

The Prevalence of Caregiving among Young People



Abstract
1. Introduction
2. Methods
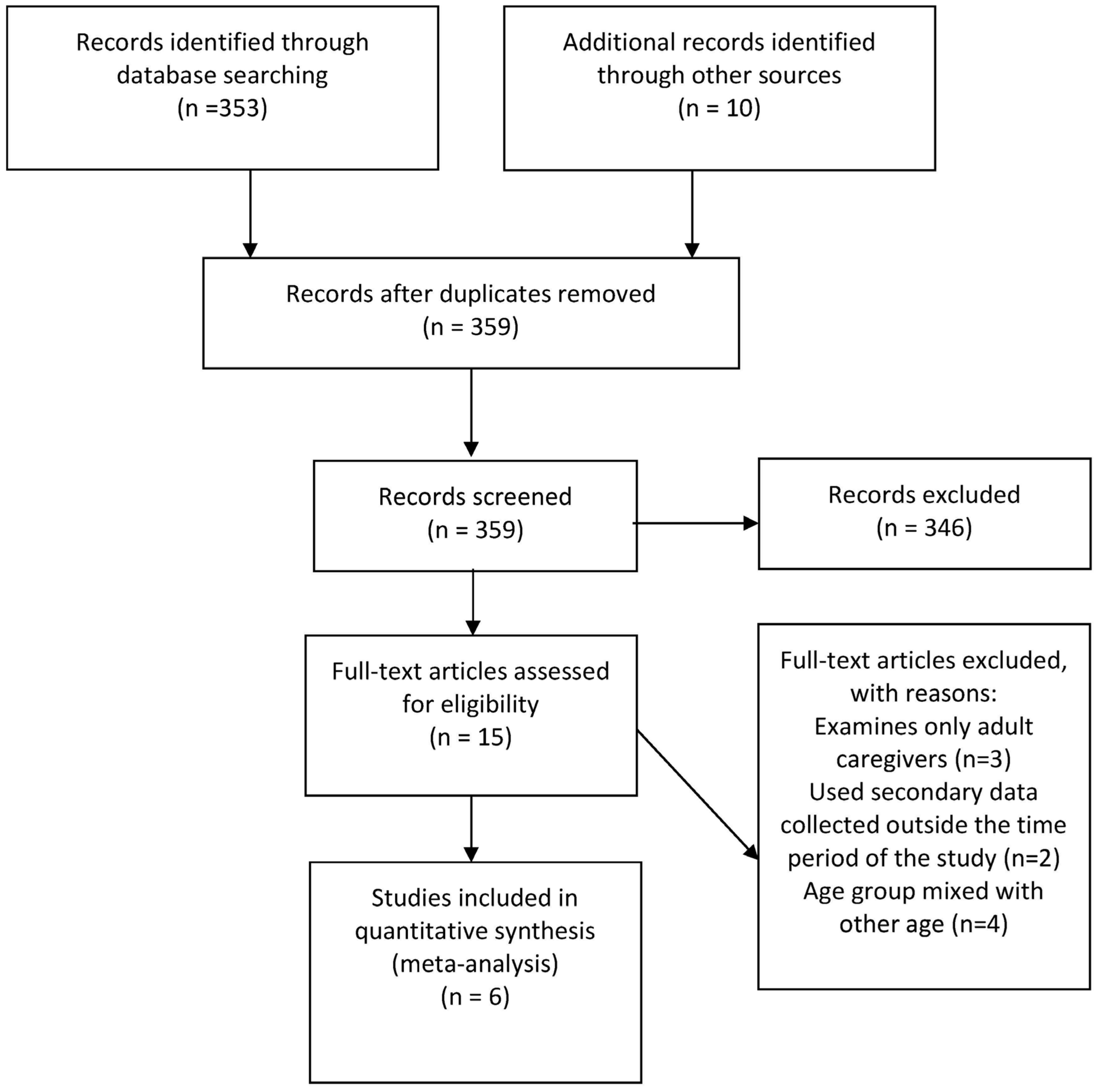
2.1. Search Strategies
2.2. Selection of Articles
2.3. Assessment of the Study Quality
2.4. Information Extraction and Analysis
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2015, 388, 1545–1602. [Google Scholar] [CrossRef] [PubMed]
- Andrews, G.; Faulkner, D.; Andrews, M.; Cai, J. A Glossary of Terms for Community Health Care and Services for Older Persons; World Health Organization: Kobe, Japan, 2004. [Google Scholar]
- Smyth, C.; Hamilton, M. Young carers. In The Encyclopedia of Child and Adolescent Development; John Wiley & Sons, Inc.: New York, NY, USA, 2020. [Google Scholar] [CrossRef]
- Gilhooly, K.J.; Gilhooly, M.L.; Sullivan, M.P.; McIntyre, A.; Wilson, L.; Harding, E.; Woodbridge, R.; Crutch, S. A meta-review of stress, coping and interventions in dementia and dementia caregiving. BMC Geriatr. 2016, 16, 106. [Google Scholar] [CrossRef]
- Fick, D.M.; Resnick, B. 2012 Beers criteria update: How should practising nurses use the criteria? J. Gerontol. Nurs. 2012, 38, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Schulz, H.; Auer, S.; Span, E.; Adler, C.; Donabauer, Y.; Weber, S.; Wimmer-Elias, J.; Meyer, M. [A training program for dementia trainers: Does this program have practical relevance?]. Z. Fur Gerontol. Und Geriatr. 2012, 45, 637–641. [Google Scholar] [CrossRef] [PubMed]
- Vitaliano, P.P.; Murphy, M.; Young, H.M.; Echeverria, D.; Borson, S. Does caring for a spouse with dementia promote cognitive decline? A hypothesis and proposed mechanisms. J. Am. Geriatr. Soc. 2011, 59, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.W.; Zebrack, B. Caring for family members with chronic physical illness: A critical review of caregiver literature. Health Qual. Life Outcomes 2004, 2, 50. [Google Scholar] [CrossRef]
- Moore, M.J.; Zhu, C.W.; Clipp, E.C. Informal costs of dementia care: Estimates from the National Longitudinal Caregiver Study. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2001, 56, S219–S228. [Google Scholar] [CrossRef]
- Chen, M.-L. The growing costs and burden of family caregiving of older adults: A review of paid sick leave and family leave policies. Gerontologist 2014, 56, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; O’Brien, A.T.; Bookwala, J.; Fleissner, K. Psychiatric and Physical Morbidity Effects of Dementia Caregiving: Prevalence, Correlates, and Causes. Gerontologist 1995, 35, 771–791. [Google Scholar] [CrossRef]
- Dassel, K.B.; Carr, D.C. Does dementia caregiving accelerate frailty? Findings from the Health and Retirement Study. Gerontologist 2016, 56, 444–450. [Google Scholar] [CrossRef]
- Vitaliano, P.P.; Zhang, J.; Scanlan, J.M. Is caregiving hazardous to one’s physical health? A meta-analysis. Psychol. Bull. 2003, 129, 946. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, S.T.; Moyle, W.; Zimmer-Gembeck, M.; De Leo, D. Suicidal ideation in family caregivers of people with dementia. Aging Ment. Health 2016, 20, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Sörensen, S. Differences between caregivers and non-caregivers in psychological health and physical health: A meta-analysis. Psychol. Aging 2003, 18, 250. [Google Scholar] [CrossRef] [PubMed]
