Sexually Transmitted Infections in Adolescents and Young Adults: A Cross Section of Public Health


 ,
,  and
and
Abstract
1. Introduction
- Unprotected and condomless sex with promiscuity (increased number of relationships);
- Cultural reticence about speaking of sexual topics [10];
- Inadequate funding for prevention efforts, diagnostic tests, and existing treatments and for the development of new tests and treatment;
- Predisposition to re-infection when both partners are not treated contemporaneously;
- Incomplete treatment, which can lead the microorganisms to develop drug resistance;
- International travel, which facilitates rapid global spread of STIs.
- time passed since first sexual intercourse;
- sexual activity in early and mid-adolescence;
- multiple partners, new partners, or partners who have several other partners;
- inconsistent use of condoms, especially with regular partners;
- alcohol and drug use;
- rectal douching or enemas in preparation for receptive anal sex.
2. Materials and Methods
2.1. The Setting
2.2. Study Design
STI Panel Collection
2.3. Laboratory Method
2.4. Ethics Approval and Privacy Aspects
3. Results
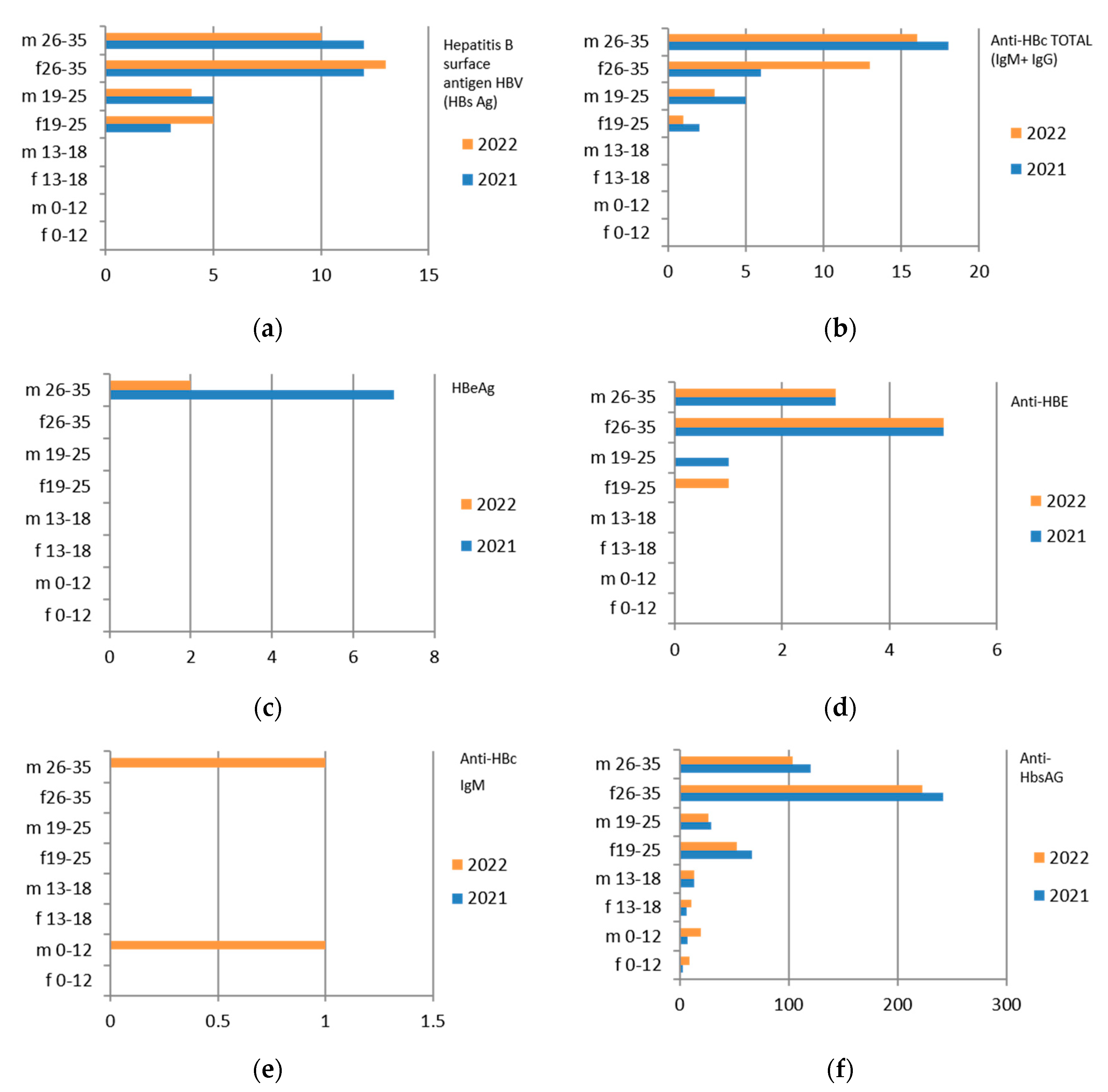
3.1. Hepatitis B
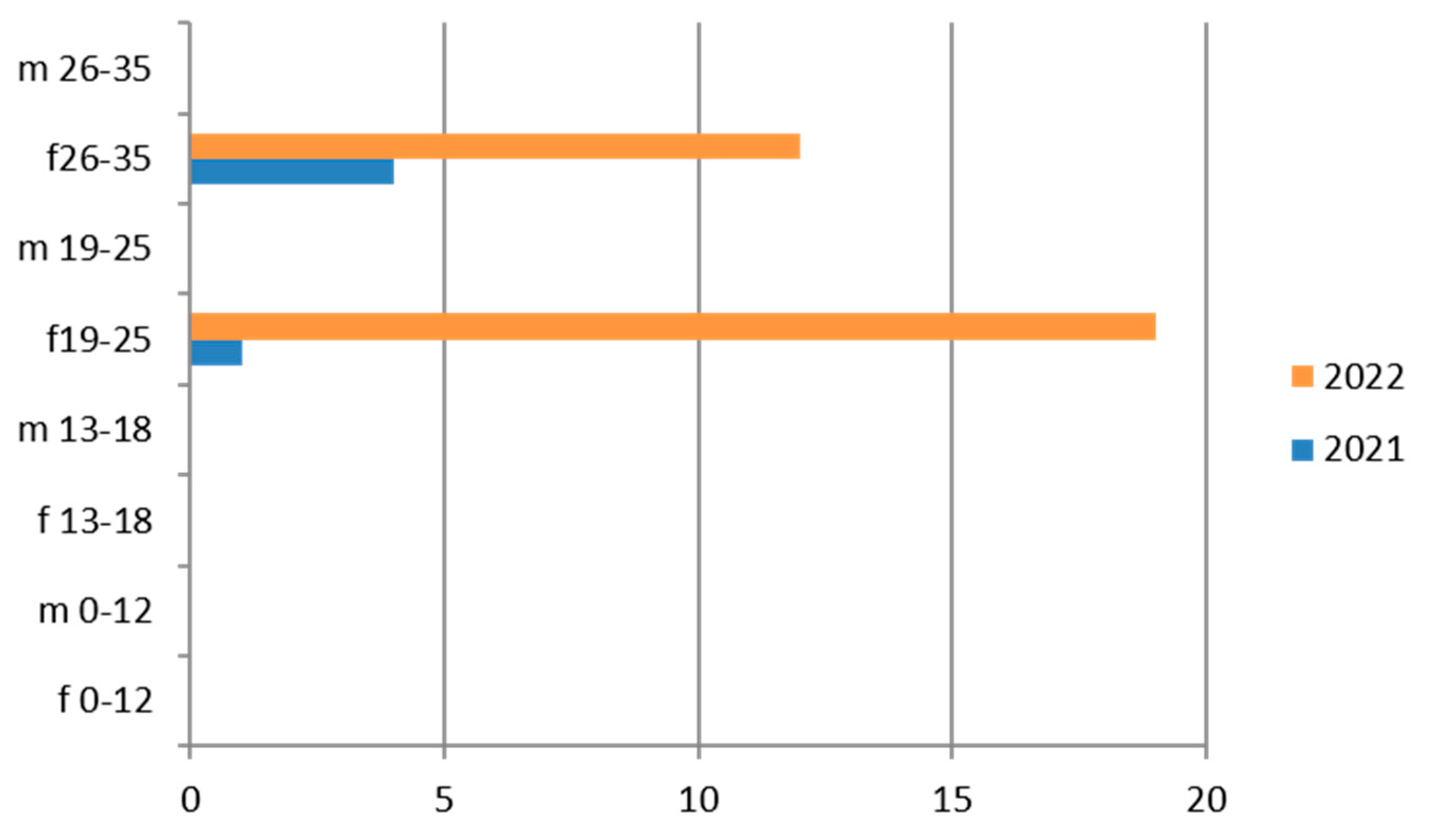
3.2. Hepatitis C
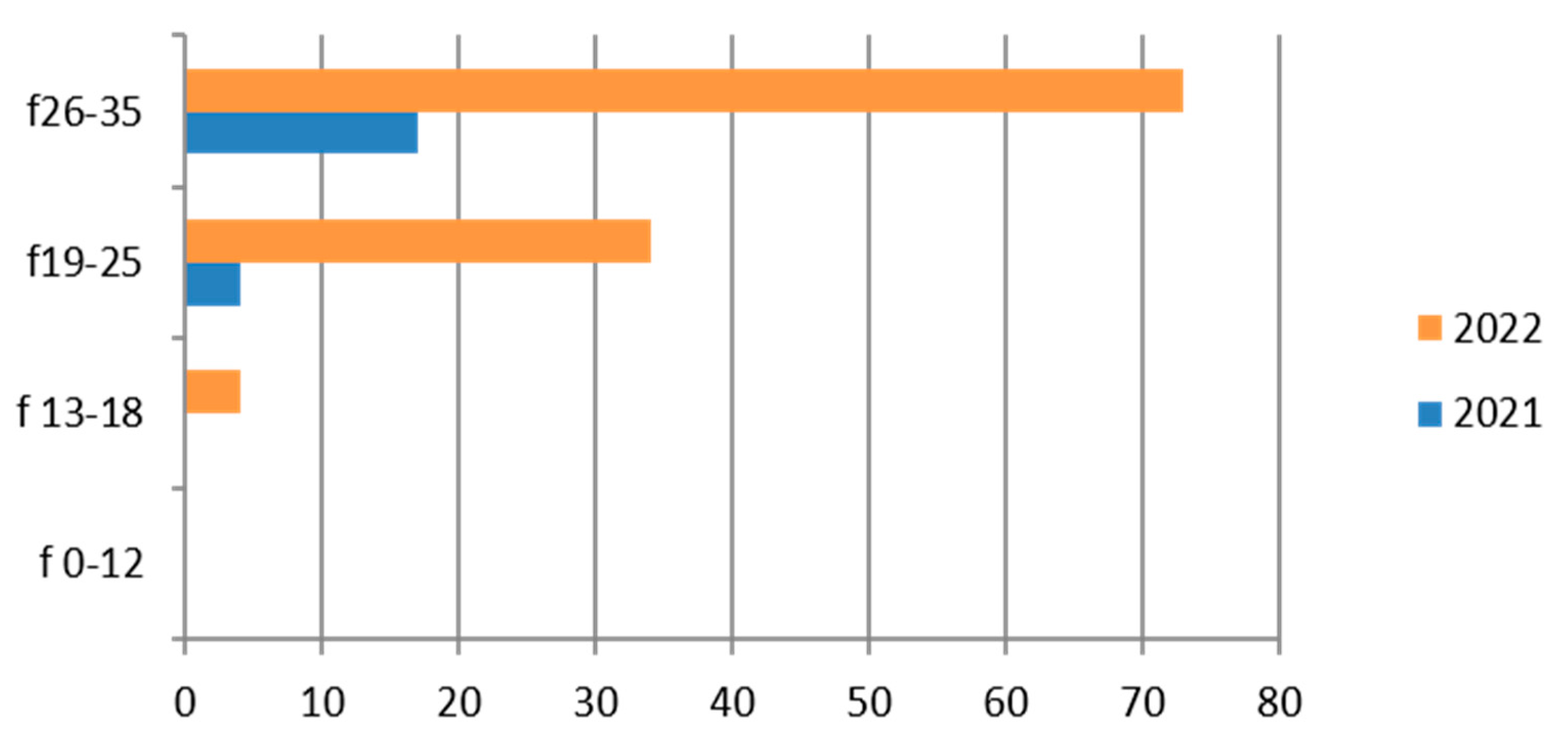
3.3. Chlamydia trachomatis
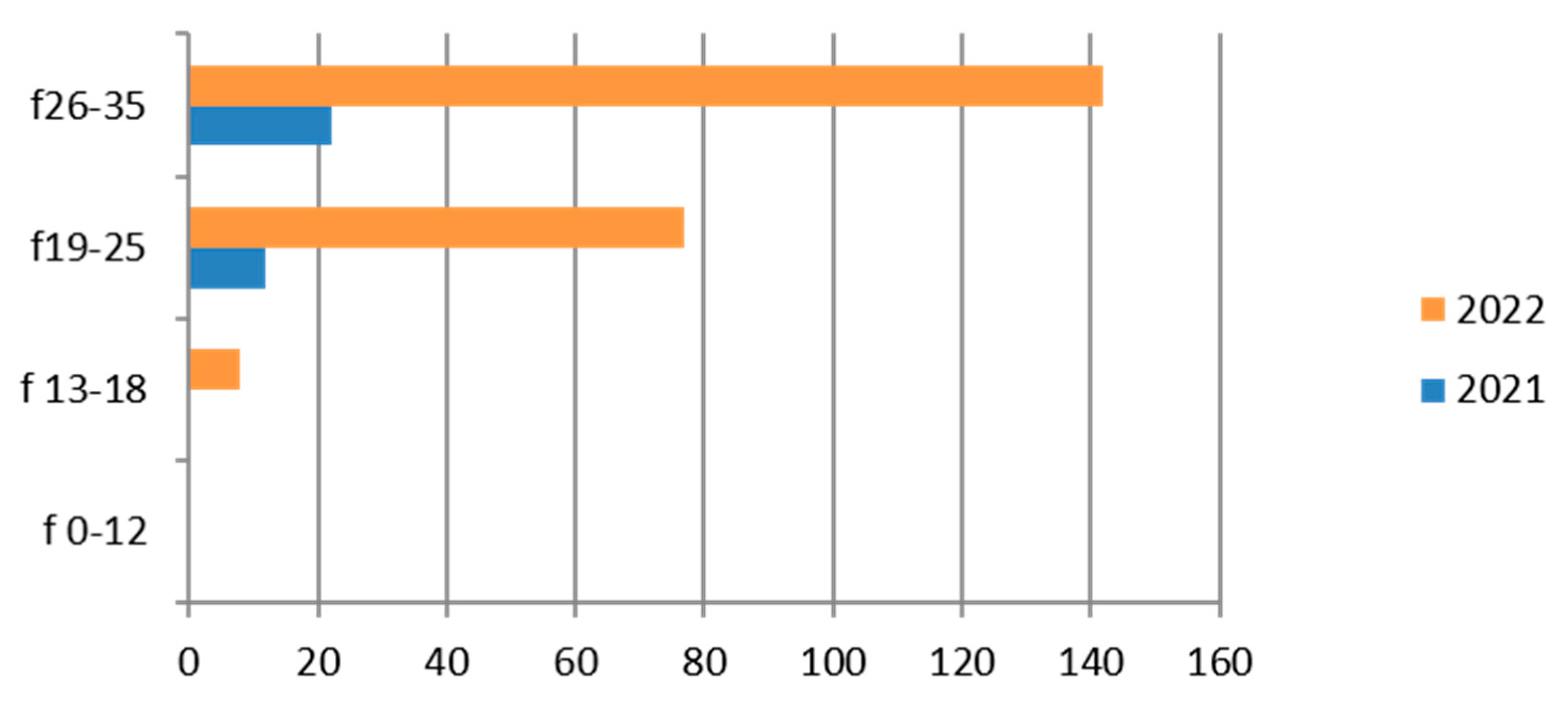
3.4. Gardnerella vaginalis
3.5. HPV
3.6. Mycoplasma/Ureaplasma
3.7. Neisseria gonorrhoeae
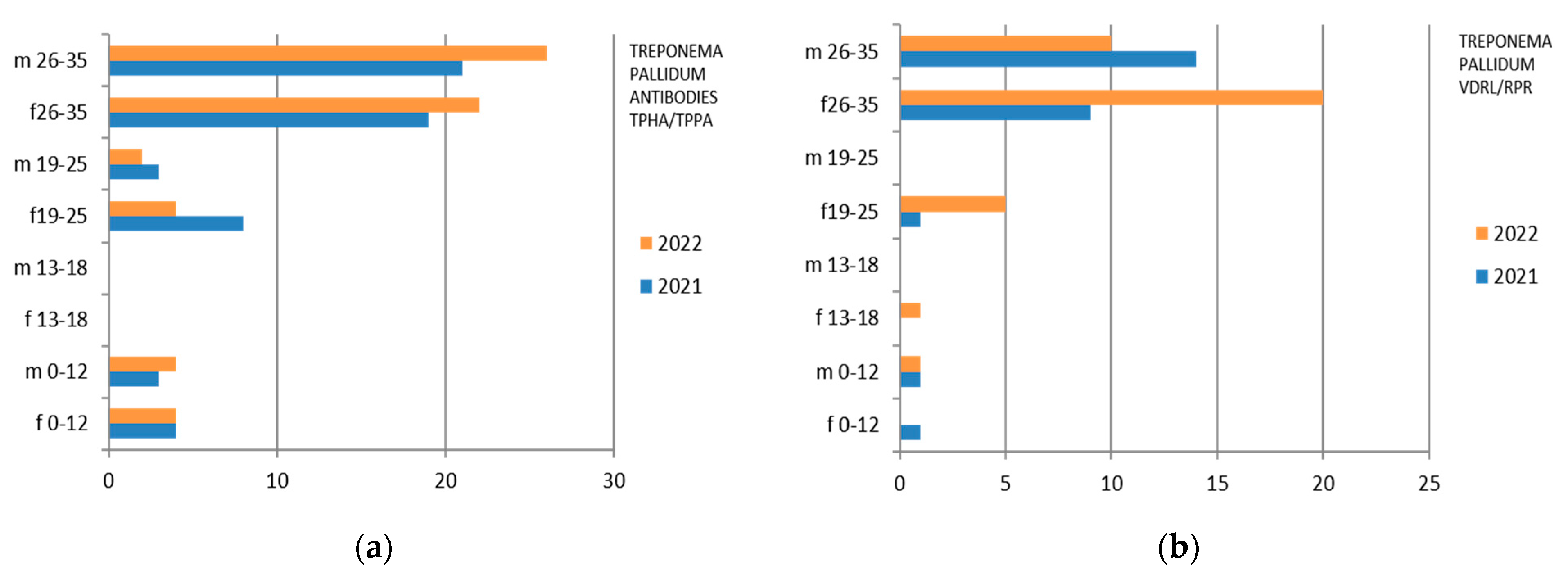
3.8. Treponema pallidum
3.9. Virus HIV 1–2
4. Discussion
4.1. Summary of Findings
4.2. Comparison with Other Studies
4.3. Interpretation of the Findings
- (a)
- Consideration about age and sex
- (b)
- Consideration about geographical areas
- (c)
- Consideration about test results
- (d)
- Implications of the findings
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rowley, J.; Vander Hoorn, S.; Korenromp, E.; Low, N.; Unemo, M.; Abu-Raddad, L.J.; Chico, R.M.; Smolak, A.; Newman, L.; Gottlieb, S.; et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: Global prevalence and incidence estimates. Bull. World Health Organ. 2019, 97, 548–562. [Google Scholar] [CrossRef]
- Benson, P.A.S. Patient Education: Adolescent Sexuality (Beyond the Basics). 2023. Available online: https://www.uptodate.com/contents/adolescent-sexuality-beyond-the-basics?csi=38bd0dd3-e759-41e5-b929-5613c3791a9d&source=contentShare (accessed on 5 January 2023).
