
Use of General Health Examination and Cancer Screening among People with Disability Who Need Support from Others: Analysis of the 2016 Comprehensive Survey of Living Conditions in Japan


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Overview of the Preventive Healthcare Service in Japan
2.3. Data Source
2.4. Inclusion and Exclusion Criteria
2.5. Outcome Variables
- Did you receive a GHE in the last year? (Answer option: Yes or No)
- Did you receive a gastric cancer screening (barium swallow test or endoscopic examination) in the last year? (Answer option: Yes or No). As mentioned earlier, recommended frequency for the gastric cancer varied based on the type of examination: X-ray annually or endoscopic examination every two years. However, in the CSLC in 2016, the questionnaire item only enquired the use of gastric cancer screening in the last year; no questionnaire item enquired of the use of the examination in the last two years. Thus, we used this questionnaire item as an outcome variable for gastric cancer screening.
- Did you receive a lung cancer screening (chest X-ray or sputum examination) in the last year? (Answer option: Yes or No)
- Did you receive a colorectal cancer screening (Fecal occult blood tests) in the last year? (Answer option: Yes or No)
- Did you receive a breast cancer screening (mammography or breast ultrasound) in the last two years? (Answer option: Yes or No)
- Did you receive a cervical cancer screening (Pap Smear) in the last two years? (Answer option: Yes or No).
2.6. Explanatory and Cofounding Variables
- Do you need any support or supervision from others due to your disability or declining physical function? (Answer option: Yes or No).We considered individuals to be people with disability if they answered “Yes”.
- Sex (male, female).
- Age. The data for age were categorized into three groups: group one, those who were not eligible for GHE and cancer screening (specifically 20 to 40 or 50 years old, depending on the outcome variables); group 2, those who were eligible for GHE and cancer screening (specifically older than 40 or 50 years old, depended on the outcome variables); group 3, those who were eligible for GHE and cancer screening and 65 years and older. The age of 65 is used as a common threshold of elderly age in policy making as well as the research community in Japan. Thus, we divided the data from individuals eligible for GHE and cancer screening into two groups using the age threshold of 65 years old.
- Marital status (married, single, divorced/widowed).
- Educational qualification (primary/junior high school, high school, vocational school/junior college/community (technical) college/university/post-graduate school).
- Constant visits to hospitals or clinics, including for dentistry, acupuncture, moxibustion, Japanese massage or Judo therapy (Yes/No). The “constant visit” means regular visit to the hospital or other facilities. Unfortunately, clear definition of frequency (e.g., once a week or once a month) was not described in the questionnaire of the CSLC.
- Subjective health status (good, normal, bad).
- Alcohol consumption (never drank or quit drinking, social drinker/low-risk group (>0 to ≤100 g/week); middle-risk drinking (>100 to ≤350 g/week); high-risk drinking (>350 g/week)) [31].
- Smoking habit (never/ex-smoker, current smoker).
- Subjective financial state (wealthy; not poor, not wealthy; poor).