- Burton, L. Childhood adultification in economically disadvantaged families: A conceptual model. Fam. Relat. 2007, 56, 329–345. [Google Scholar] [CrossRef]
- Kuperminc, G.P.; Jurkovic, G.J.; Casey, S. Relation of filial responsibility to the personal and social adjustment of Latino adolescents from immigrant families. J. Fam. Psychol. 2009, 23, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Becker, S. Global perspectives on children’s unpaid caregiving in the family: Research and policy on ‘young caregivers’ in the UK, Australia, the USA and Sub-Saharan Africa. Glob. Soc. Policy 2007, 7, 23–50. [Google Scholar] [CrossRef]
- Doran, T.; Drever, F.; Whitehead, M. Health of young and elderly informal caregivers: Analysis of UK census data. BMJ Br. Med. J. 2003, 327, 1388. [Google Scholar] [CrossRef] [PubMed]
- Ireland, M.J.; Pakenham, K.I. The nature of youth care tasks in families experiencing chronic illness/disability: Development of the Youth Activities of Caregiving Scale (YACS). Psychol. Health 2010, 25, 713–731. [Google Scholar] [CrossRef]
- Ryan, A.; Fox, A. Working with Young Caregivers in the United Kingdom; Princess Royal Trust for Caregivers: London, UK, 2003. [Google Scholar]
- Siskowski, C. Young Caregivers: Effect of Family Health Situations on School Performance. J. Sch. Nurs. 2006, 22, 163–169. [Google Scholar] [CrossRef]
- Dearden, C.; Becker, S. Young Caregivers in the UK. The 2004 Report; Loughborough University: London, UK, 2004. [Google Scholar]
- Young, H.; Grundy, E.; Jitlal, M. Care Providers, Care Receivers. A Longitudinal Perspective York; Joseph Rowntree Foundation: York, UK, 2006. [Google Scholar]
- Becker, S.; Aldridge, J.; Dearden, C. Young Caregivers and Their Families; Blackwell Science: Oxford, UK, 1998. [Google Scholar]
- National Alliance of Caregiving. Young Caregivers in the US: Findings from a National Survey; National Alliance of Caregiving: Bethesda, MD, USA, 2005. [Google Scholar]
- Lackey, N.R.; Gates, M.F. Adults’ recollections of their experiences as young caregivers of family members with chronic physical illnesses. J. Adv. Nurs. 2001, 34, 320–328. [Google Scholar] [CrossRef]
- Becker, F.; Becker, S. Young Adult Caregivers in the UK: Experiences, Needs and Services for Caregivers Aged 16–24; Princess Royal Trust for Caregivers: London, UK, 2008. [Google Scholar]
- Aldridge, J. Where are we now? Twenty-five years of research, policy and practice on young carers. Crit. Soc. Policy 2018, 38, 155–165. [Google Scholar] [CrossRef]
- Becker, S. Young carers. In The Blackwell Encyclopaedia of Social Work; Davies, M., Ed.; Blackwell: Oxford, UK, 2000; p. 378. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia. 2023. Available online: www.covidence.org (accessed on 1 March 2024).
