
A Pilot and Feasibility Study on a Mindfulness-Based Intervention Adapted for LGBTQ+ Adolescents

 , , and
, , and
Abstract
1. Introduction
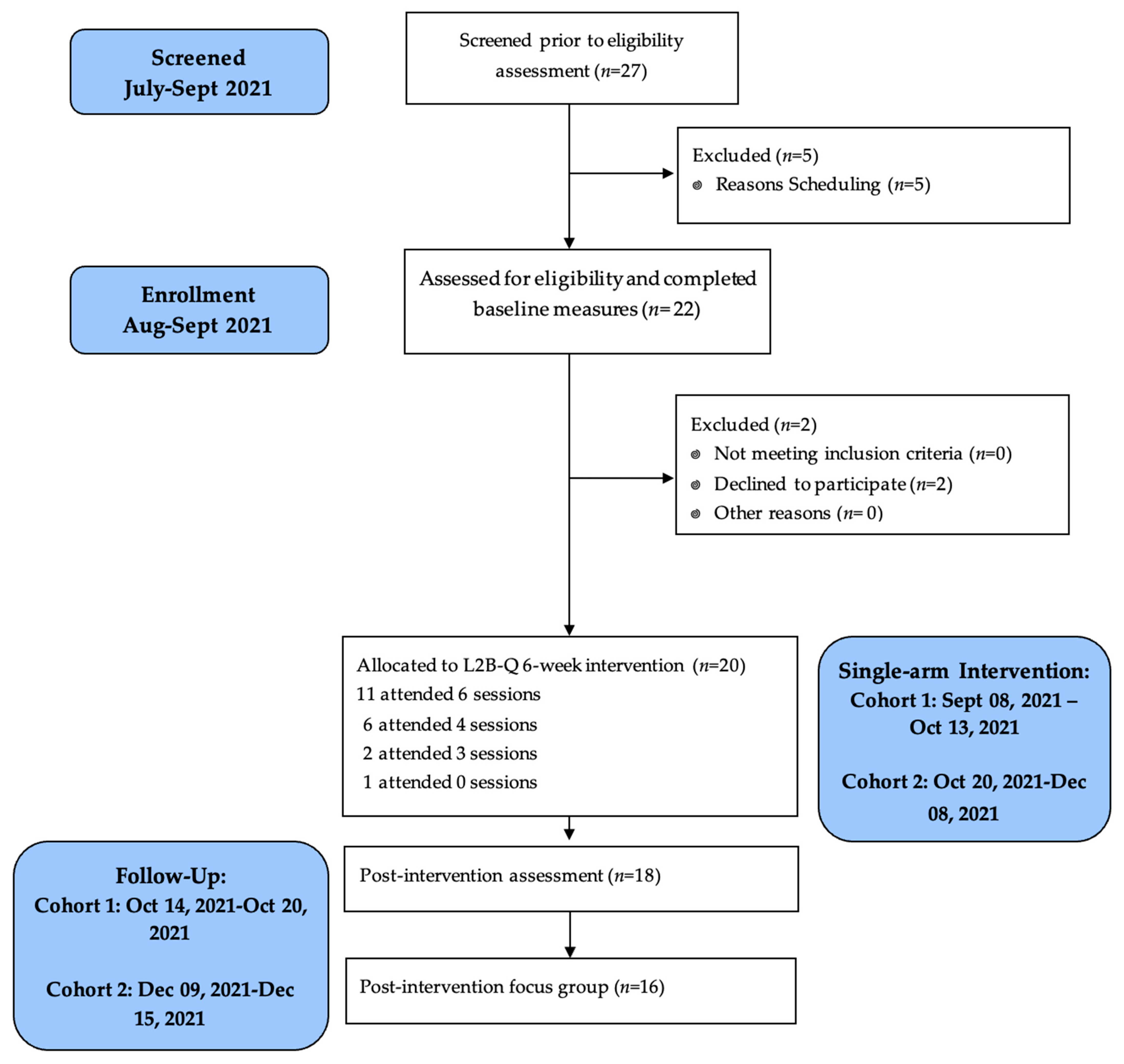
2. Materials and Methods
3. Results
3.1. Participant Descriptives
3.2. Primary Aim: Quantitative Indicators of Acceptability and Feasibility
3.3. Primary Aim: Qualitative Indicators of Acceptability and Feasibility
3.3.1. Acceptability
3.3.2. Implementation
3.3.3. Practicality
3.3.4. Demand
3.4. Safety and Tolerability
3.5. Baseline to Post-Intervention Changes in Outcomes
3.5.1. Mental Health: Anxiety and Depression Symptoms
3.5.2. Mindfulness
3.5.3. Stress-Related Health Behaviors: Eating, Sleep, Physical Activity
3.5.4. Physical Stress Experiences
3.5.5. LGBTQ+ Identity Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lothwell, L.E.; Libby, N.; Adelson, S.L. Mental Health Care for LGBT Youths. Focus 2020, 18, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Mongellii, F.; Perrone, D.; Balducci, J.; Sacchetti, A.; Ferrari, S.; Mattei, G.; Galeazzi, G.M. Minority Stress and Mental Health Among LGBT Populations: An Update on the Evidence. Minerva Psichiatr. 2019, 60, 27–50. [Google Scholar] [CrossRef]
- Green, A.E.; Taliaferro, L.A.; Price, M.N. Understanding Risk and Protective Factors to Improve the Well-Being and Prevent Suicide among LGBTQ Youth. In Handbook of Youth Suicide Prevention: Integrating Research into Practice; Miranda, R., Jeglic, E.L., Eds.; Springer Nature: Berlin, Germany, 2022; pp. 177–194. [Google Scholar]
- Compas, B.E.; Orosan, P.G.; Grant, K.E. Adolescent Stress and Coping: Implications for Psychopathology During Adolescence. J. Adolesc. 1993, 16, 331–349. [Google Scholar] [CrossRef] [PubMed]
- Lindholdt, L.; Labriola, M.; Andersen, J.H.; Kjeldsen, M.Z.; Obel, C.; Lund, T. Perceived Stress Among Adolescents as A Marker for Future Mental Disorders: A Prospective Cohort Study. Scand. J. Public. Health 2022, 50, 412–417. [Google Scholar] [CrossRef]
