
Attention Deficits in Healthcare Workers with Non-Clinical Burnout: An Exploratory Investigation

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Classification of the Participants Based on Their Maslach Burnout Inventory (MBI) Scores
2.3. Power Analysis
2.4. Procedures
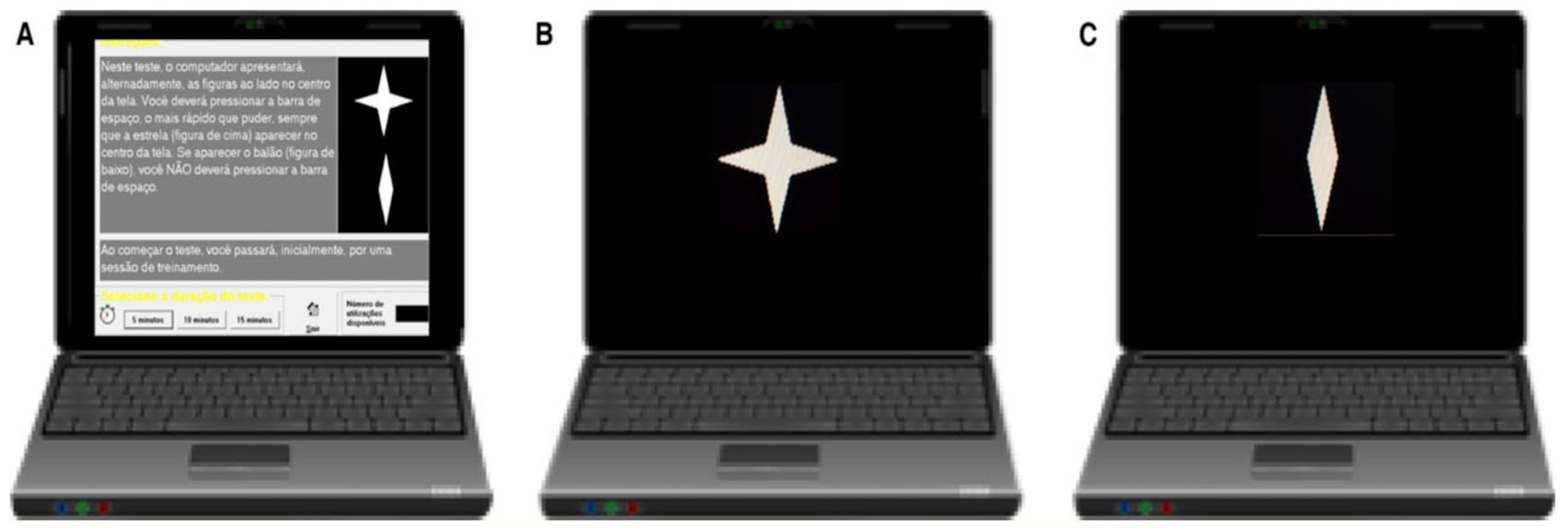
2.4.1. Computerized Visual Attention Test (CVAT)
2.4.2. Maslach Burnout Inventory (MBI)
2.5. Statistical Analysis
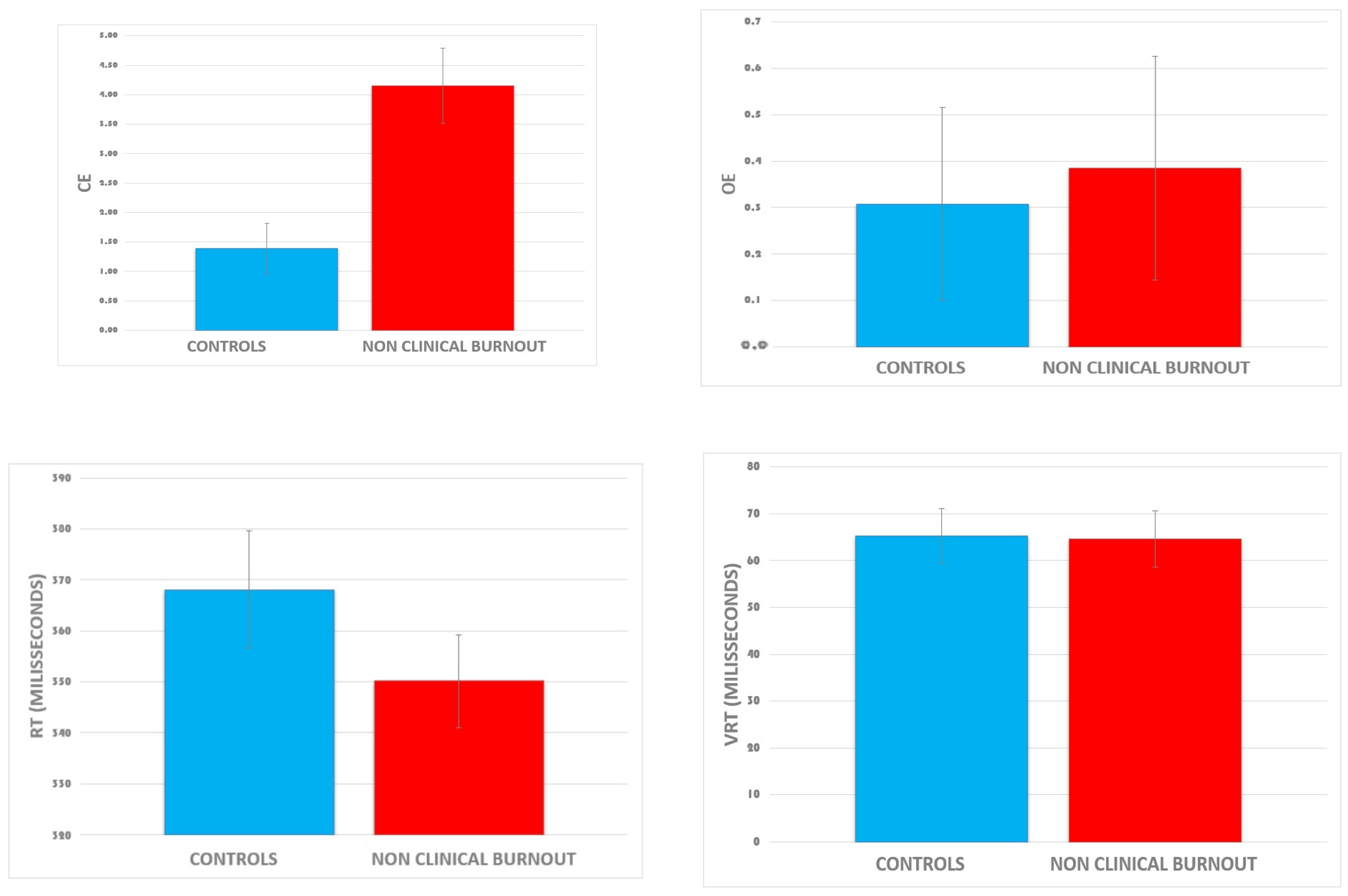
2.5.1. Mean Differences in Attention Performance between Two Groups Dichotomized According to the Presence of Burnout Symptoms
2.5.2. Correlation between Burnout Dimensions and Attention Subdomains
3. Results
4. Discussion
4.1. Executive Deficits in NCB in Healthcare Workers during the COVID-19 Pandemic
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leka, S.; Jain, A.; WHO. Health Impact of Psychosocial Hazards at Work: An Overview. World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Schaufeli, W.; Salanova, M. Burnout, Boredom and Engagement at the Workplace. People at Work: An Introduction to Contemporary Work Psychology; Wiley: Chichester, UK, 2014; pp. 293–320. [Google Scholar]
- Feuerhahn, N.; Stamov-Roßnagel, C.; Wolfram, M.; Bellingrath, S.; Kudielka, B.M. Emotional Exhaustion and Cognitive Performance in Apparently Healthy Teachers: A Longitudinal Multi-Source Study. Stress Health 2013, 29, 297–306. [Google Scholar] [CrossRef]
- Jonsdottir, I.H.; Nordlund, A.; Ellbin, S.; Ljung, T.; Glise, K.; Währborg, P.; Sjörs, A.; Wallin, A. Working Memory and Attention Are Still Impaired after Three Years in Patients with Stress-Related Exhaustion. Scand. J. Psychol. 2017, 58, 504–509. [Google Scholar] [CrossRef]
- Krabbe, D.; Ellbin, S.; Nilsson, M.; Jonsdottir, I.H.; Samuelsson, H. Executive Function and Attention in Patients with Stress-Related Exhaustion: Perceived Fatigue and Effect of Distraction. Stress 2017, 20, 333–340. [Google Scholar] [CrossRef]
- Lemonaki, R.; Xanthopoulou, D.; Bardos, A.N.; Karademas, E.C.; Simos, P.G. Burnout and Job Performance: A Two-Wave Study on the Mediating Role of Employee Cognitive Functioning. Eur. J. Work. Organ. Psychol. 2021, 30, 692–704. [Google Scholar] [CrossRef]