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, SA, Australia, 2020. [Google Scholar]
- Cass, B.; Brennan, D.; Thomson, C.; Hill, T.; Purcal, C.; Hamilton, M.; Adamson, E. Young Caregivers: Social Policy Impacts of the Caring Responsibilities of Children and Young Adults; University of New South Wales: Sydney, NSW, Australia, 2011. [Google Scholar]
- Hunt, G.; Reinhard, S. The National Alliance for Caregiving (NAC) Caregiving in the U.S.; NAC and AARP Public Policy Institute Washington, DC, USA, 2015.
- Hunt, G.; Levine, C.; Naiditch, L. Young Caregivers in the US Report of Findings; National Alliance of Caregivers in collaboration with United Hospital Fund: Washington, DC, USA, 2009. [Google Scholar]
- Cohen, D.; Greene, J.A.; Toyinbo, P.A.; Siskowski, C.T. Impact of Family Caregiving by Youth on Their Psychological Well-Being: A Latent Trait Analysis. J. Behav. Health Serv. Res. 2012, 39, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Disability, Ageing and Caregivers, Australia: First Results, 2015; Australian Bureau of Statistics: Canberra, ACT, Australia, 2015.
- Central Statistics Office Ireland. Our Bill of Health; Central Statistics Office Ireland: Cork, Ireland, 2012.
- Nagl-Cupal, M.P.R.N.; Daniel, M.M.A.P.; Koller, M.M.M.A.; Mayer, H.P.R.N. Prevalence and effects of caregiving on children. J. Adv. Nurs. 2014, 70, 2314. [Google Scholar] [CrossRef] [PubMed]
- Statistics New Zealand. 2013 Census Information by Variable: Unpaid Activities; Statistics New Zealand: Auckland, New Zealand, 2013.
- Hill, T.; Smyth, C.; Thomson, C.; Cass, B. Young Caregivers: Their Characteristics and Geographical Distribution; Social Policy Research Centre: Canberra, ACT, Australia, 2009. [Google Scholar]
- Carers Australia. Available online: http://www.carersaustralia.com.au/about-carers/young-carers2/ (accessed on 1 April 2024).
- Leu, A.; Frech, M.; Wepf, H.; Sempik, J.; Joseph, S.; Helbling, L.; Moser, U.; Becker, S.; Jung, C. Counting young carers in Switzerland—A study of prevalence. University of Sussex. J. Contrib. 2019, 33, 53–67. [Google Scholar]
- Lloyd, K. Happiness and well-being of young carers: Extent, nature and correlates of caring among 10 and 11 year old school children. J. Happiness Stud. 2013, 14, 67–80. [Google Scholar] [CrossRef]
- Metzing, S.; Ostermann, T.; Robens, S.; Galatsch, M. The prevalence of young carers—A standardised survey amongst school students (KiFam-study). Scand. J. Caring Sci. 2020, 34, 501–513. [Google Scholar] [CrossRef]
- Stamatopoulos, V. One million and counting: The hidden army of young carers in Canada. J. Youth Stud. 2015, 18, 809–822. [Google Scholar] [CrossRef]

{kind=link}
| Author, Year, Place | Age Groups Included | Type of Report | Information Source/Study Methods | Population Size | Results | Comments |
|---|---|---|---|---|---|---|
| Cohen et al., 2012, USA [37] | 10–14 years | Journal article | Information was obtained from a cross-sectional survey administered to 1281 students from two schools in Florida. Students responded to questions asking whether they lived with the person who required care from the respondent and the type of assistance provided by the caregiver. | N = 1281 of a sample obtained from schools | 459 (35.8%) reported as a caregiver, with 249 (19.4%) boys and 210 (16.4%) girls. Information on the extent, type, and duration of caregiving was not available. | Only two schools that did not constitute a representative sample were included in the study. This was a purposive sample targeting schools with a high prevalence of young caregivers. This constitutes selection bias. |
| Central Statistics Office, 2012, Ireland [39] | All ages, including 0–17 years | Government report on national census data | Census data based on standard data collection procedures. | N = 653,219, with 370,200 aged 14 years or younger and 283,019 aged between 15 and 19 years. | In total, 8472 (1.3%) young caregivers were identified among 4228 (1.1%) children and young adolescents aged <15 years, as well as 4244 (1.5%) of young caregivers aged 15–19 years. Information on the extent, the types, and the duration of caregiving was unavailable. | Population data with direct calculation of the prevalence |
