
The Effects of an Inclusive Badminton Program on Static Postural Control for Individuals with Intellectual and Developmental Disabilities


 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
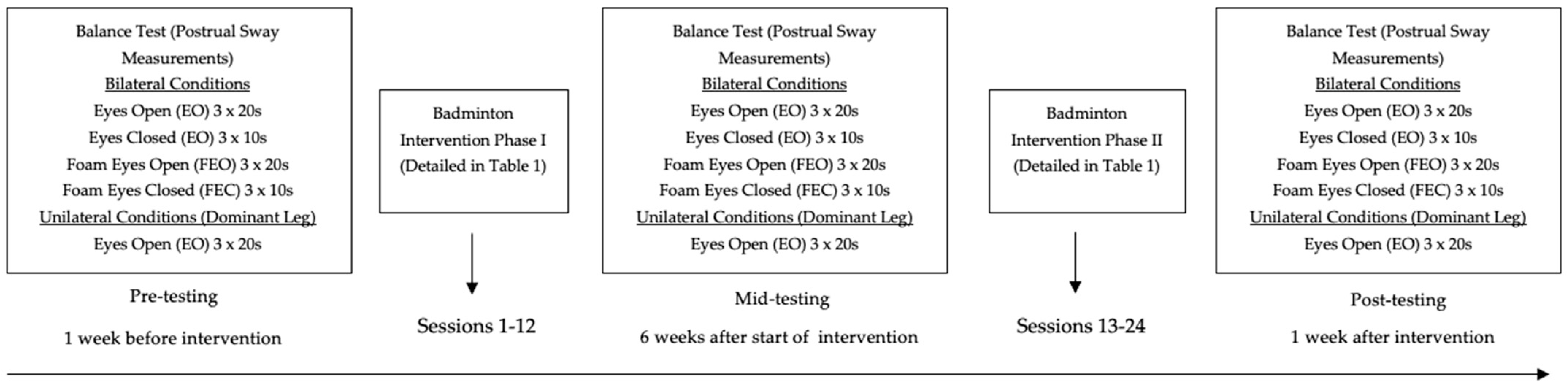
2.2. Experimental Procedures
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Eyes Open (EO)
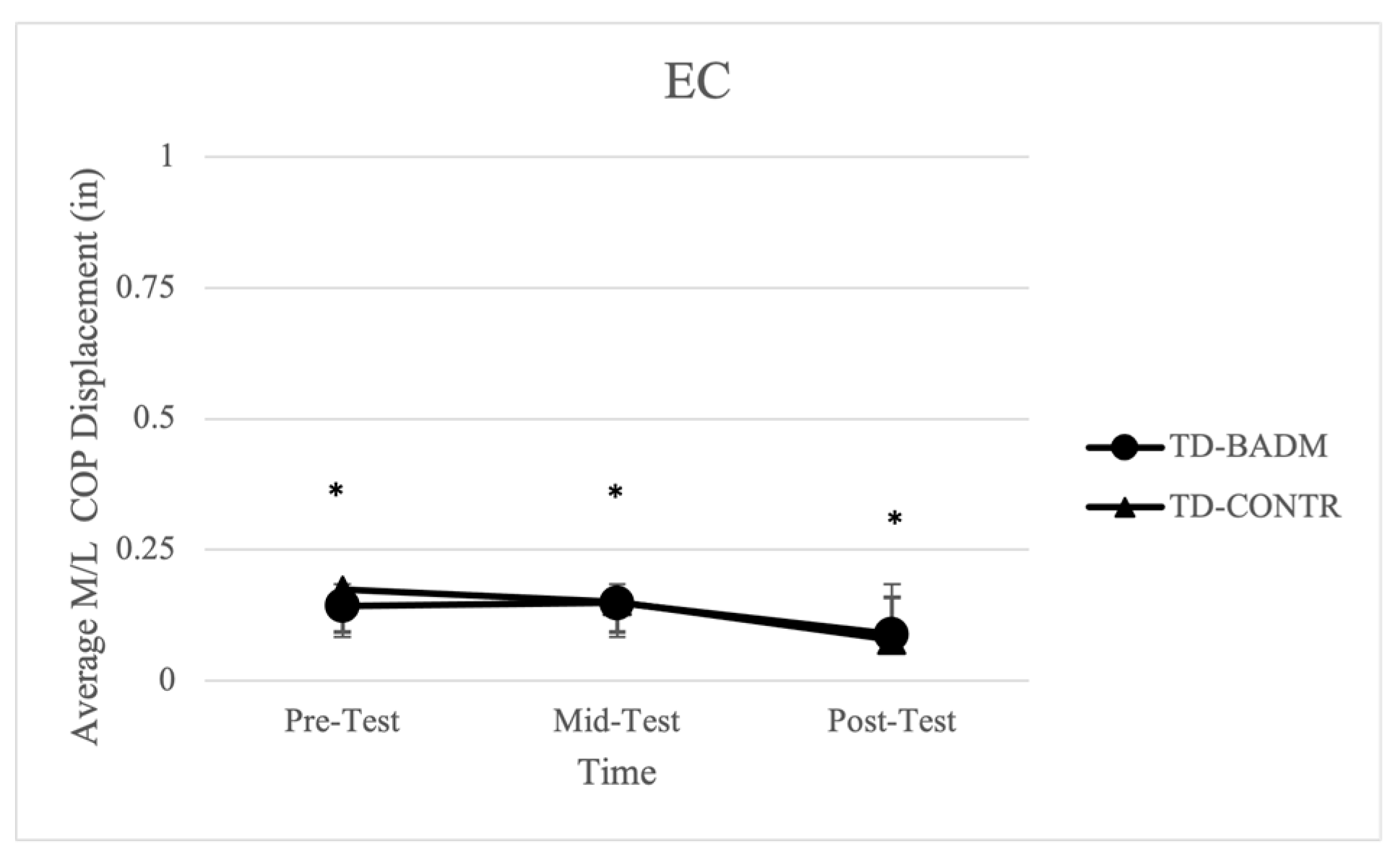
3.2. Eyes Closed
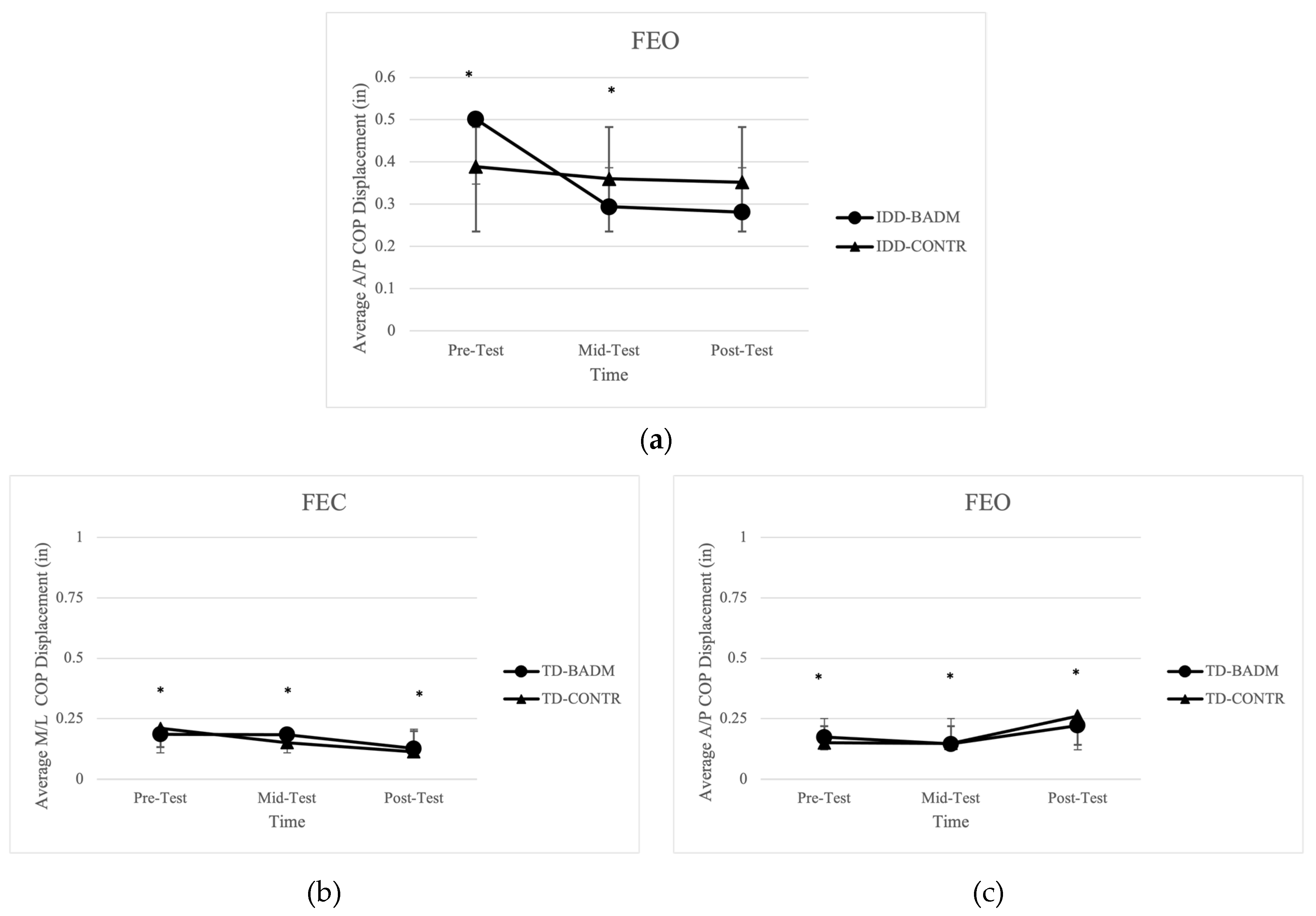
3.3. Foam Eyes Open (FEO)
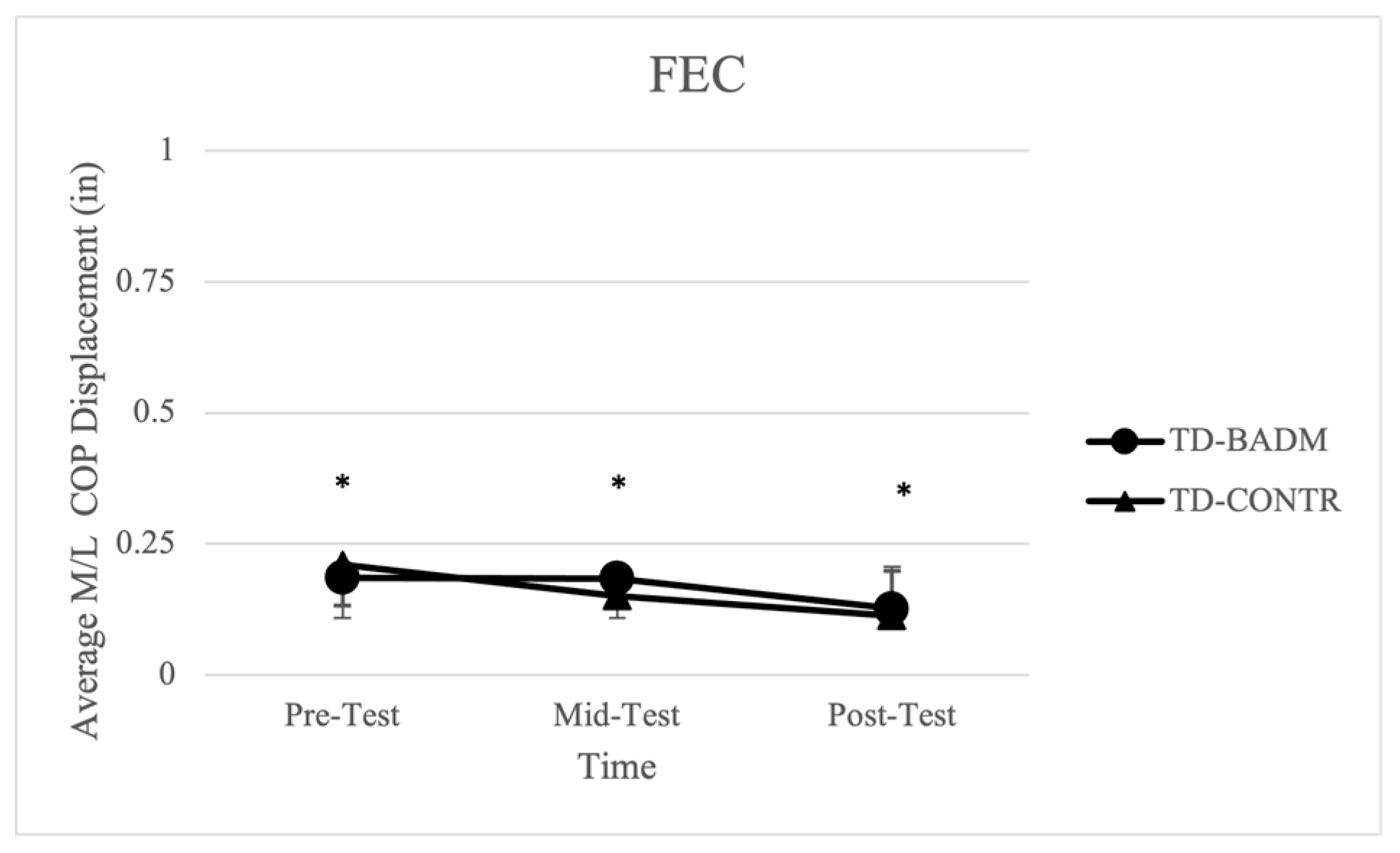
3.4. Foam Eyes Closed (FEC)
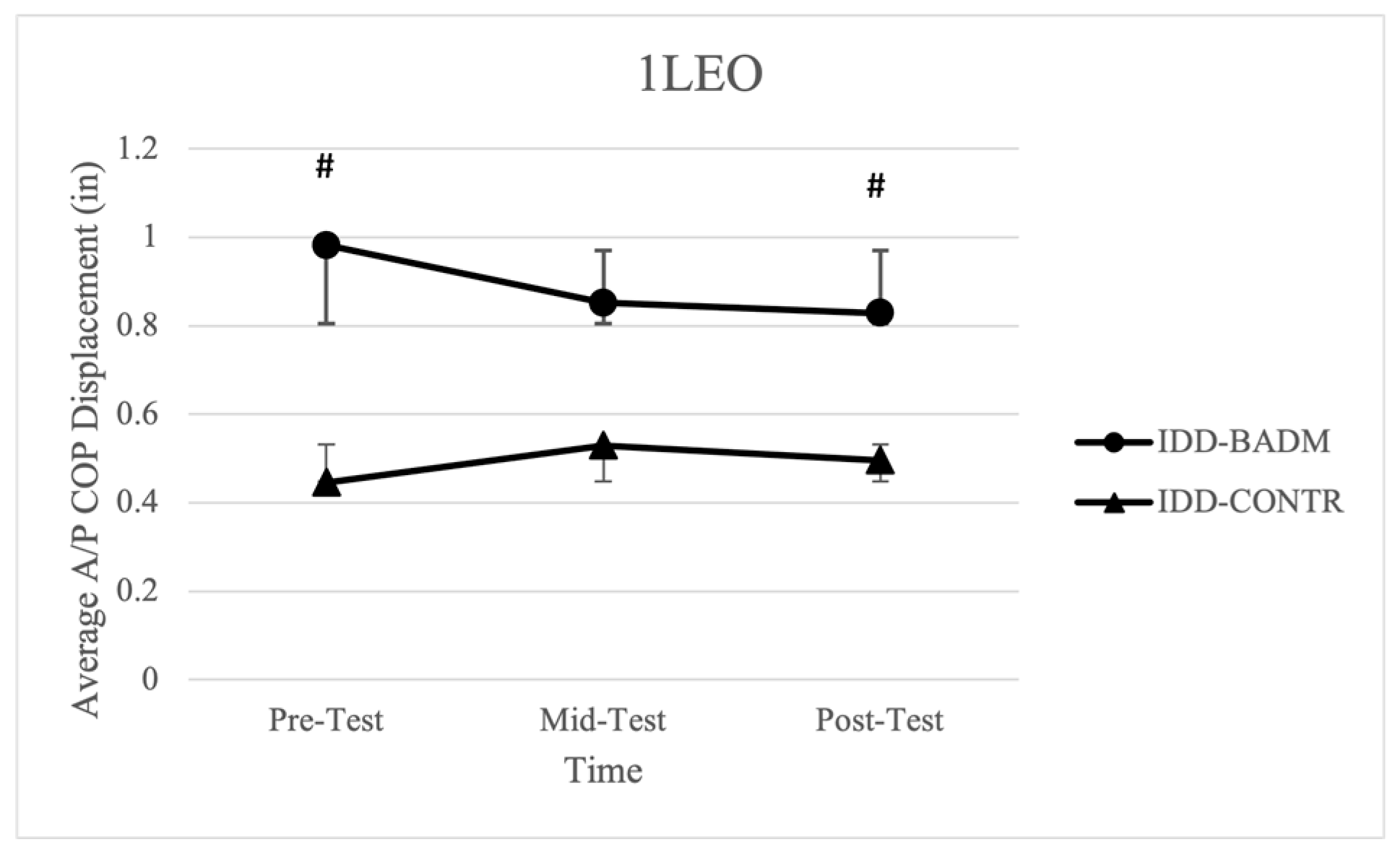
3.5. Unilateral Eyes Open (1LEO)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviations | Definitions |
| COG | Center of gravity |
| BOS | Base of support |
| IDD | Intellectual and developmental disabilities |
| TD | Typically developing |
| BADM | Badminton |
| EO | Eyes open |
| EC | Eyes closed |
| FEO | Foam eyes closed |
| FEC | Foam eyes open |
| 1LEO | Single-leg eyes open |
| COP | Center of pressure |
| CONTR | Control |
References
- Harris, J.C. Intellectual Disability: Understanding Its Development, Causes, Classification, Evaluation, and Treatment; Oxford University Press: Oxford, UK, 2006; pp. 42–98. [Google Scholar]
- King, B.H.; Toth, K.E.; Hodapp, R.M.; Dykens, E.M. Intellectual disability. In Comprehensive Textbook of Psychiatry, 9th ed.; Sadock, B.J., Sadock, V.A., Ruiz, P., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009; pp. 3444–3474. ISBN 978-0-7817-6899-3. [Google Scholar]
- Maulik, P.K.; Mascarenhas, M.N.; Mathers, C.D.; Dua, T.; Saxena, S. Prevalence of intellectual disability: A meta-analysis of population-based studies. Res. Dev. Disabil. 2011, 32, 419–436. [Google Scholar] [CrossRef] [PubMed]