- World Health Organization. Global Health Sector Strategy on Sexually Transmitted Infections 2016–2021. 2016. Available online: http://apps.who.int/iris/bitstream/10665/246296/1/WHO-RHR-16.09-eng.pdf?ua=1 (accessed on 5 June 2023).
- European Centre for Disease Prevention and Control—Sexually Transmitted Infections. Available online: https://www.ecdc.europa.eu/en/sexually-transmitted-infections (accessed on 5 June 2023).
- Torrone, E.; Papp, J.; Weinstock, H.; Centers for Disease Control and Prevention (CDC). Prevalence of Chlamydia trachomatis genital infection among persons aged 14–39 years–United States, 2007–2012. Morb. Mortal. Wkly. Rep. 2014, 63, 834–838. [Google Scholar]
- World Health Organitation. Guidelines for the Management of Symptomatic Sexually Transmitted Infections; WHO: Geneva, Switzerland, 2021; ISBN 978-92-4-002416-8. Available online: https://www.who.int/publications/i/item/9789240024168 (accessed on 5 June 2023).
- Istituto Superiore di Sanità. Infezioni Sessualmente Trasmesse—20/7/2023—I Nuovi Dati Sulle IST in Italia. Available online: https://www.epicentro.iss.it/ist/aggiornamenti (accessed on 5 August 2023).
- Dal Conte, I.; Lucchini, A.; Contuzzi, E.; Di Perri, G.; Bingham, J. Sexually transmitted infections in Italy: An overview. Int. J. STD AIDS 2001, 12, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.S.R. Panoramica Sulle Infezioni a Trasmissione Sessuale; University of California San Diego: La Jolla, CA, USA, 2023; Available online: https://www.msdmanuals.com/it-it/professionale/malattie-infettive/malattie-a-trasmissione-sessuale-mts/panoramica-sulle-malattie-a-trasmissione-sessuale (accessed on 5 June 2023).
- Gilbert, A.L.; Rickert, V.I.; Aalsma, M.C. Clinical conversations about health: The impact of confidentiality in preventive adolescent care. J. Adolesc. Health 2014, 55, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Bechtel, M.A.; Trout, W. Sexually transmitted diseases. Clin. Obstet. Gynecol. 2015, 58, 172–184. [Google Scholar] [CrossRef]
- Tu, W.; Batteiger, B.E.; Wiehe, S.; Ofner, S.; Van Der Pol, B.; Katz, B.P.; Orr, D.P.; Fortenberry, J.D. Time from first intercourse to first sexually transmitted infection diagnosis among adolescent women. Arch. Pediatr. Adolesc. Med. 2009, 163, 1106–1111. [Google Scholar] [CrossRef] [PubMed]
- Newbern, E.C.; Anschuetz, G.L.; Eberhart, M.G.; Salmon, M.E.; Brady, K.A.; De Los Reyes, A.; Baker, J.M.; Asbel, L.E.; Johnson, C.C.; Schwarz, D.F. Adolescent sexually transmitted infections and risk for subsequent HIV. Am. J. Public Health 2013, 103, 1874–1881. [Google Scholar] [CrossRef]
- Kahn, J.A.; Rosenthal, S.L.; Succop, P.A.; Ho, G.Y.; Burk, R.D. Mediators of the association between age of first sexual intercourse and subsequent human papillomavirus infection. Pediatrics 2002, 109, E5. [Google Scholar] [CrossRef]
- Niccolai, L.M.; Ethier, K.A.; Kershaw, T.S.; Lewis, J.B.; Meade, C.S.; Ickovics, J.R. New sex partner acquisition and sexually transmitted disease risk among adolescent females. J. Adolesc. Health 2004, 34, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Burstein, G.R.; Gaydos, C.A.; Diener-West, M.; Howell, M.R.; Zenilman, J.M.; Quinn, T.C. Incident Chlamydia trachomatis infections among inner-city adolescent females. JAMA 1998, 280, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Fasciana, T.; Capra, G.; Lipari, D.; Firenze, A.; Giammanco, A. Sexually Transmitted Diseases: Diagnosis and Control. Int. J. Environ. Res. Public Health 2022, 19, 5293. [Google Scholar] [CrossRef] [PubMed]
- Patchin, J.W.; Hinduja, S. The Nature and Extent of Sexting among a National Sample of Middle and High School Students in the U.S. Arch. Sex. Behav. 2019, 48, 2333–2343. [Google Scholar] [CrossRef] [PubMed]
- Workowski, K.A.; Bachmann, L.H.; Chan, P.A.; Johnston, C.M.; Muzny, C.A.; Park, I.; Reno, H.; Zenilman, J.M.; Bolan, G.A. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm. Rep. 2021, 70, 1–187. [Google Scholar] [PubMed]
- US Preventive Services Task Force; Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Donahue, K.; Doubeni, C.A.; Epling, J.W., Jr.; et al. Behavioral Counseling Interventions to Prevent Sexually Transmitted Infections: US Preventive Services Task Force. Recommendation Statement. JAMA 2020, 324, 674–681. [Google Scholar] [PubMed]
- Brookmeyer, K.A.; Hogben, M.; Kinsey, J. The role of behavioral counseling in sexually transmitted disease prevention program settings. Sex. Transm. Dis. 2016, 43, S102–S112. [Google Scholar] [CrossRef] [PubMed]
- Crespillo-Andujar, C.; Díaz-Menéndez, M.; Mora-Rillo, M. Evidence for Previously Unidentified Sexual Transmission of Protozoan Parasites. Emerg. Infect. Dis. 2018, 24, 602–603. [Google Scholar] [CrossRef]
- Fortenberry, J.D.; Brizendine, E.J.; Katz, B.P.; Wools, K.K.; Blythe, M.J.; Orr, D.P. Subsequent sexually transmitted infections among adolescent women with genital infection due to Chlamydia trachomatis, Neisseria gonorrhoeae, or Trichomonas vaginalis. Sex. Transm. Dis. 1999, 26, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Kreisel, K.M.; Weston, E.J.; St Cyr, S.B.; Spicknall, I.H. Estimates of the Prevalence and Incidence of Chlamydia and Gonorrhea among US Men and Women, 2018. Sex. Transm. Dis. 2021, 48, 222–231. [Google Scholar] [CrossRef]
- Tosh, A.K.; Van Der Pol, B.; Fortenberry, J.D.; Williams, J.A.; Katz, B.P.; Batteiger, B.E.; Orr, D.P. Mycoplasma genitalium among adolescent women and their partners. J. Adolesc. Health 2007, 40, 412–417. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cohen, M.S.; Council, O.D.; Chen, J.S. Sexually transmitted infections and HIV in the era of antiretroviral treatment and prevention: The biologic basis for epidemiologic synergy. J. Int. AIDS Soc. 2019, 22, e25355. [Google Scholar] [CrossRef] [PubMed]
