
Comparative Study on the Periodontal Parameters Used in Diagnosing Periodontitis in Puerperae and Periodontitis’ Relationship with the Birth of Preterm Infants: A Case-Control Study


 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
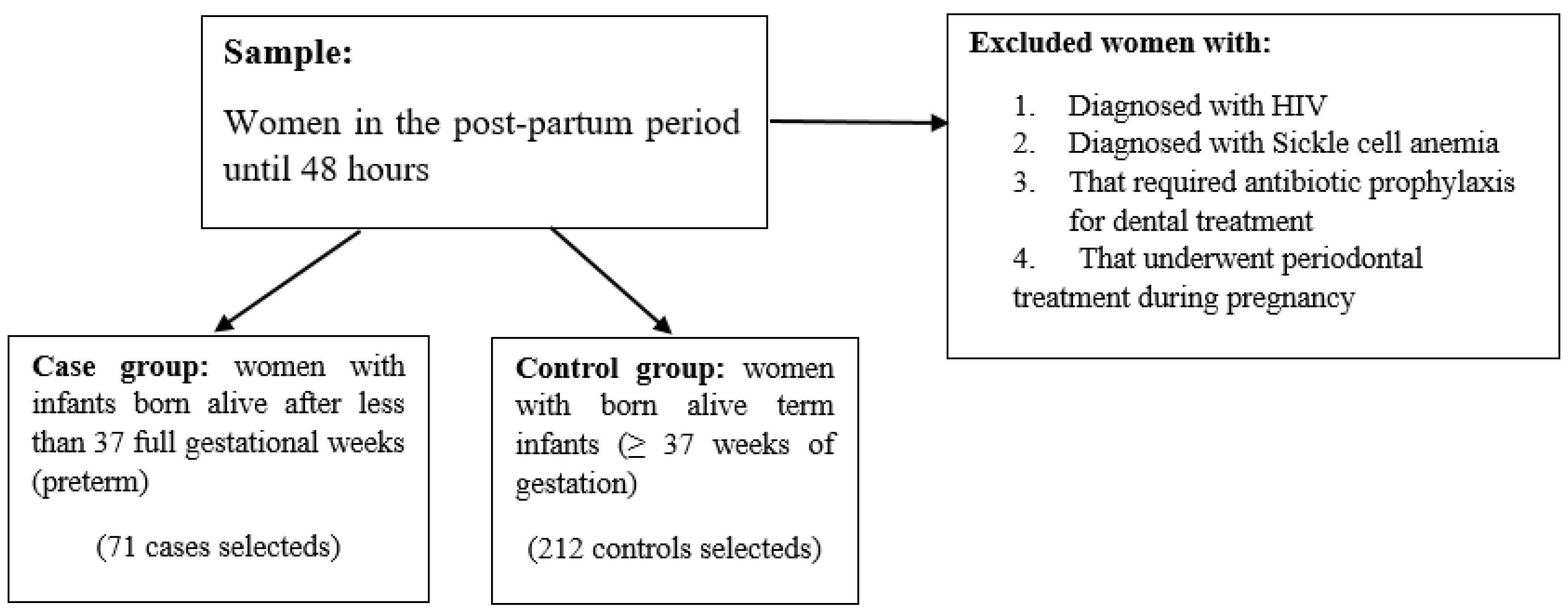
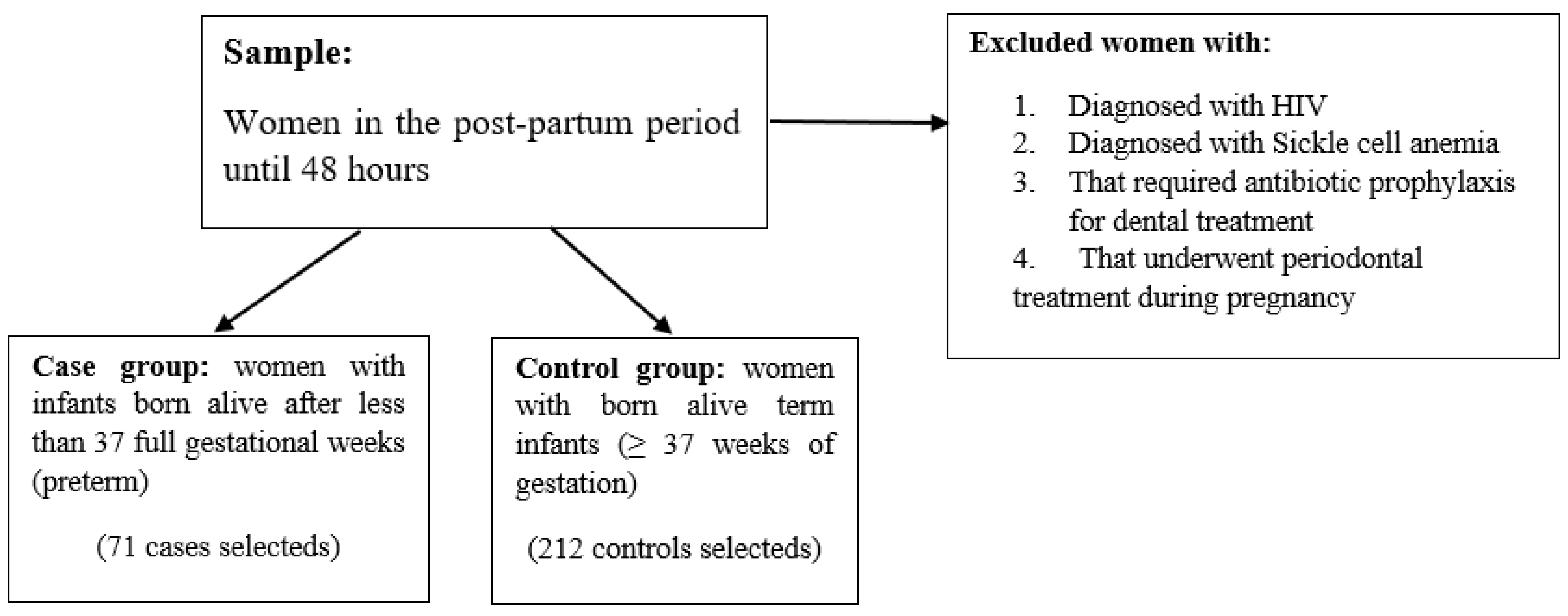
2.1. Study Design and Sample Selection
2.2. Periodontal Evaluation
2.3. Periodontitis Diagnostic Criteria
2.4. Statistical Analysis
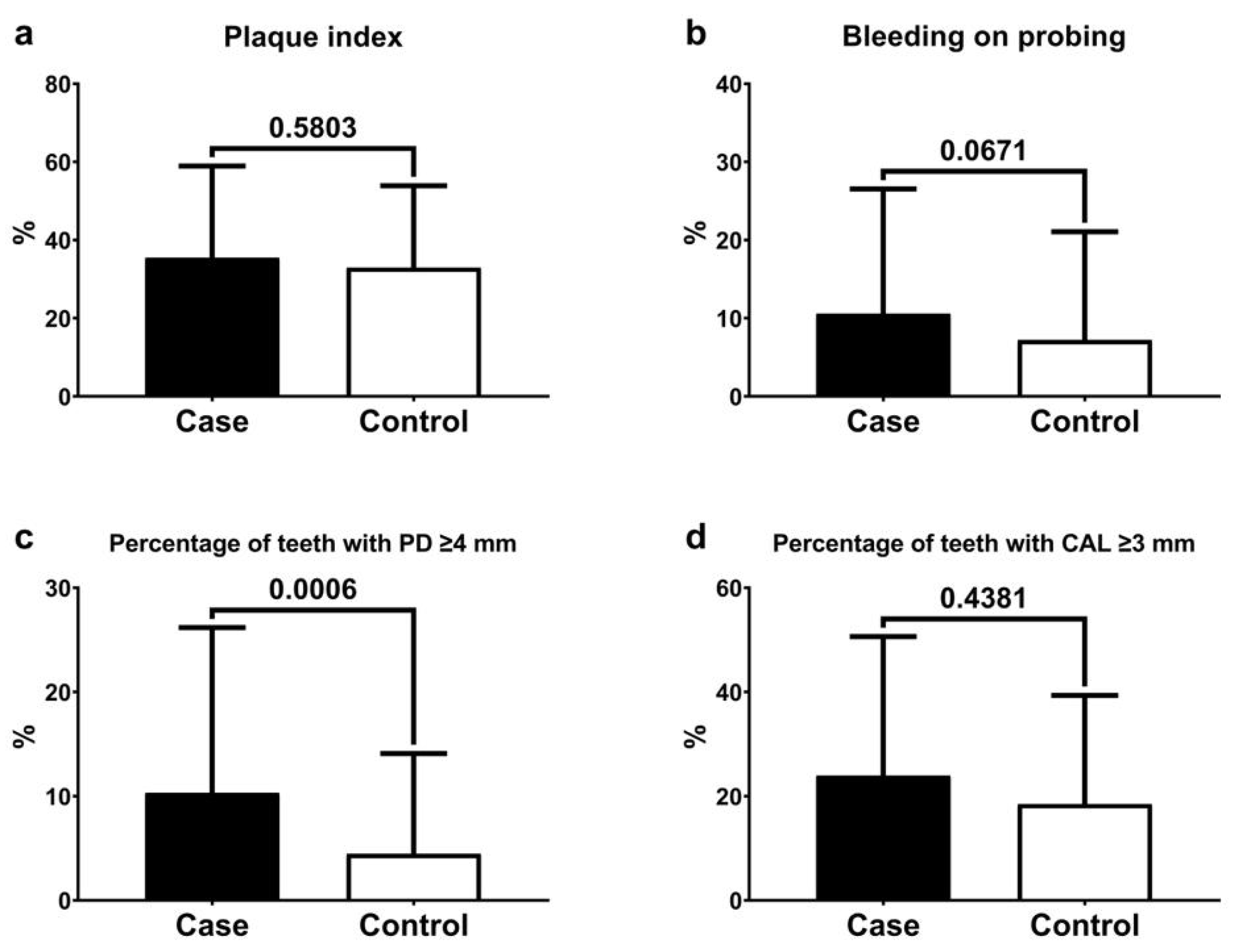
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S149–S161. [Google Scholar] [CrossRef]
- Favero, V.; Bacci, C.; Volpato, A.; Bandiera, M.; Favero, L.; Zanette, G. Pregnancy and dentistry: A literature review on risk management during dental surgical procedures. Dent. J. 2021, 9, 46. [Google Scholar] [CrossRef]
- Figueiredo, M.G.O.P.; Takita, S.Y.; Dourado, B.M.R.; Mendes, H.d.S.; Terakado, E.O.; Nunes, H.R.d.C.; da Fonseca, C.R.B. Periodontal disease: Repercussions in pregnant woman and newborn health-a cohort study. PLoS ONE 2019, 14, e0225036. [Google Scholar] [CrossRef]
- Escobar-Arregoces, F.; Latorre-Uriza, C.; Velosa-Porras, J. Inflammatory response in pregnant women with a high risk of preterm delivery and its relationship with periodontal disease: A pilot study. Acta Odontol. Latinoam. 2018, 31, 53–57. [Google Scholar] [PubMed]
- Puertas, A.; Magan-Fernandez, A.; Blanc, V.; Revelles, L.; O’Valle, F.; Pozo, E.; León, R.; Mesa, F. Association of periodontitis with preterm birth and low birth weight: A comprehensive review. J. Matern. Fetal Neonatal Med. 2018, 31, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Bobetsis, Y.A.; Graziani, F.; Gürsoy, M.; Madianos, P.N. Periodontal disease and adverse pregnancy outcomes. Periodontology 2000, 83, 154–174. [Google Scholar] [CrossRef]
- Lopez, N.J.; Smith, P.C.; Gutierrez, J. Periodontal therapy may reduce the risk of preterm low birth weight in women with periodontal disease: A randomized controlled trial. J. Periodontol. 2002, 73, 911–924. [Google Scholar] [CrossRef]
