
Global Suicide Mortality Rates (2000–2019): Clustering, Themes, and Causes Analyzed through Machine Learning and Bibliographic Data


Abstract
1. Introduction
2. Materials and Methods
2.1. Suicide Mortality Rate Dataset
2.2. Web of Science (WoS) Bibliographic Records and Keywords
2.3. Clustering
2.4. Quantification of Countries into High-, Medium-, and Low-Suicide-Mortality-Rate Groups
2.5. Analysis of Keyword Co-Occurrences Using VOSviewer
2.6. Association Rule Mining
2.7. Network Visualization
2.8. Deep Learning
2.9. Data Analytics Software
3. Results
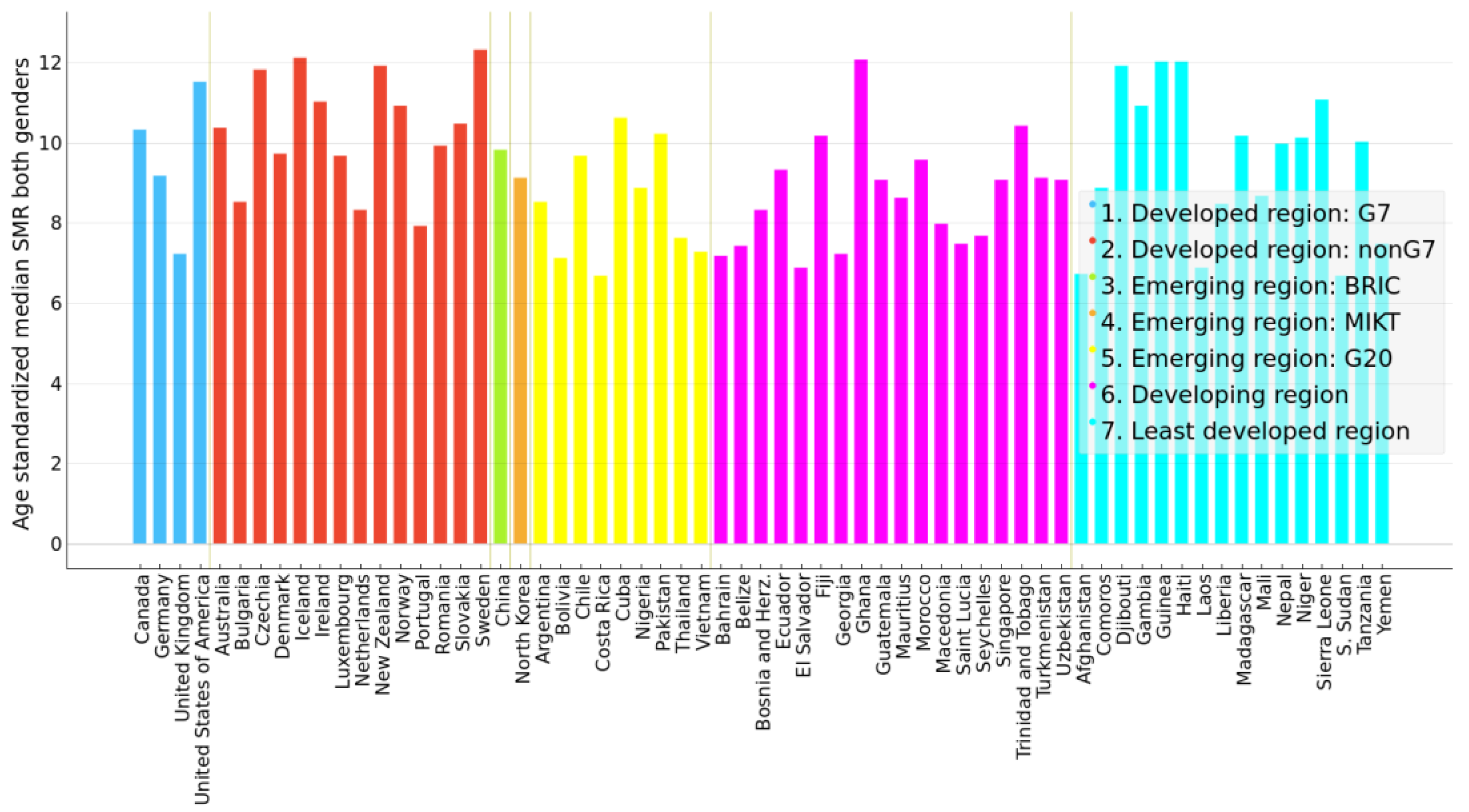
3.1. Summary Statistics of Suicide Mortality Rates
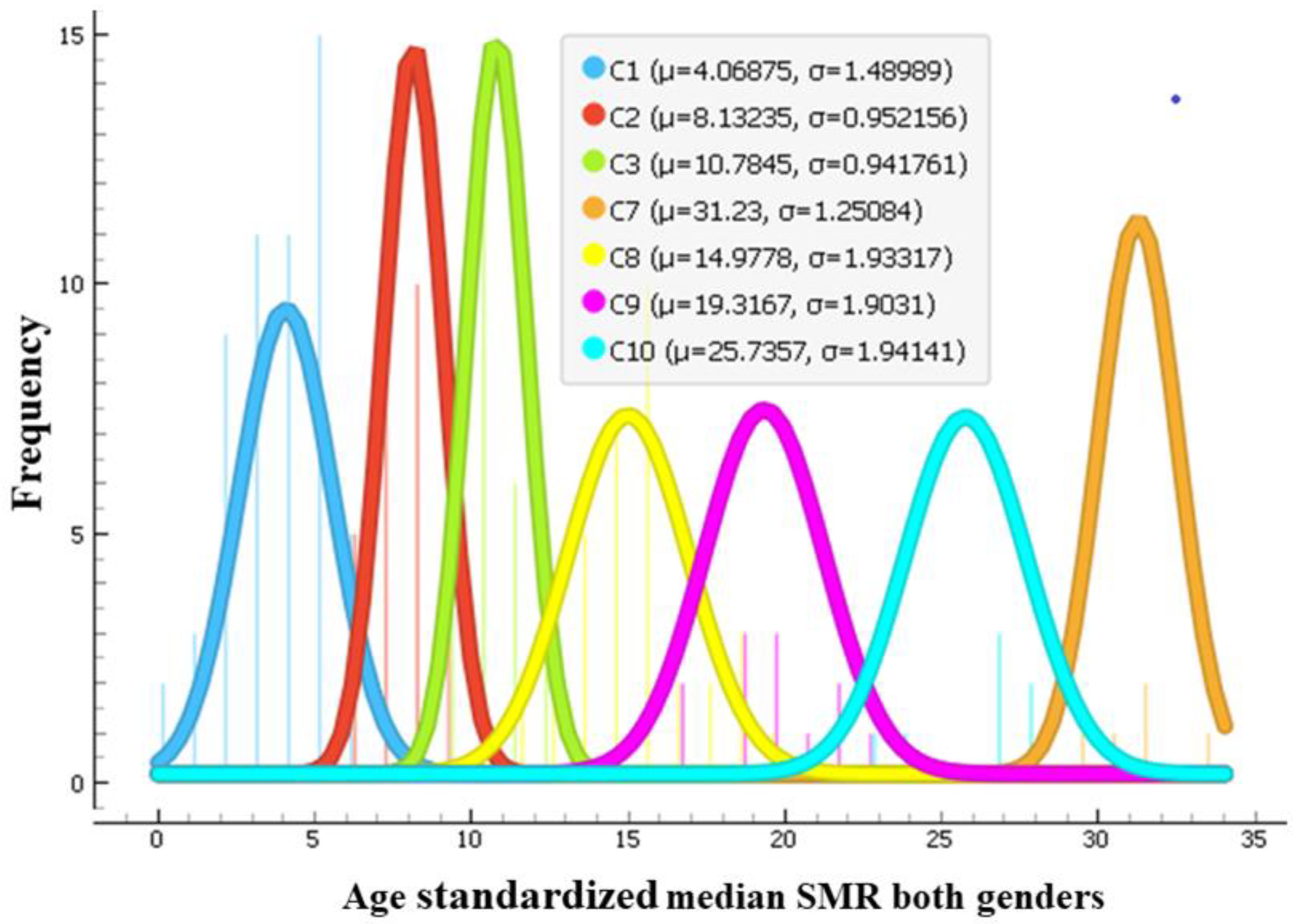
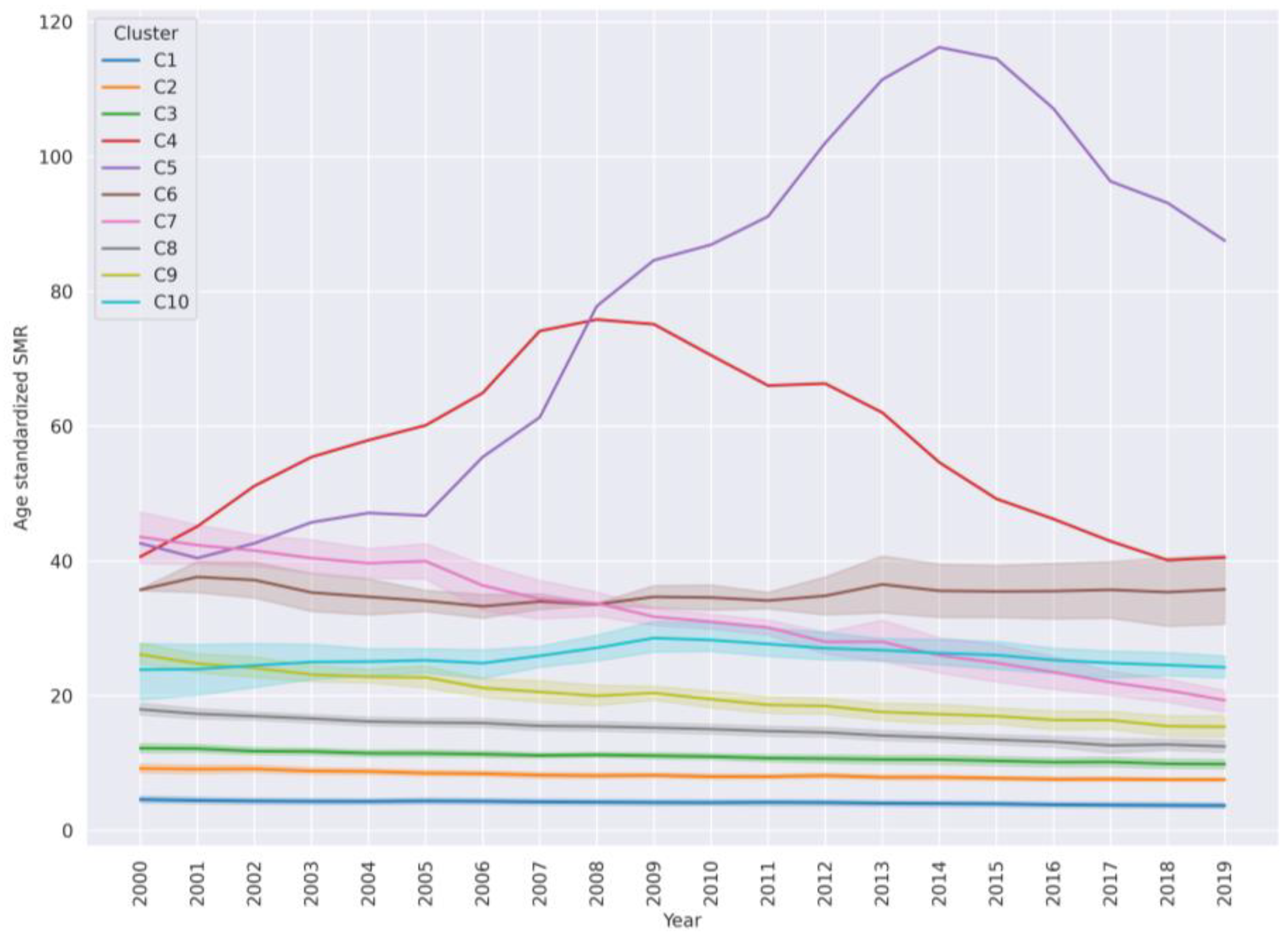
3.2. Clustering of Countries into Groups of Similar SMR Magnitude and Dynamics
3.3. Characteristics of High-, Medium-, and Low-SMR Country Clusters
3.3.1. High- and Mixed-High-and-Medium-Suicide-Mortality-Rate Country Clusters
3.3.2. Medium-SMR Country Clusters
3.3.3. Low-Suicide-Mortality-Rate Country Clusters
3.3.4. Increasing SMR
3.4. Results of Association Rule Mining
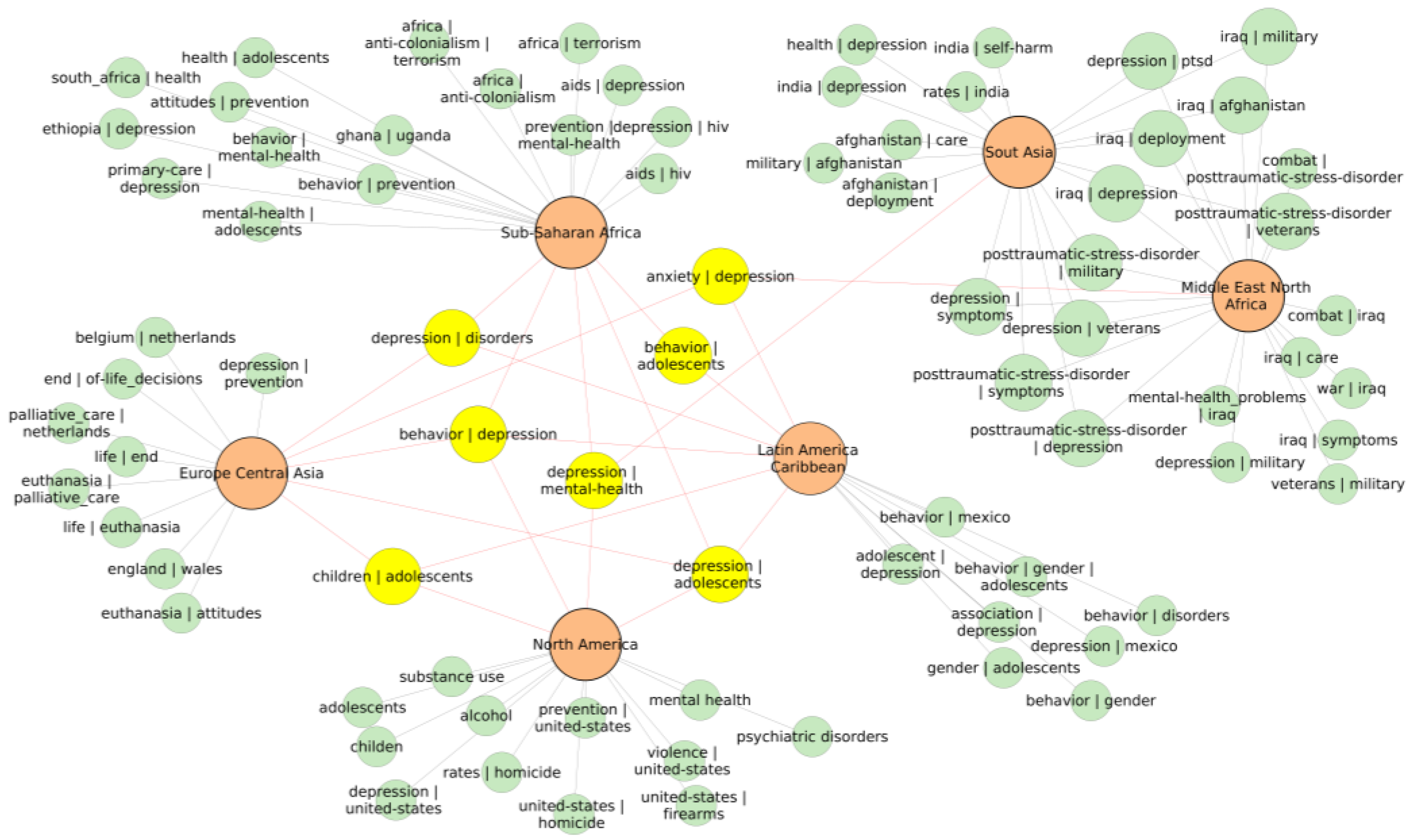
3.5. Descriptive Analysis of High-, Medium-, and Low-SMR Country Clusters Across Geographic Regions Using Visualization of Similarities Viewer (VOSviewer) Tool and Frequent Keyword Occurrences
3.5.1. Europe and Central Asia
3.5.2. Sub-Saharan Africa
3.5.3. Middle East and North Africa
3.5.4. East Asia and Pacific
3.5.5. South Asia
3.5.6. Latin America and Caribbean
3.5.7. North America
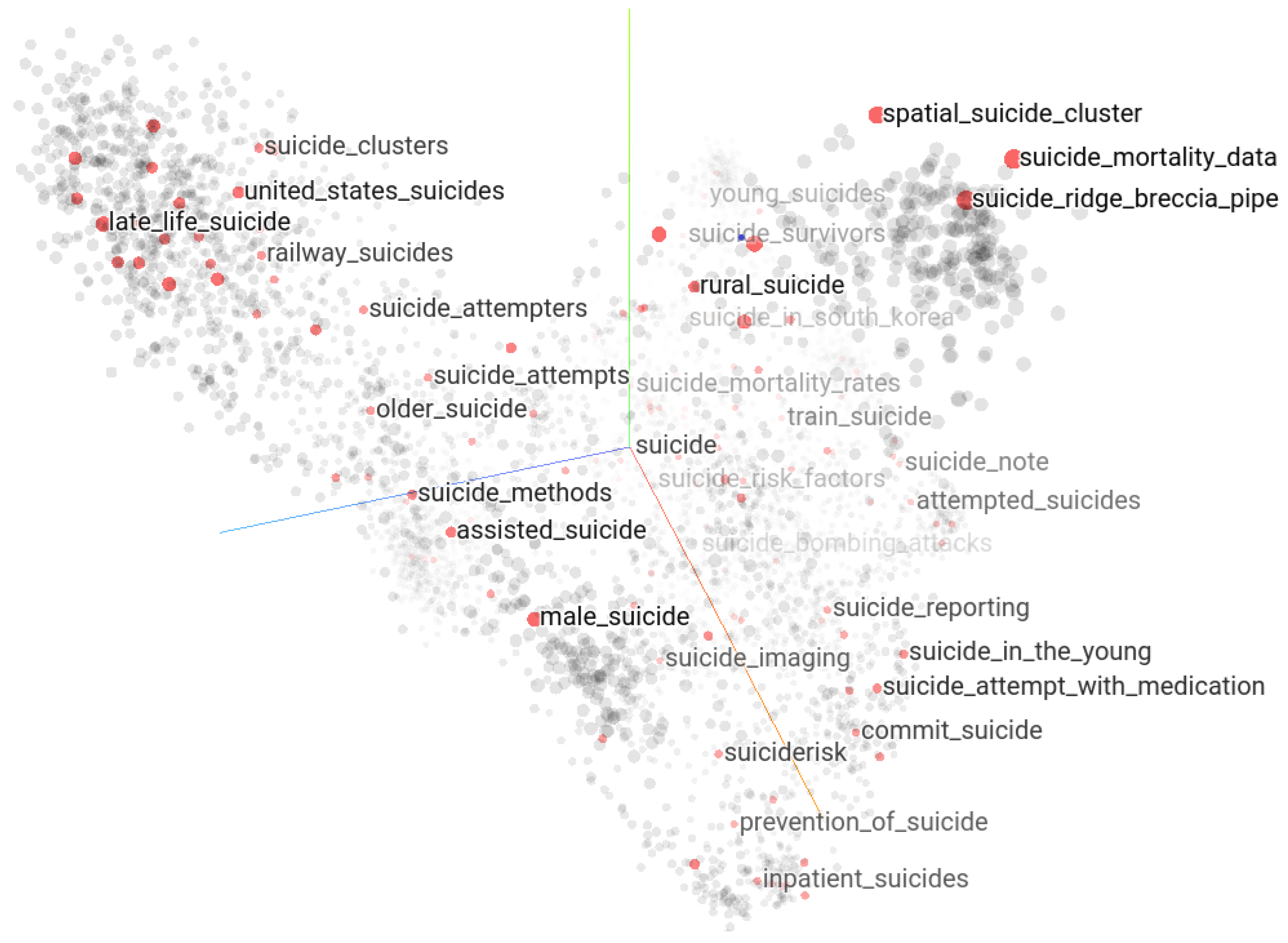
3.6. Word Embedding of Suicide-Related Keywords
3.7. How Keyword Analysis and Word Embedding Helps: Use Case about Loneliness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Global Health Observatory. Suicide Rates. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/age-standardized-suicide-rates-(per-100-000-population) (accessed on 29 July 2024).
- World Bank. DataBank World Development Indicators. Suicide Mortality Rate (per 100,000 Population). Available online: https://databank.worldbank.org/reports.aspx?source=2&series=SH.STA.SUIC.P5 (accessed on 1 November 2023).
- World Health Organization Suicide Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 13 August 2024).
- Aleman, A.; Denys, D. A roadmap for suicide research and prevention. Nature 2014, 509, 421–423. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.J.; Apter, A.; Bertolote, J.; Beautrais, A.; Currier, D.; Haas, A.; Hegerl, U.; Lonnqvist, J.; Malone, K.; Marusic, A.; et al. Suicide prevention strategies: A systematic review. JAMA 2005, 294, 2064–2074. [Google Scholar] [CrossRef] [PubMed]
- Zalsman, G.; Hawton, K.; Wasserman, D.; van Heeringen, K.; Arensman, E.; Sarchiapone, M.; Carli, V.; Höschl, C.; Barzilay, R.; Balazs, J.; et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry 2016, 3, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.J.; Michel, C.A.; Auerbach, R.P. Improving suicide prevention through evidence-based strategies: A systematic review. Am. J. Psychiatry 2021, 178, 611–624. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, D.; Carli, V.; Iosue, M.; Javed, A.; Herrman, H. Suicide prevention in childhood and adolescence: A narrative review of current knowledge on risk and protective factors and effectiveness of interventions. Asia-Pac. Psychiatry 2021, 13, 12452. [Google Scholar] [CrossRef]
- Glenn, C.R.; Kleiman, E.M.; Kellerman, J.; Pollak, O.; Cha, C.B.; Esposito, E.C.; Porter, A.C.; Wyman, P.A.; Boatman, A.E. Annual research review: A meta-analytic review of worldwide suicide rates in adolescents. J. Child Psychol. Psychiatr. 2020, 61, 294–308. [Google Scholar] [CrossRef]
- Castellví, P.; Lucas-Romero, E.; Miranda-Mendizábal, A.; Parés-Badell, O.; Almenara, J.; Alonso, I.; Blasco, M.J.; Cebrià, A.; Gabilondo, A.; Gili, M.; et al. Longitudinal association between self-injurious thoughts and behaviors and suicidal behavior in adolescents and young adults: A systematic review with meta-analysis. J. Affect. Disord. 2017, 215, 37–48. [Google Scholar] [CrossRef]
- Bhatia, G.; Thapa, P.; Mathur, R. The top 100 most cited publications on suicide: A citation analysis. OMEGA J. Death Dying 2023, 302228231189642. [Google Scholar] [CrossRef]
- Värnik, P. Suicide in the world. Int. J. Environ. Res. Public Health 2012, 9, 760–771. [Google Scholar] [CrossRef]
- Claveria, O. Global economic uncertainty and suicide: Worldwide evidence. Soc. Sci. Med. 2022, 305, 115041. [Google Scholar] [CrossRef]