- American Association of Intellectual and Developmental Disabilities. Definition, Classification, and Systems of Support, 11th ed.; American Association of Intellectual and Developmental Disabilities: Washington, DC, USA, 2010. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- CDC. National center for chronic disease prevention and health promotion, guidelines for school and community programs to promote lifelong physical activity among young people. J. Sch. Health 1997, 67, 202–219. [Google Scholar] [CrossRef] [PubMed]
- Rimmer, J.H.; Yamaki, K.; Lowry BM, D.; Wang, E.; Vogel, L.C. Obesity and obesity-related secondary conditions in adolescents with intellectual/developmental disabilities. J. Intellect. Disabil. Res. 2010, 54, 787–794. [Google Scholar] [CrossRef]
- Winter, D.A.; Patla, A.E.; Prince, F.; Ishac, M.; Gielo-Perczak, K. Stiffness Control of Balance in Quiet Standing. J. Neurophysiol. 1998, 80, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- Kohen-Raz, R.; Volkman, F.R.; Cohen, D.J. Postural control in children with autism. J. Autism Dev. Disord. 1992, 22, 419–432. [Google Scholar] [CrossRef] [PubMed]
- Memari, A.; Ghanouni, P.; Gharibzadeh, S.; Eghlidi, J.; Ziaee, V.; Moshayedi, P. Postural sway patterns in children with autism spectrum disorder compared with typically developing children. Res. Autism Spectr. Disord. 2013, 7, 325–332. [Google Scholar] [CrossRef]
- Minshew, N.J.; Sung, K.; Jones, B.L.; Furman, J.M. Underdevelopment of the postural control system in autism. Neurology 2004, 63, 2056. [Google Scholar] [CrossRef]
- Sacrey, L.-A.R.; Germani, T.; Bryson, S.E.; Zwaigenbaum, L. Reaching and Grasping in Autism Spectrum Disorder: A Review of Recent Literature. Front. Neurol. 2014, 5, 6. [Google Scholar] [CrossRef]
