Gender, Mental Health Stigma, and Help-Seeking in Arabic- and Swahili-Speaking Communities in Australia

 ,
,  , , and
, , and
Abstract
1. Introduction
1.1. Mental Health of CaLD Communities
1.2. Help-Seeking Among CaLD Communities
1.3. Stigma in CaLD Communities
1.4. Gender Differences in Stigma and Help-Seeking
1.5. ‘What Matters Most’ Framework
1.6. Current Study
2. Methods
2.1. Study Design and Context
2.2. Participants
2.3. Data Collection
2.4. Data Analysis

{kind=link}
| Step | Description |
|---|---|
| Step 1: Data immersion | English transcripts from the focus group discussions and interviews were read and re-read several times by the primary researcher (analyst) to be familiar with the entire body of data. Informal notes and early impressions were jotted down during this step. |
| Step 2: Data coding | The data were then organised in a meaningful and systematic way using codes. The researcher coded each segment of data according to the domains relevant to the research question, namely, stigma and help-seeking. |
| Step 3: Data categorisation | Fortnightly supervision meetings were held by the researcher with her primary supervisors (S.S-Y. and R.N.) to group initial codes into categories. The connections between the categories were then searched to generate sub-themes and themes. Triangulation of data sources (members and leaders) and collection methods (focus groups discussions and interviews) enabled the researcher to explore a broad range of perspectives and make comparisons within and between the CaLD communities and gender. The regular supervision meetings also enabled the research to consider aspects of analysis including that of reflexivity, also addressed through note keeping. |
| Step 4: Theme mapping from categories | At this step, the preliminary themes were reviewed and modified based on whether the data supported the theme and whether the themes work in the context of the entire data set. The previous papers published under this project were also reviewed to identify if preliminary themes found were in line with previous research and were value-adding to the overall research topic. |
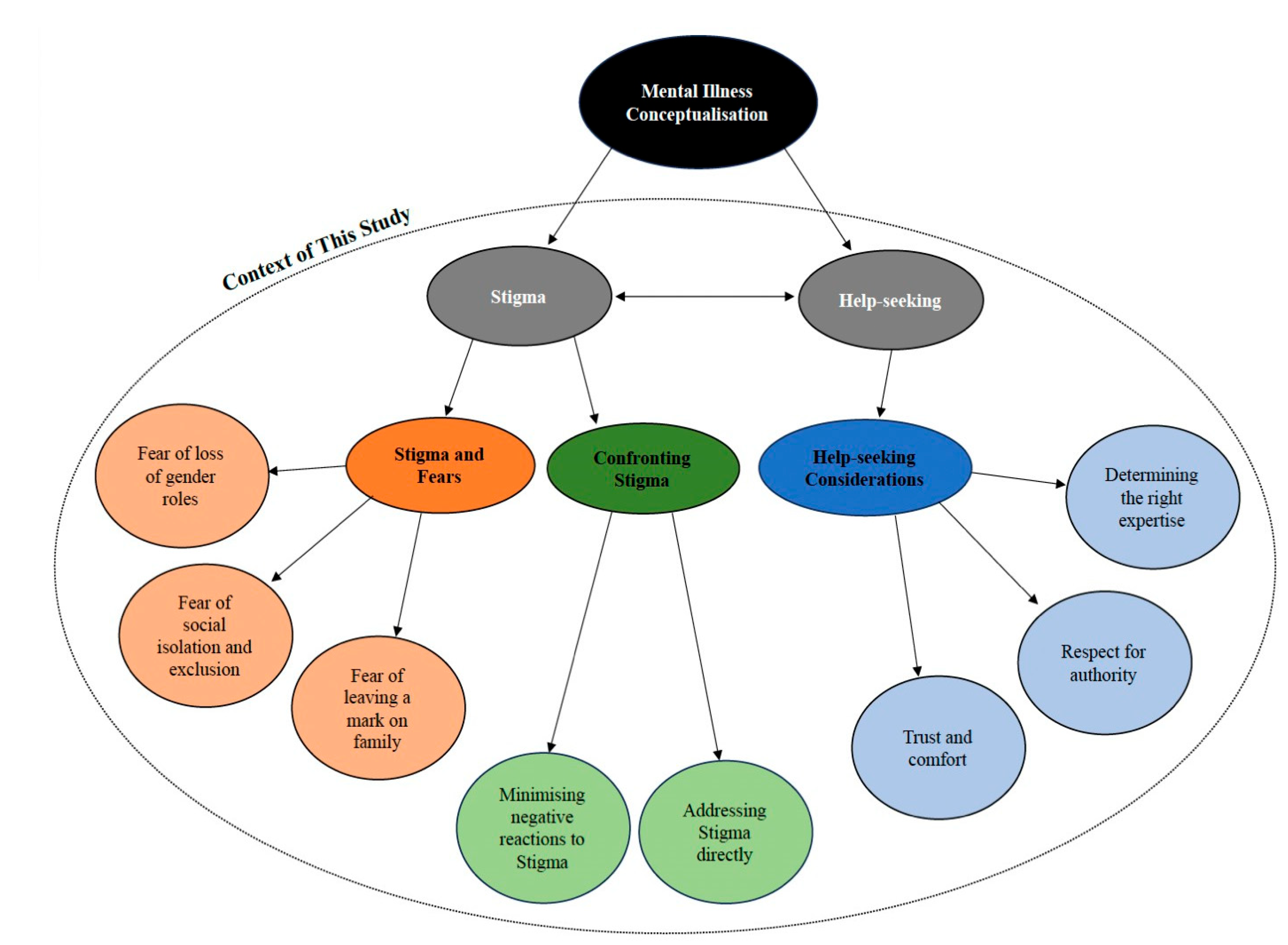
| Step 5: Define and finalise themes | At this step, supervision meetings were held on a weekly basis. The themes underwent a final refinement to identify the ‘essence’ of what each theme is about and whether the sub-themes interacted and related to the main theme. A thematic map (see Figure 1) that illustrated the relationships between the themes was also created to aid in the refinement process. Feedback regarding the cultural sensitivity of the themes and sub-themes found, as well as comments regarding the application of these findings were discussed. This meeting aided in the descriptive validity and transparency of interpretation. |