- Miller, R.L.; Moran, M.; Shomaker, L.B.; Seiter, N.; Sanchez, N.; Verros, M.; Rayburn, S.; Johnson, S.; Lucas-Thompson, R. Health Effects of COVID-19 For Vulnerable Adolescents in A Randomized Controlled Trial. Sch. Psychol. 2021, 36, 293–302. [Google Scholar] [CrossRef]
- Pascoe, M.; Bailey, A.P.; Craike, M.; Carter, T.; Patten, R.; Stepto, N.; Parker, A. Physical Activity and Exercise in Youth Mental Health Promotion: A Scoping Review. BMJ Open Sport. Exerc. Med. 2020, 6, e000677. [Google Scholar] [CrossRef]
- Walls, J.; Grose, R.G.; Farewell, C.; Quirk, K.; Puma, J.E.; Shomaker, L.; Brittain, D. A Qualitative Study of Stress and Coping among LGBTQ+ Colorado Youth. under review.
- Meyer, I.H. Minority Stress and Mental Health in Gay Men. J. Health Soc. Behav. 1995, 36, 38–56. [Google Scholar] [CrossRef]
- Meyer, I.H. Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef]
- Flentje, A.; Clark, K.D.; Cicero, E.; Capriotti, M.R.; Lubensky, M.E.; Sauceda, J.; Neilands, T.B.; Lunn, M.R.; Obedin-Maliver, J. Minority Stress, Structural Stigma, and Physical Health Among Sexual and Gender Minority Individuals: Examining the Relative Strength of the Relationships. Ann. Behav. Med. 2022, 56, 573–591. [Google Scholar] [CrossRef]
- Kosciw, J.G.; Clark, C.M.; Menard, L. The 2021 National School Climate Survey: The Experiences of LGBTQ+ Youth in Our Nation’s Schools; GLSEN: New York, NY, USA, 2022; p. xiv-167. [Google Scholar]
- Meyer, I.H.; Teylan, M.; Schwartz, S. The Role of Help-Seeking In Preventing Suicide Attempts Among Lesbians, Gay Men, and Bisexuals. Suicide Life Threat. Behav. 2015, 45, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Choukas-Bradley, S.; Thoma, B.C. Mental Health Among LGBT Youth. In Gender and Sexuality Development: Contemporary Theory and Research; Wong, W.I., VanderLaan, D., Eds.; Springer Publishing Company: New York, NY, USA, 2022; pp. 539–565. [Google Scholar]
- The Trevor Project: 2023, U.S. National Survey on The Mental Health of LGBTQ Young People. Available online: https://www.thetrevorproject.org/survey-2023/#suicide-by-gender (accessed on 23 September 2023).