- Paz-Bailey, G.; Ramaswamy, M.; Hawkes, S.J.; Geretti, A.M. Herpes simplex virus type 2: Epidemiology and management options in developing countries. Sex. Transm. Infect. 2007, 83, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Gaydos, C.; Hardick, J. Point of care diagnostics for sexually transmitted infections: Perspectives and advances. Expert Rev. Anti Infect. Ther. 2014, 12, 657–672. [Google Scholar] [CrossRef] [PubMed]
- Merchant, J.S.; Oh, K.; Klerman, L.V. Douching: A problem for adolescent girls and young women. Arch. Pediatr. Adolesc. Med. 1999, 153, 834–837. [Google Scholar] [CrossRef] [PubMed]
- Piñeiro, L.; Idigoras, P.; Cilla, G. Molecular Typing of Mycoplasma genitalium-Positive Specimens Discriminates between Persistent and Recurrent Infections in Cases of Treatment Failure and Supports Contact Tracing. Microorganisms 2019, 7, 609. [Google Scholar] [CrossRef]
- Ness, R.B.; Soper, D.E.; Holley, R.L.; Peipert, J.; Randall, H.; Sweet, R.L.; Sondheimer, S.J.; Hendrix, S.L.; Hillier, S.L.; Amortegui, A.; et al. Evaluation and Clinical Health (PEACH) Study Investigators. Douching and endometritis: Results from the PID evaluation and clinical health (PEACH) study. Sex. Transm. Dis. 2001, 28, 240–245. [Google Scholar] [CrossRef]
- DiCarlo, R.P.; Martin, D.H. The clinical diagnosis of genital ulcer disease in men. Clin. Infect. Dis. 1997, 25, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Kawata, K.; Koga, H. Sexually transmitted infections and cervical cancer: Knowledge and prevention awareness among female university students in Japan. Nurs. Open 2020, 7, 1139–1145. [Google Scholar] [CrossRef]
- Gaydos, C.A.; Manabe, Y.C.; Melendez, J.H. A Narrative Review of Where We Are with Point-of-Care Sexually Transmitted Infection Testing in the United States. Sex. Transm. Dis. 2021, 48, S71–S77. [Google Scholar] [CrossRef] [PubMed]
- Braverman, P.K.; Breech, L.; Committee on Adolescence; American Academy of Pediatrics. Clinical report—Gynecologic examination for adolescents in the pediatric office setting. Pediatrics 2010, 126, 583–590. [Google Scholar] [CrossRef] [PubMed]
- European Testing Week 2023—10th Anniversary of the Campaign. Available online: https://www.testingweek.eu/ (accessed on 29 December 2023).
- Deliberazione Della Giunta Regionale n. 1640 del 28 Dicembre 2021. Approvazione del Piano Regionale Della Prevenzione 2020–2025. Available online: https://www.salute.gov.it/portale/prevenzione/DELIBERE_PRP_2020-2025/Marche/DGR_approvazione_PRP_2020_2025.pdf (accessed on 29 December 2023).
- Regione Marche. Report Demografia Marche Popolazione 2020. Available online: https://statistica.regione.marche.it/Portals/0/Settori/popolazione/f699a69a-2c10-4e97-b0ba-bbfd0f1f739e.pdf (accessed on 29 December 2023).
- Fondazione Cassa di Risparmio Della Provincia di Macerata. Strategie di Sviluppo Economico Nel Territorio Della Provincia di Macerata. 2012 CCIAA di Macerata e Fondazione CARIMA. Available online: https://www.marche.camcom.it/fai-crescere-la-tua-impresa/progetti-della-camera-di-commercio/visualizza-archivio-progetti-della-camera/orientamenti-per-una-strategia-di-sviluppo-economico-della-provincia-di-macerata/2012-11-strategie-sviluppo-economico-territorio-provincia-macerata.pdf (accessed on 23 September 2023).
- Beayni, N.E.; Hamad, L.; Nakad, C.; Keleshian, S.; Yazbek, S.N.; Mahfouz, R. Molecular prevalence of eight different sexually transmitted infections in a Lebanese major tertiary care center: Impact on public health. Int. J. Mol. Epidemiol. Genet. 2021, 12, 16–23. [Google Scholar]
- Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the Protection of Natural Persons with Regard to the Processing of Personal Data and on the Free Movement of Such Data, and Repealing Directive 95/46/EC (General Data Protection Regulation). Official Journal of the European Union n. 119/1 of the May 4th 2016. 2016. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32016R0679 (accessed on 5 June 2023).
- Legislative Decree 30 June 2003, n. 196 “Codice in Materia di Protezione dei Dati Personali”. S.O n. 123 alla G.U. 29 Luglio 2003, n. 174. Available online: https://www.garanteprivacy.it/documents/10160/0/Codice+in+materia+di+protezione+dei+dati+personali+%28Testo+coordinato%29 (accessed on 5 June 2023).
- Legislative Decree 10 August 2018, n. 101“Disposizioni per L’adeguamento Della Normativa Nazionale alle Disposizioni del Regolamento (UE) 2016/679 del Parlamento Europeo e del Consiglio, del 27 Aprile 2016, Relativo alla Protezione delle Persone Fisiche con Riguardo al Trattamento dei dati Personali, Nonché alla Libera Circolazione di tali dati e che Abroga la Direttiva 95/46/CE. GU Serie Generale n.205 of the September 4th 2018. Available online: https://www.gazzettaufficiale.it/eli/id/2018/09/04/18G00129/sg (accessed on 5 June 2023).
- The Italian Data Protection Authority. “Provvedimento Recante le Prescrizioni Relative al Trattamento di Categorie Particolari di Dati, ai Sensi DELL’ART. 21, Comma 1 del d.lgs. 10 Agosto 2018, n. 101 Adottato il 5 Giugno 2019. Gazzetta Ufficiale Serie Generale n. 176 del 29 Luglio 2019”. 2019. Available online: https://www.garanteprivacy.it/home/docweb/-/docweb-display/docweb/9124510 (accessed on 5 June 2023).
- The Italian Data Protection Authority. “Regole Deontologiche per Trattamenti a Fini Statistici o di Ricerca Scientifica Adottate dal Garante, ai Sensi DELL’ART. 20, Comma 4, del d.lgs. 10 agosto 2018, n. 101, con Provvedimento n. 515, del 19 Dicembre 2018. Gazzetta Ufficiale n. 11 del 14 Gennaio 2019”. 2019. Available online: https://www.garanteprivacy.it/home/docweb/-/docweb-display/docweb/9069637 (accessed on 5 June 2023).