- Sanz, M.; Kornman, K.; Working Group 3 of the Joint EFP/AAP Workshop. Periodontitis and adverse pregnancy outcomes: Consensus report of the Joint EFP/AAP workshop on periodontitis and systemic diseases. J. Clin. Periodontol. 2013, 40, S164–S169. [Google Scholar] [CrossRef] [PubMed]
- Lawn, J.E.; Blencowe, H.; Oza, S.; You, D.; Lee, A.C.; Waiswa, P.; Lalli, M.; Bhutta, Z.; Barros, A.J.D.; Christian, P.; et al. Lancet Every Newborn Study Group. Every Newborn: Progress, priorities, and potential beyond survival. Lancet 2014, 384, 189–205, Erratum in: Lancet 2014, 384, 132.. [Google Scholar] [CrossRef]
- Karimi, N.; Samiee, N.; Moradi, Y. The association between periodontal disease and adverse maternal or neonatal outcomes risk: A systematic review and meta-analysis of analytical observational studies. Health Sci. Rep. 2023, 6, e1630. [Google Scholar] [CrossRef]
- Gomes-Filho, I.S.; Cruz, S.S.; Rezende, E.J.; Dos Santos, C.A.S.T.; Soledade, K.R.; Magalhães, M.A.; De Azevedo, A.C.O.; Trindade, S.C.; Vianna, M.I.P.; Passos, J.d.S.; et al. Exposure measurement in the association between periodontal disease and prematurity/low birth weight. J. Clin. Periodontol. 2007, 34, 957–963. [Google Scholar] [CrossRef]
- Oliveira, M.C.; Vellarde, G.C.; Sá, R.A.M. Entendendo a pesquisa clínica IV: Estudos de caso controle. Feminina 2015, 43, 176–180. [Google Scholar]
- Brasil Ministério da Saúde; Secretaria de Vigilância em Saúde; SBBrasil. Pesquisa Nacional de Saúde Bucal: Resultados Principais; DF: Brasília, Brazil, 2012.
- Critério de Classificação Econômica do Brasil. Associação Brasileira de Pesquisa de Mercado. Available online: http://www.abep.org/criterio-brasil (accessed on 20 July 2023).
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent J. 1975, 25, 229–235. [Google Scholar] [PubMed]
- Gomes Filho, I.S.; Macedo, T.C.N.; Cruz, S.S.; Soledade, K.R.; Trindade, S.C.; Sarmento, V.A. Comparison of clinical diagnosis criteria to establish periodontal disease. Rev. Odonto Ciência (PUCRS) 2006, 21, 77–81. [Google Scholar]