- Brådvik, L. Suicide risk and mental disorders. Int. J. Environ. Res. Public Health 2018, 15, 2028. [Google Scholar] [CrossRef] [PubMed]
- San Too, L.; Spittal, M.J.; Bugeja, L.; Reifels, L.; Butterworth, P.; Pirkis, J. The association between mental disorders and suicide: A systematic review and meta-analysis of record linkage studies. J. Affect. Disord. 2019, 259, 302–313. [Google Scholar]
- Lari, M.S.; Sefiddashti, S.E. Socio-economic, health and environmental factors influencing suicide rates: A cross-country study in the Easter Mediterranean region. J. Forensic Leg. Med. 2023, 93, 102463. [Google Scholar] [CrossRef]
- Li, Z.; Page, A.; Martin, G.; Taylor, R. Attributable risk of psychiatric and socio-economic factors for suicide from individual-level, population-based studies: A systematic review. Soc. Sci. Med. 2011, 72, 608–616. [Google Scholar] [PubMed]
- Chandler, A. Socioeconomic inequalities of suicide: Sociological and psychological intersections. Eur. J. Soc. Theory 2020, 23, 33–51. [Google Scholar] [CrossRef]
- Al-Shannaq, Y.; Aldalaykeh, M. Suicide literacy, suicide stigma, and psychological help seeking attitudes among Arab youth. Curr. Psychol. 2023, 42, 6532–6544. [Google Scholar] [CrossRef] [PubMed]
- Yao, Z.-Y.; Wang, T.; Yu, Y.-K.; Li, R.; Sang, X.; Fu, Y.-N.; Gong, X.-J.; Sun, W.-J.; Liu, J.J.-W.; Wong, J.P.-H.; et al. Mental health literacy and suicidal ideation among Chinese college students: The mediating role of depressive symptoms and anxiety symptoms. J. Affect. Disord. 2023, 339, 293–301. [Google Scholar] [CrossRef]
- Donnelly, H.K.; Richardson, D.; Solberg, V.S.H. Identifying important predictors of adolescent suicide ideation, planning, and attempt in low- and middle-income countries. Suicide Life-Threat. Behav. 2023. early view. [Google Scholar] [CrossRef]
- Knipe, D.; John, A.; Padmanathan, P.; Eyles, E.; Dekel, D.; Higgins, J.P.; Bantjes, J.; Dandona, R.; Macleod-Hall, C.; McGuinness, L.A.; et al. Suicide and self-harm in low-and middle-income countries during the COVID-19 pandemic: A systematic review. PLoS Glob. Public Health 2022, 2, 0000282. [Google Scholar] [CrossRef]
- Mann, J.J.; Rizk, M.M. A brain-centric model of suicidal behavior. Am. J. Psychiatry 2020, 177, 902–916. [Google Scholar] [PubMed]
- Bertuccio, P.; Ameria, A.; Grande, E.; La Vecchia, C.; Costanza, A.; Aguglia, A.; Berardelli, I.; Serafini, G.; Amore, M.; Pompili, M.; et al. Global trends in youth suicide from 1990 to 2020: An analysis of data from the WHO mortality database. Clin. Med. 2024, 70, 102506. [Google Scholar] [CrossRef]
- Lersch, K.M. Exploring the geography of suicide threats and suicide attempts: An application of Risk Terrain Modeling. Soc. Sci. Med. 2020, 249, 112860. [Google Scholar] [CrossRef] [PubMed]
- Pranckeviciene, E. Global Suicide Mortality Rates (2000–2019) and Bibliographic Data (v1.0) [Data Set]. Zenodo. Available online: https://zenodo.org/records/12267302 (accessed on 1 November 2023).
- Web of Science Bibliographic Database. Available online: https://www.webofknowledge.com (accessed on 1 November 2023).
- Github Repository. Available online: https://github.com/erinijapranckeviciene/idkwdan (accessed on 29 September 2023).
- Demsar, J.; Curk, T.; Erjavec, A.; Gorup, C.; Hocevar, T.; Milutinovic, M.; Mozina, M.; Polajnar, M.; Toplak, M.; Staric, A.; et al. Orange: Data Mining Toolbox in Python. J. Mach. Learn. Res. 2013, 14, 2349–2353. [Google Scholar]
- Van Eck, N.J.; Waltman, L. Citation-based clustering of publications using CitNetExplorer and VOSviewer. Scientometrics 2017, 111, 1053–1070. [Google Scholar] [CrossRef] [PubMed]
- Waltman, L.; Van Eck, N.J.; Noyons, E.C.M. A unified approach to mapping and clustering of bibliometric networks. J. Informetr. 2010, 4, 629–635. [Google Scholar] [CrossRef]
- Raschka, S. MLxtend: Providing machine learning and data science utilities and extensions to Python’s scientific computing stack. J. Open Source Softw. 2018, 3, 638. [Google Scholar] [CrossRef]
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A software environment for integrated models of biomolecular interaction networks. Genome Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef]
- Chollet, F. Deep Learning with Python; Simon Schuster: New York, NY, USA, 2021. [Google Scholar]
- Keras Tensorflow Projector. Available online: https://projector.tensorflow.org/ (accessed on 1 November 2023).
- Anthony, M.; Groh, C.; Gash, J. Suicide in Guyana: Nurses’ perspectives. J. Forensic Nurs. 2017, 13, 14–19. [Google Scholar] [CrossRef]