- Fournier, K.A.; Kimberg, C.I.; Radonovich, K.J.; Tillman, M.D.; Chow, J.W.; Lewis, M.H.; Bodfish, J.W.; Hass, C.J. Decreased static and dynamic postural control in children with autism spectrum disorders. Gait Posture 2010, 32, 6–9. [Google Scholar] [CrossRef]
- Rinehart, N.J.; Bellgrove, M.A.; Tonge, B.J.; Brereton, A.V.; Howells-Rankin, D.; Bradshaw, J.L. An Examination of Movement Kinematics in Young People with High-functioning Autism and Asperger’s Disorder: Further Evidence for a Motor Planning Deficit. J. Autism Dev. Disord. 2006, 36, 757–767. [Google Scholar] [CrossRef]
- Schmitz, C.; Martineau, J.; Barthélémy, C.; Assaiante, C. Motor control and children with autism: Deficit of anticipatory function? Neurosci. Lett. 2003, 348, 17–20. [Google Scholar] [CrossRef]
- Martineau, J.; Schmitz, C.; Assaiante, C.; Blanc, R.; Barthélémy, C. Impairment of a cortical event-related desynchronisation during a bimanual load-lifting task in children with autistic disorder. Neurosci. Lett. 2004, 367, 298–303. [Google Scholar] [CrossRef]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35 (Suppl. S2), ii7–ii11. [Google Scholar] [CrossRef]
- Ghez, C.; Hening, W.; Gordon, J. Organization of voluntary movement. Curr. Opin. Neurobiol. 1991, 1, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Lee, M.; Song, C. Balance training improves postural balance, gait, and functional strength in adolescents with intellectual disabilities: Single-blinded, randomized clinical trial. Disabil. Health J. 2016, 9, 416–422. [Google Scholar] [CrossRef]
- Dehghani, M.; Gunay, M. The Effect of Balance Training on Static and Dynamic Balance in Children with Intellectual Disability. J. Appl. Environ. Biol. Sci. 2015, 5, 127–131. [Google Scholar]