- Linden, D.V.D.; Keijsers, G.P.J.; Eling, P.; Schaijk, R.V. Work Stress and Attentional Difficulties: An Initial Study on Burnout and Cognitive Failures. Work Stress 2005, 19, 23–36. [Google Scholar] [CrossRef]
- Deligkaris, P.; Panagopoulou, E.; Montgomery, A.J.; Masoura, E. Job Burnout and Cognitive Functioning: A Systematic Review. Work Stress 2014, 28, 107–123. [Google Scholar] [CrossRef]
- Brenninkmeijer, V.; VanYperen, N. How to Conduct Research on Burnout: Advantages and Disadvantages of a Unidimensional Approach in Burnout Research. Occup. Environ. Med. 2003, 60, i16–i20. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, D.M.; van Rhenen, W.; Murre, J.M.J.; Verwijk, E. Cognitive Functioning, Sleep Quality, and Work Performance in Non-Clinical Burnout: The Role of Working Memory. PLoS ONE 2020, 15, e0231906. [Google Scholar] [CrossRef]
- Bauernhofer, K.; Bassa, D.; Canazei, M.; Jiménez, P.; Paechter, M.; Papousek, I.; Fink, A.; Weiss, E.M. Subtypes in Clinical Burnout Patients Enrolled in an Employee Rehabilitation Program: Differences in Burnout Profiles, Depression, and Recovery/Resources-Stress Balance. BMC Psychiatry 2018, 18, 10. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine; National Academy of Medicine; Committee on Systems Approaches to Improve Patient Care by Supporting Clinician Well-Being. Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being; National Academies Press (US): Washington, DC, USA, 2019; ISBN 978-0-309-49547-9. [Google Scholar]
- Wright, T.; Mughal, F.; Babatunde, O.O.; Dikomitis, L.; Mallen, C.D.; Helliwell, T. Burnout among Primary Health-Care Professionals in Low- and Middle-Income Countries: Systematic Review and Meta-Analysis. Bull. World Health Organ. 2022, 100, 385A–401A. [Google Scholar] [CrossRef] [PubMed]
- Poghosyan, L.; Clarke, S.P.; Finlayson, M.; Aiken, L.H. Nurse Burnout and Quality of Care: Cross-National Investigation in Six Countries. Res. Nurs. Health 2010, 33, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; West, C.P.; Sinsky, C.; Trockel, M.; Tutty, M.; Satele, D.V.; Carlasare, L.E.; Dyrbye, L.N. Changes in Burnout and Satisfaction With Work-Life Integration in Physicians and the General US Working Population Between 2011 and 2017. Mayo Clin. Proc. 2019, 94, 1681–1694. [Google Scholar] [CrossRef] [PubMed]