- Goldbach, J.T.; Rhoades, H.; Mamey, M.R.; Senese, J.; Karys, P.; Marsiglia, F.F. Reducing Behavioral Health Symptoms by Addressing Minority Stressors in LGBTQ Adolescents: A Randomized Controlled Trial of Proud & Empowered. BMC Public Health 2021, 21, 2315. [Google Scholar]
- Toomey, R.B.; Syvertsen, A.K.; Shramko, M. Transgender Adolescent Suicide Behavior. Pediatrics 2018, 142, e20174218. [Google Scholar] [CrossRef] [PubMed]
- Green, A.E.; Price-Feeney, M.; Dorison, S.H. Association of Sexual Orientation Acceptance with Reduced Suicide Attempts Among Lesbian, Gay, Bisexual, Transgender, Queer, and Questioning Youth. LGBT Health 2021, 8, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.D. Obesity in Sexual and Gender Minority Populations: Prevalence and Correlates. Curr. Obes. Rep. 2023, 12, 175–182. [Google Scholar] [CrossRef]
- Caceres, B.A.; Brody, A.; Luscombe, R.E.; Primiano, J.E.; Marusca, P.; Sitts, E.M.; Chyun, D. A Systematic Review of Cardiovascular Disease in Sexual Minorities. Am. J. Public Health 2017, 107, e13–e21. [Google Scholar] [CrossRef]
- Fredriksen-Goldsen, K.I. Resilience and Disparities Among Lesbian, Gay, Bisexual, and Transgender Older Adults. Public Policy Aging Rep. 2011, 21, 3–7. [Google Scholar] [CrossRef]
- Fredriksen-Goldsen, K.I.; Romanelli, M.; Jung, H.H.; Kim, H.J. Health, Economic, and Social Disparities Among Lesbian, Gay, Bisexual, and Sexually Diverse Adults: Results from A Population-Based Study. Behav. Med. 2023, 50, 141–152. [Google Scholar] [CrossRef]
- Beach, L.B.; Elasy, T.A.; Gonzales, G. Prevalence of Self-Reported Diabetes by Sexual Orientation: Results from the 2014 Behavioral Risk Factor Surveillance System. LGBT Health 2018, 5, 121–130. [Google Scholar] [CrossRef]
- Grammer, A.C.; Byrne, M.E.; Pearlman, A.T.; Klein, D.A.; Schvey, N.A. Overweight and Obesity in Sexual and Gender Minority Adolescents: A Systematic Review. Obes. Rev. 2019, 20, 1350–1366. [Google Scholar] [CrossRef]
- Brown, C.; Porta, C.M.; Eisenberg, M.E.; McMorris, B.J.; Sieving, R.E. Family Relationships and the Health and Well-Being of Transgender and Gender-Diverse Youth: A Critical Review. LGBT Health 2020, 7, 407–419. [Google Scholar] [CrossRef] [PubMed]
- National Scientific Council on the Developing Child: Excessive Stress Disrupts the Architecture of the Developing Brain: Working Paper #3. Available online: https://developingchild.harvard.edu/wp-content/uploads/2005/05/Stress_Disrupts_Architecture_Developing_Brain-1.pdf (accessed on 23 September 2023).