- Hsu, T.-Y. Effects of Wii Fit® balance game training on the balance ability of students with intellectual disabilities. J. Phys. Ther. Sci. 2016, 28, 1422–1426. [Google Scholar] [CrossRef]
- Azadeh, M.; Yahya, S.; Reza, S. The Effect of 8 Weeks of Tai Chi Exercises on Girls’ Static and Dynamic Balance with Intellectual Disability. Biol. Forum 2015, 7, 1256–1259. [Google Scholar]
- Teu, K.K.; Kim, W.; Tan, J.; Fuss, F.K. Using dual Euler angles for the analysis of arm movement during the badminton smash. Sports Eng. 2005, 8, 171–178. [Google Scholar] [CrossRef]
- Faude, O.; Meyer, T.; Rosenberger, F.; Fries, M.; Huber, G.; Kindermann, W. Physiological characteristics of badminton match play. Eur. J. Appl. Physiol. 2007, 100, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Masu, Y.; Muramatsu, K.; Hayashi, N. Characteristics of Sway in the Center of Gravity of Badminton Players. J. Phys. Ther. Sci. 2014, 26, 1671–1674. [Google Scholar] [CrossRef]
- Yüksel, M.; Cengiz, A.; Zorba, E.; Gokdemir, K. Effects of Badminton Training on Physical Parameters of Players. Anthropologist 2015, 21, 542–547. [Google Scholar] [CrossRef]
- Singh, J.; Raza, S.; Mohammad, A. Physical Characteristics and Level of Performance in Badminton: A Relationship Study. J. Educ. Pract. 2011, 2, 6–10. [Google Scholar]
- Sheppard, J.M.; Young, W.B. Agility literature review: Classifications, training and testing. J. Sports Sci. 2006, 24, 919–932. [Google Scholar] [CrossRef] [PubMed]