- Buselli, R.; Corsi, M.; Baldanzi, S.; Chiumiento, M.; Del Lupo, E.; Dell’Oste, V.; Bertelloni, C.A.; Massimetti, G.; Dell’Osso, L.; Cristaudo, A.; et al. Professional Quality of Life and Mental Health Outcomes among Health Care Workers Exposed to SARS-CoV-2 (COVID-19). Int. J. Environ. Res. Public Health 2020, 17, 6180. [Google Scholar] [CrossRef] [PubMed]
- Duarte, I.; Teixeira, A.; Castro, L.; Marina, S.; Ribeiro, C.; Jácome, C.; Martins, V.; Ribeiro-Vaz, I.; Pinheiro, H.C.; Silva, A.R.; et al. Burnout among Portuguese Healthcare Workers during the COVID-19 Pandemic. BMC Public Health 2020, 20, 1885. [Google Scholar] [CrossRef] [PubMed]
- Haidari, E.; Main, E.K.; Cui, X.; Cape, V.; Tawfik, D.S.; Adair, K.C.; Sexton, B.J.; Profit, J. Maternal and Neonatal Health Care Worker Well-Being and Patient Safety Climate amid the COVID-19 Pandemic. J. Perinatol. 2021, 41, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fernández, M.D.; Pérez-García, E.; Ortega-Galán, Á.M. Quality of Life in Nursing Professionals: Burnout, Fatigue, and Compassion Satisfaction. Int. J. Environ. Res. Public Health 2020, 17, 1253. [Google Scholar] [CrossRef]
- Sexton, J.B.; Adair, K.C.; Proulx, J.; Profit, J.; Cui, X.; Bae, J.; Frankel, A. Emotional Exhaustion Among US Health Care Workers Before and During the COVID-19 Pandemic, 2019–2021. JAMA Netw. Open 2022, 5, e2232748. [Google Scholar] [CrossRef]
- Ulfa, M.; Azuma, M.; Steiner, A. Burnout Status of Healthcare Workers in the World during the Peak Period of the COVID-19 Pandemic. Front. Psychol. 2022, 13, 952783. [Google Scholar] [CrossRef] [PubMed]
- De Medeiros, A.I.C.; de Mesquita, R.B.; de Macêdo, F.S.; de Matos, A.G.C.; Pereira, E.D. Prevalence of Burnout among Healthcare Workers in Six Public Referral Hospitals in Northeastern Brazil during the COVID-19 Pandemic: A Cross-Sectional Study. Sao Paulo Med. J. 2022, 140, 553–558. [Google Scholar] [CrossRef]
- Castaneda, A.E.; Suvisaari, J.; Marttunen, M.; Perälä, J.; Saarni, S.I.; Aalto-Setälä, T.; Lönnqvist, J.; Tuulio-Henriksson, A. Cognitive Functioning in Relation to Burnout Symptoms and Social and Occupational Functioning in a Population-Based Sample of Young Adults. Nord. J. Psychiatry 2011, 65, 32–39. [Google Scholar] [CrossRef]