| Step 6: Write up | Lastly, once the main themes and sub-themes were finalised, the information was written up. This comprised of an existing literature review, reporting of the findings, as well as a discussion of the applications, strengths, and limitations of the findings. |
3. Results
3.1. Theme 1: Stigma and Fear
3.1.1. Sub-Theme: Fear of Loss of Gender Roles
3.1.2. Sub-Theme: Fear of Social Isolation and Exclusion
3.1.3. Sub-Theme: Fear of Leaving a Mark on Family
3.2. Theme 2: Confronting Stigma
3.2.1. Sub-Theme: Minimising Negative Reactions to Stigma
3.2.2. Sub-Theme: Addressing Stigma Directly
3.3. Theme 3: Help-Seeking Considerations
3.3.1. Sub-Theme: Trust and Comfort
3.3.2. Sub-Theme: Respect for Authority
3.3.3. Sub-Theme: Determining the Right Expertise
4. Discussion
4.1. Theoretical Implications
4.2. Clinical Implications
4.3. Public Health Implications
4.4. Limitations and Strengths of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Department of Home Affairs. Permanent Settlers (Humanitarian Stream) in All States/Territories with a Date of Settlement Between 01 Jul 2014 and 30 Jun 2024 by Age Band, Gender, English Proficiency, Marital Status, LGA, Country of Birth, Ethnicity, Religion, Language, Year of Settlement, Financial Year Settlement and Visa Subclass. Department of Home Affairs, 2024. Available online: https://data.gov.au/data/dataset/settlement-reports/resource/f9669dbd-ea7e-4c93-a23c-ef1e3d9e0493 (accessed on 29 October 2024).
- Johnson, K.; Scott, J.; Rughita, B.; Kisielewski, M.; Asher, J.; Ong, R.; Lawry, L. Association of sexual violence and human rights violations with physical and mental health in territories of the Eastern Democratic Republic of the Congo. JAMA 2010, 304, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare (AIHW). Australian Burden of Disease Study 2022. 2022. Available online: https://www.aihw.gov.au/reports/burden-of-disease/australian-burden-of-disease-study-2022/contents/summary (accessed on 29 October 2024).
- Chu, T.; Keller, A.; Rasmussen, A. Effects of post-migration factors on PTSD outcomes among immigrant survivors of political violence. J. Immigr. Minor. Health 2013, 15, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Ziersch, A.; Due, C.; Walsh, M. Discrimination: A health hazard for people from refugee and asylum-seeking backgrounds resettled in Australia. BMC Public Health 2020, 20, 108. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare (AIHW). Chronic Health Conditions Among Culturally and Linguistically Diverse Australians 2023. 2021. Available online: https://www.aihw.gov.au/reports/cald-australians/chronic-conditions-cald-2021/contents/summary (accessed on 29 October 2024).