- Garcia, J.; Vargas, N.; Clark, J.L.; Magaña Álvarez, M.; Nelons, D.A.; Parker, R.G. Social Isolation and Connectedness as Determinants of Well-Being: Global Evidence Mapping Focused on LGBTQ Youth. Glob. Public Health 2020, 15, 497–519. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.B.; Kelly, P.L. LGBT Health. In Health and Social Work: Practice, Policy, and Research; Heyman, J.C., Congress, E.P., Eds.; Springer Publishing Company: New York, NY, USA, 2018; Volume 1, pp. 269–286. [Google Scholar]
- Calzo, J.P.; Turner, B.C.; Marro, R.; Phillips, G.L. Alcohol Use and Disordered Eating in a US Sample of Heterosexual and Sexual Minority Adolescents. J. Am. Acad. Child. Adolesc. Psychiatry 2019, 58, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Pham, A.H.; Eadeh, H.M.; Garrison, M.M.; Ahrens, K.R. A Longitudinal Study on Disordered Eating in Transgender and Nonbinary Adolescents. Acad. Pediatr. 2023, 23, 1247–1251. [Google Scholar] [CrossRef]
- Parker, L.L.; Harriger, J.A. Eating Disorders and Disordered Eating Behaviors in the LGBT Population: A Review of the Literature. J. Eat. Disord. 2020, 8, 51. [Google Scholar] [CrossRef]
- Hysing, M.; Askeland, K.G.; La Greca, A.M.; Solberg, M.E.; Breivik, K.; Sivertsen, B. Bullying involvement in adolescence: Implications for sleep, mental health, and academic outcomes. J. Interpers. Violence 2021, 36, NP8992–NP9014. [Google Scholar] [CrossRef]
- Butler, E.S.; McGlinchey, E.; Juster, R.P. Sexual and Gender Minority Sleep: A Narrative Review and Suggestions for Future Research. J. Sleep. Res. 2020, 29, e12928. [Google Scholar] [CrossRef]
- Buysse, D.J. Sleep Health: Can We Define It? Does It Matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef]
- Riemann, D.; Krone, L.B.; Wulff, K.; Nissen, C. Sleep, Insomnia, and Depression. Neuropsychopharmacology 2020, 45, 74–89. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, X.; Liu, Z.Z.; Tein, J.Y.; Jia, C.X. Life Stress, Insomnia, and Anxiety/Depressive Symptoms in Adolescents: A Three-Wave Longitudinal Study. J. Affect. Disord. 2023, 322, 91–98. [Google Scholar] [CrossRef]
- Lewis-Smith, H.; Bray, I.; Salmon, D.; Slater, A. Prospective Pathways to Depressive Symptoms and Disordered Eating in Adolescence: A 7-Year Longitudinal Cohort Study. J. Youth Adolesc. 2020, 49, 2060–2074. [Google Scholar] [CrossRef] [PubMed]
- Morrissey, B.; Taveras, E.; Allender, S.; Strugnell, C. Sleep and Obesity Among Children: A Systematic Review of Multiple Sleep Dimensions. Pediatr. Obes. 2020, 15, e12619. [Google Scholar] [CrossRef] [PubMed]
- Marino, F.; Failla, C.; Carrozza, C.; Ciminata, M.; Chilà; P.; Minutoli, R.; Pioggia, G. Mindfulness-Based Interventions for Physical and Psychological Wellbeing in Cardiovascular Diseases: A Systematic Review and Meta-Analysis. Brain Sci. 2021, 11, 727. [Google Scholar] [CrossRef] [PubMed]
- Shankland, R.; Tessier, D.; Strub, L.; Gauchet, A.; Baeyens, C. Improving Mental Health and Well-Being Through Informal Mindfulness Practices: An Intervention Study. Appl. Psychol. Health Well-Being 2021, 13, 63–83. [Google Scholar] [CrossRef] [PubMed]
- Lassander, M.; Hintsanen, M.; Suominen, S.; Mullola, S.; Vahlberg, T.; Volanen, S.M. Effects of School-Based Mindfulness Intervention on Health-Related Quality of Life: Moderating Effect of Gender, Grade, and Independent Practice in Cluster Randomized Controlled Trial. Qual. Life Res. 2021, 30, 3407–3419. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Raab, C.; Stoffel, M.; Hernández, C.; Rahn, S.; Moessner, M.; Steinhilber, B.; Ditzen, B. Effects of A Mindfulness-Based Intervention on Mindfulness, Stress, Salivary Alpha-Amylase and Cortisol in Everyday Life. Psychophysiology 2021, 58, e13937. [Google Scholar] [CrossRef]