- McInerney, S.; Rowan, M.; Lawlor, B. Burnout and Its Effect on Neurocognitive Performance. Ir. J. Psychol. Med. 2012, 29, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.G.; Suchy, Y.; Rau, H.K. Individual Differences in Executive Functioning: Implications for Stress Regulation. Ann. Behav. Med. 2009, 37, 126–140. [Google Scholar] [CrossRef] [PubMed]
- Eskildsen, A.; Andersen, L.P.; Pedersen, A.D.; Andersen, J.H. Cognitive Impairments in Former Patients with Work-Related Stress Complaints—One Year Later. Stress 2016, 19, 559–566. [Google Scholar] [CrossRef]
- Koutsimani, P.; Montgomery, A. Cognitive Functioning in Non-Clinical Burnout: Using Cognitive Tasks to Disentangle the Relationship in a Three-Wave Longitudinal Study. Front. Psychiatry 2022, 13, 978566. [Google Scholar] [CrossRef] [PubMed]
- He, S.C.; Zhang, Y.Y.; Zhan, J.Y.; Wang, C.; Du, X.D.; Yin, G.Z.; Cao, B.; Ning, Y.P.; Soares, J.C.; Zhang, X.Y. Burnout and Cognitive Impairment: Associated with Serum BDNF in a Chinese Han Population. Psychoneuroendocrinology 2017, 77, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. What Is Cognitive Reserve? Theory and Research Application of the Reserve Concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Vohs, K.D. Self-Regulation and the Executive Function of the Self. In Handbook of Self and Identity, 2nd ed.; The Guilford Press: New York, NY, USA, 2012; pp. 180–197. ISBN 978-1-4625-0305-6. [Google Scholar]
- Mackie, M.-A.; Van Dam, N.T.; Fan, J. Cognitive Control and Attentional Functions. Brain Cogn. 2013, 82, 301–312. [Google Scholar] [CrossRef]
- Altarabichi, M.G.; Ahmed, M.; Begum, S.; Ciceri, M.; Balzarotti, S.; Biassoni, F.; Lombardi, D.; Perego, P. Reaction Time Variability Association with Safe Driving Indexes. In Proceedings of the Transport Research Arena TRA2020, Helsinki, Finland, 27–30 April 2020. [Google Scholar]
- Anderson, B.A.; Kim, N.; Gregoire, L.; Yan, N.; Ahn, C.R. Attention Failures Cause Workplace Accidents: Why Workers Ignore Hazards and What To Do About It. Available online: https://www.citedrive.com/en/discovery/attention-failures-cause-workplace-accidents-why-workers-ignore-hazards-and-what-to-do-about-it/ (accessed on 1 January 2024).