- Kessler Psychological Distress Scale (K6), a measure of mood and anxiety disorder (normal (total score ≤ 4), mild illness (5 to 12), severe illness (13 ≥ total score)) [31].
- Health insurance (National Health Insurance, employee insurance, other).
- Employment status (employed, self-employed, employed (other), unemployed).
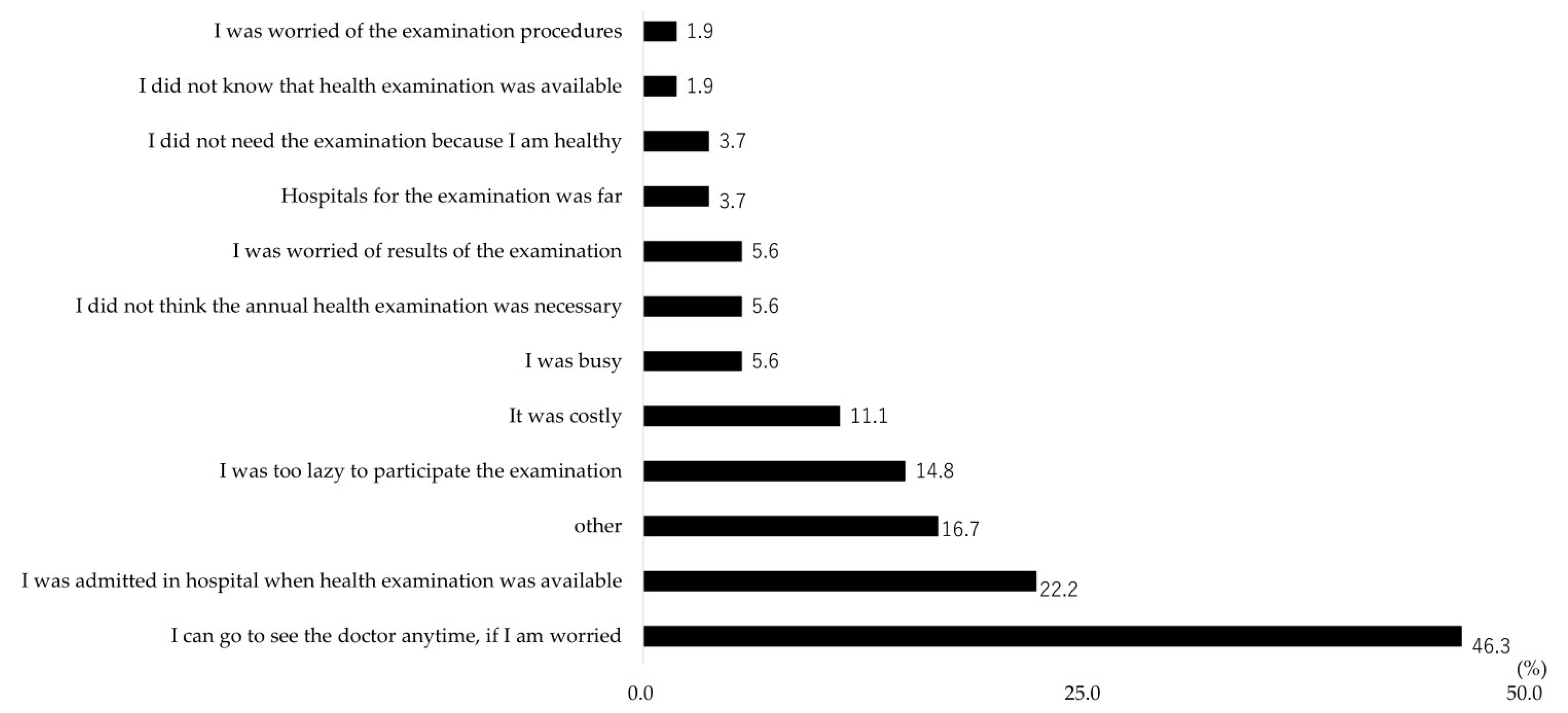
2.7. Reasons of Non-Participation in the General Health Examination
2.8. Statistical Analysis
3. Results
4. Discussion
4.1. Key Points
4.2. Association between Disability and Preventive Healthcare Service Use in Japan
4.3. Reasons for Non-Participation in the General Health Examination
4.4. Implication for Future Studies Aiming to Eliminate Disability-Based Disparity in Preventive Service Utilization
4.5. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reinehr, T.; Dobe, M.; Winkel, K.; Schaefer, A.; Hoffmann, D. Obesity in disabled children and adolescents: An overlooked group of patients. Dtsch. Arztebl. Int. 2010, 107, 268–275. [Google Scholar] [PubMed]
- Rimmer, J.H.; Wang, E. Obesity prevalence among a group of Chicago residents with disabilities. Arch. Phys. Med. Rehabil. 2005, 86, 1461–1464. [Google Scholar] [CrossRef] [PubMed]
- Emerson, E. Smoking among adults with and without disabilities in the UK. J. Public Health 2018, 40, e502–e509. [Google Scholar] [CrossRef] [PubMed]
- Havercamp, S.M.; Scandlin, D.; Roth, M. Health disparities among adults with developmental disabilities, adults with other disabilities, and adults not reporting disability in North Carolina. Public Health Rep. 2004, 119, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Wilber, N.; Mitra, M.; Walker, D.K.; Allen, D.; Meyers, A.R.; Tupper, P. Disability as a public health issue: Findings and reflections from the Massachusetts survey of secondary conditions. Milbank Q. 2002, 80, 393–421. [Google Scholar] [CrossRef]
- Coyle, C.P.; Santiago, M.C.; Shank, J.W.; Ma, G.X.; Boyd, R. Secondary conditions and women with physical disabilities: A descriptive study. Arch. Phys. Med. Rehabil. 2000, 81, 1380–1387. [Google Scholar] [CrossRef]
- Son, K.Y.; Kim, S.H.; Sunwoo, S.; Lee, J.Y.; Lim, S.; Kim, Y.S. Association between disability and cardiovascular event and mortality: A nationwide representative longitudinal study in Korea. PLoS ONE 2020, 15, e0236665. [Google Scholar] [CrossRef]
- Kposowa, A.J.; Breault, K. Disability status, unemployment, and alcohol-related liver disease (ALD) mortality: A large sample individual level longitudinal study. Subst. Abuse Rehabil. 2021, 12, 81–88. [Google Scholar] [CrossRef]
- Lin, E.; Balogh, R.; Chung, H.; Dobranowski, K.; Durbin, A.; Volpe, T.; Lunsky, Y. Looking across health and healthcare outcomes for people with intellectual and developmental disabilities and psychiatric disorders: Population-based longitudinal study. Br. J. Psychiatry 2021, 218, 51–57. [Google Scholar] [CrossRef]
- Burns, T.J.; Batavia, A.I.; Smith, Q.W.; DeJong, G. Primary health care needs of persons with physical disabilities: What are the research and service priorities? Arch. Phys. Med. Rehabil. 1990, 71, 138–143. [Google Scholar]
- Smith, R. Promoting the health of people with physical disabilities: A discussion of the financing and organization of public health services in Australia. Health Promot. Int. 2000, 15, 79–86. [Google Scholar] [CrossRef][Green Version]
- The U.S. Preventive Services Task Force Works. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/ (accessed on 5 December 2023).