- Ahmad, F.; El Morr, C.; Ritvo, P.; Othman, N.; Moineddin, R.; MVC Team. An Eight-Week, Web-Based Mindfulness Virtual Community Intervention for Students’ Mental Health: Randomized Controlled Trial. JMIR Ment. Health 2020, 7, e15520. [Google Scholar] [CrossRef]
- Galante, J.; Friedrich, C.; Dawson, A.F.; Modrego-Alarcón, M.; Gebbing, P.; Delgado-Suárez, I.; Jones, P.B. Mindfulness-based programmes for mental health promotion in adults in nonclinical settings: A systematic review and meta-analysis of randomised controlled trials. PLoS Med. 2021, 18, e1003481. [Google Scholar] [CrossRef]
- Villalba, D.K.; Lindsay, E.K.; Marsland, A.L.; Greco, C.M.; Young, S.; Brown, K.W.; Smyth, J.M.; Walsh, C.P.; Gray, K.; Chin, B.; et al. D. Mindfulness Training and Systemic Low-Grade Inflammation in Stressed Community Adults: Evidence from Two Randomized Controlled Trials. PLoS ONE 2019, 14, e0219120. [Google Scholar] [CrossRef]
- Broderick, P.C. Learning to Breathe: A Mindfulness Curriculum for Adolescents to Cultivate Emotion Regulation, Attention, and Performance, 1st ed.; New Harbinger: Oakland, CA, USA, 2013. [Google Scholar]
- Broderick, P.C. Learning to Breathe: A Mindfulness Curriculum for Adolescents to Cultivate Emotion Regulation, Attention, and Performance, 2nd ed.; New Harbinger: Oakland, CA, USA, 2021. [Google Scholar]
- Broderick, P.C.; Metz, S.M. Learning to BREATHE: A Pilot Trial of a Mindfulness Curriculum for Adolescents. Adv. Sch. Ment. Health Promot. 2009, 2, 35–46. [Google Scholar] [CrossRef]
- Broderick, P.C.; Jennings, P.A. Mindfulness For Adolescents: A Promising Approach to Supporting Emotion Regulation and Preventing Risky Behavior. New Dir. Youth Dev. 2012, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Bluth, K.; Campo, R.A.; Pruteanu-Malinici, S.; Reams, A.; Mullarkey, M.; Broderick, P.C. A School-Based Mindfulness Pilot Study for Ethnically Diverse At-Risk Adolescents. Mindfulness 2016, 7, 90–104. [Google Scholar] [CrossRef] [PubMed]
- Broderick, P.C.; Frank, J.L. Learning to BREATHE: An Intervention to Foster Mindfulness in Adolescence. New Dir. Youth Dev. 2014, 2014, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Dvořáková, K.; Kishida, M.; Li, J.; Elavsky, S.; Broderick, P.C.; Agrusti, M.R.; Greenberg, M.T. Promoting Healthy Transition to College Through Mindfulness Training with First-Year College Students: Pilot Randomized Controlled Trial. J. Am. Coll. Health 2017, 6, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Eva, A.L.; Thayer, N.M. Learning to BREATHE: A Pilot Study of A Mindfulness-Based Intervention to Support Marginalized Youth. J. Evid. Based Complement. Altern. Med. 2017, 22, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Felver, J.C.; Clawson, A.J.; Morton, M.L.; Brier-Kennedy, E.; Janack, P.; DiFlorio, R.A. School-Based Mindfulness Intervention Supports Adolescent Resiliency: A Randomized Controlled Pilot Study. Int. J. Sch. Educ. Psychol. 2018, 7, 111–122. [Google Scholar] [CrossRef]
- Metz, S.M.; Frank, J.L.; Reibel, D.; Cantrell, T.; Sanders, R.; Broderick, P.C. The Effectiveness of the Learning to BREATHE Program on Adolescent Emotion Regulation. Res. Hum. Dev. 2013, 10, 252–272. [Google Scholar] [CrossRef]
- Gonzales, N.A. Expanding the Cultural Adaptation Framework for Population-Level Impact. Prev. Sci. 2017, 18, 689–693. [Google Scholar] [CrossRef]
- Iacono, G. Tuned In! An Affirmative Mindfulness Intervention for Sexual and Gender Diverse Young People. J. LGBT Youth 2024, 1, 1–26. [Google Scholar] [CrossRef]
- Quirk, K.; Klimo, K.D.; Jensen, S.; Grose, R.G.; Farewell, C.; Puma, J.E.; Brittain, D.; Shomaker, L. Iterative Culturally-Attuned Intervention Adaptation: Example from a LGBTQ+ Mindfulness Pilot Study. in preparation.