- Bassani, D.G.; Olinto, M.T.A.; Kreiger, N. Periodontal disease and perinatal outcomes: A case-control study. J. Clin. Periodontol. 2007, 34, 31–39. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Oral Health Survey: Basic Methods; WHO Library Ca: Geneva, Switzerland, 2013. [Google Scholar]
- López, N.J.; Smith, P.C.; Gutiérrez, J. Higher risk of preterm birth and low birth weight in women with periodontal disease. J. Den. Res. 2002, 8, 58–63. [Google Scholar] [CrossRef]
- Armitage, G. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Radnai, M.; Gorzó, I.; Urbán, E.; Eller, J.; Novák, T.; Pál, A. Possible association between mother’s periodontal status and preterm delivery. J. Clin. Periodontol. 2006, 33, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Macedo, J.F.; Ribeiro, R.A.; Machado, F.C.; Assis, N.M.S.P.; Alves, R.T.; Oliveira, A.S.; Ribeiro, L.C. Periodontal disease and oral health-related behavior as factors associated with preterm birth: A case–control study in south-eastern. Brazil. J. Periodontal. Res. 2014, 49, 458–464. [Google Scholar] [CrossRef]
- Hsieh, K.; Murthy, S.; Heller, T.; Rimmer, J.H.; Yen, G. Reported gum disease as a cardiovascular risk factor in adults with intellectual disabilities. J. Intellect. Disabil. Res. 2018, 62, 187–198. [Google Scholar] [CrossRef]
- Vivares-Builes, A.M.; Rangel-Rincón, L.J.; Botero, J.E.; Agudelo-Suárez, A.A. Gaps in Knowledge About the Association Between Maternal Periodontitis and Adverse Obstetric Outcomes: An Umbrella Review. J. Evid. Based Dent. Pract. 2018, 18, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.J.; Cademartori, M.G.; Schuch, H.S.; Barros, F.C.; Silveira, M.F.; Correa, M.B.; Demarco, F.F. Periodontal disease and preterm birth: Findings from the 2015 Pelotas birth cohort study. Oral Dis. 2021, 27, 1519–1527. [Google Scholar] [CrossRef]
