
Trajectories of Adjustment Disorder and Well-Being in Austria and Croatia during 20 Months of the COVID-19 Pandemic

 , , ,
, , , 
Abstract
:1. Introduction
1.1. Adjustment Disorder Amidst COVID-19
1.2. Trajectories of Adjustment Disorder Amidst COVID-19
1.3. Current Study
1.4. Aims and Research Questions
- How do the trajectories of AD symptoms and well-being develop over time in Austria and Croatia?
- To what extent can sociodemographic characteristics (country, age, gender, income and education) predict the trajectories of AD and well-being?
- To what extent can the symptoms of anxiety and depression predict the trajectories of AD and well-being?
2. Materials and Methods
2.1. Procedure and Participants
2.2. Measures
2.3. Data Analysis
2.3.1. Measurement Invariance
2.3.2. Latent Growth Modelling
- Univariate models: Firstly, univariate unconditional models were estimated to explore changes over time in AD and well-being separately. Next, the time-invariant covariates (TICs [64]) age, gender, country, education and income were included as predictors of the variability in the intercept and slope in two conditional models for AD symptoms and well-being, respectively. In a third step, depression (determined via the PHQ-2) and anxiety (determined via the GAD-2) scores were added as time-varying covariates (TVCs [64]).
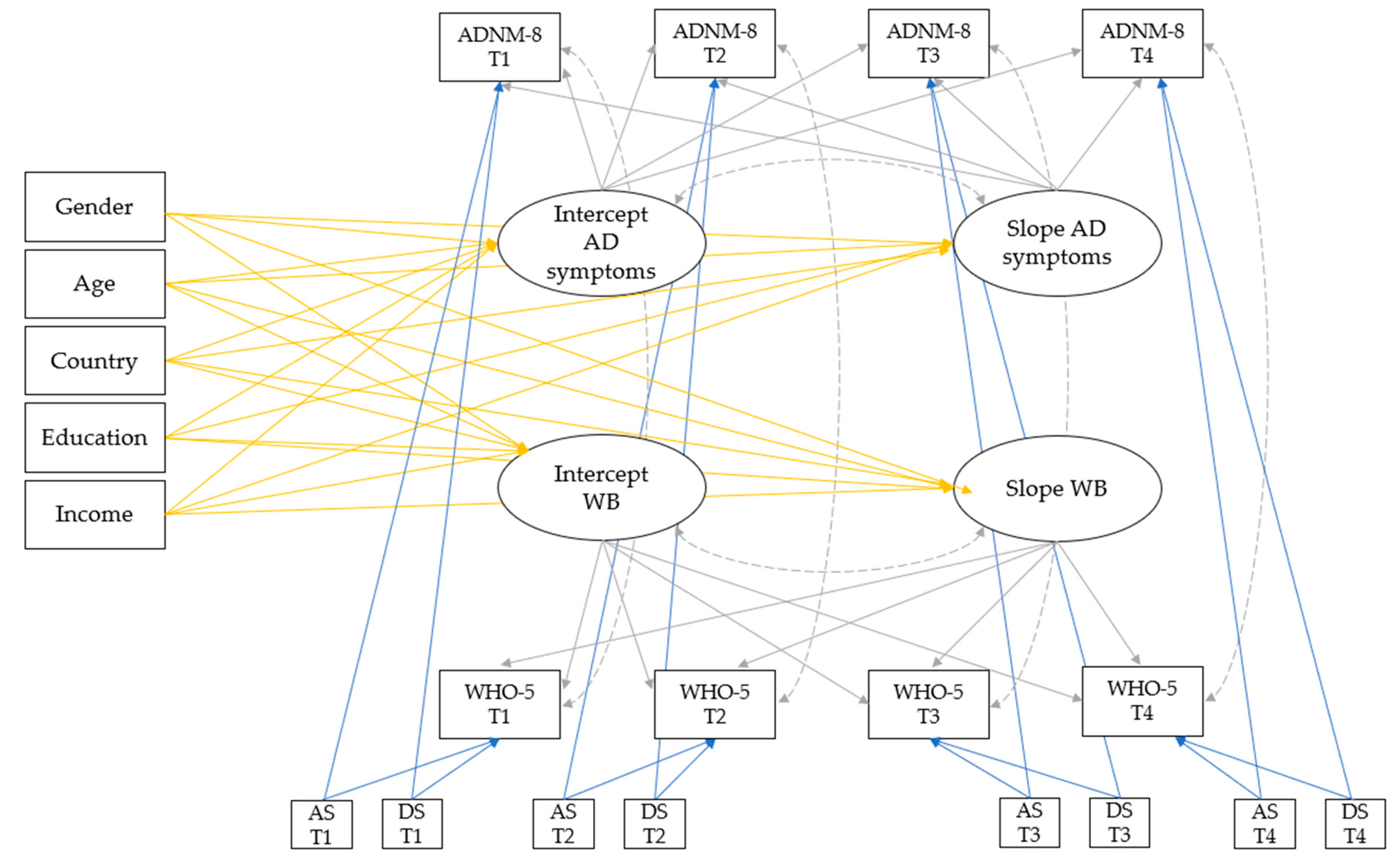
- Multivariate models: The same procedure was repeated for multivariate models (i.e., joint models for AD symptoms and well-being) to investigate how AD symptoms and well-being simultaneously unfold over time [65]. The final model included all TICs and TVCs to explore whether these can explain the residual variance in the joint model. Moreover, the covariance between the intercept and slope was estimated for each primary outcome. Residuals between the primary outcomes were allowed to correlate within one timepoint. Figure 1 shows the proposed multivariate model of AD symptoms and well-being with all predictors and covariances.
- Multivariate models by country: In the last step, the final model was executed in the Austrian and Croatian samples separately in order to explore possible differences in the growth trajectory and predictors between the two countries. For this final analysis, the predictor “country” was obsolete; thus, it was excluded from the analysis. The other model specifications remained unchanged.