- Rezaeian, M. The geographical belt of self-immolation. Burns 2017, 43, 896–897. [Google Scholar] [CrossRef]
- Arafat, S.Y.; Singh, R.; Singh, K.; Amin, R. Trend and Geographical Distribution of Suicide Research: A Bibliometric Analysis of Three Decades. Int. J. Ment. Health Addict. 2024, 5, 1–10. [Google Scholar] [CrossRef]
- Sinyor, M.; Hawton, K.; Appleyby, L.; Armstrong, G.; Ueda, M.; Gunnell, D.; Kapur, N.; Chang, S.; Arensman, E.; O’Connor, R.C.; et al. The coming global economic downturn and suicide: A call to action. Nat. Ment. Health 2023, 1, 233–235. [Google Scholar] [CrossRef]
- Stack, S. Suicide: A 15-year review of the sociological literature part I: Cultural and economic factors. Suicide Life-Threat. Behav. 2000, 30, 145–162. [Google Scholar] [CrossRef] [PubMed]
- Stack, S. Contributing factors to suicide: Political, social, cultural and economic. Prev. Med. 2021, 1, 106498. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G.; Brent, D.A.; Gunnel, D.; O’Connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B.H. Suicide and suicide risk. Nat. Rev. Dis. Primers 2019, 5, 74. [Google Scholar] [CrossRef] [PubMed]
- Boldrini, M.; Xiao, Y.; Sing, T.; Zhu, C.; Jabbi, M.; Pantazopoulos, H.; Gürsoy, G.; Martinowich, K.; Punzi, G.; Vallender, E.J.; et al. Omics approaches to investigate the pathogenesis of suicide. Biol. Psychiatry 2024. [Google Scholar] [CrossRef]
- Marušič, A. History and geography of suicide: Could genetic risk factors account for the variation in suicide rates? Am. J. Med. Genet. Part C Semin. Med. Genet. 2005, 133, 43–47. [Google Scholar] [CrossRef]
- Ernst, C.; Mechawar, N.; Turecki, G. Suicide neurobiology. Prog. Neurobiol. 2009, 89, 315–330. [Google Scholar] [CrossRef]
- Strumila, R.; Lengvenyte, A.; Zdanavicius, L.; Badaras, R.; Dlugauskas, E.; Lesinskiene, S.; Matiekus, E.; Marcinkevicius, M.; Venceviciene, L.; Utkus, A.; et al. Higher levels of plasma Adrenocorticotropic hormone (ACTH) are associated with lower suicidal ideation in depressed patients compared to controls and suicide attempters, independently from depression severity. Compr. Psychoneuroendocrinol. 2024, 19, 100235. [Google Scholar] [CrossRef]
- Thorlindsson, T.; Bernburg, J.G. Durkheim’s theory of social order and deviance: A multi-level test. Eur. Sociol. Rev. 2004, 20, 271–285. [Google Scholar] [CrossRef]
- Boggs, J.M.; Kafka, J.M. A critical review of text mining applications for suicide research. Curr. Epidemiol. Rep. 2022, 9, 126–134. [Google Scholar] [CrossRef]
- Cheng, Q.; Lui, C.S. Applying text mining methods to suicide research. Suicide Life-Threat. Behav. 2021, 51, 137–147. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Interval of Percentiles | Label of the SMR Level | Abbreviation | Corresponding Interval of Age-Standardized Suicide Mortality Rate per 100,000 Population |
|---|---|---|---|
| [0, 10) | Low | L | [0, 3.4) |
| [10, 20) | Low medium | LM | [3.4, 5.1) |
| [20, 30) | Low high | LH | [5.1, 6.6) |
| [30, 40) | Medium low | ML | [6.6, 8.119) |
| [40, 50) 1 | Medium | M | [8.119, 9.9) |
| [50, 60) | Medium | M | [9.9, 11.5) |
| [60, 70) | Medium high | MH | [11.5, 13.7) |
| [70, 80) | High low | HL | [13.7, 16.6) |
| [80, 90) | High medium | HM | [16.6, 22.8) |
| [90, 100] | High | H | [22.8, 117] |
| Year | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SMR Estonia | 25 | 26.1 | 25.8 | 22.3 | 23.1 | 19.1 | 16.8 | 17.5 | 16.2 | 19.2 | 15.4 | 14.7 | 17.2 | 14.9 | 16.2 | 13.4 | 12.5 | 15.2 | 11.6 | 12 |
| Percentile interval | [90, 100] | [90, 100] | [90, 100] | [80, 90) | [90, 100] | [80, 90) | [80, 90) | [80, 90) | [70, 80) | [80, 90) | [70, 80) | [70, 80) | [80, 90) | [70, 80) | [70, 80) | [60, 70) | [60, 70) | [70, 80) | [60, 70) | [60, 70) |
| Bin | [22.8, 117) | [22.8, 117) | [22.8, 117) | [16.6, 22.8) | [22.8, 117) | [16.6, 22.8) | [16.6, 22.8) | [16.6, 22.8) | [13.7, 16.6) | [16.6, 22.8) | [13.7, 16.6) | [13.7, 16.6) | [16.6, 22.8) | [13.7, 16.6) | [13.7, 16.6) | [11.5, 13.7) | [11.5, 13.7) | [13.7, 16.6) | [11.5, 13.7) | [11.5, 13.7) |
| Label | H | H | H | HM | H | HM | HM | HM | HL | HM | HL | HL | HM | HL | HL | MH | MH | HL | MH | MH |
| Year | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SMR Qatar | 7.6 | 7.6 | 7.4 | 6.9 | 6.6 | 6.3 | 6.1 | 7.2 | 6.8 | 6.7 | 6.4 | 6.2 | 5.8 | 5.3 | 5 | 4.9 | 4.8 | 4.6 | 4.6 | 4.7 |
| Label | ML | ML | ML | ML | ML | LH | LH | ML | ML | ML | LH | LH | LH | LH | LM | LM | LM | LM | LM | LM |
| Statistics | Males | Females | Both Genders |
|---|---|---|---|