- Güçlüöver, A.; Demirkan, E.; Kutlu, M.; Cigerci, A.E.; Tolga, H.; Üniversitesi, K.; Fakültesi, E.; Eğitimi, B.; Spor, V.; Bölümü, Ö.; et al. The Comparison Of Some Physical And Physiological Features Of Elite Youth National And Amateur Badminton Players. Niğde Üniversitesi Beden Eğitimi Ve Spor Bilim. Derg. 2012, 6, 244–250. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Badminton Intervention Phase I (Sessions 1–12) | Badminton Intervention Phase II (Sessions 13–24) |
|---|---|
| Grips Wrist movements Ready position Basic underhand stroke Low short serve (backhand) Serve returns Underhand net rally | High deep serves Forehand overhead clear Forehand overhead smash Overhand backhand clear Overhand backhand drop |
| Dynamic Warm-Up (10 min) | Badminton Instruction (30 min) | Cooldown (10 min) |
|---|---|---|
| Walking laps (around gym) Arm circles and swings Heel walks Toe walks Walking quadriceps stretch Lunges Side Shuffles | Introduction of new skill (5 min) Practice with TD peer through drills (previous skills and new skills) (15 min) Game play (10 min) | Cross arm stretch Hamstring stretch Quadriceps stretch Rounded back stretch Butterfly stretch |
| Dependent Variables | Independent Variables | Controlled Variables |
|---|---|---|
| COP Average displacement (A/P) direction (in.) COP Average displacement (M/L) direction (in.) COP average 95% ellipsoid area (in2) COP average velocity (ft/s) COP average length (in) | Groups (IDD and TD) Time of testing (Pre, Mid, Post) Balance Testing Conditions (EO, EC, FEO, FEC, 1LEO) | Groups– IDD CONTR and TD CONTR |
| Variable (Condition) | Main Effect or Interaction | F-Value | p-Value | ηp2 | Post Hoc Pairwise Comparisons and p-Values |
|---|---|---|---|---|---|
| Average Velocity (EO) | Time × Group Interaction (IDD-BADM) | F (2, 12) = 7.415 | 0.030 | 0.673 | Pre > Mid p = 0.002 Pre > Post p = 0.006 |