- World Health Organization. WHO Global Disability Action Plan 2014–2021. Better Health for All People with Disability; WHO: Geneva, Switzerland, 2015; Available online: https://www.who.int/publications/i/item/who-global-disability-action-plan-2014-2021 (accessed on 5 December 2023).
- Carey, I.M.; Hosking, F.J.; Harris, T.; DeWilde, S.; Beighton, C.; Shah, S.M.; Cook, D.G. Do health checks for adults with intellectual disability reduce emergency hospital admissions? Evaluation of a natural experiment. J. Epidemiol. Community Health 2017, 71, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, N.; Kennedy, J.; Kerr, M.; Dredge, S.; Brophy, S. Health checks for adults with intellectual disability and association with survival rates: A linked electronic records matched cohort study in Wales, UK. BMJ Open 2022, 12, e049441. [Google Scholar] [CrossRef] [PubMed]
- Iezzoni, L.I.; McCarthy, E.P.; Davis, R.B.; Siebens, H. Mobility impairments and use of screening and preventive services. Am. J. Public Health 2000, 90, 955–961. [Google Scholar] [PubMed]
- Chiu, T.Y. Predictors of use of preventative health services for people with disabilities in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 1661. [Google Scholar] [CrossRef] [PubMed]
- Sakellariou, D.; Rotarou, E.S. Access to healthcare for men and women with disabilities in the UK: Secondary analysis of cross-sectional data. BMJ Open 2017, 7, e016614. [Google Scholar] [CrossRef] [PubMed]
- Andiwijaya, F.R.; Davey, C.; Bessame, K.; Ndong, A.; Kuper, H. Disability and participation in breast and cervical cancer screening: A systematic review and meta-analysis. Int. J. Environ. Res. Public. Health 2022, 19, 9465. [Google Scholar] [CrossRef] [PubMed]
- Hisamichi, S. Community screening programs of cancer and cardiovascular diseases in Japan. J. Epidemiol. 1996, 6, S159–S163. [Google Scholar] [CrossRef]
- National Institute of Health and Nutrition. Available online: https://www.nibiohn.go.jp/eiken/kenkounippon21/en/kenkounippon21/index.html (accessed on 5 December 2023).
- Ministry of Health, Labor and Welfare of Japan. Annual Health, Labor and Welfare Report 2007–2008. Section 3, Measures against Lifestyle Related Diseases through “Health Japan 21” and Promotion of “Shokuiku (Food and Nutrition Education)”. Available online: https://www.mhlw.go.jp/english/wp/wp-hw2/part2/p2c1s3.pdf (accessed on 5 December 2023).
- Ministry of Health, Labour and Welfare of Japan. Basic Plan to Promote Cancer Control Program. Available online: https://www.mhlw.go.jp/content/10900000/001138884.pdf (accessed on 5 December 2023). (In Japanese)
- Cabinet Office, the Government of Japan. Annual Report on Government Measures for Persons with Disabilities (Summary) 2023. Available online: https://www8.cao.go.jp/shougai/english/annualreport/2023/pdf/index.pdf (accessed on 5 December 2023).
- Fukuda, Y.; Nakamura, K.; Takano, T.; Nakao, H.; Imai, H. Socioeconomic status and cancer screening in Japanese males: Large inequality in middle-aged and urban residents. Environ. Health Prev. Med. 2007, 12, 90–96. [Google Scholar] [CrossRef]
- Imamura, H.; Kogure, M.; Kita, Y.; Nakagawa, H.; Hozawa, A.; Okamura, T.; Murakami, Y.; Nishi, N.; Okuda, N.; Kadota, A.; et al. Factors Related to Participation in Health Examinations for Japanese National Health Insurance: NIPPON DATA2010. J. Epidemiol. 2018, 28, S53–S58. [Google Scholar] [CrossRef]
- Seko, R.; Kawado, M.; Saito, S.; Shibuya, T.; Miyamoto, M.; Yamada, H.; Taniwaki, H.; Hashimoto, S. Associations of occupation, employment type and company size with actions related to health examinations among Japanese employees. Ind. Health 2019, 57, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Okui, T. Analysis of predictors of breast cancer screening among Japanese women using nationally representative survey data, 2001–2013. Asian Pac. J. Cancer Prev. 2021, 22, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Nakao, M. Social-life factors associated with participation in screening and further assessment of colorectal cancer: Nationwide ecological study in Japanese municipalities. SSM Popul. Health 2021, 15, 100839. [Google Scholar] [CrossRef] [PubMed]