- Chen, X.; Lu, Y.; Chen, T.; Li, R. The Female Vaginal Microbiome in Health and Bacterial Vaginosis. Front. Cell. Infect. Microbiol. 2021, 11, 631972. [Google Scholar] [CrossRef] [PubMed]
- Schwebke, J.R.; Muzny, C.A.; Josey, W.E. Role of Gardnerella vaginalis in the pathogenesis of bacterial vaginosis: A conceptual model. J. Infect. Dis. 2014, 210, 338–343. [Google Scholar] [CrossRef]
- Sexually Transmitted Infections (STIs)—Official WHO Updates. Available online: https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis)?gclid=Cj0KCQiAmNeqBhD4ARIsADsYfTdPw4lXwfnkOE6Zgm8nfs8HYNQ-4s4Zxi0-iapK3twWOsw-OmbQz_kaAi0hEALw_wcB (accessed on 10 October 2023).
- Garcia, M.R.; Leslie, S.W.; Wray, A.A. Sexually Transmitted Infections. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Newman, L.; Rowley, J.; Vander Hoorn, S.; Wijesooriya, N.S.; Unemo, M.; Low, N.; Stevens, G.; Gottlieb, S.; Kiarie, J.; Temmerman, M. Global Estimates of the Prevalence and Incidence of Four Curable Sexually Transmitted Infections in 2012 Based on Systematic Review and Global Reporting. PLoS ONE 2015, 10, e0143304. [Google Scholar] [CrossRef] [PubMed]
- Leli, C.; Mencacci, A.; Latino, M.A.; Clerici, P.; Rassu, M.; Perito, S.; Castronari, R.; Pistoni, E.; Luciano, E.; De Maria, D.; et al. Prevalence of cervical colonization by Ureaplasma parvum, Ureaplasma urealyticum, Mycoplasma hominis and Mycoplasma genitalium in childbearing age women by a commercially available multiplex real-time PCR: An Italian observational multicentre study. J. Microbiol. Immunol. Infect. 2018, 51, 220–225. [Google Scholar] [CrossRef]
- Berçot, B.; Amarsy, R.; Goubard, A.; Aparicio, C.; Loeung, H.U.; Segouin, C.; Gueret, D.; Jacquier, H.; Meunier, F.; Mougari, F.; et al. Assessment of coinfection of sexually transmitted pathogen microbes by use of the anyplex II STI-7 molecular kit. J. Clin. Microbiol. 2015, 53, 991–993. [Google Scholar] [CrossRef] [PubMed]
- Mitjà, O.; Padovese, V.; Folch, C.; Rossoni, I.; Marks, M.; Rodríguez, I.; Arias, M.A.; Telenti, A.; Ciuffi, A.; Blondeel, K.; et al. Epidemiology and determinants of reemerging bacterial sexually transmitted infections (STIs) and emerging STIs in Europe. Lancet Reg. Health Eur. 2023, 34, 100742. [Google Scholar] [CrossRef]
- Perry, M.D.; Jones, S.; Bertram, A.; de Salazar, A.; Barrientos-Durán, A.; Schiettekatte, G.; Lewinski, M.; Arcenas, R.; Hansra, A.; Njoya, M.; et al. The prevalence of Mycoplasma genitalium (MG) and Trichomonas vaginalis (TV) at testing centers in Belgium, Germany, Spain, and the UK using the cobas TV/MG molecular assay. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2023, 42, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Hiller, J.; Schatz, K.; Drexler, H. Gender influence on health and risk behavior in primary prevention: A systematic review. Z. Gesundh Wiss. 2017, 25, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Panchanadeswaran, S.; Johnson, S.C.; Mayer, K.H.; Srikrishnan, A.K.; Sivaran, S.; Zelaya, C.E.; Go, V.F.; Solomon, S.; Bentley, M.E.; Celentano, D.D. Gender differences in the prevalence of sexually transmitted infections and genital symptoms in an urban setting in southern India. Sex. Transm. Infect. 2006, 82, 491–495. [Google Scholar] [CrossRef]
- Wang, Y.; Hunt, K.; Nazareth, I.; Freemantle, N.; Petersen, I. Do men consult less than women? An analysis of routinely collected UK general practice data. BMJ Open 2013, 3, e003320. [Google Scholar] [CrossRef]
- Stary, A. The Changing Spectrum of Sexually Transmitted Infections in Europe. Acta Derm. Venereol. 2020, 100, adv00114. [Google Scholar] [CrossRef] [PubMed]
- Guidelines, Recommendations and Reports Vol. 70 No. 4. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8344968/pdf/rr7004a1.pdf (accessed on 5 June 2023).
- Donisi, A.; Colpani, A.; Zauli, B.; De Vito, A.; Fiore, V.; Babudieri, S.; Madeddu, G. Sexually Transmitted Infections Prevalence and Cascade of Care among Undocumented Sex Workers: A Twenty-Year-Long Experience. Life 2023, 13, 606. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Comuni in Provincia di Macerata per Popolazione. Available online: https://www.tuttitalia.it/marche/provincia-di-macerata/20-comuni/popolazione/ (accessed on 5 June 2023).
- Dionne-Odom, J.; Cozzi, G.D.; Franco, R.A.; Njei, B.; Tita, A.T.N. Treatment and Prevention of Viral Hepatitis in Pregnancy. Am. J. Obstet. Gynecol. 2022, 226, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Law 27 May 1991, n. 165 “Obbligatorietà Della Vaccinazione Contro L’epatite Virale B. GU Serie Generale n.127 del 01/06/1991”. Available online: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=1991-06-01&atto.codiceRedazionale=091G0201&elenco30giorni=false (accessed on 5 June 2023).
- Suay-García, B.; Pérez-Gracia, M.-T. Neisseria gonorrhoeae Infections. Pathogens 2020, 9, 647. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. “Campagna di Comunicazione Sulla Vaccinazione Anti-HPV”. 2022. Available online: https://www.salute.gov.it/portale/vaccinazioni/dettaglioCampagneVaccinazioni.jsp?lingua=italiano&menu=campagne&p=dacampagne&id=167#:~:text=In%20Italia%20la%20vaccinazione%20anti,le%20dosi%20previste%20sono%20tre (accessed on 5 June 2023).
- Bergamini, M.; Cucchi, A.; Guidi, E.; Stefanati, A.; Bonato, B.; Lupi, S.; Gregorio, P. Risk perception of sexually transmitted diseases and teenage sexual behaviour: Attitudes towards in a sample of Italian adolescents. J. Prev. Med. Hyg. 2013, 54, 114–119. [Google Scholar] [PubMed]
- Panatto, D.; Amicizia, D.; Lugarini, J.; Sasso, T.; Sormani, M.P.; Badolati, G.; Gasparini, R. Sexual behaviour in Ligurian (Northern Italy) adolescents and young people: Suggestions for HPV vaccination policies. Vaccine 2009, 27, A6–A10. [Google Scholar] [CrossRef] [PubMed]
- Italian Ministry of Education. D.P.R. 9 ottobre 1990, n. 309. Testo Unico Delle Leggi in Materia di Disciplina Degli Stupefacenti e Sostanze Psicotrope, Prevenzione, Cura e Riabilitazione dei Relativi Stati di Tossicodipendenze. GU 31-10-1990, n. 255. Available online: https://www.gazzettaufficiale.it/eli/id/1990/10/31/090G0363/sg (accessed on 5 June 2023).