- Li, S.S.; Liddell, B.J.; Nickerson, A. The relationship between post-migration stress and psychological disorders in refugees and asylum seekers. Curr. Psychiatry Rep. 2016, 18, 82. [Google Scholar] [CrossRef]
- Kirmayer, L.J.; Narasiah, L.; Munoz, M.; Rashid, M.; Ryder, A.G.; Guzder, J.; Hassan, G.; Rousseau, C.; Pottie, K. Common mental health problems in immigrants and refugees: General approach in primary care. Can. Med. Assoc. J. 2011, 183, 959–967. [Google Scholar] [CrossRef]
- Mwanri, L.; Mude, W. Alcohol, other drugs use and mental health among African migrant youths in South Australia. Int. J. Environ. Res. Public Health 2021, 18, 1534. [Google Scholar] [CrossRef]
- Schlaudt, V.A.; Bosson, R.; Williams, M.T.; German, B.; Hooper, L.M.; Frazier, V.; Carrico, R.; Ramirez, J. Traumatic experiences and mental health risk for refugees. Int. J. Environ. Res. Public Health 2020, 17, 1943. [Google Scholar] [CrossRef]
- Slewa-Younan, S.; Mond, J.M.; Bussion, E.; Melkonian, M.; Mohammad, Y.; Dover, H.; Smith, M.; Milosevic, D.; Jorm, A.F. Psychological trauma and help seeking behaviour amongst resettled Iraqi refugees in attending English tuition classes in Australia. Int. J. Ment. Health Syst. 2015, 9, 5. [Google Scholar] [CrossRef]
- Fauk, N.K.; Ziersch, A.; Gesesew, H.; Ward, P.R.; Green, E.; Oudih, E.; Tahir, R.; Mwanri, L. Migrants and service providers’ perspectives of barriers to accessing mental health services in South Australia: A case of African migrants with a refugee background in South Australia. Int. J. Environ. Res. Public Health 2021, 18, 8906. [Google Scholar] [CrossRef]
- Slewa-Younan, S.; McKenzie, M.; Thomson, R.; Smith, M.; Mohammad, Y.; Mond, J. Improving the mental wellbeing of Arabic speaking refugees: An evaluation of a mental health promotion program. BMC Psychiatry 2020, 20, 314. [Google Scholar] [CrossRef]
- Byrow, Y.; Pajak, R.; Specker, P.; Nickerson, A. Perceptions of mental health and perceived barriers to mental health help-seeking amongst refugees: A systematic review. Clin. Psychol. Rev. 2020, 75, 101–812. [Google Scholar] [CrossRef] [PubMed]
- Kayrouz, R.; Dear, B.F.; Johnston, L.; Keyrouz, L.; Nehme, E.; Laube, R.; Titov, N. Intergenerational and cross-cultural differences in emotional wellbeing, mental health service utilisation, treatment-seeking preferences, and acceptability of psychological treatments for Arab Australians. Int. J. Soc. Psychiatry 2015, 61, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Piwowarczyk, L.; Bishop, H.; Yusuf, A.; Mudymba, F.; Raj, A. Congolese and Somali beliefs about mental health services. J. Nerv. Ment. Dis. 2014, 202, 209–216. [Google Scholar] [CrossRef]
- McCann, T.V.; Mugavin, J.; Renzaho, A.; Lubman, D.I. Sub-Saharan African migrant youths’ help-seeking barriers and facilitators for mental health and substance use problems: A qualitative study. BMC Psychiatry 2016, 16, 275. [Google Scholar] [CrossRef]
- Slewa-Younan, S.; Krstanoska-Blazeska, K.; Blignault, I.; Li, B.; Reavley, N.J.; Renzaho, A.M.N. Conceptualisations of mental illness and stigma in Congolese, Arabic- speaking and Mandarin-speaking communities: A qualitative study. BMC Public Health 2022, 22, 2353. [Google Scholar] [CrossRef]
- Scull, N.C.; Khullar, N.; Al-Awadhi, N.; Erheim, R.A. Qualitative study of the perceptions of mental health Care in Kuwait. Int. Perspect. Psychol. 2014, 3, 284–299. [Google Scholar] [CrossRef]
- Youssef, J.; Deane, F.P. Factors influencing mental-health help-seeking in Arabic- speaking communities in Sydney Australia. Ment. Health Relig. Cult. 2006, 9, 43–66. [Google Scholar] [CrossRef]
- Fauk, N.K.; Ziersch, A.; Gesesew, H.; Ward, P.R.; Mwanri, L. Strategies to improve access to mental health services: Perspectives of African migrants and service providers in South Australia. SSM-Mental Health 2022, 2, 100058. [Google Scholar] [CrossRef]
- McCann, T.V.; Renzaho, A.; Mugavin, J.; Lubman, D.I. Stigma of mental illness and substance misuse in Sub-Saharan African migrants: A qualitative study. Int. J. Ment. Health Nurs. 2018, 27, 956–965. [Google Scholar] [CrossRef]
- Sullivan, C.; Vaughan, C. Migrant and Refugee Women’s Mental Health in Australia: A Literature Review; Multicultural Centre for Women’s Health, School of Population and Global Health, University of Melbourne: Melbourne, Australia, 2020. [Google Scholar]
- Australian Institute of Health and Welfare (AIHW). Culturally and Linguistically Diverse Australians. 2022. Available online: https://www.aihw.gov.au/reports-data/population-groups/cald-australians/overview (accessed on 29 October 2024).