3. Results
3.1. Participant Flow and Missing Data
3.2. Cross-Country Differences and Measurement Invariance
3.3. Mental Health Outcomes over Time
3.4. Univariate LGCMs
3.5. Multivariate LGCMs
3.6. Multivariate LGCMs by Country
4. Discussion
4.1. Mental Health Outcomes over Time
4.2. Trajectories of Adjustment and Well-Being
4.3. Predictors of Adjustment and Well-Being Trajectories
4.4. Cross-Country Differences in Adjustment and Well-Being Trajectories
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Javakhishvili, J.D.; Ardino, V.; Bragesjö, M.; Gorniak, J.; Kazlauskas, E.; Schäfer, I.; Schäflein, E.; Williamson, V. ESTSS Recommendations on Mental Health and Psychosocial Care During Pandemics. 2020. Available online: https://estss.org/wp-content/uploads/2020/05/ESTSS.Covid-19-Recommendations-2020-26-May.pdf (accessed on 26 September 2023).
- Giusti, L.; Salza, A.; Mammarella, S.; Bianco, D.; Ussorio, D.; Casacchia, M.; Roncone, R. #Everything will be fine. Duration of home confinement and “all-or-nothing” cognitive thinking style as predictors of traumatic distress in young university students on a digital platform during the COVID-19 Italian lockdown. Front. Psychiatry 2020, 11, 574812. [Google Scholar] [CrossRef] [PubMed]
- Kira, I.A.; Shuwiekh, H.A.M.; Ashby, J.S.; Elwakeel, S.A.; Alhuwailah, A.; Sous, M.S.F.; Baali, S.B.A.; Azdaou, C.; Oliemat, E.M.; Jamil, H.J. The impact of COVID-19 traumatic stressors on mental health: Is COVID-19 a new trauma type. Int. J. Ment. Health Addict. 2023, 21, 51–70. [Google Scholar] [CrossRef] [PubMed]
- Kazlauskas, E.; Quero, S. Adjustment and coronavirus: How to prepare for COVID-19 pandemic-related adjustment disorder worldwide? Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S22–S24. [Google Scholar] [CrossRef] [PubMed]
- Brunet, A.; Rivest-Beauregard, M.; Lonergan, M.; Cipolletta, S.; Rasmussen, A.; Meng, X.; Jaafari, N.; Romero, S.; Superka, J.; Brown, A.D.; et al. PTSD is not the emblematic disorder of the COVID-19 pandemic; adjustment disorder is. BMC Psychiatry 2022, 22, 300. [Google Scholar] [CrossRef]
- Federal Ministry for European and International Affairs. Austria’s Neighbours. Available online: https://www.bmeia.gv.at/en/european-foreign-policy/foreign-policy/europe/austrias-neighbours/ (accessed on 26 September 2023).
- Helliwell, J.F.; Layard, R.; Sachs, J.D.; De Neve, J.-E.; Aknin, L.B.; Wang, S. World Happiness Report 2023; Sustainable Development Solutions Network: New York, NY, USA, 2023; ISBN 978-1-7348080-5-6. [Google Scholar]
- The World Bank. World Development Indicators. Available online: https://databank.worldbank.org/source/world-development-indicators (accessed on 31 August 2023).
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- Zelviene, P.; Kazlauskas, E. Adjustment disorder: Current perspectives. Neuropsychiatr. Dis. Treat. 2018, 14, 375–381. [Google Scholar] [CrossRef]
- O’Donnell, M.L.; Agathos, J.A.; Metcalf, O.; Gibson, K.; Lau, W. Adjustment disorder: Current developments and future directions. Int. J. Environ. Res. Public Health 2019, 16, 2537. [Google Scholar] [CrossRef]
- World Health Organization. The 11th Revision of the International Classification of Diseases. Available online: https://icd.who.int/browse11/l-m/en (accessed on 31 August 2023).
- O’Donnell, M.L.; Alkemade, N.; Creamer, M.; McFarlane, A.C.; Silove, D.; Bryant, R.A.; Felmingham, K.; Steel, Z.; Forbes, D. A longitudinal study of adjustment disorder after trauma exposure. Am. J. Psychiatry 2016, 173, 1231–1238. [Google Scholar] [CrossRef]
- Vancappel, A.; Jansen, E.; Bachem, R.; Bray, A.; Egreteau, L.; Réveillère, C.; Maercker, A.; El-Hage, W. Validation of the French ADNM-20 in the assessment of emotional difficulties resulting from COVID-19 quarantine and outbreak. BMC Psychol. 2021, 9, 3–9. [Google Scholar] [CrossRef]
- Jannini, T.B.; Rossi, R.; Socci, V.; Reda, F.; Pacitti, F.; Di Lorenzo, G. Psychometric and factorial validity of the International Adjustment Disorder Questionnaire (IADQ) in an Italian sample: A validation and prevalence estimate study. Clin. Psychol Psychother. 2022, 30, 436–445. [Google Scholar] [CrossRef]
- Bohlken, J.; Kostev, K.; Riedel-Heller, S.; Hoffmann, W.; Michalowsky, B. Effect of the COVID-19 pandemic on stress, anxiety, and depressive disorders in German primary care: A cross-sectional study. J. Psychiatr. Res. 2021, 143, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Makhashvili, N.; Javakhishvili, J.D.; Sturua, L.; Pilauri, K.; Fuhr, D.C.; Roberts, B. The influence of concern about COVID-19 on mental health in the Republic of Georgia: A cross-sectional study. Glob. Health 2020, 16, 111. [Google Scholar] [CrossRef] [PubMed]
- Lotzin, A.; Krause, L.; Acquarini, E.; Ajdukovic, D.; Ardino, V.; Arnberg, F.; Böttche, M.; Bragesjö, M.; Dragan, M.; Figueiredo-Braga, M.; et al. Risk and protective factors, stressors, and symptoms of adjustment disorder during the COVID-19 pandemic—First results of the ESTSS COVID-19 pan-European ADJUST Study. Eur. J. Psychotraumatol. 2021, 12, 1964197. [Google Scholar] [CrossRef] [PubMed]
