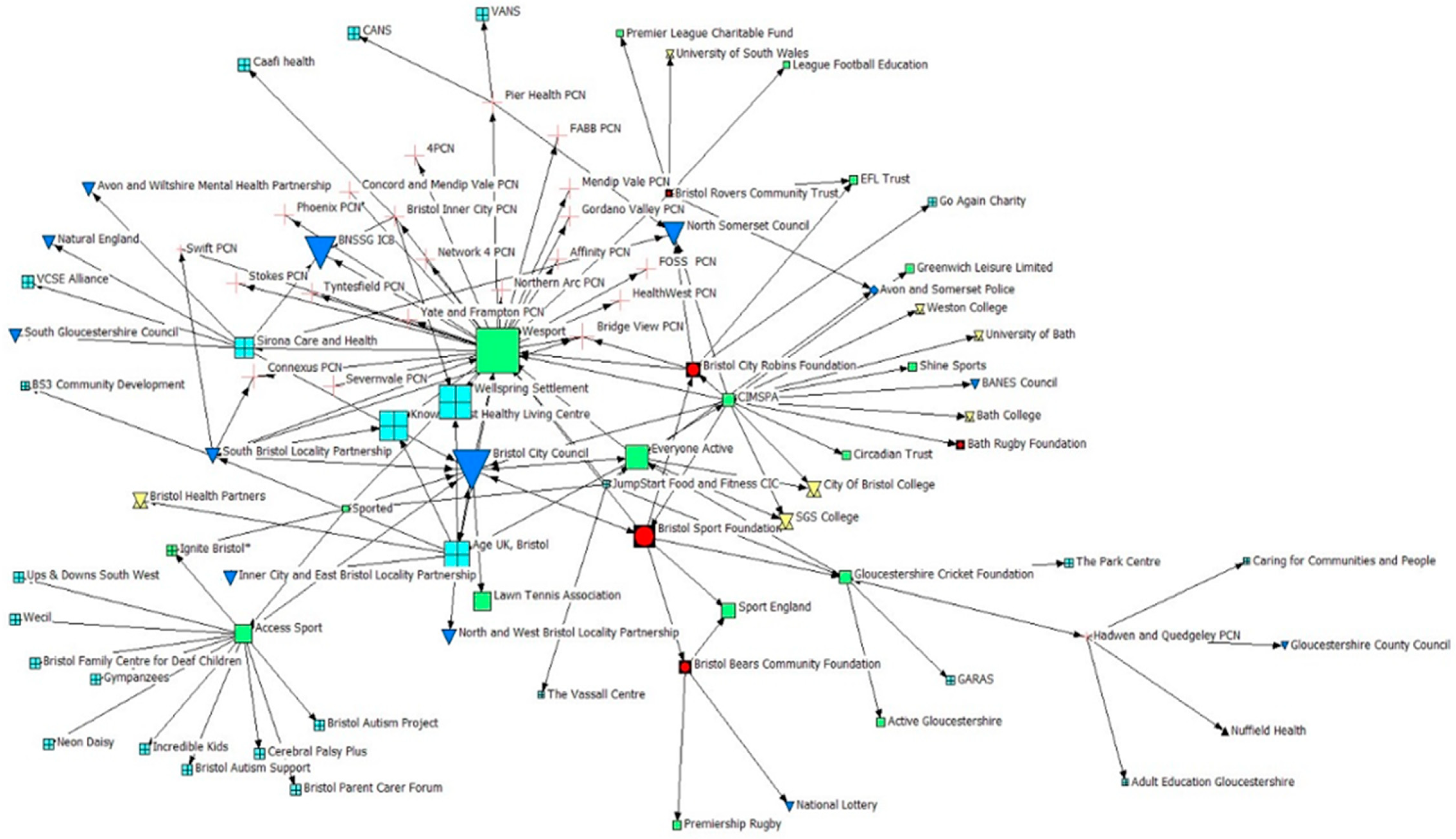
3.2. Indegree Centrality: Who Identifies PSCOs as a Key Partner in the Delivery of HP Projects?
3.3. Betweenness Centrality: With Whom Do PSCOs Share Information, Knowledge, and Resources?
3.4. Ineigenvector Centrality: What Is the Perceived Importance of PSCOs to the System from Other Organisations in It?
3.5. Geodesic Distance
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PSCO | Professional Sports Club and Organisations |
| HP | Health Promotion |
| PA | Physical Activity |
| EFL | English Football League |
| U.K. | United Kingdom |
| BNSSG | Bristol, North Somerset, and South Gloucestershire |
| SNA | Social Network Analysis |
| VCFSE | Voluntary, Community, Faith and Social Enterprise |
| PCN | Primary Care Network |
References
- Bostock, J. Mission vs. Market: Theorizing the tensions within community sport trusts. Int. J. Sport Soc. 2021, 13, 1–22. [Google Scholar] [CrossRef]
- François, A.; Bayle, E.; Gond, J.P. A multilevel analysis of implicit and explicit CSR in French and UK professional sport. Eur. Sport Manag. Q. 2019, 19, 15–37. [Google Scholar] [CrossRef]
- Lozano-Sufrategui, L.; Pringle, A.; Zwolinsky, S.; Drew, K.J. Professional football clubs’ involvement in health promotion in Spain: An audit of current practices. Health Promot. Int. 2020, 35, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Røynesdal, Ø.; Van Nassau, F.; Chng, N.; Pereira, H.; Andersen, E.; Bunn, C.; Jelsma, J.; Nijhuis-Van Der Sanden, M.; Roberts, G.; Sørensen, M.; et al. Exploring the provision and motives behind the adoption of health-promotion programmes in professional football clubs across four European countries. PLoS ONE 2021, 16, e0259458. [Google Scholar] [CrossRef] [PubMed]