| Minimum | 0 | 0 | 0 |
| 1st Quartile (Q25) | 8.3 | 2.5 | 5.6 |
| Median (Q50) | 14.5 | 4.75 | 9.8 |
| 3rd Quartile (Q75) | 23.9 | 7.2 | 14.9 |
| Maximum | 195.2 | 46.3 | 116.2 |
| Mean | 18.75 | 5.4 | 9.8 |
| Standard Deviation | 16.99 | 4.2 | 11.7 |
| Cluster | Geographic Region | Country |
|---|---|---|
| C4, Very high SMR N = 1 | Sub-Saharan Africa n = 1 | Eswatini |
| C5, Very high SMR N = 1 | Sub-Saharan Africa n = 1 | Lesotho |
| C6, High SMR N = 2 | East Asia and Pacific n = 1 | Kiribati |
| Latin America and Caribbean n = 1 | Guyana | |
| C7, High SMR N = 5 | Europe and Central Asia n = 4 | Belarus, Kazakhstan, Lithuania, Russian Federation |
| Sub-Saharan Africa n = 1 | Botswana | |
| C9, High SMR N = 12 | East Asia and Pacific n = 2 | Mongolia, Vanuatu |
| Europe and Central Asia n = 5 | Estonia, Hungary, Latvia, Slovenia, Ukraine | |
| South Asia n = 1 | Sri Lanka | |
| Sub-Saharan Africa n = 4 | Cote d’Ivoire, Eritrea, Namibia, Zambia | |
| C10, High SMR N = 7 | East Asia and Pacific n = 2 | Micronesia, South Korea |
| Latin America and Caribbean n = 2 | Suriname | |
| Sub-Saharan Africa n = 4 | Central African Republic, Mozambique, South Africa, Zimbabwe |
| Geographic Region | Country |
|---|---|
| East Asia and Pacific n = 3 | Japan, Samoa, Solomon Islands |
| Europe and Central Asia n = 11 | Austria, Belgium, Croatia, Finland, France, Kyrgyzstan, Moldova, Montenegro, Poland, Serbia, Switzerland |
| Latin America and Caribbean n = 1 | Uruguay |
| South Asia n = 1 | India |
| Sub-Saharan Africa n = 20 | Angola, Benin, Burkina Faso, Burundi, Cabo Verde, Cameroon, Chad, Congo, Dem. Rep. Congo, Equatorial Guinea, Ethiopia, Gabon, Guinea-Bissau, Kenya, Malawi, Rwanda, Senegal, Somalia, Togo, Uganda |
| Cluster | Geographic Region | Country |
|---|---|---|
| Cluster C2 Medium SMR, N = 34 | East Asia and Pacific n = 5 | Laos, North Korea, Singapore, Thailand, Vietnam |
| Europe and Central Asia n = 11 | Bosnia and Herzegovina, Bulgaria, Denmark, Georgia, Germany, Macedonia, Netherlands, Portugal, Romania, United Kingdom, Uzbekistan | |
| Latin America and Caribbean n = 7 | Argentina, Belize, Bolivia, Costa Rica, Ecuador, El Salvador, St. Lucia | |
| Middle East and North Africa n = 3 | Bahrain, Morocco, Yemen | |
| South Asia n = 1 | Afghanistan | |
| Sub-Saharan Africa n = 7 | Comoros, Liberia, Mali, Mauritius, Nigeria, South Sudan, Seychelles | |
| Cluster C3 Medium High SMR N = 29 | East Asia and Pacific n = 4 | Australia, China, Fiji, New Zealand |
| Europe and Central Asia n = 8 | Czechia, Iceland, Ireland, Luxembourg, Norway, Slovakia, Sweden, Turkmenistan | |
| Latin America and Caribbean n = 5 | Chile, Cuba, Guatemala, Haiti, Trinidad and Tobago | |
| Middle East and North Africa n = 1 | Djibouti | |
| North America n = 2 | United States, Canada | |
| South Asia n = 2 | Nepal, Pakistan | |
| Sub-Saharan Africa n = 7 | Gambia, Ghana, Guinea, Madagascar, Niger, Sierra Leone, Tanzania |
| Geographic Region | Country |
|---|---|
| East Asia and Pacific n = 9 | Brunei Darussalam, Cambodia, Indonesia, Malaysia, Myanmar, Papua New Guinea, Philippines, Timor Leste, Tonga |
| Europe and Central Asia n = 9 | Albania, Armenia, Azerbaijan, Cyprus, Greece, Italy, Spain, Tajikistan, Turkey |
| Latin America and Caribbean n = 16 | Antigua and Barbuda, Bahamas, Barbados, Brazil, Colombia, Dominican Republic, Grenada, Honduras, Jamaica, Mexico, Nicaragua, Panama, Paraguay, Peru, St. Vincent and the Grenadines, Venezuela |
| Middle East and North Africa n = 16 | Algeria, Egypt, Iran, Iraq, Israel, Jordan, Kuwait, Lebanon, Libya, Malta, Oman, Qatar, Saudi Arabia, Syria, Tunisia, United Arab Emirates |
| South Asia n = 3 | Bangladesh, Bhutan, Maldives |
| Sub-Saharan Africa n = 3 | Mauritania, Sao Tome and Principe, Sudan |
| Cluster, SMR Category | Country | [SMR Q25, SMR Median, SMR Q75] | SMR Label | WoS Records | VOSviewer Keyword Annotations |
|---|---|---|---|---|---|
| C1, Low SMR N = 56 n = 9 | Albania | [4.425, 4.85, 7.625] | 1 Low Med. | 12 | Abuse, adolescents, schizophrenia, alcohol, depression, hopelessness, children, unemployment, financial crisis, economic crisis, mental health, care, euthanasia. |
| Armenia | [3.1, 4.15, 5.075] | Low | 2 | ||
| Azerbaijan | [3.9, 4.15, 4.525] | Low | 4 | ||
| Cyprus | [2.25, 3.45, 4.3] | Low | 9 | ||
| Greece | [2.675, 2.9, 3.7] | Low | 146 | ||
| Italy | [4.775, 4.9, 5.3] | Low | 296 | ||
| Spain | [5.475,5.7,6.2] | Low | 298 | ||
| Tajikistan | [4.775, 5, 5.125] | Low | 2 | ||