- Coiro, M.J.; Asraf, K.; Tzischinsky, O.; Hadar-Shoval, D.; Tannous-Haddad, L.; Wolfson, A.R. Sleep quality and COVID-19-related stress in relation to mental health symptoms among Israeli and U.S. adults. Sleep Health 2021, 7, 127–133. [Google Scholar] [CrossRef]
- Fioravanti, G.; Bocci Benucci, S.; Prostamo, A.; Banchi, V.; Casale, S. Effects of the COVID-19 pandemic on psychological health in a sample of Italian adults: A three-wave longitudinal study. Psychiatry Res. 2022, 315, 114705. [Google Scholar] [CrossRef] [PubMed]
- Witteveen, A.B.; Young, S.Y.; Cuijpers, P.; Ayuso-Mateos, J.L.; Barbui, C.; Bertolini, F.; Cabello, M.; Cadorin, C.; Downes, N.; Franzoi, D.; et al. COVID-19 and common mental health symptoms in the early phase of the pandemic: An umbrella review of the evidence. PLoS Med. 2023, 20, e1004206. [Google Scholar] [CrossRef]
- Dworakowski, O.; Huber, Z.M.; Meier, T.; Boyd, R.L.; Horn, A.B. Emotion regulation across the lifespan: Age differences in intrapersonal and interpersonal strategies for the adjustment to the COVID-19 pandemic in four countries. Aging Ment. Health 2022, 26, 2048–2053. [Google Scholar] [CrossRef]
- Mahat-Shamir, M.; Pitcho-Prelorentzos, S.; Kagan, M.; Kestler-Peleg, M.; Lavenda, O. Adjustment disorder in the face of COVID-19 outbreak: The impact of death anxiety, media exposure, fear of contagion and hypochondriasis symptoms. Omega 2021, 87, 1189–1206. [Google Scholar] [CrossRef]
- Hamama-Raz, Y.; Goodwin, R.; Leshem, E.; Ben-Ezra, M. The toll of a second lockdown: A longitudinal study. J. Affect. Disord. 2021, 294, 60–62. [Google Scholar] [CrossRef]
- Levin, Y.; Bachem, R.; Goodwin, R.; Hamama-Raz, Y.; Leshem, E.; Ben-Ezra, M. Relationship between adjustment disorder symptoms and probable diagnosis before and after second lockdown in Israel: Longitudinal symptom network analysis. BJPsych Open 2022, 8, e186. [Google Scholar] [CrossRef]
- Bartels, C.; Hessmann, P.; Schmidt, U.; Vogelgsang, J.; Ruhleder, M.; Kratzenberg, A.; Treptow, M.; Reh-Bergen, T.; Abdel-Hamid, M.; Heß, L.; et al. Medium-term and peri-lockdown course of psychosocial burden during the ongoing COVID-19 pandemic: A longitudinal study on patients with pre-existing mental disorders. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 272, 757–771. [Google Scholar] [CrossRef] [PubMed]
- Ben-Ezra, M.; Hamama-Raz, Y.; Goodwin, R.; Leshem, E.; Levin, Y. Association between mental health trajectories and somatic symptoms following a second lockdown in Israel: A longitudinal study. BMJ Open 2021, 11, e050480. [Google Scholar] [CrossRef] [PubMed]
- Kazlauskas, E.; Gelezelyte, O.; Nomeikaite, A.; Zelviene, P. Posttraumatic stress disorder and adjustment disorder in Lithuanian healthcare in 2018–2020: A nation-wide cohort study of the effects of COVID-19 pandemic. Healthcare 2021, 9, 1422. [Google Scholar] [CrossRef] [PubMed]
- Salanti, G.; Peter, N.; Tonia, T.; Holloway, A.; White, I.R.; Darwish, L.; Low, N.; Egger, M.; Haas, A.D.; Fazel, S.; et al. The impact of the COVID-19 pandemic and associated control measures on the mental health of the general population: A systematic review and dose-response meta-analysis. Ann. Intern. Med. 2022, 175, 1560–1571. [Google Scholar] [CrossRef] [PubMed]
- Farrell, A.H.; Vitoroulis, I.; Eriksson, M.; Vaillancourt, T. Loneliness and well-being in children and adolescents during the COVID-19 pandemic: A systematic review. Children 2023, 10, 279. [Google Scholar] [CrossRef]
- Thygesen, L.C.; Møller, S.P.; Ersbøll, A.K.; Santini, Z.I.; Nielsen, M.B.D.; Grønbæk, M.K.; Ekholm, O. Decreasing mental well-being during the COVID-19 pandemic: A longitudinal study among Danes before and during the pandemic. J. Psychiatr. Res. 2021, 144, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Lotzin, A.; Acquarini, E.; Ajdukovic, D.; Ardino, V.; Böttche, M.; Bondjers, K.; Bragesjö, M.; Dragan, M.; Grajewski, P.; Figueiredo-Braga, M.; et al. Stressors, coping and symptoms of adjustment disorder in the course of the COVID-19 pandemic—Study protocol of the European Society for Traumatic Stress Studies (ESTSS) pan-European study. Eur. J. Psychotraumatol. 2020, 11, 1780832. [Google Scholar] [CrossRef]
- Looi, M.-K. Covid-19: Is a second wave hitting Europe? BMJ 2020, 371, m4113. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus (accessed on 23 March 2023).
- Helliwell, J.F.; Layard, R.; Sachs, J.D.; De Neve, J.-E.; Aknin, L.B.; Wang, S. World Happiness Report 2022; Sustainable Development Solutions Network: New York, NY, USA, 2022; ISBN 978-1-7348080-2-5. [Google Scholar]
- Ivanović, V.; Šimac, B.; Trako Poljak, T. Subjective wellbeing in rural and urban central Europe: Evidence from the European Social Survey (2008 and 2018). Int. J. Sociol. 2022, 52, 397–419. [Google Scholar] [CrossRef]
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 30 August 2023).