- Pringle, A.; Zwolinsky, S.; Lozano-Sufrategui, L. Investigating the delivery of health improvement interventions through professional football club community trusts-strengths and challenges. Public Health Pract. 2021, 2, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Brazier, J.; Foster, C.; Townsend, N.; Murphy, J.; Northcote, M.; Smith, A. Mapping the provision and evaluation practices of local community health and wellbeing programmes delivered by professional sports clubs in England: A practice-based targeted review. Int. J. Sport Policy Politics 2023, 16, 39–58. [Google Scholar] [CrossRef]
- Brown, K. Association between alcohol sports sponsorship and consumption: A systematic review. Alcohol Alcohol. 2016, 51, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Purves, R.I.; Critchlow, N.; Morgan, A.; Stead, M.; Dobbie, F. Examining the frequency and nature of gambling marketing in televised broadcasts of professional sporting events in the United Kingdom. Public Health 2020, 184, 71–78. [Google Scholar] [CrossRef]
- Sanders, A.; Keech, M.; Burdsey, D.; Maras, P.; Moon, A. CEO perspectives on the first twenty-five years of football in the community: Challenges, developments and opportunities. Manag. Sport Leis. 2021, 26, 7–21. [Google Scholar] [CrossRef]
- Watson, N. Football in the community: What’s the Score? Soccer Soc. 2000, 1, 114–125. [Google Scholar] [CrossRef]
- EFL in the Community (2022) Measuring the Impact of EFL Clubs in the Community. Available online: https://eflinthecommunity.com/3d-flip-book/22126/?_gl=1*5z246v*_ga*NTc5MDA3NjIzLjE3MTE0NDc5Mjc.*_ga_SWZ2NEX865*MTczOTAxNzE3NS4zLjAuMTczOTAxNzE3NS42MC4wLjA (accessed on 20 September 2024).