- Lezak, M.D.; Howieson, D.B.; Bigler, E.D.; Tranel, D. Neuropsychological Assessment, 5th ed.; Oxford University Press: New York, NY, USA, 2012; pp. xxv, 1161. ISBN 978-0-19-539552-5. [Google Scholar]
- Egeland, J.; Kovalik-Gran, I. Measuring Several Aspects of Attention in One Test: The Factor Structure of Conners’s Continuous Performance Test. J. Atten. Disord. 2010, 13, 339–346. [Google Scholar] [CrossRef]
- Petersen, S.E.; Posner, M.I. The Attention System of the Human Brain: 20 Years after. Annu. Rev. Neurosci. 2012, 35, 73–89. [Google Scholar] [CrossRef]
- Schmidt, S.L.; Simões, E.N.; Novais Carvalho, A.L. Association between Auditory and Visual Continuous Performance Tests in Students with ADHD. J. Atten. Disord. 2019, 23, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Simões, E.N.; Carvalho, A.L.N.; Schmidt, S.L. The Role of Visual and Auditory Stimuli in Continuous Performance Tests: Differential Effects on Children With ADHD. J. Atten. Disord. 2021, 25, 53–62. [Google Scholar] [CrossRef]
- do Carmo Filho, A.; van Duinkerken, E.; Tolentino, J.C.; Schmidt, S.L. Attention Profile of Physically Recovered COVID-19 Inpatients on the Day of Discharge. J. Psychiatr. Res. 2022, 150, 189–196. [Google Scholar] [CrossRef]
- Schmidt, S.L.; Araguez, I.M.; Neves, V.V.; van Duinkerken, E.; Schmidt, G.J.; Tolentino, J.C.; Gjorup, A.L.T. Attention Deficits in Brazilian Health Care Workers with Chronic Pain. Front. Psychol. 2022, 13, 1024584. [Google Scholar] [CrossRef]
- Tolentino, J.C.; Gjorup, A.L.T.; Schmidt, G.J.; Schmidt, S.L. Early Attention Impairment in a Patient with COVID-19. Psychiatry Clin. Neurosci. 2021, 75, 66–67. [Google Scholar] [CrossRef]
- Gómez-Urquiza, J.L.; Vargas, C.; De la Fuente, E.I.; Fernández-Castillo, R.; Cañadas-De la Fuente, G.A. Age as a Risk Factor for Burnout Syndrome in Nursing Professionals: A Meta-Analytic Study. Res. Nurs. Health 2017, 40, 99–110. [Google Scholar] [CrossRef]
- Salthouse, T.A. Selective Review of Cognitive Aging. J. Int. Neuropsychol. Soc. 2010, 16, 754–760. [Google Scholar] [CrossRef]
- Harada, C.N.; Natelson Love, M.C.; Triebel, K. Normal Cognitive Aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Kivimaki, M.; Glymour, M.M.; Elbaz, A.; Berr, C.; Ebmeier, K.P.; Ferrie, J.E.; Dugravot, A. Timing of Onset of Cognitive Decline: Results from Whitehall II Prospective Cohort Study. BMJ 2012, 344, d7622. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.L.; Manhães, A.C. Manual Do Teste Computadorizado de Atenção Visual: Normas, Fidedignidade e Validade [Guidebook of the Continuous Visual Attention Test: Norms, Reliability, and Validity]; Cognitive Neuropsychology: Rio de Janeiro, Brazil, 2019. [Google Scholar]
- Maslach, C.; Jackson, S.E. The Measurement of Experienced Burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E. Maslach Burnout Inventory: Manual; Consulting Psychologists Press: Washington, DC, USA, 1986; ISBN 978-99948-922-4-2. [Google Scholar]