- Evans, S.R. Clinical Trial Structures. J. Exp. Stroke Transl. Med. 2010, 3, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Dawson, A.F.; Brown, W.W.; Anderson, J.; Datta, B.; Donald, J.N.; Hong, K.; Allan, S.; Mole, T.B.; Jones, P.B.; Galante, J. Mindfulness-Based Interventions for University Students: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Appl. Psychol. Health Well Being 2020, 12, 384–410. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Zhang, Y.; Cui, Z. Mindfulness-Based Interventions for Prevention of Depressive Symptoms in University Students: A Meta-Analytic Review. Mindfulness 2019, 10, 2209–2224. [Google Scholar] [CrossRef]
- Health Resources and Service Administration: Defining Rural Population. Available online: https://www.hrsa.gov/rural-health/about-us/what-is-rural#:~:text=The%20Census%20does%20not%20define,UCs)%20of%202%2C500%20%2D%2049%2C999%20people (accessed on 1 October 2024).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Mehodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inf. 2009, 4, 377–381. [Google Scholar] [CrossRef]
- Smith, A.U.; Schwartz, S.J. Waivers of Parental Consent for Sexual Minority Youth. Acc. Res. 2019, 26, 379–390. [Google Scholar] [CrossRef]
- Williams, N. The GAD-7 Questionnaire. Occup. Med. 2014, 64, 224. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of A Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Wu, Y.; Levis, B.; Riehm, K.E.; Saadat, N.; Levis, A.W.; Azar, M.; Thombs, B.D. Equivalency of the Diagnostic Accuracy of the PHQ-8 and PHQ-9: A Systematic Review and Individual Participant Data Meta-Analysis—ERRATUM. Psychol. Med. 2020, 50, 2816. [Google Scholar] [CrossRef]
- Dockendorff, S.A.; Petrie, T.A.; Greenleaf, C.A.; Martin, S. Intuitive Eating Scale: An Examination Among Early Adolescents. J. Couns. Psychol. 2012, 59, 604–611. [Google Scholar] [CrossRef]
- Tylka, T.L. Development and Psychometric Evaluation of a Measure of Intuitive Eating. J. Couns. Psychol. 2006, 53, 226–240. [Google Scholar] [CrossRef]
- Forrest, C.B.; Zorc, J.J.; Moon, J.; Pratiwadi, R.; Becker, B.D.; Maltenfort, M.G.; Guevara, J.P. Evaluation of the PROMIS Pediatric Global Health Scale (PGH-7) in Children with Asthma. J. Asthma 2019, 56, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Colorado Department of Public Health and the Environment Healthy Kids Colorado Survey. Available online: https://cdphe.colorado.gov/hkcs (accessed on 15 January 2021).
- Bevans, K.B.; Gardner, W.; Pajer, K.; Riley, A.W.; Forrest, C.B. Qualitative Development of the PROMIS(R) Pediatric Stress Response Item Banks. J. Pediatr. Psychol. 2013, 38, 173–191. [Google Scholar] [CrossRef] [PubMed]
- Bevans, K.B.; Gardner, W.; Pajer, K.A.; Becker, B.; Carle, A.; Tucker, C.A.; Forrest, C.B. Psychometric Evaluation of the PROMIS® Pediatric Psychological and Physical Stress Experiences Measures. J. Pediatr. Psychol. 2018, 43, 678–692. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.W.; West, A.M.; Loverich, T.M.; Biegel, G.M. Assessing Adolescent Mindfulness: Validation of an Adapted Mindful Attention Awareness Scale in Adolescent Normative and Psychiatric Populations. Psychol. Assess. 2011, 23, 1023–1033. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, M.A.; Petras, H.; Chen, D.; Chodzen, G. The Gender Minority Stress and Resilience Measure: Psychometric Validity of an Adolescent Extension. Clin. Pract. Pediatr. Psychol. 2019, 7, 278–290. [Google Scholar] [CrossRef]