- Hunt, K.; Gray, C.; Maclean, A.; Smillie, S.; Bunn, C.; Wyke, S. Do weight management programmes delivered at professional football clubs attract and engage high risk men? A mixed-methods study. BMC Public Health 2014, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hunt, K.; Wyke, S.; Bunn, C.; Donnachie, C.; Reid, N.; Gray, C. Scale-up and scale-out of a gender-sensitized weight management and healthy living program delivered to overweight men via professional sports clubs: The wider implementation of Football Fans in Training (FFIT). Int. J. Environ. Res. Public Health 2020, 17, 584. [Google Scholar] [CrossRef]
- Wilcock, R.; Smith, A.; Haycock, D. Designing community sports-based programmes for men with mental illness: A qualitative study of the offload rugby league programme. Ment. Health Phys. Act. 2021, 20, 1–8. [Google Scholar] [CrossRef]
- Parnell, D.; Pringle, A.; McKenna, J.; Zwolinsky, S.; Rutherford, Z.; Hargreaves, J.; Trotter, L.; Rigby, M.; Richardson, D. Reaching older people with PA delivered in football clubs: The reach, adoption and implementation characteristics of the Extra Time Programme. BMC Public Health 2015, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Jackman, P.; Lane, A.; Allen-Collinson, J.; Henderson, H. Older adults’ and service providers’ experiences of a settings-based health promotion initiative in English football. Health Promot. Int. 2023, 38, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Pringle, A.; Parnell, D.; Zwolinsky, S.; Hargreaves, J.; McKenna, J. Effect of a health-improvement pilot programme for older adults delivered by a professional football club: The Burton Albion case study. Soccer Soc. 2014, 15, 902–918. [Google Scholar]
- Pringle, A.; Zwolinsky, S.; McKenna, J.; Robertson, S.; Daly-Smith, A.; White, A. Health improvement for men and hard-to-engage-men delivered in English Premier League football clubs. Health Educ. Res. 2014, 29, 503–520. [Google Scholar] [CrossRef]
- Willock, R.; Smith, A. Offload Evaluation Report; Edge Hill University: Lancashire, UK, 2019. [Google Scholar]
- Fothergill, M.; Gill, G.; Graham, P. The beautiful game bringing families together: Children’s and parents’ experiences of a family football programme. Health Promot. Int. 2024, 39, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pringle, A.; Zwolinsky, S.; McKenna, J.; Daly-Smith, A.; Robertson, S.; White, A. Effect of a national programme of men’s health delivered in English Premier League football clubs. Public Health 2013, 127, 18–26. [Google Scholar] [CrossRef]
- George, E.; El Masri, A.; Kwasnicka, D.; Romeo, A.; Cavallin, S.; Bennie, A.; Kolt, G.S.; Guagliano, J. Effectiveness of adult health promotion interventions delivered through professional sport: Systematic review and meta-analysis. Sports Med. 2022, 52, 2637–2655. [Google Scholar] [CrossRef]
- Local Government Association. Public Health in Local Government: Celebrating 10 Years of Transformation. 2022. Available online: https://www.local.gov.uk/publications/public-health-local-government-celebrating-10-years-transformation (accessed on 24 October 2024).
- Misener, L.; Misener, K. Examining the integration of sport and health promotion: Partnership or paradox? Int. J. Sport Policy Politics 2016, 8, 695–712. [Google Scholar] [CrossRef]
- Duffell, T.; Haycock, D.; Smith, A. Exploring the increasing interdependence of community sport and health policy in England. Int. J. Sport Policy Politics 2023, 15, 603–618. [Google Scholar] [CrossRef]
- Sport England. Active Partnerships. 2024. Available online: https://www.sportengland.org/funding-and-campaigns/active-partnerships (accessed on 24 October 2024).
- Active Partnerships. Who We Are. 2024. Available online: https://activepartnerships.org/who-we-are/ (accessed on 24 October 2024).
- Sport England. Uniting the Movement: A 10-Year Vision to Transform Lives and Communities Through Sport and Physical Activity. 2021. Available online: https://sportengland-production-files.s3.eu-west-2.amazonaws.com/s3fs-public/2021-02/Sport%20England%20-%20Uniting%20the%20Movement%27.pdf?VersionId=7JxbS7dw40CN0g21_dL4VM3F4P1YJ5RW (accessed on 13 September 2024).
- Sport England. Implementing Uniting the Movement: Years 2–4, 2022–2025. 2021. Available online: https://sportengland-production-files.s3.eu-west-2.amazonaws.com/s3fs-public/2021-12/Implementing%20Uniting%20The%20Movement%20Years%202-4%202022-25_1.pdf?VersionId=Lx.DwY.JWxokQoRCFa2cLfVqa1QVvLsn (accessed on 13 September 2024).
- BNSSG Healthier Together. Our Future Health. 2022. Available online: https://bnssghealthiertogether.org.uk/wp-content/uploads/2022/11/OurFutureHealth-Sept-2022.pdf) (accessed on 3 October 2024).