| Turkey | [2.3, 2.5,3.05] | Low | 324 | ||
| C2, Medium SMR N = 34 n = 11 | Bosnia and Herzegovina | [8.2, 8.35, 8.5] | Medium | 6 | Adolescents, children, depression, schizophrenia, self-harm, assisted suicide, cancer, care, euthanasia, end-of-life decisions, palliative care, physicians. |
| Bulgaria | [7.025, 8.55, 9.825] | Medium Wi. | 13 | ||
| Denmark | [8.75, 9.75, 11.1] | Medium | 340 | ||
| Georgia | [6.325, 7.25, 7.95] | Medium | 32 | ||
| Germany | [8.975, 9.2, 9.95] | Medium | 462 | ||
| Macedonia | [7.275, 8, 8.35] | Medium Wi. | 0 | ||
| Netherlands | [8.075, 8.35, 9.3] | Medium | 639 | ||
| Portugal | [7.5, 7.95, 8.625] | Medium | 66 | ||
| Romania | [9.075, 9.95, 10.725] | Medium | 66 | ||
| United Kingdom | [7, 7.25, 7.525] | Medium | 253 | ||
| Uzbekistan | [8.85, 9.1, 9.9] | Medium | 2 | ||
| C3, Medium high SMR N = 29 n = 8 | Czechia | [11.2, 11.85, 12.95] | Medium Hi. | 18 | Adolescents, bipolar disorder, children, depression, major depression, mental disorders, schizophrenia, self-harm, alcohol, antidepressants, gender, homicide, prevention, abuse, women, parasuicide. |
| Iceland | [11.45, 12.15, 12.75] | Medium Hi. | 32 | ||
| Ireland | [10, 11.05, 11.55] | Medium | 1258 | ||
| Luxembourg | [8.875, 9.7, 11.6] | Medium | 18 | ||
| Norway | [10.37, 10.95, 11.45] | Medium | 238 | ||
| Slovakia | [9.875, 10.5, 11.975] | Medium | 5 | ||
| Sweden | [12.075, 12.35, 12.7] | Medium Hi. | 558 | ||
| Turkmenistan | [6.975, 9.15, 14.825] | Medium Wi. | 0 | ||
| C7, High SMR N = 5 n = 4 | Belarus | [21.1, 30.3, 36.35] | High | 36 | Adolescents, children, depression, mental health, alcohol consumption, homicide, former USSR, inequalities, men, behavior. |
| Kazakhstan | [24, 29.5, 38.375] | High | 9 | ||
| Lithuania | [29.125, 31.55, 37.2] | High | 67 | ||
| Russian Federation | [28.8, 33.15, 43.675] | High | 28 | ||
| C8, Mixed medium and high SMR N = 36 n = 11 | Austria | [11.475, 12.1, 13.375] | Medium Hi. | 158 | Children, depression, Finland, gender, mental disorders, schizophrenia, assisted suicide, Belgium, care, euthanasia, Netherlands, end-of-life decisions, palliative care, Switzerland, Austria, homicide, prevention. |
| Belgium | [15.075, 16.55, 16.7] | High | 264 | ||
| Croatia | [12.1, 13.2, 14.925] | Medium Hi. | 52 | ||
| Finland | [14.4, 16.65, 18.375] | High | 380 | ||
| France | [11.475, 13.85, 14.925] | High Lo. | 415 | ||
| Kyrgyzstan | [11.275, 12.6, 14.425] | Medium Hi. | 1 | ||
| Moldova | [13.625, 15.8, 17.1] | High | 3 | ||
| Montenegro | [16.3, 17.15, 17.925] | High | 6 | ||
| Poland | [13.275, 14.95, 15.225] | High Lo. | 90 | ||
| Serbia | [11.925, 13.65, 15.875] | High Lo. | 35 | ||
| Switzerland | [10.475, 11.4, 13.925] | Medium Hi. | 284 | ||
| C9, High SMR N = 12 n = 5 | Estonia | [14.85, 16.5, 19.975] | High | 48 | Adolescence, deliberate self-harm, gender differences, life events, mental disorders, parasuicide, schizophrenia, seasonality, age, alcohol, Europe, childhood, depression, general population, help seeking, symptoms, women. |
| Hungary | [14.9, 19, 20.775] | High | 128 | ||
| Latvia | [17.1, 18.85, 22.1] | High | 10 | ||
| Slovenia | [14.7, 16.05, 21.325] | High | 70 | ||
| Ukraine | [18.525, 21.1, 28.325] | High | 24 |
| Cluster, SMR Category | Country | [SMR Q25, SMR Median, SMR Q75] | SMR Label | WoS Records | VOSviewer Keyword Annotations |
|---|---|---|---|---|---|
| C1, Low SMR N = 56 n = 2 | Mauritania | [5.4, 5.55, 5.825] | Low Hi. | 1 | Adolescent suicide, ingestion, deadly traffic injuries, maternal and child health, maternal mortality, non-communicable diseases, sustainable development, epidemic, pandemic strains, transcriptional activator. |
| Sao Tome and Principe | [2.2, 2.2, 2.225] | Low | 0 | ||
| Sudan | [4.975, 5.2, 5.325] | Low Hi. | 5 | ||
| C2, Medium SMR N = 34 n = 7 | Comoros | [8.6, 8.9, 9.15] | Medium | 0 | Depression, disorders, population, schizophrenia, Boko Haram, gender, health, terrorism, women, HIV/AIDS, stigma, suicidality, adolescents, homicide, Nigeria, psychiatric disorders. |
| Liberia | [8.15, 8.5, 8.625] | Medium | 2 | ||
| Mali | [8.575, 8.7, 8.725] | Medium | 4 | ||
| Mauritius | [7.75, 8.65, 9.65] | Medium | 0 | ||
| Nigeria | [7.525, 8.9, 9.2] | Medium | 52 | ||
| South Sudan | [6.575, 6.7, 7.125] | Medium Lo. | 0 | ||
| Seychelles | [7.5, 7.7, 8.5] | Low Hi. | 1 | ||
| C3, Medium high SMR N = 29 n = 7 | Gambia | [10.525, 10.95, 11.32] | Medium | 1 | Contemporary Ghana, nurses, prevention, self-harm, students, Uganda, children, community, mental health, adolescents, depression, gender differences, homicide, women, psychology students, stigma, South Africa, Tanzania. |