- Okayama, M.; Nagaoka, T.; Sugisaki, K. Cancer screening rate and related factors in the Japanese child-rearing generation. Healthcare 2022, 10, 508. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, C.; Iwagami, M.; Sun, Y.; Komiyama, J.; Ito, T.; Sugiyama, T.; Bando, H.; Tamiya, N. Factors associated with non-participation in breast cancer screening: Analysis of the 2016 and 2019 comprehensive survey of living conditions in Japan. Breast Cancer 2023, 30, 952–964. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, M.; Inagaki, M.; Nakaya, N.; Fujimori, M.; Higuchi, Y.; Hayashibara, C.; So, R.; Kakeda, K.; Kodama, M.; Uchitomi, Y.; et al. Cancer screening participation in schizophrenic outpatients and the influence of their functional disability on the screening rate: A cross-sectional study in Japan. Psychiatry Clin. Neurosci. 2017, 71, 813–825. [Google Scholar] [CrossRef] [PubMed]
- Muraoka, M.; Shiga, T. Use of general health examination among community dwelling people with intellectual disability in Japan. Jpn. J. Dev. Disabil. 2018, 40, 404–412. (In Japanese) [Google Scholar]
- Takahashi, E.; Nakadate, T. An investigation of the experiences of hearing-impaired people undergoing medical examinations in health-checkups. Nihon Koshu Eisei Zasshi 2003, 50, 908–918. [Google Scholar]
- Matsuo, K. Breast cancer screening for severely disabled patients: Present status and future problems. J. Jpn. Assoc. Breast Cancer Screen. 2007, 16, 122–125. [Google Scholar] [CrossRef]
- Yamaki, C.; Takayama, T. Medical examination, cancer screening, and health information channels of people with sight impairment: A survey of the resisters of a braille library or a sight impairment support group. Nihon Koshu Eisei Zasshi 2017, 64, 270–279. [Google Scholar]
- Ministry of Health, Labour and Welfare of Japan. Available online: https://www.mhlw.go.jp/toukei/itaku/tokumei.html (accessed on 5 December 2023). (In Japanese)
- Ministry of Health, Labour and Welfare of Japan. Available online: https://www.mhlw.go.jp/content/10901000/000682242.pdf (accessed on 5 December 2023). (In Japanese)
- Japan Cancer Society. A Survey of Cancer Screening Policy. Available online: https://www.jcancer.jp/news/10017 (accessed on 5 December 2023). (In Japanese).
- World Health Organization. WHO Position Paper on Mammography Screening. Available online: https://www.who.int/publications/i/item/who-position-paper-on-mammography-screening (accessed on 5 December 2023).
- Ministry of Health, Labour and Welfare of Japan. Available online: https://www.mhlw.go.jp/toukei/list/20-21tyousa.html#anchor11 (accessed on 5 December 2023). (In Japanese)
- Ministry of Health, Labour and Welfare of Japan. Available online: https://www.mhlw.go.jp/toukei/chousahyo/index.html#00450061 (accessed on 5 December 2023). (In Japanese)
- Sato, S.; Tanimoto, A.; Yanagimura, N.; Suzuki, C.; Takumi, Y.; Nishiyama, A.; Yamashita, K.; Takeuchi, S.; Ohtsubo, K.; Makino, T.; et al. Multi institutional survey of cancer disparities in disabled patients in the region of northwestern Japan. Int. J. Clin. Oncol. 2021, 26, 1009–1014. [Google Scholar] [CrossRef]
- Reihani, A.R.; Ahari, J.; Cain, C.H.; Bade, B.C.; Zimmerman, H.G. Barriers and facilitators to lung cancer screening in the United States: A systematic review of the qualitative literature. J. Health Soc. Sci. 2021, 6, 333–348. [Google Scholar]
- Cavers, D.; Nelson, M.; Rostron, J.; Robb, K.A.; Brown, L.R.; Campbell, C.; Akram, A.R.; Dickie, G.; Mackean, M.; van Beek, E.J.R.; et al. Understanding patient barriers and facilitators to uptake of lung screening using low dose computed tomography: A mixed methods scoping review of the current literature. Respir. Res. 2022, 23, 374. [Google Scholar] [CrossRef]
- Andriacchi, R. Primary care for persons with disabilities. The internal medicine perspective. Am. J. Phys. Med. Rehabil. 1997, 76, S17–S20. [Google Scholar] [CrossRef] [PubMed]
- Sonalkar, S.; Chavez, V.; McClusky, J.; Hunter, T.A.; Mollen, C.J. Gynecologic care for women with physical disabilities: A qualitative study of patients and providers. Womens Health Issues 2020, 30, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Maart, S.; Jelsma, J. Disability and access to health care—A community based descriptive study. Disabil. Rehabil. 2014, 36, 1489–1493. [Google Scholar] [CrossRef] [PubMed]
- Bright, T.; Kuper, H. A Systematic Review of Access to General Healthcare Services for People with Disabilities in Low and Middle Income Countries. Int. J. Environ. Res. Public Health 2018, 15, 1879. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. People with Disability in Australia 2022. Available online: https://www.aihw.gov.au/reports/disability/people-with-disability-in-australia/contents/about (accessed on 1 February 2024).