- Márquez-Corona, M.D.L.; Tellez-Girón-Valdez, A.; Pontigo-Loyola, A.P.; Islas-Zarazúa, R.; Robles-Bermeo, N.L.; Gonzalez-López, B.S.; Medina-Solís, C.E. Preterm birth associated with periodontal and dental indicators: A pilot case-control study in a developing country. J. Matern.-Fetal Neonatal Med. 2021, 34, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Ide, M.; Papapanou, P.N. Epidemiology of association between maternal periodontal disease and adverse pregnancy outcomes—Systematic review. J. Periodontol. 2013, 84, S181–S194. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.D.; Offenbacher, S. Relationship among clinical measures of periodontal disease and their association with systemic markers. Ann. Periodontol. 2002, 7, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Page, R.C.; Eke, P.I. Case definitions for use in population-based surveillance of periodontitis. J. Periodontol. 2007, 78, 1387–1399. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 45, 162–170. [Google Scholar]
- Rakoto-Alson, S.; Tenebaum, H.; Davideau, J.L. Periodontal diseases, preterm births, and low birth weight: Findings from a homogeneous cohort of women in Madagascar. J. Periodontol. 2010, 81, 205–213. [Google Scholar] [CrossRef]
- Vieira, A.C.F.; Alves, C.M.C.; Rodrigues, V.P.; Ribeiro, C.C.; Gomes-Filho, I.S.; Lopes, F.F. Oral, systemic, and socioeconomic factors associated with preterm birth. Women Birth. 2019, 32, e12–e16. [Google Scholar] [CrossRef]
- Manau, C.; Echeverria, A.; Agueda, A.; Guerrero, A.; Echeverria, J.J. Periodontal disease definition may determine the association between periodontitis and pregnancy outcomes. J. Clin. Periodontol. 2008, 35, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Setia, M.S. Methodology Series Module 2: Case-control Studies. Indian J. Dermatol. 2016, 61, 146–151. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Covariates | Case | Control | p-Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Sociodemographic factors | |||||
| Age group | 0.406 | ||||
| 18 to 20 years | 12 | 16.9 | 51 | 24.1 | |
| 21 to 35 years | 52 | 73.2 | 138 | 65.1 | |
| 36 to 43 years | 7 | 9.9 | 23 | 10.8 | |
| Household income | 0.462 | ||||
| Up to one minimum wage | 32 | 48.5 | 87 | 43.3 | |