- Bonanno, G.A.; Westphal, M.; Mancini, A.D. Resilience to loss and potential trauma. Annu. Rev. Clin. Psychol. 2011, 7, 511–535. [Google Scholar] [CrossRef] [PubMed]
- Tao, T.J.; Liang, L.; Liu, H.; Hobfoll, S.E.; Hou, W.K.; Bonanno, G.A. The interrelations between psychological outcome trajectories and resource changes amid large-scale disasters: A growth mixture modeling analysis. Transl. Psychiatry 2023, 13, 57. [Google Scholar] [CrossRef] [PubMed]
- Kazlauskas, E.; Gegieckaite, G.; Eimontas, J.; Zelviene, P.; Maercker, A. A brief measure of the International Classification of Diseases-11 adjustment disorder: Investigation of psychometric properties in an adult help-seeking sample. Psychopathology 2018, 51, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Ben-Ezra, M.; Mahat-Shamir, M.; Lorenz, L.; Lavenda, O.; Maercker, A. Screening of adjustment disorder: Scale based on the ICD-11 and the Adjustment Disorder New Module. J. Psychiatr. Res. 2018, 103, 91–96. [Google Scholar] [CrossRef]
- Truskauskaite-Kuneviciene, I.; Kazlauskas, E.; Ostreikaite-Jurevice, R.; Brailovskaia, J.; Margraf, J. Positive mental health and adjustment following life-stressors among young adults. Curr. Psychol. 2022, 41, 1951–1956. [Google Scholar] [CrossRef]
- WHO. WHO (Five) Well-Being Index; WHO Regional office for Europe: Hillerod, Denmark, 1998. [Google Scholar]
- Krieger, T.; Zimmermann, J.; Huffziger, S.; Ubl, B.; Diener, C.; Kuehner, C.; Grosse Holtforth, M. Measuring depression with a well-being index: Further evidence for the validity of the WHO Well-Being Index (WHO-5) as a measure of the severity of depression. J. Affect. Disord. 2014, 156, 240–244. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Toffolutti, V.; Plach, S.; Maksimovic, T.; Piccitto, G.; Mascherini, M.; Mencarini, L.; Aassve, A. The association between COVID-19 policy responses and mental well-being: Evidence from 28 European countries. Soc. Sci. Med. 2022, 301, 114906. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. An ultra-brief screening scale for anxiety and depression: The PHQ-4. Psychosomatics 2009, 50, 613–621. [Google Scholar] [CrossRef]
- Löwe, B.; Wahl, I.; Rose, M.; Spitzer, C.; Glaesmer, H.; Wingenfeld, K.; Schneider, A.; Brähler, E. A 4-item measure of depression and anxiety: Validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J. Affect. Disord. 2010, 122, 86–95. [Google Scholar] [CrossRef]
- Marvaldi, M.; Mallet, J.; Dubertret, C.; Moro, M.R.; Guessoum, S.B. Anxiety, depression, trauma-related, and sleep disorders among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 126, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Eisinga, R.; te Grotenhuis, M.; Pelzer, B. The reliability of a two-item scale: Pearson, Cronbach, or Spearman-Brown? Int. J. Public Health 2013, 58, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Haucke, M.N.; Heinzel, S.; Heinz, A. Long-Term Impact of Economic Downturn and Loneliness on Psychological Distress: Triple Crises of COVID-19 Pandemic. J. Clin. Med. 2021, 10, 4596. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Kan, M.-Y. The varying impacts of COVID-19 and its related measures in the UK: A year in review. PLoS ONE 2021, 16, e0257286. [Google Scholar] [CrossRef]
- Kazlauskas, E.; Elklit, A.; Truskauskaite, I. A Longitudinal Course of ICD-11 Adjustment Disorder Symptom Profiles: A 12-Month Follow-Up Study. Psychopathology 2022, 55, 373–381. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 27.0; IBM Corp.: Armonk, NY, USA, 2020. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- West, S.G.; Taylor, A.B.; Wu, W. Model fit and model selection in structural equation modeling. In Handbook of Structural Equation Modeling; Hoyle, R.H., Ed.; Guilford Press: New York, NY, USA, 2012; pp. 209–231. ISBN 9781606230770. [Google Scholar]
- Little, T.D.; Card, N.A. Longitudinal Structural Equation Modeling; The Guilford Press: New York, NY, USA; London, UK, 2013; ISBN 9781462510160. [Google Scholar]
- Putnick, D.L.; Bornstein, M.H. Measurement invariance conventions and reporting: The state of the art and future directions for psychological research. Dev. Rev. 2016, 41, 71–90. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA; London, UK, 2016; ISBN 9781462523344. [Google Scholar]
- Li, C.-H. Confirmatory factor analysis with ordinal data: Comparing robust maximum likelihood and diagonally weighted least squares. Behav. Res. Methods 2016, 48, 936–949. [Google Scholar] [CrossRef]
- Rosseel, Y. lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Curran, P.J.; Obeidat, K.; Losardo, D. Twelve frequently asked questions about growth curve modeling. J. Cogn. Dev. 2010, 11, 121–136. [Google Scholar] [CrossRef]
- Newsom, J.T. Longitudinal Structural Equation Modeling; Routledge: New York, NY, USA; East Sussex, UK, 2015; ISBN 9781317975359. [Google Scholar]
- Bollen, K.A.; Curran, P.J. Latent Curve Models: A Structural Equation Perspective; Wiley-Interscience: Hoboken, NJ, USA, 2006; ISBN 978-0-471-45592-9. [Google Scholar]
- Preacher, K.; Wichman, A.; MacCallum, R.; Briggs, N. Latent Growth Curve Modeling; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2008; ISBN 9781412939553. [Google Scholar]
- Gana, K. Structural Equation with Lavaan; John Wiley & Sons Incorporated: Newark, NJ, USA, 2018; ISBN 978-1-786-30369-1. [Google Scholar]
- Rosseel, Y. The Lavaan Tutorial; Department of Data Analysis, Ghent University: Ghent, Belgium, 2023; Available online: https://lavaan.ugent.be/tutorial/tutorial.pdf (accessed on 31 July 2023).