| Average Length (EO) | Time × Group Interaction (IDD-BADM) | F (2, 12) = 7.422 | 0.030 | 0.553 | Pre > Mid p = 0.002 Pre > Post p = 0.006 |
| 95% Ellipsoid Area (EO) | Time × Group Interaction (IDD-BADM) | F (2, 12) = 3.934 | 0.049 | 0.396 | Pre > Mid p = 0.048 |
| Average Displacement in M/L direction (EO) | Time Main Effect (TD) | F (2, 12) = 15.814 | 0.001 | 0.725 | Pre > Post p = 0.005 Mid > Post p = 0.001 |
| Average Displacement in A/P direction (EO) | Time Main Effect (TD) | F (2, 12) = 10.494 | 0.006 | 0.636 | Pre < Post p = 0.017 Mid < Post p = 0.003 |
| Average Displacement in M/L direction (EC) | Time Main Effect (TD) | F (2, 12) = 12.146 | 0.004 | 0.669 | Pre > Post p = 0.002 Mid > Post p = 0.005 |
| Average Displacement in A/P direction (FEO) | Time-Main Effect (IDD) | F (2, 12) = 5.708 | 0.040 | 0.488 | Pre > Mid p = 0.048 Pre > Post p = 0.031 |
| Average Displacement in M/L direction (FEO) | Time-Main Effect (TD) | F (2, 12) = 11.416 | 0.005 | 0.530 | Pre > Post p = 0.003 Mid > Post p = 0.007 |
| Average Displacement in A/P direction (FEO) | Time-Main Effect (TD) | F (2, 12) = 13.709 | 0.005 | 0.696 | Pre < Post p = 0.005 Mid < Post p = 0.001 |
| Average Displacement in M/L direction (FEC) | Time-Main Effect (TD) | F (2, 12) = 9.489 | 0.004 | 0.613 | Pre > Post p = 0.003 |
| Average Displacement in A/P direction (1LEO) | Time × Group Interaction (IDD-BADM) | F (2, 12) = 4.621 | 0.036 | 0.435 | Pre > Post p = 0.022 |
| Sway Measurement/Condition | Group | Time | Mean and SD |
|---|---|---|---|
| Average Velocity (EO) | IDD-BADM (Time × Group Interaction) | Pre-Test Mid-Test Post-Test | 1.302 ± 0.451 0.966 ± 0.348 0.928 ± 0.278 |
| Average Length (EO) | IDD-BADM (Time × Group Interaction) | Pre-Test Mid-Test Post-Test | 26.039 ± 9.021 19.322 ± 6.953 18.556 ± 5.552 |