| Ghana | [11.225, 12.1, 12.825] | Medium | 53 | ||
| Guinea | [10.4, 12.05, 12.8] | Medium Hi. | 30 | ||
| Madagascar | [9.725, 10.2, 10.625] | Medium | 3 | ||
| Niger | [10.075, 10.15, 10.4] | Medium | 3 | ||
| Sierra Leone | [10.875, 11.1, 11.7] | Medium | 1 | ||
| Tanzania | [8.3, 10.05, 10.925] | Medium | 14 | ||
| C4, Very high SMR N = 1 | Eswatini | [45.92, 56.65, 66.075] | High | 0 | NA |
| C5, Very high SMR N = 1 | Lesotho | [47, 85.75, 97.725] | High | 0 | NA |
| C7, High SMR N = 5 | Botswana | [25.1, 31.65, 40.9] | High | 0 | NA |
| C8, Mixed medium and high SMR N = 36 n = 20 | Angola | [13.25, 14.2, 17.125] | High | 0 | Abuse, adolescents, care, community, gender, HIV/AIDS, Uganda, women, children, mental health, post-traumatic stress, trauma, war, deliberate self-harm, psychological autopsy, schizophrenia, Sub-Saharan Africa, anxiety, depression, health, Kenya, primary care, stress, validation. |
| Benin | [13.55, 14.1, 14.7] | High Lo. | 7 | ||
| Burkina Faso | [15.55, 15.8, 15.9] | High | 2 | ||
| Burundi | [13.025, 15.05, 18.05] | High | 0 | ||
| Cabo Verde | [16.85, 18.1, 18.225] | High | 0 | ||
| Cameroon | [17.7, 19.3, 19.625] | High | 9 | ||
| Chad | [14.45, 15.65, 15.8] | High Lo. | 2 | ||
| Congo | [13.25, 15.9, 17.625] | High | 10 | ||
| Dem. Rep. Congo | [12.55, 13.4, 14.125] | Medium Hi. | 1 | ||
| Equatorial Guinea | [14.05, 14.5, 15.35] | High | 0 | ||
| Ethiopia | [10. 13.4, 15.425] | Medium Hi. | 52 | ||
| Gabon | [14.45, 15.75, 16.375] | High | 0 | ||
| Guinea-Bissau | [13.85, 15.45, 15.75] | High Lo. | 1 | ||
| Kenya | [11.075, 12, 12.925] | Medium | 23 | ||
| Malawi | [12.75, 14.7, 15.75] | High Lo. | 12 | ||
| Rwanda | [10.05, 11.8, 15.3] | Medium Hi. | 6 | ||
| Senegal | [11.95, 12.4, 13.325] | Medium | 1 | ||
| Somalia | [15.15, 15.65, 16.525] | High | 7 | ||
| Togo | [17.15, 18.05, 18.625] | High | 3 | ||
| Uganda | [11.32, 15.05, 20.425] | High Lo. | 70 | ||
| C9, High SMR N = 12 n = 4 | Cote d’Ivoire | [18.3, 19.65, 20.675] | High | 0 | Adolescents, anxiety, care, criminalization, gay, heteronormativity, HIV, sexual and gender minorities, stigma, abuse, alcohol use, asylum applicants. |
| Eritrea | [18.85, 20.6, 20.975] | High | 1 | ||
| Namibia | [15.125, 18.2, 24.55] | High | 5 | ||
| Zambia | [17.6, 19.35, 21.875] | High | 0 | ||
| C10, High SMR N = 7 n = 4 | Central African Rep. | [26.525, 27.6, 28.2] | High | 1 | Alcohol use, homicide, women, care, depression, HIV/AIDS, stress, adolescents, gender, men, students, violence, youth, post-traumatic stress, suicide prevention. |
| Mozambique | [21.325, 23.15, 24.625] | High | 9 | ||
| South Africa | [25.25, 26.55, 27.6] | High | 232 | ||
| Zimbabwe | [21.87, 26.55, 31.475] | High | 21 |
| Cluster, SMR Category | Country | [SMR Q25, SMR Median, SMR Q75] | SMR Label | WoS Records | VOSviewer Keyword Annotations |
|---|---|---|---|---|---|
| C1, Low SMR N = 56 n = 16 | Algeria | [2.775, 3.1, 3.85] | Low | 11 | Adolescents, children, injuries, Iran, Israel, population, self-immolation, terrorism, women, Afghanistan, care, combat, deployment, mental health problems, military, military personnel, post-traumatic stress disorder, resilience, trauma, veterans, war, depression, mental health, social support. |
| Egypt | [3.575, 3.6, 3.7] | Low | 24 | ||
| Iran | [5.775, 6, 6.275] | Low | 259 | ||
| Iraq | [5.1, 5.2, 5.325] | Low | 397 | ||
| Israel | [5.1, 5.5, 6.15] | Low | 248 | ||
| Jordan | [1.9, 2.05, 2.85] | Low | 11 | ||
| Kuwait | [2.4, 2.65, 2.7] | Low | 12 | ||
| Lebanon | [2.875, 2.9, 3] | Low | 35 | ||
| Libya | [4.95, 5.35, 5.5] | Low | 6 | ||
| Malta | [4.9, 5.45, 6.025] | Low | 3 | ||
| Oman | [4.7, 6.05, 6.325] | Low | 4 | ||
| Qatar | [4.975, 6.25, 6.825] | Medium Lo. | 4 | ||
| Saudi Arabia | [4.075, 5.3, 5.925] | Low | 31 | ||
| Syria | [1.8, 1.85, 2] | Low | 18 | ||
| Tunisia | [3.175, 3.4, 3.725] | Low | 0 | ||
| United Arab Emir. | [5.525, 6.5, 6.8] | Medium Lo. | 7 | ||
| C2, Medium SMR N = 34 n = 3 | Bahrain | [6.65, 7.2, 8.75] | Medium | 3 | Terrorism, comorbidity, gender, schizophrenia, community, depression, liaison psychiatry, children, Morocco, poisoning, risk factors, violence. |
| Morocco | [7.825, 9.6, 10.125] | Medium | 24 | ||
| Yemen | [7.1, 7.5, 8.025] | Medium | 6 | ||
| C3, Medium high SMR N = 29 n = 1 | Djibouti | [11.07, 11.95, 12.1] | Medium Hi. | 0 | NA |
| Cluster, SMR Category | Country | [SMR Q25, SMR Median, SMR Q75] | SMR Label | WoS Records | Keyword Annotations |