- Gudlavalleti, M.V.; John, N.; Allagh, K.; Sagar, J.; Kamalakannan, S.; Ramachandra, S.S.; South India Disability Evidence Study Group. Access to health care and employment status of people with disabilities in South India, the SIDE (South India Disability Evidence) study. BMC Public Health 2014, 14, 1125. [Google Scholar] [CrossRef] [PubMed]
- Levesque, J.F.; Harris, M.F.; Russell, G. Patient-centred access to health care: Conceptualizing access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Penchansky, R.; Thomas, J.W. The concept of access: Definition and relationship to consumer satisfaction. Med. Care 1981, 19, 127–140. [Google Scholar] [CrossRef]
- Saurman, E. Improving access: Modifying Penchansky and Thomas’s Theory of Access. J. Health Serv. Res. Policy 2016, 21, 36–39. [Google Scholar] [CrossRef]
- Chen, K.L.; Brozen, M.; Rollman, J.E.; Ward, T.; Norris, K.C.; Gregory, K.D.; Zimmerman, F.J. How is the COVID-19 pandemic shaping transportation access to health care? Transp. Res. Interdiscip. Perspect. 2021, 10, 100338. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| General Health Examination (n = 8438) | Lung Cancer Screening (n = 6042) | Colorectal Cancer Screening (n = 6030) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Participants (n = 6196) | Non- Participants (n = 2242) | p-Value | Participants (n = 3163) | Non- Participants (n = 2879) | p-Value | Participants (n = 2825) | Non- Participants (n = 3205) | p-Value | |||||||
| n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | ||||
| Disability | <0.001 | <0.001 | <0.001 | ||||||||||||
| Do not need any support or supervision | 6142 | (99.13) | 2188 | (97.59) | 3135 | (99.11) | 2821 | (97.99) | 2801 | (99.15) | 3144 | (98.10) | |||
| Need support or supervision | 54 | (0.87) | 54 | (2.41) | 28 | (0.89) | 58 | (2.01) | 24 | (0.85) | 61 | (1.90) | |||
| Sex | <0.001 | <0.001 | <0.001 | ||||||||||||
| Male | 3229 | (52.11) | 880 | (39.25) | 1720 | (54.38) | 1231 | (42.76) | 1510 | (53.45) | 1421 | (44.34) | |||
| Female | 2967 | (47.89) | 1362 | (60.75) | 1443 | (45.62) | 1648 | (57.24) | 1315 | (46.55) | 1784 | (55.66) | |||
| Age (years) | <0.001 | 0.032 | 0.332 | ||||||||||||
| 65–74 | 1264 | (20.40) | 576 | (25.69) | 914 | (28.90) | 905 | (31.43) | 834 | (29.52) | 983 | (30.67) | |||
| 40–64 | 3325 | (53.66) | 982 | (43.80) | 2249 | (71.10) | 1974 | (68.57) | 1991 | (70.48) | 2222 | (69.33) | |||
| 20–39 | 1607 | (25.94) | 684 | (30.51) | - | (-) | - | (-) | - | (-) | - | (-) | |||
| Marital status | <0.001 | <0.001 | <0.001 | ||||||||||||
| Married | 4395 | (70.93) | 1439 | (64.18) | 2594 | (82.01) | 2189 | (76.03) | 2355 | (83.36) | 2425 | (75.66) | |||
| Single | 1306 | (21.08) | 585 | (26.09) | 273 | (8.63) | 346 | (12.02) | 221 | (7.82) | 391 | (12.20) | |||
| Divorced/widowed | 495 | (7.99) | 218 | (9.72) | 296 | (9.36) | 344 | (11.95) | 249 | (8.81) | 389 | (12.14) | |||
| Educational qualification | <0.001 | <0.001 | <0.001 | ||||||||||||
| Vocational school/junior college/community (technical) college/university/post-graduate school | 3278 | (52.91) | 911 | (40.63) | 1533 | (48.47) | 1108 | (38.49) | 1419 | (50.23) | 1224 | (38.19) | |||
| High school | 2512 | (40.54) | 1025 | (45.72) | 1369 | (43.28) | 1413 | (49.08) | 1199 | (42.44) | 1576 | (49.17) | |||
| Primary/junior high school | 406 | (6.55) | 306 | (13.65) | 261 | (8.25) | 358 | (12.43) | 207 | (7.33) | 405 | (12.64) | |||
| Subjective financial state | <0.001 | <0.001 | <0.001 | ||||||||||||
| Wealthy | 391 | (6.31) | 85 | (3.79) | 241 | (7.62) | 117 | (4.06) | 227 | (8.04) | 132 | (4.12) | |||
| Nor poor, not wealthy | 2492 | (40.22) | 723 | (32.25) | 1323 | (41.83) | 1018 | (35.36) | 1203 | (42.58) | 1138 | (35.51) | |||