| 95% Ellipsoid Area (EO) | IDD- BADM | Pre-Test Mid-Test Post-Test | 2.305 ± 1.0210.994 ± 0.560 0.869 ± 0.186 |
| IDD-CONTR | Pre-Test Mid-Test Post-Test | 1.272 ± 0.497 0.932 ± 0.587 1.482 ± 0.066 | |
| Average Displacement in M/L direction (EO) | TD-BADM | Pre-Test Mid-Test Post-Test | 0.135 ± 0.032 0.167 ± 0.051 0.113 ± 0.032 |
| TD-CONTR | Pre-Test Mid-Test Post-Test | 0.175 ± 0.022 0.185 ± 0.018 0.058 ± 0.021 | |
| Average Displacement in M/L direction (EC) | TD-BADM | Pre-Test Mid-Test Post-Test | 0.143 ± 0.044 0.149 ± 0.047 0.078 ± 0.026 |
| TD-CONTR | Pre-Test Mid-Test Post-Test | 0.174 ± 0.043 0.151 ± 0.058 0.078 ± 0.036 | |
| Average Displacement in A/P direction (FEO) | IDD-BADM | Pre-Test Mid-Test Post-Test | 0.501 ± 0.121 0.294 ± 0.075 0.281 ± 0.066 |
| IDD-CONTR | Pre-Test Mid-Test Post-Test | 0.389 ± 0.141 0.360 ± 0.089 0.352 ± 0.035 | |
| TD-BADM | Pre-Test Mid-Test Post-Test | 0.284 ± 0.109 0.232 ± 0.037 0.139 ± 0.040 | |
| TD-CONTR | Pre-Test Mid-Test Post-Test | 0.232 ± 0.055 0.305 ± 0.059 0.133 ± 0.028 | |
| TD-BADM | Pre-Test Mid-Test Post-Test | 0.176 ± 0.029 0.146 ± 0.036 0.222 ± 0.055 | |
| TD-CONTR | Pre-Test Mid-Test Post-Test | 0.150 ± 0.019 0.148 ± 0.015 0.261 ± 0.076 | |
| Average Displacement in M/L direction (FEC) | TD-BADM | Pre-Test Mid-Test Post-Test | 0.186 ± 0.019 0.184 ± 0.039 0.127 ± 0.041 |
| TD-CONTR | Pre-Test Mid-Test Post-Test | 0.210 ± 0.050 0.151 ± 0.032 0.113 ± 0.011 | |