| More than one minimum wage | 34 | 51.5 | 114 | 56.7 | |
| Educational level | 0.054 | ||||
| 0–8 years of schooling | 25 | 35.2 | 50 | 23.6 | |
| More than 8 years of schooling | 46 | 64.8 | 162 | 76.4 | |
| Social class a | 0.086 | ||||
| B | 6 | 8.5 | 30 | 14.2 | |
| C | 40 | 56.3 | 132 | 62.9 | |
| D and E | 25 | 35.2 | 48 | 22.9 | |
| Previous obstetric history | |||||
| Parity | 0.887 | ||||
| Primiparous | 32 | 45.1 | 93 | 44.1 | |
| Multiparous | 39 | 54.9 | 118 | 55.9 | |
| Previous preterm delivery (<37 weeks) | 0.225 | ||||
| Yes | 8 | 24.2 | 17 | 15.2 | |
| No | 25 | 75.8 | 95 | 84.8 | |
| Previous low weight delivery (<2500 g) | 0.190 | ||||
| Yes | 8 | 24.2 | 16 | 14.5 | |
| No | 25 | 75.8 | 94 | 85.5 | |
| Current obstetric history | |||||
| Arterial hypertension | <0.001 * | ||||
| Yes | 33 | 46.5 | 40 | 19.0 | |
| No | 38 | 53.5 | 171 | 81.0 | |
| Eclampsia | 1.000 | ||||
| Yes | 2 | 2.8 | 5 | 2.4 | |
| No | 69 | 97.2 | 207 | 97.6 | |
| Hyperemesis gravidarum | 0.120 | ||||
| Yes | 6 | 9.0 | 8 | 4.0 | |
| No | 61 | 91.0 | 194 | 96.0 | |
| Urinary infection | 1.000 | ||||
| Yes | 23 | 32.9 | 69 | 32.5 | |
| No | 47 | 67.1 | 143 | 67.5 | |
| Predictor | Estimated | Standard Error | p-Value |
|---|---|---|---|
| Educational level (Reference: ≤8 years) | |||
| >8 years of schooling | −1.42 | 1.06 | 0.181 |
| Arterial hypertension (reference: No) | |||
| Yes | 3.49 | 1.02 | <0.001 |
| Social (reference: B class) | |||
| C class | 3.88 | 1.97 | 0.051 |
| D-E class | 2.7 | 2.37 | 0.257 |
| Diagnostic Criteria | Periodontitis Frequency (%) | Crude OR (95% CI) | p-Value | Adjusted OR a (95% CI) | p-Value | |
|---|---|---|---|---|---|---|
| Case | Control | |||||
| Criterion 1 | 49.3 | 32.1 | 2.05 (1.19–3.55) | 0.009 * | 1.76 (0.98–3.14) | 0.054 |
| Criterion 2 | 40.8 | 24.5 | 2.12 (1.20–3.74) | 0.008 * | 1.65 (0.90–3.02) | 0.100 |
| Criterion 3 | 32.4 | 21.2 | 1.77 (0.97–3.22) | 0.056 | 1.38 (0.73–2.61) | 0.317 |
| Criterion 4 | 40.0 | 15.1 | 2.52 (1.34–4.73) | 0.003 * | 1.95 (0.99–3.80) | 0.050 |