- Halbesleben, J.R.B.; Demerouti, E. The Construct Validity of an Alternative Measure of Burnout: Investigating the English Translation of the Oldenburg Burnout Inventory. Work Stress 2005, 19, 208–220. [Google Scholar] [CrossRef]
- Ricardo, Y.R.; Paneque, F.R.R. Hacia un estudio bidimensional del Síndrome de Burnout en estudiantes universitarios. Ciênc. Saúde Coletiva 2014, 19, 4767–4775. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; Christensen, K.B. The Copenhagen Burnout Inventory: A New Tool for the Assessment of Burnout. Work Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.; Leiter, M. The Maslach Burnout Inventory Manual; Scarecrow Education: Lanham, MD, USA, 1996; Volume 3, pp. 191–218. [Google Scholar]
- Mclaurine, W.D. Correlational Study of Job Burnout and Organizational Commitment among Correctional Officers. Ph.D. Thesis, School of Psychology, Capella University, Minneapolis, MN, USA, 2008. [Google Scholar]
- da Schuster, M.S.; da Dias, V.V.; Battistella, L.F. Maslach Burnout Inventory—General Survey (MBI-GS): Aplicação em Universidade Público Federal. Rev. Fac. Adm. Econ. 2015, 6, 182–195. [Google Scholar] [CrossRef]
- da Schuster, M.S.; da Dias, V.V.; Battistella, L.F.; Grohmann, M.Z. Validação da escala MBI-GS: Uma investigação general survey sobre a percepção de saúde dos colaboradores. REGE Rev. Gestão 2015, 22, 403–416. [Google Scholar] [CrossRef]
- Jak, A.J.; Bondi, M.W.; Delano-Wood, L.; Wierenga, C.; Corey-Bloom, J.; Salmon, D.P.; Delis, D.C. Quantification of Five Neuropsychological Approaches to Defining Mild Cognitive Impairment. Am. J. Geriatr. Psychiatry. 2009, 17, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Schafer, W.D. Interpreting Statistical Significance and Nonsignificance. J. Exp. Educ. 1993, 61, 383–387. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- STROBE Statement—Checklist of Items That Should Be Included in Reports of Observational Studies1 (© STROBE Initiative). Int. J. Public Health 2008, 53, 3–4. [CrossRef]
- Simões, E.N.; Padilla, C.S.; Bezerra, M.S.; Schmidt, S.L. Analysis of Attention Subdomains in Obstructive Sleep Apnea Patients. Front. Psychiatry 2018, 9, 435. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory Manual, 4th ed.; Mind Garden, Inc.: Menlo Park, CA, USA, 2018. [Google Scholar]
- Olejnik, S.F.; Algina, J. Parametric ANCOVA and the Rank Transform ANCOVA When the Data Are Conditionally Non-Normal and Heteroscedastic. J. Educ. Stat. 1984, 9, 129–149. [Google Scholar] [CrossRef]
- Pearce, N. Analysis of Matched Case-Control Studies. BMJ Clin. Res. Ed. 2016, 352, i969. [Google Scholar] [CrossRef] [PubMed]
- Manly, T.; Robertson, I.H.; Galloway, M.; Hawkins, K. The Absent Mind: Further Investigations of Sustained Attention to Response. Neuropsychologia 1999, 37, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Norman, D.A.; Shallice, T. Attention to Action. In Consciousness and Self-Regulation; Davidson, R.J., Schwartz, G.E., Shapiro, D., Eds.; Springer: Boston, MA, USA, 1986. [Google Scholar] [CrossRef]
- Manuel, A.L.; Foxe, D.; Bradshaw, N.; Cordato, N.J.; Hodges, J.R.; Burrell, J.R.; Piguet, O. Sustained attention failures on a 3-min reaction time task is a sensitive marker of dementia. J. Neurol. 2019, 266, 1323–1331. [Google Scholar] [CrossRef] [PubMed]