- Said, M.; Boardman, G.; Kidd, S. Barriers to accessing mental health services in Somali-Australian women: A qualitative study. Int. J. Ment. Health Nurs. 2021, 30, 931–938. [Google Scholar] [CrossRef]
- Valibhoy, M.; Szwarc, J.; Kaplan, I. Young service users from refugee backgrounds: Their perspectives on barriers to accessing Australian mental health services. Int. J. Hum. Rights Healthc. 2017, 10, 68–80. [Google Scholar] [CrossRef]
- Jorm, A.F.; Korten, A.E.; Jacomb, P.A.; Christensen, H.; Rodgers, B.; Pollitt, P. “Mental health literacy”: A survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Med. J. Aust. 1997, 166, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Kane, J.C.; Elafros, M.A.; Murray, S.M.; Mitchell EM, H.; Augustinavicius, J.L.; Causevic, S.; Baral, S.D. A scoping review of health-related stigma outcomes for high burden diseases in low- and middle-income countries. BMC Med. 2019, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Penguin: London, UK, 1963. [Google Scholar]
- Corrigan, P.W.; Watson, A.C. The paradox of self-stigma and mental illness. Clin. Psychol. 2002, 9, 35–53. [Google Scholar] [CrossRef]
- Shechtman, Z.; Alim, E.; Brenner, R.E.; Vogel, D.L. Public stigma, self-stigma, and group therapy help-seeking intentions among clinical and non-clinical Arab adults in Israel. Int. J. Cult. Ment. Health 2018, 11, 595–604. [Google Scholar] [CrossRef]
- Ayazi, T.; Lien, L.; Eide, A.; Shadar, E.J.; Hauff, E. Community attitudes and social distance towards the mentally ill in South Sudan: A survey from a post-conflict setting with no mental health services. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 771–780. [Google Scholar] [CrossRef]
- Zolezzi, M.; Alamri, M.; Shaar, S.; Rainkie, D. Stigma associated with mental illness and its treatment in the Arab culture: A systematic review. Int. J. Soc. Psychiatry 2018, 64, 597–609. [Google Scholar] [CrossRef]
- Mitha, K. Conceptualising and addressing mental disorders amongst Muslim communities: Approaches from the Islamic Golden Age. Transcult. Psychiatry 2020, 57, 763–774. [Google Scholar] [CrossRef]
- Omar, Y.S.; Kuay, J.; Tuncer, C. ‘Putting your feet in gloves designed for hands’: Horn of Africa Muslim men perspectives in emotional wellbeing and access to mental health services in Australia. Int. J. Cult. Ment. Health 2017, 10, 376–388. [Google Scholar] [CrossRef]
- Makanjuola, V.; Esan, Y.; Oladeji, B.; Kola, L.; Appiah-Poku, J.; Harris, B.; Othieno, C.; Price, L.; Seedat, S.; Gureje, O. Explanatory model of psychosis: Impact on perception of self-stigma by patients in three Sub-Saharan African cities. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1645–1654. [Google Scholar] [CrossRef]
- Egbe, C.O.; Brooke-Sumner, C.; Kathree, T.; Selohilwe, O.; Thornicroft, G.; Petersen, I. Psychiatric stigma and discrimination in South Africa: Perspectives from key stakeholders. BMC Psychiatry 2014, 14, 191. [Google Scholar] [CrossRef] [PubMed]
- Alqasir, A.; Ohtsuka, K. The Impact of Religio-Cultural Beliefs and Superstitions in Shaping the Understanding of Mental Disorders and Mental Health Treatment among Arab Muslims. J. Spirit. Ment. Health 2023, 26, 279–302. [Google Scholar] [CrossRef]