- Little, T.D.; Jorgensen, T.D.; Lang, K.M.; Moore, E.W.G. On the joys of missing data. J. Pediatr. Psychol. 2014, 39, 151–162. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 0805802835. [Google Scholar]
- Berlin, K.S.; Parra, G.R.; Williams, N.A. An introduction to latent variable mixture modeling (part 2): Longitudinal latent class growth analysis and growth mixture models. J. Pediatr. Psychol. 2014, 39, 188–203. [Google Scholar] [CrossRef] [PubMed]
- Levin, Y.; Bachem, R.; Hyland, P.; Karatzias, T.; Shevlin, M.; Ben-Ezra, M.; Maercker, A. Validation of the International Adjustment Disorder Questionnaire in Israel and Switzerland. Clin. Psychol. Psychother. 2022, 29, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Fineberg, N.A.; Pellegrini, L.; Wellsted, D.; Hall, N.; Corazza, O.; Giorgetti, V.; Cicconcelli, D.; Theofanous, E.; Sireau, N.; Adam, D.; et al. Facing the “new normal”: How adjusting to the easing of COVID-19 lockdown restrictions exposes mental health inequalities. J. Psychiatr. Res. 2021, 141, 276–286. [Google Scholar] [CrossRef]
- Gersons, B.P.R.; Smid, G.E.; Smit, A.S.; Kazlauskas, E.; McFarlane, A.C. Can a ‘second disaster’ during and after the COVID-19 pandemic be mitigated? Eur. J. Psychotraumatol. 2020, 11, 1815283. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Bi, K.; Sun, P.; Bonanno, G.A. Psychopathology and resilience following strict COVID-19 lockdowns in Hubei, China: Examining person- and context-level predictors for longitudinal trajectories. Am. Psychol. 2022, 77, 262–275. [Google Scholar] [CrossRef]
- Sandbakken, E.M.; Moss, S.M. “Now we are all in the same boat. At the same time, we are not.” Meaning-making and coping under COVID-19 lockdown in Norway. Hum. Arenas 2021, 6, 201–225. [Google Scholar] [CrossRef]
- Zrnić Novaković, I.; Ajduković, D.; Bakić, H.; Borges, C.; Figueiredo-Braga, M.; Lotzin, A.; Anastassiou-Hadjicharalambous, X.; Lioupi, C.; Javakhishvili, J.D.; Tsiskarishvili, L.; et al. Shaped by the COVID-19 pandemic: Psychological responses from a subjective perspective-A longitudinal mixed-methods study across five European countries. PLoS ONE 2023, 18, e0285078. [Google Scholar] [CrossRef]
- Spanovic Kelber, M.; Morgan, M.A.; Beech, E.H.; Smolenski, D.J.; Bellanti, D.; Galloway, L.; Ojha, S.; Otto, J.L.; Wilson, A.L.G.; Bush, N.; et al. Systematic review and meta-analysis of predictors of adjustment disorders in adults. J. Affect. Disord. 2022, 304, 43–58. [Google Scholar] [CrossRef]
- Morales-Vives, F.; Dueñas, J.-M.; Vigil-Colet, A.; Camarero-Figuerola, M. Psychological variables related to adaptation to the COVID-19 lockdown in Spain. Front. Psychol. 2020, 11, 565634. [Google Scholar] [CrossRef]
- Esterwood, E.; Saeed, S.A. Past epidemics, natural disasters, COVID19, and mental health: Learning from history as we deal with the present and prepare for the future. Psychiatr. Q. 2020, 91, 1121–1133. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Jovanović, V. Evaluation of domain satisfaction measure in cross-national perspective: Evidence from Austria and four countries of the former Yugoslavia. Soc. Indic. Res. 2018, 141, 1369–1385. [Google Scholar] [CrossRef]
- Grané, A.; Albarrán, I.; Merchán, D.E. Impact of Pandemic on European Well-Being: Visualizing Scenarios from the SHARE Database. Int. J. Environ. Res. Public Health 2021, 18, 4620. [Google Scholar] [CrossRef] [PubMed]
- Gizdic, A.; Baxter, T.; Barrantes-Vidal, N.; Park, S. Loneliness and psychosocial predictors of psychosis-proneness during COVID-19: Preliminary findings from Croatia. Psychiatry Res. 2022, 317, 114900. [Google Scholar] [CrossRef] [PubMed]
- Romic, I.; Silovski, H.; Mance, M.; Pavlek, G.; Petrovic, I.; Figl, J.; Grbavac, D.; Moric, T.; Romic, R.; Bakula, B.; et al. Psychological effects of “double crisis” (COVID-19 pandemic and earthquakes) on Croatian medical students. Psychiatr. Danub. 2021, 33, 120–125. [Google Scholar]
- Matić, I.; Takšić, I.; Božičević, M. The sense of coherence and subjective well-being as resources of resilience in the time of stressful situations: COVID-19 outbreak and earthquakes. Psychiatr. Danub. 2021, 33, 639–645. [Google Scholar] [CrossRef]
- UN General Assembly. Transforming Our World: The 2030 Agenda for Sustainable Development; A/RES/70/1; 2015. Available online: https://undocs.org/en/A/RES/70/1 (accessed on 18 September 2023).