|---|---|---|---|---|---|
| C1, Low SMR N = 56 n = 9 | Brunei Darussalam | [1.6, 1.8, 2.25] | Low | 1 | Adolescents, children, depressive symptoms, mental health, psychological distress, religion, youth, drug, gender, hopelessness, behavior, college students, self-harm, social support, depression, prevention, reliability, students, terrorism, validity. |
| Cambodia | [5.8, 6.35, 6.725] | Low Med. | 19 | ||
| Indonesia | [2.6, 2.95, 3.35] | Low | 32 | ||
| Malaysia | [5.275, 5.6, 5.8] | Low | 77 | ||
| Myanmar | [3.375, 3.85, 4.525] | Low | 7 | ||
| Papua New Guinea | [3.2, 3.3, 3.5] | Low | 6 | ||
| Philippines | [2.3, 2.55, 2.725] | Low | 28 | ||
| Timor Leste | [4.2, 4.4, 4.5] | Low | 0 | ||
| Tonga | [4.8, 5.05, 5.225] | Low | 2 | ||
| C2, Medium SMR N = 34 | Laos | [6.2, 6.9, 7.725] | Medium | 0 | Gender, mental disorders, population, predictors, prevention, risk factors, combat veteran, military, post-traumatic stress, trauma, veterans, violence, anxiety, children, depression, care, war. |
| North Korea | [9, 9.15, 9.25] | Medium | 15 | ||
| Singapore | [8.125, 9.1, 10.075] | Medium | 83 | ||
| Thailand | [7.275, 7.65, 8.85] | Medium | 52 | ||
| Vietnam | [7.075, 7.3, 7.5] | Medium | 145 | ||
| C3, Medium high SMR N = 29 | Australia | [10.075, 10.4, 11.3] | Medium | 1070 | Age, alcohol, women, adolescents, children, prevalence, self-harm, anxiety, care, community, depression, population, symptoms, China, mental disorders, psychological autopsy, schizophrenia, reliability, validity. |
| China | [7.325, 9.85, 12.575] | Medium | 896 | ||
| Fiji | [10, 10.2, 10.5] | Medium | 18 | ||
| New Zealand | [11.075, 11.95, 12.3] | Medium Hi. | 0 | ||
| C6, High SMR N = 2 | Kiribati | [31.575, 32.4, 32.925] | High | 3 | Risk, students, alcohol use initiation, cannabis, cigarette smoking, early substance use, epidemic suicide. |
| C8, Mixed medium and high SMR N = 36 | Japan | [15.575, 18, 18.8] | High | 770 | Age, gender, unemployment, depression, health, internet, population, social support, care, community, education, elderly, self-harm, euthanasia, people, schizophrenia. |
| Samoa | [14.8, 14.9, 15.3] | High | 10 | ||
| Solomon Islands | [17.35, 17.8, 18.25]. | High | 3 | ||
| C9, High SMR N = 12 | Mongolia | [19.775, 22.55, 23.45] | High | 5 | Risk, students, alcohol, cannabis, loneliness, substance use, anxiety disorders, depression. |
| Vanuatu | [21.175, 21.85, 22.275] | High | 4 | ||
| C10, High SMR N = 7 | Micronesia | [27, 27.4, 28.05] | High | 6 | Adolescents, children, depression, youth, age, economic crisis, gender, inequalities, unemployment, mental disorders, predictors. |
| South Korea | [20.725, 22.35, 24] | High | 360 |
| Cluster, SMR Category | Country | [SMR Q25, SMR Median, SMR Q75] | SMR Label | WoS Records | VOSviewer Keyword Annotations |
|---|---|---|---|---|---|
| C1, Low SMR N = 56 n = 3 | Bangladesh | [3.8, 4.95, 5.6] | Low | 52 | Asia, children, injury, verbal autopsy, violence, women, assault, domestic violence, intimate partner violence, pregnancy, anxiety, depression, demography, prevention, risk factors. |
| Bhutan | [5.2, 5.3, 6.025] | Low Hi. | 3 | ||
| Maldives | [2.9, 3.25, 3.8] | Low | 0 | ||
| C2, Medium SMR N = 34 n = 1 | Afghanistan | [6, 6.75, 7.625] | Medium Lo. | 303 | Afghanistan war veterans, depression, PTSD, symptoms, US veterans, active duty, combat, deployment, mental health, military, resilience, soldiers, traumatic brain injury, terrorism, war, trauma, veterans. |
| C3, Medium high SMR N = 29 n = 2 | Nepal | [9.8, 10, 10.425] | Medium | 41 | Attitudes, deliberate self-harm, poisoning, suicide bombing, terrorism, violence, mental health, stigma, women, anxiety, depression, medical students, stress, abuse, health, gender, low income, risk factors. |
| Pakistan | [10, 10.25, 11.025] | Medium | 111 | ||
| C8, Mixed medium and high SMR N = 36 n = 1 | India | [13.35, 15.6, 17.025] | High Lo. | 570 | Agriculture, autopsy, Kaniyambadi block, pesticides, poisoning, rural India, adolescents, children, mental health, poverty, self-harm, violence, care, depression, domestic violence, gender, risk factors, schizophrenia, women. |
| C9, High SMR N = 12 n = 1 | Sri Lanka | [14.575, 18.1, 21.95] | High | 190 | Asia, depression, women, developing world, pesticide poisoning, health, impact, ingestion, rural Sri Lanka, deliberate self-harm, pesticide, suicide prevention. |
| Cluster, SMR Category | Country | [SMR Q25, SMR Median, SMR Q75] | SMR Label | WoS Records | VOSviewer Keyword Annotations |