- Holzinger, A.; Floris, F.; Schomerus, G.; Carta, M.G.; Angermeyer, M.C. Gender differences in public beliefs and attitudes about mental disorder in western countries: A systematic review of population studies. Epidemiol. Psychiatry Sci. 2012, 21, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Hwang, J.; Ball, J.G.; Lee, J.; Yu, Y.; Albright, D.L. Mental health literacy affects mental health attitude: Is there a gender difference? Am. J. Health Behav. 2020, 44, 283–291. [Google Scholar] [CrossRef]
- Sigal, M.; Plunkett, S.W. Gender and ethnic differences in university students’ attitudes about mental health services. J. Coll. Stud. Psychother. 2023, 38, 275–292. [Google Scholar] [CrossRef]
- Lipson, S.K.; Kern, A.; Eisenberg, D.; Breland-Noble, A.M. Mental health disparities among college students of color. J. Adolesc. Health 2018, 63, 348–356. [Google Scholar] [CrossRef]
- Stickney, S.; Yanosky, D.; Black, D.R.; Stickney, N.L. Sociodemographic variables and perceptual moderators related to mental health stigma. J. Ment. Health 2012, 21, 244–256. [Google Scholar] [CrossRef]
- Auerbach, R.; Mortier, P.; Bruffaerts, R.; Alonso, J.; Benjet, C.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; Green, J.G.; Hasking, P.; et al. World Health Organisation world mental health surveys international college student project: Prevalence and distribution of mental disorders. J. Abnorm. Psychol. 2018, 127, 623–638. [Google Scholar] [CrossRef]
- Wu, I.H.C.; Bathje, G.J.; Kalibatseva, Z.; Sung, D.; Leong, F.T.L.; Collins-Eaglin, J. Stigma, mental health, and counselling service use: A person-centered approach to mental health stigma profiles. Psychol. Serv. 2017, 14, 490–501. [Google Scholar] [CrossRef]
- Coen, S.E.; Oliffe, J.L.; Johnson, J.L.; Kelly, M.T. Looking for Mr. PG: Masculinities and men’s depression in a northern resource-based Canadian community. Health Place 2013, 21, 94–101. [Google Scholar] [CrossRef]
- Good, G.E.; Wood, P.K. Male gender role conflict, depression, and help seeking: Do college men face double jeopardy? J. Couns. Dev. 1995, 74, 70–75. [Google Scholar] [CrossRef]
- Mansfield, A.; Addis, M.; Mahalik, J. “Why won’t he go to the doctor?”: The psychology of men’s help seeking. Int. J. Men’s Health 2003, 2, 93–109. [Google Scholar] [CrossRef]
- Nam, S.K.; Chu, H.J.; Lee, M.K.; Lee, J.H.; Kim, N.; Lee, S.M. A meta-analysis of gender differences in attitudes towards seeking professional psychological help. J. Am. Coll. Health 2010, 59, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Seidler, Z.E.; Dawes, A.J.; Rice, S.M.; Oliffe, J.L.; Dhillon, H.M. The role of masculinity in men’s help-seeking for depression: A systematic review. Clin. Psychol. Rev. 2016, 49, 106–118. [Google Scholar] [CrossRef]
- Rugema, L.; Persson, M.; Mogren, I.; Ntaganira, J.; Krantz, G. A qualitative study of healthcare professionals’ perceptions of men and women’s mental healthcare seeking in Rwanda. J. Community Psychol. 2020, 48, 891–903. [Google Scholar] [CrossRef]
- Latalova, K.; Kamaradova, D.; Prasko, J. Perspectives on perceived stigma and self-stigma in adult male patients with depression. Neuropsychiatr. Dis. Treat. 2014, 10, 1399–1405. [Google Scholar] [CrossRef]
- Al-Krenawi, A.; Graham, J.R.; Dean, Y.Z.; Eltaiba, N. Cross-national study of attitudes towards seeking professional help: Jordan, United Arab Emirates (UAE) and Arabs in Israel. Int. J. Soc. Psychiatry 2004, 50, 102–114. [Google Scholar] [CrossRef]
- Yang, L.H.; Thornicroft, G.; Alvarado RVega, E.; Link, B.G. Recent advances in cross-cultural measurement in psychiatric epidemiology: Utilizing ‘what matters most’ to identify culture-specific aspects of stigma. Int. J. Epidemiol. 2014, 43, 494–510. [Google Scholar] [CrossRef]