- Office for Health Improvement and Disparities Public health profiles: Obesity profile. 2024. Available online: https://fingertips.phe.org.uk/profile/national-child-measurement-programme/data#page/1/gid/8000011/pat/221/par/nE54000039/ati/66/are/nE38000222/iid/90316/age/200/sex/4/cat/-1/ctp/-1/yrr/1/cid/4/tbm/1 (accessed on 15 November 2024).
- Bristol City Council. A Sport and Physical Activity Strategy for Bristol, 2020–2025. 2020. Available online: https://www.bristol.gov.uk/files/documents/4791-sport-physical-activity-strategy-2020-2025/file (accessed on 3 October 2024).
- BNSSG Healthier Together. Bristol, North Somerset and South Gloucestershire Integrated Care System Strategy. 2023. Available online: https://bnssghealthiertogether.org.uk/wp-content/uploads/2024/10/ICS_Strategy_V2.8_01112024.pdf (accessed on 3 October 2024).
- Bristol City Council. The Power of Us: One City, Many Communities. Director of Public Health Annual Report 2023. 2023. Available online: https://democracy.bristol.gov.uk/documents/s90214/BD16068%20Public%20Health%20Report%202023%20Power%20of%20Us%2023-11-23.pdf (accessed on 3 October 2024).
- Bristol Sport Foundation. Our Programmes. 2025. Available online: https://www.bristol-sport.co.uk/bristol-sport-foundation/programmes/our-programmes/ (accessed on 15 January 2024).
- Robins Foundation. Health and Wellbeing. 2025. Available online: https://www.bcfc.co.uk/robins-foundation/what-we-do/health-and-wellbeing/ (accessed on 15 January 2024).
- Bristol Bears Foundation. Programmes. 2025. Available online: https://www.bristolbearsrugby.com/bears-foundation/programmes/ (accessed on 15 January 2024).
- Bristol Rovers Community Trust. Projects. 2025. Available online: https://www.bristolroverscommunity.org.uk/projects (accessed on 15 January 2024).
- Bristol Sport Foundation. Our Impact. 2024. Available online: https://www.bristol-sport.co.uk/bristol-sport-foundation/programmes/our-impact/ (accessed on 4 October 2024).
- Bristol Bears Community Foundation About the Foundation. 2024. Available online: https://www.bristolbearsrugby.com/bears-foundation/about-the-foundation/ (accessed on 4 October 2024).
- Luke, D.; Harris, J. Network Analysis in Public Health: History, methods, and applications. Annu. Rev. Public Health 2007, 28, 69–93. [Google Scholar] [CrossRef]
- Timm, I.; Rapp, S.; Jeuter, C.; Bachert, P.; Reichert, M.; Woll, A.; Waesche, H. Interorganizational networks in physical activity promotion: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 7306. [Google Scholar] [CrossRef] [PubMed]
- Freeman, L. The Development of Social Network Analysis: A Study in the Sociology of Science; Empirical Press: New York, NY, USA, 2004. [Google Scholar]
- Knoke, D.; Yang, S. Social Network Analysis: Quantitative Applications in the Social Sciences, 2nd ed; SAGE: Newcastle upon Tyne, UK, 2008. [Google Scholar]
- Brazier, J.; Foster, C.; Murphy, J.; Townsend, N. Stakeholders’ Perceptions on the Role of Professional Sports Clubs and Organisations in Local Community Health Promotion. Health Promot. Int. ubmitted. 2025. [Google Scholar]
- Borgatti, S.; Everett, M.; Freeman, L. Ucinet 6 for Windows: Software for Social Network Analysis; Analytic Technologies: Harvard, MA, USA, 2002. [Google Scholar]
- Kornbluh, M.; Neal, J. Social Network Analysis. In Handbook of Methodological Approaches to Community-Based Research: Qualitative, Quantitative, and Mixed-Methods; Jason, L., Glenwick, D., Eds.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Alonso, A.; O’Shea, M. You only get back what you put in: Perceptions of professional sport organizations as community anchors. Community Dev. 2012, 43, 656–676. [Google Scholar] [CrossRef]