| Nagl-Cupal et al., 2014, Austria [40] | 10–14 years | Journal article | Data were collected from a cross-sectional survey of 85 schools and 474 classes, 4 school grades between 5th and 8th grade from 2 populous provinces in Austria. Multilevel probability samples based on the proportions of school types in each area were generated. A young caregiver was defined as one who provided care for patients with long-term illness or disability. | In total, 7403 responded to the survey with useful information. | 335 (4.5%) young caregivers identified with 234 girls and 101 boys. For the extent of caregiving, 81% of them helped their mother ‘often’ or ‘very often’; 63% and 60% reported helping a sibling and their father. No information on the duration was available. | A well-designed study with a random and representative sample. The only drawback was a low response rate of 47.2%. |
| Australian Bureau of Statistics, 2015, Australia [38] | All ages, including 0–19 years; the age groups were categorised as <15 years and 15–24 years | Government report on national survey data | A survey of disabilities and chronic diseases was conducted using a multistage sampling technique. Information on caring status was elicited through questions on care provision. | 25,555 responded to the survey with useful information on caregiving. However, there was no information on the number of respondents broken down by age group. | 1.3% of young people aged <15 years were primary caregivers. Information on the extent, type, and duration of caregiving was not available. | The survey achieved a high response rate of 80% with little selection biases. However, due to the lack of information on the number of respondents by age group, further calculation on the prevalence was difficult. |
| Llyod, 2013, Northern Ireland [45] | 10 and 11 years | Journal article | Information was collected through an online survey of 292 primary schools, representing 32% of the total 899 primary schools in Northern Ireland. Caregiving was identified as a positive answer to a question asking whether the child helped looking after someone in the family. | A total of 4192 children participated in the survey, representing 50% of the participating schools. | 12% of the respondents reported having provided care to someone living with them. The types of care provided were mostly physical personal care, such as getting out of bed, walking, and dressing. No information on the duration of caregiving was reported. | A study with a large sample. However, it was not certain whether the sample was generated randomly. According to the description in the Methods, it was unlikely a random sample. |
| Leu et al., 2019, Switzerland [44] | 10–15 years | Journal article | Data were collected from a cross-sectional survey conducted in 230 schools in Switzerland using a 2-stage stratified sampling approach. The caregiving status was assessed using them Multidimensional Assessment of Caring Activities (MACA-YC18). | A total of 3991 students responded and provided useful data. | 7.9% (95%C.I. 6.7–9.3%) of children responded positively to the question on caring for a family member. In terms of the extent of caregiving, 17% and 22% reported providing very high and high amounts of caring, respectively; 32% and 30% provided a moderate and low amount of care. This involved emotional, financial, and personal care. There was quantifiable information on the duration of caregiving. | A high response rate of 97.8% was achieved with reasonably little selection bias. The prevalence estimated was also weighed to adjust for the sampling effect. |
| Study | Prevalence (95%C.I.) | |
|---|---|---|
| <15 Years | 10–15 Years | |
| Central Statistics Office Ireland [39] | 1.1% (1.06–1.14%) | - |
| Llyod [45] | 12.0% (11.02–12.98%) | - |
| Nagl-Cupal et al. [40] | 4.5% (4.03–4.97%) | - |
| Australian Bureau of Statistics [38] | 1.3% (1.16–1.44%) | - |
| Leu et al. [44] | - | 7.9% (6.7–9.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lam, L.T.; Lam, M.K. The Prevalence of Caregiving among Young People. Int. J. Environ. Res. Public Health 2024, 21, 621. https://doi.org/10.3390/ijerph21050621
Lam LT, Lam MK. The Prevalence of Caregiving among Young People. International Journal of Environmental Research and Public Health. 2024; 21(5):621. https://doi.org/10.3390/ijerph21050621
Chicago/Turabian StyleLam, Lawrence T., and Mary K. Lam. 2024. "The Prevalence of Caregiving among Young People" International Journal of Environmental Research and Public Health 21, no. 5: 621. https://doi.org/10.3390/ijerph21050621
APA StyleLam, L. T., & Lam, M. K. (2024). The Prevalence of Caregiving among Young People. International Journal of Environmental Research and Public Health, 21(5), 621. https://doi.org/10.3390/ijerph21050621