| Average Displacement in A/P direction (1LEO) | IDD-BADM (Time × Group Interaction) | Pre-Test Mid-Test Post-Test | 0.982 ± 0.548 0.852 ± 0.589 0.829 ± 0.580 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turner, A.J.; Chander, H.; Kodithuwakku Arachchige, S.N.K.; Griffith, A.; Chen, P.-L.; Chen, C.-C.; Knight, A.C.; Bates-Brantley, K.; Stratton-Gadke, K.; Smith, J.C. The Effects of an Inclusive Badminton Program on Static Postural Control for Individuals with Intellectual and Developmental Disabilities. Int. J. Environ. Res. Public Health 2024, 21, 210. https://doi.org/10.3390/ijerph21020210
Turner AJ, Chander H, Kodithuwakku Arachchige SNK, Griffith A, Chen P-L, Chen C-C, Knight AC, Bates-Brantley K, Stratton-Gadke K, Smith JC. The Effects of an Inclusive Badminton Program on Static Postural Control for Individuals with Intellectual and Developmental Disabilities. International Journal of Environmental Research and Public Health. 2024; 21(2):210. https://doi.org/10.3390/ijerph21020210
Chicago/Turabian StyleTurner, Alana J., Harish Chander, Sachini N. K. Kodithuwakku Arachchige, Aaron Griffith, Po-Lin Chen, Chih-Chia (JJ) Chen, Adam C. Knight, Kayla Bates-Brantley, Kasee Stratton-Gadke, and J. Chadwick Smith. 2024. "The Effects of an Inclusive Badminton Program on Static Postural Control for Individuals with Intellectual and Developmental Disabilities" International Journal of Environmental Research and Public Health 21, no. 2: 210. https://doi.org/10.3390/ijerph21020210
APA StyleTurner, A. J., Chander, H., Kodithuwakku Arachchige, S. N. K., Griffith, A., Chen, P.-L., Chen, C.-C., Knight, A. C., Bates-Brantley, K., Stratton-Gadke, K., & Smith, J. C. (2024). The Effects of an Inclusive Badminton Program on Static Postural Control for Individuals with Intellectual and Developmental Disabilities. International Journal of Environmental Research and Public Health, 21(2), 210. https://doi.org/10.3390/ijerph21020210