- Ehlers, A.; Wild, J.; Warnock-Parkes, E.; Grey, N.; Murray, H.; Kerr, A.; Rozental, A.; Thew, G.; Janecka, M.; Beierl, E.T.; et al. Therapist-assisted online psychological therapies differing in trauma focus for post-traumatic stress disorder (STOP-PTSD): A UK-based, single-blind, randomised controlled trial. Lancet Psychiatry 2023, 10, 608–622. [Google Scholar] [CrossRef]
- Salza, A.; Giusti, L.; Ussorio, D.; Casacchia, M.; Roncone, R. Cognitive behavioral therapy (CBT) anxiety management and reasoning bias modification in young adults with anxiety disorders: A real-world study of a therapist-assisted computerized (TACCBT) program vs. “person-to-person” group CBT. Internet Interv. 2020, 19, 100305. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| T1 | T2 | T3 | T4 | |||||
|---|---|---|---|---|---|---|---|---|
| Austria | Croatia | Austria | Croatia | Austria | Croatia | Austria | Croatia | |
| Recruitment period | 27 June 2020– 22 September 2020 | 15 June 2020– 16 August 2020 | 14 January 2021– 29 March 2021 | 30 November 2020– 7 January 2021 | 13 July 2021– 8 October 2021 | 21 June 2021– 26 July 2021 | 26 November 2021– 13 December 2021 a | 8 December 2021– 11 January 2022 |
| Duration of data collection | 88 days ≈ 13 weeks | 63 days ≈ 9 weeks | 75 days ≈ 11 weeks | 39 days ≈ 6 weeks | 88 days ≈ 13 weeks | 36 days ≈ 5 weeks | 18 days ≈ 3 weeks | 35 days ≈ 5 weeks |
| Stringency index | ||||||||
| M (SD) | 38.59 | 44.98 | 77.58 | 58.57 | 50.11 | 35.19 | 51.70 | 36.97 |
| Range | 36.11–50.00 | 35.19–54.63 | 73.15–82.41 | 47.22–67.59 | 46.23–55.05 | 30.49–41.67 | 49.30–52.06 | 33.26–38.08 |
| Incidence | ||||||||
| M (SD) | 24.73 (20.42) | 14.55 (7.20) | 214.75 (67.75) | 639.83 (243.16) | 126.58 (72.32) | 22.81 (5.40) | 413.46 (418.22) | 613.41 (350.14) |
| Range | 4.25–83.34 | 0.18–31.09 | 142.82–351.49 | 276.26–905.02 | 17.45–232.98 | 16.91–36.37 | 0.00–1257.42 | 0.00–981.76 |
| Deaths | ||||||||
| M (SD) | 0.19 (0.06) | 0.22 (0.19) | 4.57 (1.38) | 16.35 (1.92) | 0.59 (0.43) | 0.59 (0.29) | 7.50 (0.34) | 12.15 (1.88) |
| Range | 0.06–0.37 | 0.00–0.60 | 3.02–7.34 | 12.73–19.57 | 0.16–1.37 | 0.25–1.49 | 6.76–7.86 | 9.39–15.24 |
| Total Sample N = 1144 | Austria n = 415 | Croatia n = 729 | |
|---|---|---|---|
| Age | M = 44.0 SD = 13.5 | M = 46.5 SD = 14.7 | M = 42.7 SD = 12.6 |
| n (%) | n (%) | n (%) | |
| Gender a | |||
| Male | 300 (26.2) | 128 (30.8) | 172 (23.6) |
| Female | 841 (73.6) | 285 (68.7) | 556 (76.4) |
| Other | 2 (0.2) | 2 (0.5) | 0 (0.0) |
| Education | |||
| Low | 6 (0.5) | 5 (1.2) | 1 (0.1) |
| Middle | 306 (26.7) | 166 (40.0) | 140 (19.2) |
| High | 832 (72.7) | 244 (58.8) | 588 (80.7) |
| Income b | |||
| Very low | 126 (11.3) | 43 (11.2) | 83 (11.4) |
| Low | 346 (31.1) | 140 (36.5) | 206 (28.3) |
| Medium | 344 (30.9) | 31 (8.1) | 313 (43.0) |
| High | 296 (26.6) | 170 (44.3) | 126 (17.3) |
| Relationship status | |||
| Single | 269 (23.5) | 102 (24.6) | 167 (22.9) |
| In a relationship | 875 (76.5) | 313 (75.4) | 562 (77.1) |
| Employment status c | |||
| Training/Study | 124 (25.5) | 52 (12.5) | 72 (9.9) |
| Employed part-time | 154 (34.5) | 122 (29.4) | 32 (4.4) |
| Employed full-time | 742 (77.0) | 193 (46.5) | 549 (75.3) |
| Self-employed | 68 (15.2) | 36 (8.7) | 32 (4.4) |
| Retired | 84 (19.0) | 57 (13.7) | 27 (3.7) |
| Job-seeking | 57 (12.3) | 8 (1.9) | 49 (6.7) |
| Other | 26 (6.0) | 10 (2.4) | 16 (2.2) |
| Diagnosis of a mental disorder | |||
| Yes | 167 (14.6) | 96 (23.1) | 71 (9.7) |
| No | 977 (85.4) | 319 (76.9) | 658 (90.3) |
| Timepoint | ADNM-8 | PHQ-2 | GAD-2 | WHO-5 a | ||||
|---|---|---|---|---|---|---|---|---|
| M (SD) | % (n) | M (SD) | % (n) | M (SD) | % (n) | M (SD) | % (n) | |
| T1 n = 1144 | 14.3 (5.3) | 9.8 (112) | 1.3 (1.5) | 15.4 (176) | 1.4 (1.3) | 15.8 (181) | 58.0 (21.4) | 33.7 (386) |
| T2 n = 993 | 15.8 (5.7) | 15.1 (150) | 1.5 (1.5) | 16.2 (161) | 1.3 (1.5) | 15.5 (154) | 51.5 (22.1) | 45.1 (448) |
| T3 n = 837 | 14.3 (5.4) | 9.9 (83) | 1.2 (1.4) | 12.9 (108) | 1.1 (1.4) | 11.6 (97) | 57.3 (21.6) | 34.5 (289) |
| T4 n = 674 | 15.0 (5.6) | 11.7 (79) | 1.3 (1.6) | 16.2 (109) | 1.3 (1.5) | 14.5 (98) | 53.8 (22.7) | 40.8 (275) |
| Univariate Unconditional Model | Univariate Conditional Model with TICs | Univariate Conditional Model with TVCs | Univariate Model with TICs and TVCs | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| AD | WB | AD | WB | AD | WB | AD | WB | |||
| Fit indices | ||||||||||
| Χ2 (df) | 105.89 *** (5) | 136.80 *** (5) | 131.84 *** (15) | 158.36 *** (15) | 148.70 *** (29) | 140.68 *** (29) | 169.82 *** (39) | 147.65 *** (39) | ||