| Poor | 3313 | (53.47) | 1434 | (63.96) | 1599 | (50.55) | 1744 | (60.58) | 1395 | (49.38) | 1935 | (60.37) | |||
| Health insurance | <0.001 | <0.001 | <0.001 | ||||||||||||
| Employee insurance | 4519 | (72.93) | 1151 | (51.34) | 2132 | (67.40) | 1517 | (52.69) | 1866 | (66.05) | 1780 | (55.54) | |||
| National Health Insurance | 1590 | (25.66) | 995 | (44.38) | 985 | (31.14) | 1249 | (43.38) | 917 | (32.46) | 1310 | (40.87) | |||
| Other | 87 | (1.40) | 96 | (4.28) | 46 | (1.45) | 113 | (3.92) | 42 | (1.49) | 115 | (3.59) | |||
| Employment status | <0.001 | <0.001 | <0.001 | ||||||||||||
| Employed | 4058 | (65.49) | 845 | (37.69) | 1867 | (59.03) | 1228 | (42.65) | 1584 | (56.07) | 1504 | (46.93) | |||
| Self-employed | 333 | (5.37) | 218 | (9.72) | 219 | (6.92) | 268 | (9.31) | 194 | (6.87) | 291 | (9.08) | |||
| Employed (other) | 400 | (6.46) | 193 | (8.61) | 267 | (8.44) | 246 | (8.54) | 244 | (8.64) | 270 | (8.42) | |||
| Unemployed | 1405 | (22.68) | 986 | (43.98) | 810 | (25.61) | 1137 | (39.49) | 803 | (28.42) | 1140 | (35.57) | |||
| Kessler Psychological Distress Scale | 0.002 | 0.007 | <0.001 | ||||||||||||
| Normal (total score ≤ 4) | 4510 | (72.79) | 1549 | (69.09) | 2376 | (75.12) | 2068 | (71.83) | 2139 | (75.72) | 2295 | (71.61) | |||
| Mild illness (5 ≤ total score ≤ 12) | 1468 | (23.69) | 591 | (26.36) | 705 | (22.29) | 711 | (24.70) | 614 | (21.73) | 801 | (24.99) | |||
| Severe illness (13 ≤ total score) | 218 | (3.52) | 102 | (4.55) | 82 | (2.59) | 100 | (3.47) | 72 | (2.55) | 109 | (3.40) | |||
| Constant visits to hospitals † | <0.001 | <0.001 | <0.001 | ||||||||||||
| Yes (visit) | 2668 | (43.06) | 858 | (38.27) | 1653 | (52.26) | 1341 | (46.58) | 1527 | (54.05) | 1467 | (45.77) | |||
| No (no visit) | 3528 | (56.94) | 1384 | (61.73) | 1510 | (47.74) | 1538 | (53.42) | 1298 | (45.95) | 1738 | (54.23) | |||
| Subjective health status | <0.001 | 0.002 | 0.024 | ||||||||||||
| Good | 2288 | (36.93) | 781 | (34.83) | 1089 | (34.43) | 931 | (32.34) | 971 | (34.37) | 1043 | (32.54) | |||
| Normal | 3262 | (52.65) | 1158 | (51.65) | 1731 | (54.73) | 1552 | (53.91) | 1540 | (54.51) | 1735 | (54.13) | |||
| Bad | 646 | (10.43) | 303 | (13.51) | 343 | (10.84) | 396 | (13.75) | 314 | (11.12) | 427 | (13.32) | |||
| Alcohol consumption | <0.001 | <0.001 | <0.001 | ||||||||||||
| Never or quit drinking | 3197 | (51.60) | 1410 | (62.89) | 1529 | (48.34) | 1704 | (59.19) | 1373 | (48.60) | 1856 | (57.91) | |||
| Social drinker/low-risk group (>0 to ≤100 g/week) | 1534 | (24.76) | 444 | (19.80) | 776 | (24.53) | 564 | (19.59) | 708 | (25.06) | 627 | (19.56) | |||
| Middle-risk drinking (>100 to ≤350 g/week) | 1278 | (20.63) | 322 | (14.36) | 765 | (24.19) | 520 | (18.06) | 655 | (23.19) | 629 | (19.63) | |||
| High-risk drinking (>350 g/week) | 187 | (3.02) | 66 | (2.94) | 93 | (2.94) | 91 | (3.16) | 89 | (3.15) | 93 | (2.90) | |||
| Smoking habit | 0.157 | 0.058 | <0.001 | ||||||||||||
| Never/ex-smoker | 4881 | (78.78) | 1734 | (77.34) | 2507 | (79.26) | 2224 | (77.25) | 2301 | (81.45) | 2429 | (75.79) | |||
| Current smoker | 1315 | (21.22) | 508 | (22.66) | 656 | (20.74) | 655 | (22.75) | 524 | (18.55) | 776 | (24.21) | |||
| Gastric Cancer Screening (n = 4318) | Cervical Cancer Screening (n = 4261) | Breast Cancer Screening (n = 3098) | |||||||||||||
| Participants (n = 2033) | Non- Participants (n = 2285) | p-Value | Participants (n = 1864) | Non- Participants (n = 2397) | p-Value | Participants (n = 1469) | Non- Participants (n = 1629) | p-Value | |||||||
| n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | ||||
| Disability | <0.001 | <0.001 | 0.004 | ||||||||||||
| Do not need any support or supervision | 2016 | (99.16) | 2234 | (97.77) | 1853 | (99.41) | 2355 | (98.25) | 1459 | (99.32) | 1599 | (98.16) | |||