- Pringle, A.; Zwolinsky, S.; McKenna, J.; Daly-Smith, A.; Robertson, S.; White, A. Delivering men’s health interventions in English Premier League football clubs: Key design characteristics. Public Health 2013, 127, 716–726. [Google Scholar] [CrossRef]
- Lansley, S.; Parnell, D. Football for Health: Getting Strategic. Soccer Soc. 2015, 17, 259–266. [Google Scholar] [CrossRef]
- Pringle, A.; Parnell, D.; Rutherford, Z.; McKenna, J.; Zwolinsky, S.; Hargreaves, J. Sustaining health improvement activities delivered in English professional football clubs using evaluation: A short communication. Soccer Soc. 2016, 17, 759–769. [Google Scholar] [CrossRef]
- Curran, K.; Rosenbaum, S.; Parnell, D.; Stubbs, B.; Pringle, A.; Hargreaves, J. Tackling mental health: The role of professional football clubs. Sport Soc. 2017, 20, 281–291. [Google Scholar] [CrossRef]
- Rutherford, Z.; Zwolinsky, S.; Kime, N.; Pringle, A. A Mixed-Methods Evaluation of CARE (Cancer and Rehabilitation Exercise): A physical activity and health intervention, delivered in a community football trust. Int. J. Environ. Res. Public Health 2021, 18, 3327. [Google Scholar] [CrossRef]
- Tell, D.; Oldeide, O.; Larsen, T.; Haug, E. Lessons learned from an intersectoral collaboration between the public sector, NGOs, and sports clubs to meet the needs of vulnerable youths. Societies 2022, 12, 13. [Google Scholar] [CrossRef]
- Nobles, J.; Fox, C.; Inman-Ward, A.; Beasley, T.; Redwood, S.; Jago, R.; Foster, C. Navigating the river (s) of systems change: A multi-methods, qualitative evaluation exploring the implementation of a systems approach to physical activity in Gloucestershire, England. BMJ Open 2022, 12, e063638. [Google Scholar] [CrossRef] [PubMed]
- Crane, M.; Nathan, N.; McKay, H.; Lee, K.; Wiggers, J.; Bauman, A. Understanding the sustainment of population health programmes from a whole-of-system approach. Health Res. Policy Syst. 2022, 20, 37–49. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organisation Classification | % of Survey Respondents | % of Network | Representation in Figures |
|---|---|---|---|
| PSCO | 22.2% (n = 4) | 5.6% (n = 5) |  |
| Sport/PA Sector | 33.3% (n = 6) | 18.9% (n = 17) |  |
| Public Sector | 11.1% (n = 2) | 13.3% (n = 12) |  |
| VCFSE Sector | 16.7% (n = 3) | 28.9% (n = 26) |  |
| Education/Research Sector | 0% (n = 0) | 7.8% (n = 7) |  |
| PCN/Health | 16.7% (n = 3) | 24.4% (n = 22) |  |
| Other | 0% (n = 0) | 1.1% (n = 1) |  |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brazier, J.; Murphy, J.; Foster, C.; Townsend, N. Where Do Professional Sports Clubs and Organisations Sit Within a Local Health Promotion System? A Social Network Analysis Study. Int. J. Environ. Res. Public Health 2025, 22, 244. https://doi.org/10.3390/ijerph22020244
Brazier J, Murphy J, Foster C, Townsend N. Where Do Professional Sports Clubs and Organisations Sit Within a Local Health Promotion System? A Social Network Analysis Study. International Journal of Environmental Research and Public Health. 2025; 22(2):244. https://doi.org/10.3390/ijerph22020244
Chicago/Turabian StyleBrazier, Jack, Joey Murphy, Charlie Foster, and Nick Townsend. 2025. "Where Do Professional Sports Clubs and Organisations Sit Within a Local Health Promotion System? A Social Network Analysis Study" International Journal of Environmental Research and Public Health 22, no. 2: 244. https://doi.org/10.3390/ijerph22020244
APA StyleBrazier, J., Murphy, J., Foster, C., & Townsend, N. (2025). Where Do Professional Sports Clubs and Organisations Sit Within a Local Health Promotion System? A Social Network Analysis Study. International Journal of Environmental Research and Public Health, 22(2), 244. https://doi.org/10.3390/ijerph22020244