| CFI | 0.933 | 0.925 | 0.929 | 0.924 | 0.925 | 0.940 | 0.919 | 0.941 | ||
| TLI | 0.919 | 0.910 | 0.876 | 0.869 | 0.901 | 0.921 | 0.879 | 0.912 | ||
| RMSEA [90% CI] | 0.165 [0.136, 0.196] | 0.182 [0.153, 0.213] | 0.101 [0.084, 0.119] | 0.107 [0.091, 0.125] | 0.097 [0.082, 0.113] | 0.091 [0.076, 0.107] | 0.089 [0.075, 0.103] | 0.078 [0.065, 0.092] | ||
| SRMR | 0.063 | 0.068 | 0.034 | 0.037 | 0.119 | 0.106 | 0.085 | 0.070 | ||
| Parameter estimates (SE) | ||||||||||
| Intercept | 14.57 *** (0.16) | 56.77 *** (0.64) | 16.34 *** (1.28) | 39.88 *** (4.70) | 11.73 *** (0.22) | 69.32 *** (0.85) | 10.78 *** (1.34) | 61.49 *** (5.17) | ||
| Slope | 0.15 * (0.06) | −1.10 *** (0.22) | 0.17 (0.47) | −2.76 (1.67) | 0.24 ** (0.09) | −1.34 *** (0.30) | −0.33 (0.56) | −0.76 (1.84) | ||
| Covariances (SE) | ||||||||||
| i ~~ s | −0.78 (0.51) | 8.31 (6.71) | −0.97 † (0.50) | 5.98 (6.86) | 0.17 (0.37) | 4.04 (5.05) | 0.07 (0.37) | 2.85 (5.10) | ||
| Variances (SE) | ||||||||||
| Intercept | 18.87 *** (1.38) | 286.64 *** (19.74) | 18.31 *** (1.36) | 274.99 *** (20.02) | 7.13 *** (1.11) | 114.14 *** (14.58) | 6.52 *** (1.16) | 115.11 *** (14.53) | ||
| Slope | 1.24 *** (0.30) | 3.66 (3.80) | 1.30 *** (0.29) | 3.78 (3.82) | 0.59* (0.23) | 0.83 (2.88) | 0.58 * (0.23) | 1.47 (2.94) | ||
| TICs (SE) | ||||||||||
| Gender | - | - | i: s: | 1.25 ** (0.37) 0.04 (0.13) | −1.55 (1.48) −0.52 (0.49) | - | - | 1.10 ** (0.39) 0.04 (0.15) | −0.88 (1.60) −0.09 (0.51) | |
| Age | - | - | i: s: | −0.00 (0.01) 0.01 (0.00) | 0.22 *** (0.05) −0.00 (0.02) | - | - | 0.04 ** (0.01) 0.01 (0.01) | 0.11 * (0.05) −0.01 (0.02) | |
| Country | - | - | i: s: | −1.12 ** (0.35) −0.09 (0.14) | 4.04 ** (1.36) 0.93 † (0.47) | - | - | −0.81 * (0.38) −0.00 (0.15) | 2.75 † (1.40) −0.42 (0.50) | |
| Education | - | - | i: s: | −0.64 (0.39) −0.08 (0.16) | −0.01 (1.52) 0.57 (0.56) | - | - | −0.42 (0.44) 0.05 (0.18) | 0.51 (1.76) 0.34 (0.58) | |
| Income | - | - | i: s: | −0.51 ** (0.17) −0.01 (0.07) | 1.86 ** (0.67) 0.08 (0.23) | - | - | −0.36 † (0.19) 0.03 (0.08) | −0.57 (0.70) 0.14 (0.25) | |
| TVCs (SE) | ||||||||||
| T1 | Depression Anxiety | - | - | - | - | 1.00 *** (0.17) 1.01 *** (0.17) | −5.28 *** (0.52) −3.25 *** (0.48) | 0.98 *** (0.17) 1.00 *** (0.18) | −4.99 *** (0.53) −3.42 *** (0.48) | |
| T2 | Depression Anxiety | - | - | - | - | 1.29 *** (0.17) 1.31 *** (0.18) | −6.31 *** (0.54) −4.54 *** (0.53) | 1.26 *** (0.18) 1.32 *** (0.18) | −6.30 *** (0.55) −4.46 *** (0.55) | |
| T3 | Depression Anxiety | - | - | - | - | 0.85 *** (0.17) 1.27 *** (0.17) | −5.63 *** (0.62) −2.97 *** (0.67) | 0.94 *** (0.17) 1.16 *** (0.17) | −5.39 *** (0.64) −3.23 *** (0.68) | |
| T4 | Depression Anxiety | - | - | - | - | 0.94 *** (0.14) 1.01 *** (0.15) | −6.03 *** (0.58) −3.23 *** (0.59) | 0.96 *** (0.15) 1.04 *** (0.16) | −5.92 *** (0.62) −3.36 *** (0.62) | |
| Multivariate Unconditional Model a | Multivariate Conditional Model (All Predictors) | ||||
|---|---|---|---|---|---|
| Fit indices | |||||
| Χ2 (df) | 188.49 *** (21) | 310.69 *** (89) | |||
| CFI | 0.978 | 0.937 | |||
| TLI | 0.971 | 0.906 | |||
| RMSEA [90% CI] | 0.081 [0.071, 0.092] | 0.075 [0.066, 0.084] | |||
| SRMR | 0.060 | 0.103 | |||
| Parameter estimates (SE) | |||||
| Intercept | adnm_i: 14.58 *** (0.22) | well_i: 57.33 *** (0.86) | adnm_i: 10.86 *** (1.36) | well_i: 61.39 *** (5.21) | |
| Slope | adnm_s: 0.10 (0.07) | well_s: −1.03 *** (0.25) | adnm_s: −0.35 (0.56) | well_s: −0.92 (1.83) | |
| Covariances (SE) | |||||
| adnm_i ~~ adnm_s | −0.85 (0.55) | 0.09 (0.37) | |||
| well_i ~~ well_s | 9.08 (6.69) | 3.02 (5.04) | |||
| adnm_i ~~ well_i | −52.34 *** (5.45) | −7.41 * (3.10) | |||
| adnm_s ~~ well_s | −1.19 * (0.55) | 0.04 (0.38) | |||
| Variances (SE) | |||||
| Intercept | adnm: 20.18 *** (1.94) | well: 277.56 *** (24.23) | adnm: 6.65 *** (1.18) | well: 116.78 *** (14.73) | |
| Slope | adnm: 1.33 *** (0.35) | well: 4.66 (3.99) | adnm: 0.52 * (0.23) | well: 0.98 (2.88) | |
| Time-invariant covariates (SE) | |||||
| Gender | - | - | adnm_i: 1.13 ** (0.40) adnm_s: 0.03 (0.15) | well_i: −0.94 (1.60) well_s: −0.07 (0.52) | |
| Age | - | - | adnm_i: 0.04 ** (0.01) adnm_s: 0.01 (0.01) | well_i: 0.11 * (0.05) well_s: −0.01 (0.02) | |
| Country | - | - | adnm_i: −0.82 * (0.38) adnm_s: 0.01 (0.15) | well_i: 2.74 † (1.40) well_s: −0.39 (0.50) | |
| Education | - | - | adnm_i: −0.43 (0.44) adnm_s: 0.05 (0.18) | well_i: 0.54 (1.76) well_s: 0.32 (0.58) | |
| Income | - | - | adnm_i: −0.37 † (0.19) adnm_s: 0.03 (0.08) | well_i: −0.56 (0.71) well_s: 0.16 (0.25) | |