|---|---|---|---|---|---|
| C1, Low SMR N = 56 n = 16 | Antigua and Barbu. | [ 0.175, 0.35, 1.3] | Low | 0 | Alcohol, homicide, violence, women, care, mental disorders, population, prevention, abuse, adolescents, children, students, substance use, youth, anxiety, bipolar disorder, depression, prevalence. |
| Bahamas | [3.2, 3.35, 3.42] | Low | 1 | ||
| Barbados | [0.3, 0.65, 1.225] | Low | 1 | ||
| Brazil | [4.9, 5.2, 5.45] | Low | 300 | ||
| Colombia | [3.875, 4.25, 4.55] | Low | 54 | ||
| Dominican Republic | [5.3, 5.5, 5.85] | Low | 4 | ||
| Grenada | [0.6, 1.35, 2.225] | Low | 0 | ||
| Honduras | [2.7, 3, 3] | Low | 3 | ||
| Jamaica | [1.975, 2.1, 2.2] | Low | 21 | ||
| Mexico | [4.3, 4.75, 5.4] | Low | 282 | ||
| Nicaragua | [4.975, 5.45, 5.95] | Low Med. | 11 | ||
| Panama | [3.475, 4.7, 5.9] | Low | 1 | ||
| Paraguay | [3.875, 4.65, 5.675] | Low | 2 | ||
| Peru | [2.8, 3.05, 3.225] | Low | 21 | ||
| St. Vincent and the Grenadines | [2.375, 4.8, 6.25] | Low | 1 | ||
| Venezuela | [2.375, 3.65, 4.875] | Low | 12 | ||
| C2, Medium SMR N = 34 n = 7 | Argentina | [8.4, 8.55, 9.05] | Medium | 30 | Behavior, bipolar disorder, depression, HIV, lithium, psychopathology, women, adolescents, aggression, gender, mental health, firearms, homicide, violence, health, impact. |
| Belize | [6.9, 7.45, 8.125] | Medium | 0 | ||
| Bolivia | [7, 7.15, 7.425] | Medium | 4 | ||
| Costa Rica | [5.75, 6.7, 7.3] | Medium | 6 | ||
| Ecuador | [8.775, 9.35, 10.3] | Medium | 12 | ||
| El Salvador | [6.175, 6.9, 7.325] | Medium | 8 | ||
| St. Lucia | [7.1, 7.5, 7.9] | Medium | 1 | ||
| C3, Medium high SMR N = 29 n = 5 | Chile | [9.2, 9.7, 10.525] | Medium | 74 | Adolescents, behavior, care, health, age, mental health, euthanasia, life, mental health, depression, mental disorders, psychiatric disorders, women, children, predictors, violence. |
| Cuba | [10.35, 10.65, 11.55] | Medium | 23 | ||
| Guatemala | [6.4, 9.1, 13.55] | Medium Wi. | 4 | ||
| Haiti | [11.925, 12.05, 12.525] | Medium Hi. | 4 | ||
| Trinidad and Tob. | [9.2, 10.45, 12.65] | Medium | 8 | ||
| C6, High SMR N = 2 n = 1 | Guyana | [35.75, 37.85, 39.825] | High | 18 | Adolescents, depression, forensic science, Guyana, Johnstown. |
| C8, Mixed medium and high SMR N = 36 n = 1 | Uruguay | [13.875, 14.75, 17] | High | 10 | Aggression, alcohol drinking, bullying, childhood, middle school students, school health, substance use, criminal law, assisted suicide, cocaine base post, elderly, human rights, depression, intimate partner violence. |
| C10, High SMR N = 7 n = 1 | Suriname | [25.9, 26.55, 27.075] | High | 4 | Teenagers, youth suicide, pesticides, Hindustan culture, psychological autopsy, economic policy, indigenous health, global health governance, mercury exposure. |
| Cluster, SMR Category | Country | [SMR Q25, SMR Median, SMR Q75] | SMR Label | WoS Records | Keyword Annotations |
|---|---|---|---|---|---|
| C3, Medium high SMR N = 29 n = 2 | United States | [10.775, 11.55, 12.525] | Medium | 730 | Alcohol, depression, mental disorders, population, substance use, adolescent suicide, firearms, gender, health, homicide, prevention, rates, violence, women, attitudes, Canada, care, euthanasia, life, children, stress, youth. |
| Canada | [10.175, 10.35, 10.75] | Medium | 3563 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pranckeviciene, E.; Kasperiuniene, J. Global Suicide Mortality Rates (2000–2019): Clustering, Themes, and Causes Analyzed through Machine Learning and Bibliographic Data. Int. J. Environ. Res. Public Health 2024, 21, 1202. https://doi.org/10.3390/ijerph21091202
Pranckeviciene E, Kasperiuniene J. Global Suicide Mortality Rates (2000–2019): Clustering, Themes, and Causes Analyzed through Machine Learning and Bibliographic Data. International Journal of Environmental Research and Public Health. 2024; 21(9):1202. https://doi.org/10.3390/ijerph21091202
Chicago/Turabian StylePranckeviciene, Erinija, and Judita Kasperiuniene. 2024. "Global Suicide Mortality Rates (2000–2019): Clustering, Themes, and Causes Analyzed through Machine Learning and Bibliographic Data" International Journal of Environmental Research and Public Health 21, no. 9: 1202. https://doi.org/10.3390/ijerph21091202
APA StylePranckeviciene, E., & Kasperiuniene, J. (2024). Global Suicide Mortality Rates (2000–2019): Clustering, Themes, and Causes Analyzed through Machine Learning and Bibliographic Data. International Journal of Environmental Research and Public Health, 21(9), 1202. https://doi.org/10.3390/ijerph21091202