- Gabarron, E.; Wynn, R. Use of social media for sexual health promotion: A scoping review. Glob. Health Action 2016, 9, 32193. [Google Scholar] [CrossRef]
- Zizza, A.; Guido, M.; Recchia, V.; Grima, P.; Banchelli, F.; Tinelli, A. Knowledge, Information Needs and Risk Perception about HIV and Sexually Transmitted Diseases after an Education Intervention on Italian High School and University Students. Int. J. Environ. Res. Public Health 2021, 18, 2069. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Yan, W.; Jing, W.; Qin, C.; Liu, Q.; Liu, M.; Liu, J. Increasing incidence rates of sexually transmitted infections from 2010 to 2019: An analysis of temporal trends by geographical regions and age groups from the 2019 Global Burden of Disease Study. BMC Infect. Dis. 2022, 22, 574. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exam | Laboratory Method Used |
|---|---|
| Hepatitis B surface antigen HBV (HBs Ag) | Chemioluminescence |
| HBeAg | Chemioluminescence |
| Anti-HBc IgM | Chemioluminescence |
| Anti-HBc TOTAL (IgM + IgG) | Chemioluminescence |
| Anti-HBE | Chemioluminescence |
| Anti-HbsAG | Chemioluminescence |
| Anti-HCV IgG | Chemioluminescence |
| Chlamydia trachomatis—PCR on cervical swab | PCR-real time |
| Culture exam for Gardnerella on vaginal swab | Sowing on agar |
| HPV typing cervical swab | PCR-real time |
| Mycoplasma/Ureaplasma vaginal culture | Cultural examination on “Galleria” |
| Neisseria gonorrhoeae search culture cervical swab | Cultural sowing on biomerieux plate |
| Neisseria gonorrhoeae PCR on cervical swab | PCR real time |
| Treponema antibodies TPHA/TPPA | Chemioluminescence |
| Treponema pallidum VDRL/RPR | Agglutination test (manual) |
| Trichomonas search (PCR) vaginal swab | PCR real time or immunochromotgraphy on paper |
| Virus HIV 1–2 antibodies and antigens p24 | Chemioluminescence |
| Sex | Age Group | 2021 | 2022 | Total |
|---|---|---|---|---|
| F | 0–12 | 27 | 38 | 65 |
| 13–18 | 60 | 121 | 181 | |
| 19–25 | 644 | 945 | 1589 | |
| 26–35 | 2223 | 3630 | 5853 | |
| Total | 2954 | 4734 | 7688 | |
| M | 0–12 | 28 | 37 | 65 |
| 13–18 | 54 | 44 | 98 | |
| 19–25 | 180 | 215 | 395 | |
| 26–35 | 485 | 508 | 993 | |
| Total | 747 | 804 | 1551 | |
| F + M | 3701 | 5538 | 9239 |
| Sex | 2021 | 2022 | Total |
|---|---|---|---|
| F | 19,642 | 91,300 | 110,942 |
| M | 4771 | 5502 | 10,273 |
| Total | 24,413 | 96,802 | 121,215 |
| Exam | Sex | Age Group | MT | HL | CT | Total |
|---|---|---|---|---|---|---|
| Hepatitis B surface antigen HBV (HBs Ag) | F | 0–12 | 14 | 32 | 16 | 62 |
| 13–18 | 18 | 98 | 70 | 186 | ||
| 19–25 | 176 | 582 | 622 | 1380 | ||
| 26–35 | 576 | 2484 | 2302 | 5362 | ||
| M | 0–12 | 26 | 42 | 10 | 78 | |
| 13–18 | 24 | 88 | 40 | 152 | ||
| 19–25 | 68 | 224 | 248 | 540 | ||
| 26–35 | 140 | 608 | 474 | 1222 | ||
| Total | 1042 | 4158 | 3782 | 8982 | ||
| ANTIGEN and HBV (HBeAg) | F | 0–12 | 0 | 6 | 4 | 10 |
| 13–18 | 2 | 26 | 4 | 32 | ||
| 19–25 | 6 | 46 | 40 | 92 | ||
| 26–35 | 20 | 84 | 76 | 180 | ||
| M | 0–12 | 0 | 8 | 2 | 10 | |
| 13–18 | 2 | 8 | 4 | 14 | ||
| 19–25 | 12 | 38 | 36 | 86 | ||
| 26–35 | 32 | 104 | 94 | 230 | ||
| Total | 74 | 320 | 260 | 654 | ||
| ANTI-HBc Ig M | F | 0–12 | 0 | 4 | 6 | 10 |
| 13–18 | 2 | 32 | 4 | 38 | ||
| 19–25 | 20 | 84 | 70 | 174 | ||
| 26–35 | 28 | 144 | 162 | 334 | ||
| M | 0–12 | 0 | 8 | 2 | 10 | |
| 13–18 | 2 | 14 | 6 | 22 | ||
| 19–25 | 20 | 64 | 82 | 166 | ||
| 26–35 | 34 | 160 | 160 | 354 | ||
| Total | 106 | 510 | 492 | 1108 | ||
| ANTI-HBc IgTotal (HBV) | F | 0–12 | 0 | 8 | 6 | 14 |
| 13–18 | 2 | 42 | 4 | 48 | ||
| 19–25 | 56 | 122 | 94 | 272 | ||
| 26–35 | 146 | 284 | 208 | 638 | ||
| M | 0–12 | 0 | 10 | 4 | 14 | |
| 13–18 | 2 | 20 | 4 | 26 | ||
| 19–25 | 36 | 136 | 110 | 282 | ||
| 26–35 | 78 | 356 | 224 | 658 | ||
| Total | 320 | 978 | 654 | 1952 | ||
| ANTI-HBE HBV | F | 0–12 | 0 | 8 | 6 | 14 |
| 13–18 | 2 | 26 | 4 | 32 | ||
| 19–25 | 2 | 48 | 44 | 94 | ||
| 26–35 | 16 | 78 | 68 | 162 | ||
| M | 0–12 | 0 | 8 | 2 | 10 | |
| 13–18 | 2 | 6 | 4 | 12 | ||
| 19–25 | 10 | 44 | 40 | 94 | ||
| 26–35 | 28 | 102 | 78 | 208 | ||
| Total | 60 | 320 | 246 | 626 | ||
| Anti-HbsAG (HBV) | F | 0–12 | 16 | 32 | 14 | 62 |
| 13–18 | 18 | 96 | 32 | 146 | ||
| 19–25 | 126 | 328 | 332 | 786 | ||
| 26–35 | 276 | 760 | 766 | 1802 | ||
| M | 0–12 | 24 | 42 | 14 | 80 | |
| 13–18 | 22 | 90 | 28 | 140 | ||
| 19–25 | 62 | 216 | 194 | 472 | ||
| 26–35 | 132 | 518 | 350 | 1000 | ||