| Time-varying covariates (SE) | Adjustment disorder | Well-being | |||
| T1 | Depression Anxiety | 0.96 *** (0.18) 0.98 *** (0.18) | −4.95 *** (0.53) −3.37 *** (0.49) | ||
| T2 | Depression Anxiety | 1.24 *** (0.18) 1.30 *** (0.18) | −6.26 *** (0.56) −4.38 *** (0.56) | ||
| T3 | Depression Anxiety | 0.93 *** (0.17) 1.15 *** (0.17) | −5.31 *** (0.63) −3.15 *** (0.68) | ||
| T4 | Depression Anxiety | 0.94 *** (0.15) 1.04 *** (0.16) | −5.86 *** (0.61) −3.22 *** (0.61) | ||
| Austria | Croatia a | ||||
|---|---|---|---|---|---|
| Fit indices | |||||
| Χ2 (df) | 185.19 *** (85) | 229.42 *** (84) | |||
| CFI | 0.932 | 0.938 | |||
| TLI | 0.901 | 0.908 | |||
| RMSEA [90% CI] | 0.081 [0.064, 0.097] | 0.076 [0.064, 0.088] | |||
| SRMR | 0.109 | 0.112 | |||
| Parameter estimates (SE) | |||||
| Intercept | adnm_i: 9.93 *** (2.00) | well_i: 61.37 *** (7.59) | adnm_i: 9.44 *** (1.50) | well_i: 76.33 *** (6.85) | |
| Slope | adnm_s: 0.12 (0.91) | well_s: −3.28 (2.49) | adnm_s: −0.84 (0.57) | well_s: −7.05 (4.81) | |
| Covariances (SE) | |||||
| adnm_i ~~ adnm_s | −0.13 (0.71) | 0.10 (0.39) | |||
| well_i ~~ well_s | −2.82 (10.05) | −3.90 (29.67) | |||
| adnm_i ~~ well_i | −13.05 * (6.59) | −2.72 (3.10) | |||
| adnm_s ~~ well_s | 0.40 (0.77) | −0.72 (1.53) | |||
| Variances (SE) | |||||
| Intercept | adnm: 6.93 ** (2.17) | well: 156.40 *** (28.84) | adnm: 6.46 *** (1.27) | well: 100.84 ** (34.12) | |
| Slope | adnm: 0.85 † (0.45) | well: 3.37 (5.56) | adnm: 0.36 (0.21) | well: 16.97 (34.22) | |
| Time-invariant covariates (SE) | |||||
| Gender | adnm_i: 0.98 (0.66) adnm_s: −0.14 (0.27) | well_i: 2.27 (2.49) well_s: 1.25 (0.83) | adnm_i: 1.09 * (0.48) adnm_s: 0.23 (0.16) | well_i: −4.37 (2.38) well_s: −1.08 (1.87) | |
| Age | adnm_i: 0.06 ** (0.02) adnm_s: 0.00 (0.01) | well_i: 0.08 (0.08) well_s: −0.02 (0.02) | adnm_i: 0.03 (0.02) adnm_s: 0.01 (0.01) | well_i: 0.07 (0.07) well_s: 0.04 (0.05) | |
| Education | adnm_i: −0.62 (0.63) adnm_s: −0.01 (0.30) | well_i: 0.82 (2.43) well_s: 0.13 (0.80) | adnm_i: −0.35 (0.62) adnm_s: 0.14 (0.21) | well_i: 0.90 (2.62) well_s: −0.12 (1.92) | |
| Income | adnm_i: −0.64 * (0.28) adnm_s: 0.08 (0.12) | well_i: −0.14 (1.02) well_s: 0.07 (0.33) | adnm_i: −0.08 (0.25) adnm_s: −0.05 (0.09) | well_i: −1.31 (1.06) well_s: 1.25 (0.91) | |
| Time-varying covariates (SE) | Adjustment disorder | Well-being | Adjustment disorder | Well-being | |
| T1 | Depression Anxiety | 0.90 ** (0.31) 1.54 *** (0.31) | −5.36 *** (0.83) −5.09 *** (0.85) | 0.93 *** (0.21) 0.75 *** (0.19) | −5.00 *** (0.68) −3.42 *** (0.61) |
| T2 | Depression Anxiety | 1.61 *** (0.26) 1.18 *** (0.26) | −7.72 *** (0.85) −4.33 *** (0.84) | 0.92 *** (0.23) 1.45 *** (0.25) | −4.24 *** (0.70) −3.55 *** (0.74) |
| T3 | Depression Anxiety | 0.75 * (0.29) 1.70 *** (0.25) | −5.21 *** (0.82) −4.57 *** (1.01) | 1.10 *** (0.20) 0.69 ** (0.21) | −5.55 *** (0.88) −2.07 ** (0.94) |
| T4 | Depression Anxiety | 1.37 *** (0.26) 1.11 *** (0.27) | −6.59 *** (1.02) −3.27 *** (0.94) | 0.53 ** (0.19) 1.03 *** (0.20) | −5.24 *** (0.73) −3.59 *** (0.78) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zrnić Novaković, I.; Streicher, A.; Ajduković, D.; Ajduković, M.; Kiralj Lacković, J.; Lotzin, A.; Lueger-Schuster, B. Trajectories of Adjustment Disorder and Well-Being in Austria and Croatia during 20 Months of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 6861. https://doi.org/10.3390/ijerph20196861
Zrnić Novaković I, Streicher A, Ajduković D, Ajduković M, Kiralj Lacković J, Lotzin A, Lueger-Schuster B. Trajectories of Adjustment Disorder and Well-Being in Austria and Croatia during 20 Months of the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2023; 20(19):6861. https://doi.org/10.3390/ijerph20196861
Chicago/Turabian StyleZrnić Novaković, Irina, Alina Streicher, Dean Ajduković, Marina Ajduković, Jana Kiralj Lacković, Annett Lotzin, and Brigitte Lueger-Schuster. 2023. "Trajectories of Adjustment Disorder and Well-Being in Austria and Croatia during 20 Months of the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 20, no. 19: 6861. https://doi.org/10.3390/ijerph20196861
APA StyleZrnić Novaković, I., Streicher, A., Ajduković, D., Ajduković, M., Kiralj Lacković, J., Lotzin, A., & Lueger-Schuster, B. (2023). Trajectories of Adjustment Disorder and Well-Being in Austria and Croatia during 20 Months of the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 20(19), 6861. https://doi.org/10.3390/ijerph20196861