- Chirico, F.; Magnavita, N. Burnout Syndrome and Meta-Analyses: Need for Evidence-Based Research in Occupational Health. Comments on Prevalence of Burnout in Medical and Surgical Residents: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, doi:10.3390/ijerph16091479. Int. J. Environ. Res. Public Health 2020, 17, 741. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Demographics and Burnout Dimensions | Non-Clinical Burnout (n = 13) | Controls (n = 13) | Group DIFF (P) |
|---|---|---|---|
| FEMALE | 5 (38.46%) | 4 (30.76%) | ns |
| AGE | 34.23 ± 7.0 | 36.38 ± 3.2 | ns |
| PHYSICIANS | 5 (38.46%) | 6 (46.15%) | ns |
| NURSES AND NURSE AIDES | 8 (61.15%) | 7 (53.38%) | ns |
| AVERAGE EXH | 5.11 ± 0.59 | 0.73 ± 0.43 | <0.01 |
| AVERAGE CY | 4.49 ± 1.12 | 0.14 ± 0.25 | <0.01 |
| AVERAGE PE | 3.23 ± 0.32 | 5.53 ± 0.56 | <0.01 |
| Variables | Average EXH | Average CY | Average PE |
|---|---|---|---|
| CE | |||
| R Pearson | 0.545 * | 0.563 * | −0.522 * |
| p-value | 0.004 | 0.003 | 0.006 |
| OE | |||
| R Pearson | 0.013 | 0.047 | −0.079 |
| p-value | 0.950 | 0.818 | 0.703 |
| RT | |||
| R Pearson | −0.228 | −0.318 | 0.334 |
| p-value | 0.262 | 0.114 | 0.095 |
| VRT | |||
| R Pearson | 0.011 | −0.106 | 0.074 |
| p-value | 0.957 | 0.608 | 0.720 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmidt, S.L.; da Silva Cunha, B.; Tolentino, J.C.; Schmidt, M.J.; Schmidt, G.J.; Marinho, A.D.; van Duinkerken, E.; Gjorup, A.L.T.; Landeira-Fernandez, J.; Mello, C.R.; et al. Attention Deficits in Healthcare Workers with Non-Clinical Burnout: An Exploratory Investigation. Int. J. Environ. Res. Public Health 2024, 21, 239. https://doi.org/10.3390/ijerph21020239
Schmidt SL, da Silva Cunha B, Tolentino JC, Schmidt MJ, Schmidt GJ, Marinho AD, van Duinkerken E, Gjorup ALT, Landeira-Fernandez J, Mello CR, et al. Attention Deficits in Healthcare Workers with Non-Clinical Burnout: An Exploratory Investigation. International Journal of Environmental Research and Public Health. 2024; 21(2):239. https://doi.org/10.3390/ijerph21020239
Chicago/Turabian StyleSchmidt, Sergio L., Bruno da Silva Cunha, Julio Cesar Tolentino, Marcela J. Schmidt, Guilherme J. Schmidt, Alice D. Marinho, Eelco van Duinkerken, Ana Lucia Taboada Gjorup, Jesus Landeira-Fernandez, Carolina Ribeiro Mello, and et al. 2024. "Attention Deficits in Healthcare Workers with Non-Clinical Burnout: An Exploratory Investigation" International Journal of Environmental Research and Public Health 21, no. 2: 239. https://doi.org/10.3390/ijerph21020239
APA StyleSchmidt, S. L., da Silva Cunha, B., Tolentino, J. C., Schmidt, M. J., Schmidt, G. J., Marinho, A. D., van Duinkerken, E., Gjorup, A. L. T., Landeira-Fernandez, J., Mello, C. R., & de Souza, S. P. (2024). Attention Deficits in Healthcare Workers with Non-Clinical Burnout: An Exploratory Investigation. International Journal of Environmental Research and Public Health, 21(2), 239. https://doi.org/10.3390/ijerph21020239