- Yang, L.H.; Kleinman, A.; Link, B.G.; Phelan, J.C.; Lee, S.; Good, B. Culture and stigma: Adding moral experience to stigma theory. Soc. Sci. Med. 2007, 64, 1524–1535. [Google Scholar] [CrossRef]
- Schomerus, G.; Angermeyer, M. Blind spots in stigma research? Broadening our perspective on mental illness stigma by exploring ‘what matters most’ in modern Western societies. Epidemiol. Psychiatr. Sci. 2021, 30, e26. [Google Scholar] [CrossRef]
- Kpanake, L. Cultural concepts of the person and mental health in Africa. Transcult. Psychiatry 2018, 55, 198–218. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Madsen, J.; Jobson, L.; Slewa-Younan, S.; Li, H.; King, K. Mental health literacy among Arab men living in high-income Western countries: A systematic review and narrative synthesis. Soc. Sci. Med. 2024, 346, 116718. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association (APA). Clinical Practice Guideline for the Treatment of Depression Across Three Age Cohorts. 2019. Available online: https://www.apa.org/depression-guideline (accessed on 29 October 2024).
- National Institute for Health and Care Excellence (NICE). Depression in Adults: Treatment and Management. NICE Guidelines. 2022. Available online: https://www.nice.org.uk/guidance/ng222 (accessed on 29 October 2024).
- United Nations. Sustainable Development Goals–The 17 Goals. Department of Economic and Social Affairs Sustainable Development. 2015. Available online: https://sdgs.un.org/goals (accessed on 29 October 2024).
| Arabic-Speaking | Swahili-Speaking | |||
|---|---|---|---|---|
| Focus Group Discussions n = 3 | Interviews | Focus Group Discussions n = 2 | Interviews | |
| Gender | ||||
| Male | 5 | 7 | 8 | 4 |
| Female | 13 | 3 | 4 | 4 |
| Age | ||||
| 18–30 | 3 | - | 9 | - |
| 30–39 | 4 | - | 2 | - |
| 40–49 | 7 | 2 | - | 4 |
| >50 | 4 | 8 | 1 | 4 |
| Years in Australia | ||||
| 1–2 | 3 | - | 4 | - |
| 3–4 | 11 | - | 3 | - |
| >5 | 4 | - | 5 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slewa-Younan, S.; Narchal, R.; Das, R.; Krstanoska-Blazeska, K.; Blignault, I.; Li, B.; Reavley, N.; Renzaho, A. Gender, Mental Health Stigma, and Help-Seeking in Arabic- and Swahili-Speaking Communities in Australia. Int. J. Environ. Res. Public Health 2024, 21, 1619. https://doi.org/10.3390/ijerph21121619
Slewa-Younan S, Narchal R, Das R, Krstanoska-Blazeska K, Blignault I, Li B, Reavley N, Renzaho A. Gender, Mental Health Stigma, and Help-Seeking in Arabic- and Swahili-Speaking Communities in Australia. International Journal of Environmental Research and Public Health. 2024; 21(12):1619. https://doi.org/10.3390/ijerph21121619
Chicago/Turabian StyleSlewa-Younan, Shameran, Renu Narchal, Ruth Das, Klimentina Krstanoska-Blazeska, Ilse Blignault, Bingqin Li, Nicola Reavley, and Andre Renzaho. 2024. "Gender, Mental Health Stigma, and Help-Seeking in Arabic- and Swahili-Speaking Communities in Australia" International Journal of Environmental Research and Public Health 21, no. 12: 1619. https://doi.org/10.3390/ijerph21121619
APA StyleSlewa-Younan, S., Narchal, R., Das, R., Krstanoska-Blazeska, K., Blignault, I., Li, B., Reavley, N., & Renzaho, A. (2024). Gender, Mental Health Stigma, and Help-Seeking in Arabic- and Swahili-Speaking Communities in Australia. International Journal of Environmental Research and Public Health, 21(12), 1619. https://doi.org/10.3390/ijerph21121619