| Need support or supervision | 17 | (0.84) | 51 | (2.23) | 11 | (0.59) | 42 | (1.75) | 10 | (0.68) | 30 | (1.84) | |||
| Sex | <0.001 | - | - | ||||||||||||
| Male | 1106 | (54.40) | 1003 | (43.89) | - | (-) | - | (-) | - | (-) | - | (-) | |||
| Female | 927 | (45.60) | 1282 | (56.11) | 1864 | (100.00) | 2397 | (100.00) | 1469 | (100.00) | 1629 | (100.00) | |||
| Age (years) | 0.033 | <0.001 | <0.001 | ||||||||||||
| 65–74 | - | (-) | - | (-) | 284 | (15.24) | 629 | (26.24) | 325 | (22.12) | 590 | (36.22) | |||
| 40–64 | - | (-) | - | (-) | 1096 | (58.80) | 1075 | (44.85) | 1144 | (77.88) | 1039 | (63.78) | |||
| 20–39 | - | (-) | - | (-) | 484 | (25.97) | 693 | (28.91) | - | (-) | - | (-) | |||
| 65–74 | 821 | (40.38) | 996 | (43.59) | - | (-) | - | (-) | - | (-) | - | (-) | |||
| 50–64 | 1212 | (59.62) | 1289 | (56.41) | - | (-) | - | (-) | - | (-) | - | (-) | |||
| Marital status | <0.001 | <0.001 | <0.001 | ||||||||||||
| Married | 1705 | (83.87) | 1757 | (76.89) | 1451 | (77.84) | 1491 | (62.20) | 1195 | (81.35) | 1222 | (75.02) | |||
| Single | 124 | (6.10) | 207 | (9.06) | 221 | (11.86) | 588 | (24.53) | 94 | (6.40) | 125 | (7.67) | |||
| Divorced/widowed | 204 | (10.03) | 321 | (14.05) | 192 | (10.30) | 318 | (13.27) | 180 | (12.25) | 282 | (17.31) | |||
| Educational qualification | <0.001 | <0.001 | <0.001 | ||||||||||||
| Vocational school/junior college/community (technical) college/university/post-graduate school | 912 | (44.86) | 767 | (33.57) | 1015 | (54.45) | 1080 | (45.06) | 722 | (49.15) | 573 | (35.17) | |||
| High school | 921 | (45.30) | 1173 | (51.33) | 765 | (41.04) | 1061 | (44.26) | 660 | (44.93) | 842 | (51.69) | |||
| Primary/junior high school | 200 | (9.84) | 345 | (15.10) | 84 | (4.51) | 256 | (10.68) | 87 | (5.92) | 214 | (13.14) | |||
| Subjective financial state | <0.001 | <0.001 | <0.001 | ||||||||||||
| Wealthy | 175 | (8.61) | 84 | (3.68) | 137 | (7.35) | 93 | (3.88) | 118 | (8.03) | 58 | (3.56) | |||
| Not poor, not wealthy | 868 | (42.70) | 853 | (37.33) | 772 | (41.42) | 838 | (34.96) | 611 | (41.59) | 592 | (36.34) | |||
| Poor | 990 | (48.70) | 1348 | (58.99) | 955 | (51.23) | 1466 | (61.16) | 740 | (50.37) | 979 | (60.10) | |||
| Health insurance | <0.001 | <0.001 | <0.001 | ||||||||||||
| Employee insurance | 1188 | (58.44) | 1001 | (43.81) | 1399 | (75.05) | 1465 | (61.12) | 1003 | (68.28) | 855 | (52.49) | |||
| National Health Insurance | 810 | (39.84) | 1185 | (51.86) | 452 | (24.25) | 862 | (35.96) | 455 | (30.97) | 717 | (44.01) | |||
| Other | 35 | (1.72) | 99 | (4.33) | 13 | (0.70) | 70 | (2.92) | 11 | (0.75) | 57 | (3.50) | |||
| Employment status | <0.001 | <0.001 | <0.001 | ||||||||||||
| Employed | 992 | (48.79) | 822 | (35.97) | 1070 | (57.40) | 1195 | (49.85) | 777 | (52.89) | 652 | (40.02) | |||
| Self-employed | 168 | (8.26) | 231 | (10.11) | 44 | (2.36) | 64 | (2.67) | 40 | (2.72) | 54 | (3.31) | |||
| Employed (other) | 184 | (9.05) | 218 | (9.54) | 130 | (6.97) | 179 | (7.47) | 122 | (8.30) | 159 | (9.76) | |||
| Unemployed | 689 | (33.89) | 1014 | (44.38) | 620 | (33.26) | 959 | (40.01) | 530 | (36.08) | 764 | (46.90) | |||
| Kessler Psychological Distress Scale | 0.063 | 0.931 | 0.627 | ||||||||||||
| Normal (total score ≤ 4) | 1558 | (76.64) | 1681 | (73.57) | 1302 | (69.85) | 1685 | (70.30) | 1040 | (70.80) | 1178 | (72.31) | |||
| Mild illness (5 ≤ total score ≤ 12) | 423 | (20.81) | 542 | (23.72) | 483 | (25.91) | 609 | (25.41) | 378 | (25.73) | 395 | (24.25) | |||
| Severe illness (13 ≤ total score) | 52 | (2.56) | 62 | (2.71) | 79 | (4.24) | 103 | (4.30) | 51 | (3.47) | 56 | (3.44) | |||
| Constant visits to hospitals † | <0.001 | 0.004 | 0.001 | ||||||||||||
| Yes (visit) | 1249 | (61.44) | 1225 | (53.61) | 848 | (45.49) | 985 | (41.09) | 782 | (53.23) | 771 | (47.33) | |||