| Criterion 5 | 39.4 | 21.7 | 2.34 (1.31–4.18) | 0.003 * | 1.85 (1.01–3.43) | 0.049 * |
| Criterion 6 | 35.2 | 13.7 | 3.42 (1.83–6.40) | <0.001 * | 2.55 (1.30–4.99) | 0.006 * |
| Criterion 7 | 28.2 | 9.9 | 3.56 (1.79–7.08) | <0.001 * | 2.69 (1.30–5.56) | 0.007 * |
| Criterion 8 b | 22.5 | 7.1 | 3.82 (1.77–8.21) | <0.001 * | 2.60 (1.14–5.89) | 0.021 * |
| Criterion 9 | 57.7 | 54.2 | 1.15 (0.66–1.98) | 0.607 | 0.89 (0.50–1.60) | 0.720 |
| Criterion 10 | 45.1 | 27.4 | 2.17 (1.24–3.80) | 0.005 * | 1.89 (1.05–3.42) | 0.032 * |
| Criterion 11 | 26.7 | 11.3 | 2.86 (1.45–5.62) | 0.001 * | 2.10 (1.01–4.33) | 0.044 * |
| Criterion 12 | 49.3 | 34.4 | 1.85 (1.07–3.19) | 0.025 * | 1.46 (0.82–2.61) | 0.195 |
| Criterion 13 | 11.3 | 7.1 | 1.66 (0.67–4.11) | 0.263 | 1.44 (0.55–3.74) | 0.451 |
| Criterion 14 | 47.9 | 30.7 | 2.07 (1.19–3.60) | 0.008 * | 1.77 (0.99–3.17) | 0.051 |
| Diagnostic Criteria | n | % | Sensitivity (%) (95% CI) | Specificity (%) (95% CI) | PPV (%) (95% CI) | NPV (%) (95% CI) |
|---|---|---|---|---|---|---|
| Criterion 1 | 103 | 36.4 | 100 (86.3–100) | 71.4 (65.3–76.8) | 30.1 (21.6–40.0) | 100 (97.4–100) |
| Criterion 2 | 81 | 28.6 | 100 (86.3–100) | 80.1 (74.5–84.7) | 38.3 (27.9–49.8) | 100 (97.7–100) |
| Criterion 3 | 68 | 24.0 | 100 (86.3–100) | 85.3 (80.2–89.3) | 45.6 (33.6–58.0) | 100 (97.8–100) |
| Criterion 4 | 54 | 19.1 | 100 (86.3–100) | 90.9 (86.4–94.0) | 57.4 (43.3–70.5) | 100 (97.9–100) |
| Criterion 5 | 74 | 26.2 | 100 (86.3–100) | 82.9 (77.6–87.2) | 41.9 (30.7–53.9) | 100 (97.7–100) |
| Criterion 6 | 54 | 19.1 | 100 (86.3–100) | 90.9 (86.4–94.0) | 57.4 (43.3–70.5) | 100 (97.9–100) |
| Criterion 7 | 41 | 14.5 | 100 (86.3–100) | 96.0 (92.6–97.9) | 75.6 (59.3–87.0) | 100 (98.0–100) |
| Criterion 9 | 156 | 55.1 | 100 (86.3–100) | 50.4 (44.1–56.7) | 19.9 (14.1–27.1) | 100 (96.3–100) |
| Criterion 10 | 90 | 31.8 | 100 (86.3–100) | 76.6 (70.8–81.6) | 34.4 (24.9–45.3) | 100 (97.6–100) |
| Criterion 11 | 43 | 15.2 | 100 (86.3–100) | 95.2 (91.6–97.4) | 72.0 (56.1–84.2) | 100 (98.0–100) |