| Total | 676 | 2082 | 1730 | 4488 |
| Exam | Sex | Age Group | MT | HL | CT | Total |
|---|---|---|---|---|---|---|
| Anti-HCV IgG | F | 0–12 | 4 | 14 | 14 | 32 |
| 13–18 | 8 | 86 | 60 | 154 | ||
| 19–25 | 176 | 592 | 626 | 1394 | ||
| 26–35 | 696 | 2652 | 2618 | 5966 | ||
| M | 0–12 | 2 | 21 | 4 | 27 | |
| 13–18 | 6 | 38 | 30 | 74 | ||
| 19–25 | 70 | 226 | 236 | 532 | ||
| 26–35 | 154 | 726 | 564 | 1444 | ||
| Total | 1116 | 4355 | 4152 | 9623 |
| Exam | Sex | Age Group | MT | HL | CT | Total |
|---|---|---|---|---|---|---|
| Chlamydia trachomatis search (PCR) cervical swab | F | 0–12 | 4 | 2 | 6 | |
| 13–18 | 15 | 22 | 25 | 62 | ||
| 19–25 | 81 | 333 | 246 | 660 | ||
| 26–35 | 201 | 1054 | 781 | 2036 | ||
| Total | 297 | 1413 | 1054 | 2764 |
| Exam | Sex | Age Group | MT | HL | CT | Total |
|---|---|---|---|---|---|---|
| Culture exam for Gardnerella vaginalis on vaginal swab | F | 0–12 | 1 | 1 | ||
| 13–18 | 8 | 11 | 9 | 28 | ||
| 19–25 | 28 | 120 | 74 | 222 | ||
| 26–35 | 74 | 393 | 280 | 747 | ||
| Total | 111 | 524 | 363 | 998 |
| Exam | Sex | Age Group | MT | HL | CT | Total |
|---|---|---|---|---|---|---|
| HPV typing cervical swab | F | 13–18 | 5 | 2 | 7 | |
| 19–25 | 9 | 51 | 24 | 84 | ||
| 26–35 | 19 | 209 | 90 | 318 | ||
| Total | 28 | 268 | 116 | 412 |
| Exam | Sex | Age Group | MT | HL | CT | Total |
|---|---|---|---|---|---|---|
| Mycoplasma/Ureaplasma vaginal culture | F | 0–12 | 6 | 12 | 18 | |
| 13–18 | 45 | 75 | 93 | 213 | ||
| 19–25 | 198 | 1140 | 837 | 2175 | ||
| 26–35 | 528 | 3921 | 2742 | 7191 | ||
| Total | 777 | 5148 | 3672 | 9597 |
| Exam | Sex | Age Group | MT | HL | CT | Total |
|---|---|---|---|---|---|---|
| Neisseria gonorrhoeae search cervical culture swab | F | 0–12 | 4 | 4 | ||
| 13–18 | 12 | 30 | 42 | |||
| 19–25 | 8 | 102 | 188 | 298 | ||
| 26–35 | 10 | 234 | 514 | 758 | ||
| Total | 18 | 352 | 732 | 1102 |
| Exam | Sex | Age Group | MT | HL | CT | Total |
|---|---|---|---|---|---|---|
| Treponema antibodies TPHA/TPPA | F | 0–12 | 4 | 7 | 11 | |
| 13–18 | 1 | 10 | 10 | 21 | ||
| 19–25 | 36 | 137 | 141 | 314 | ||
| 26–35 | 145 | 723 | 778 | 1646 | ||
| M | 0–12 | 9 | 6 | 15 | ||
| 13–18 | 7 | 1 | 8 | |||
| 19–25 | 2 | 30 | 8 | 40 | ||
| 26–35 | 17 | 120 | 62 | 199 | ||
| Total | 201 | 1040 | 1013 | 2254 | ||
| Treponema pallidum VDRL/RPR | F | 0–12 | 4 | 7 | 11 | |
| 13–18 | 1 | 5 | 11 | 17 | ||
| 19–25 | 41 | 127 | 196 | 364 | ||
| 26–35 | 198 | 715 | 1042 | 1955 | ||
| M | 0–12 | 7 | 8 | 15 | ||
| 13–18 | 1 | 3 | 1 | 5 | ||
| 19–25 | 1 | 17 | 8 | 26 | ||
| 26–35 | 19 | 92 | 70 | 181 | ||
| Total | 261 | 970 | 1343 | 2574 |
| Exam | Sex | Age Group | MT | HL | CT | Total |
|---|---|---|---|---|---|---|
| Virus HIV 1–2 antibodies and antigene p24 | F | 0–12 | 10 | 4 | 14 | |
| 13–18 | 76 | 58 | 134 | |||
| 19–25 | 636 | 638 | 1274 | |||
| 26–35 | 2816 | 3122 | 5938 | |||
| M | 0–12 | 12 | 8 | 20 | ||
| 13–18 | 32 | 12 | 44 | |||
| 19–25 | 278 | 194 | 472 | |||
| 26–35 | 750 | 538 | 1288 | |||
| Total | 0 | 4610 | 4574 | 9184 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cannovo, N.; Bianchini, E.; Gironacci, L.; Garbati, E.; Di Prospero, F.; Cingolani, M.; Scendoni, R.; Fedeli, P. Sexually Transmitted Infections in Adolescents and Young Adults: A Cross Section of Public Health. Int. J. Environ. Res. Public Health 2024, 21, 501. https://doi.org/10.3390/ijerph21040501
Cannovo N, Bianchini E, Gironacci L, Garbati E, Di Prospero F, Cingolani M, Scendoni R, Fedeli P. Sexually Transmitted Infections in Adolescents and Young Adults: A Cross Section of Public Health. International Journal of Environmental Research and Public Health. 2024; 21(4):501. https://doi.org/10.3390/ijerph21040501
Chicago/Turabian StyleCannovo, Nunzia, Elena Bianchini, Luciana Gironacci, Elisabetta Garbati, Filiberto Di Prospero, Mariano Cingolani, Roberto Scendoni, and Piergiorgio Fedeli. 2024. "Sexually Transmitted Infections in Adolescents and Young Adults: A Cross Section of Public Health" International Journal of Environmental Research and Public Health 21, no. 4: 501. https://doi.org/10.3390/ijerph21040501
APA StyleCannovo, N., Bianchini, E., Gironacci, L., Garbati, E., Di Prospero, F., Cingolani, M., Scendoni, R., & Fedeli, P. (2024). Sexually Transmitted Infections in Adolescents and Young Adults: A Cross Section of Public Health. International Journal of Environmental Research and Public Health, 21(4), 501. https://doi.org/10.3390/ijerph21040501