| No (no visit) | 784 | (38.56) | 1060 | (46.39) | 1016 | (54.51) | 1412 | (58.91) | 687 | (46.77) | 858 | (52.67) | |||
| Subjective health status | 0.099 | 0.023 | 0.495 | ||||||||||||
| Good | 651 | (32.02) | 677 | (29.63) | 713 | (38.25) | 820 | (34.21) | 508 | (34.58) | 531 | (32.60) | |||
| Normal | 1134 | (55.78) | 1289 | (56.41) | 940 | (50.43) | 1296 | (54.07) | 784 | (53.37) | 892 | (54.76) | |||
| Bad | 248 | (12.20) | 319 | (13.96) | 211 | (11.32) | 281 | (11.72) | 177 | (12.05) | 206 | (12.65) | |||
| Alcohol consumption | <0.001 | 0.008 | 0.004 | ||||||||||||
| Never or quit drinking | 1001 | (49.24) | 1340 | (58.64) | 1230 | (65.99) | 1690 | (70.50) | 984 | (66.98) | 1178 | (72.31) | |||
| Social drinker/low-risk group (>0 to ≤100 g/week) | 504 | (24.79) | 437 | (19.12) | 433 | (23.23) | 507 | (21.15) | 345 | (23.49) | 298 | (18.29) | |||
| Middle-risk drinking (>100 to ≤350 g/week) | 478 | (23.51) | 448 | (19.61) | 178 | (9.55) | 176 | (7.34) | 125 | (8.51) | 137 | (8.41) | |||
| High-risk drinking (>350 g/week) | 50 | (2.46) | 60 | (2.63) | 23 | (1.23) | 24 | (1.00) | 15 | (1.02) | 16 | (0.98) | |||
| Smoking habit | <0.001 | 0.003 | <0.001 | ||||||||||||
| Never/ex-smoker | 1692 | (83.23) | 1790 | (78.34) | 1708 | (91.63) | 2130 | (88.86) | 1368 | (93.12) | 1435 | (88.09) | |||
| Current smoker | 341 | (16.77) | 495 | (21.66) | 156 | (8.37) | 267 | (11.14) | 101 | (6.88) | 194 | (11.91) | |||
| General Health Examination | Cancer Screening | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lung | Colorectal | Gastric | Cervical | Breast | ||||||||
| Unadjusted OR (95%CI) | Adjusted OR (95%CI) | Unadjusted OR (95%CI) | Adjusted OR (95%CI) | Unadjusted OR (95%CI) | Adjusted OR (95%CI) | Unadjusted OR (95%CI) | Adjusted OR (95%CI) | Unadjusted OR (95%CI) | Adjusted OR (95%CI) | Unadjusted OR (95%CI) | Adjusted OR (95%CI) | |
| Disability | ||||||||||||
| Do not need any support or supervision | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) |
| Need support or supervision | 2.81 (1.92, 4.11) | 1.73 (1.14, 2.62) | 2.30 (1.46, 3.62) | 1.56 (0.96, 2.51) | 2.26 (1.40, 3.64) | 1.78 (1.08, 2.94) | 2.71 (1.56, 4.70) | 2.27 (1.27, 4.05) | 3.00 (1.54, 5.85) | 2.12 (1.04, 4.32) | 2.74 (1.33, 5.62) | 2.22 (1.04, 4.72) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, T.; Imahashi, K.; Yamaki, C. Use of General Health Examination and Cancer Screening among People with Disability Who Need Support from Others: Analysis of the 2016 Comprehensive Survey of Living Conditions in Japan. Int. J. Environ. Res. Public Health 2024, 21, 219. https://doi.org/10.3390/ijerph21020219
Saito T, Imahashi K, Yamaki C. Use of General Health Examination and Cancer Screening among People with Disability Who Need Support from Others: Analysis of the 2016 Comprehensive Survey of Living Conditions in Japan. International Journal of Environmental Research and Public Health. 2024; 21(2):219. https://doi.org/10.3390/ijerph21020219
Chicago/Turabian StyleSaito, Takashi, Kumiko Imahashi, and Chikako Yamaki. 2024. "Use of General Health Examination and Cancer Screening among People with Disability Who Need Support from Others: Analysis of the 2016 Comprehensive Survey of Living Conditions in Japan" International Journal of Environmental Research and Public Health 21, no. 2: 219. https://doi.org/10.3390/ijerph21020219
APA StyleSaito, T., Imahashi, K., & Yamaki, C. (2024). Use of General Health Examination and Cancer Screening among People with Disability Who Need Support from Others: Analysis of the 2016 Comprehensive Survey of Living Conditions in Japan. International Journal of Environmental Research and Public Health, 21(2), 219. https://doi.org/10.3390/ijerph21020219