| Criterion 12 | 108 | 38.2 | 100 (86.3–100) | 69.4 (63.2–74.9) | 28.7 (20.6–38.3) | 100 (97.3–100) |
| Criterion 13 | 23 | 8.1 | 45.2 (27.7–63.7) | 96.4 (93.1–98.2) | 60.8 (38.7–79.5) | 93.4 (89.5–96.0) |
| Criterion 14 | 99 | 35.0 | 100 (86.3–100) | 73.0 (67.0–78.3) | 31.3 (22.6–41.5) | 100 (97.4–100) |
| Criterion 8 b | 31 | 10.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Vasconcelos Calixto, N.R.; Lopes, F.F.; Franco, M.M.P.; Gomes-Filho, I.S.; Benatti, B.B.; Alves, C.M.C. Comparative Study on the Periodontal Parameters Used in Diagnosing Periodontitis in Puerperae and Periodontitis’ Relationship with the Birth of Preterm Infants: A Case-Control Study. Int. J. Environ. Res. Public Health 2024, 21, 156. https://doi.org/10.3390/ijerph21020156
de Vasconcelos Calixto NR, Lopes FF, Franco MMP, Gomes-Filho IS, Benatti BB, Alves CMC. Comparative Study on the Periodontal Parameters Used in Diagnosing Periodontitis in Puerperae and Periodontitis’ Relationship with the Birth of Preterm Infants: A Case-Control Study. International Journal of Environmental Research and Public Health. 2024; 21(2):156. https://doi.org/10.3390/ijerph21020156
Chicago/Turabian Stylede Vasconcelos Calixto, Nayra Rodrigues, Fernanda Ferreira Lopes, Marcela Mayana Pereira Franco, Isaac Suzart Gomes-Filho, Bruno Braga Benatti, and Cláudia Maria Coêlho Alves. 2024. "Comparative Study on the Periodontal Parameters Used in Diagnosing Periodontitis in Puerperae and Periodontitis’ Relationship with the Birth of Preterm Infants: A Case-Control Study" International Journal of Environmental Research and Public Health 21, no. 2: 156. https://doi.org/10.3390/ijerph21020156
APA Stylede Vasconcelos Calixto, N. R., Lopes, F. F., Franco, M. M. P., Gomes-Filho, I. S., Benatti, B. B., & Alves, C. M. C. (2024). Comparative Study on the Periodontal Parameters Used in Diagnosing Periodontitis in Puerperae and Periodontitis’ Relationship with the Birth of Preterm Infants: A Case-Control Study. International Journal of Environmental Research and Public Health, 21(2), 156. https://doi.org/10.3390/ijerph21020156