- Riggle, E.D.; Mohr, J.J.; Rostosky, S.S.; Fingergut, A.W.; Balsam, K.F. A Multi-Factor Gay, Lesbian, and Bisexual Positive Identity Measure (LGB-PIM). Psychol. Sex. Orientat. Gend. Divers. 2014, 1, 398–411. [Google Scholar] [CrossRef]
- Bowen, D.J.; Kreuter, M.; Spring, B.; Cofta-Woerpel, L.; Linnan, L.; Weiner, D.; Bakken, S.; Kaplan, C.P.; Squiers, L.; Fabrizio, C.; et al. How We Design Feasibility Studies. Am. J. Prev. Med. 2009, 36, 452–457. [Google Scholar] [CrossRef]
- Vindrola-Padros, C.; Johnson, G.A. Rapid Techniques in Qualitative Research: A Critical Review of the Literature. Qual. Health Res. 2020, 30, 1596–1604. [Google Scholar] [CrossRef]
- Cumming, G. Understanding the New Statistics: Effect Sizes, Confidence Intervals, and Meta-Analysis; Routledge Taylor & Francis Group: New York, NY, USA, 2013. [Google Scholar]
- Eich, E. Business Not as Usual. Psychol. Sci. 2014, 25, 3–6. [Google Scholar] [CrossRef]
- Kouros, C.D.; Papp, L.M.; Goeke-Morey, M.C.; Cummings, E.M. Spillover Between Marital Quality and Parent-Child Relationship Quality: Parental Depressive Symptoms as Moderators. J. Fam. Psychol. 2014, 28, 315–325. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Kirby, T.A.; Barreto, M.; Korine, R.; Hendy, J.; Osman, L.; Stadie, S.; Tan, D. To Conceal or Reveal: Identity-Conscious Diversity Ideologies Facilitate Sexual Minority Identity Disclosure. Eur. J. Soc. Psychol. 2024, 54, 199–218. [Google Scholar] [CrossRef]
- McKay, T.R.; Watson, R.J. Gender Expansive Youth Disclosure and Mental Health: Clinical Implications of Gender Identity Disclosure. Psychol. Sex. Orientat. Gend. Divers. 2020, 7, 66–75. [Google Scholar] [CrossRef] [PubMed]
- McGregor, K.; Williams, C.R.; Botta, A.; Mandel, F.; Gentile, J. Providing Essential Gender-Affirming Telehealth Services to Transgender Youth During COVID-19: A Service Review. J. Telemed. Telecare 2023, 29, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Fulambarkar, N.; Seo, B.; Testerman, A.; Rees, M.; Bausback, K.; Bunge, E. Review: Meta-Analysis on Mindfulness-Based Interventions for Adolescents’ Stress, Depression, and Anxiety in School Settings: A Cautionary Tale. Child. Adolesc. Ment. Health 2023, 28, 307–317. [Google Scholar] [CrossRef]
- Creswell, J.D.; Lindsay, E.K. How Does Mindfulness Training Effect Health? A Mindfulness Stress Buffering Account. Curr. Dir. Psychol. Sci. 2014, 23, 401–407. [Google Scholar] [CrossRef]
- Bernstein, R.; Sanchez, N.; Clark, E.L.M.; Conte, I.; Gulley, L.D.; Legget, K.T.; Cornier, M.A.; Melby, C.; Johnson, S.A.; Lucas-Thompson, R.; et al. Mindfulness-Based Intervention in Adolescents At Risk for Excess Weight Gain: 1.5-Year Follow-Up of Pilot Randomized Controlled Trial. Eat. Behav. 2021, 43, 101580. [Google Scholar] [CrossRef]
- Dunn, C.; Haubenreiser, J.; Johnson, M.; Nordby, K.; Aggarwal, S.; Myer, S.; Thomas, C. Mindfulness Approaches Weight Loss, Weight Maintenance, and Weight Regain. Curr. Obes. Rep. 2018, 7, 37–49. [Google Scholar] [CrossRef]
- Grohmann, D.; Laws, K.R. Two Decades of Mindfulness-Based Interventions for Binge Eating: A Systematic Review and Meta-Analysis. J. Psychosom. Res. 2021, 149, 110592. [Google Scholar] [CrossRef]
- Rogers, J.M.; Ferrari, M.; Mosely, K.; Lang, C.P.; Brennan, L. Mindfulness-Based Interventions for Adults Who are Overweight or Obese: A Meta-Analysis of Physical and Psychological Health Outcomes. Obes. Rev. 2017, 18, 51–67. [Google Scholar] [CrossRef]
- Shomaker, L.B.; Berman, Z.; Burke, M.; Annameier, S.K.; Pivarunas, B.; Sanchez, N.; Smith, A.D.; Hendrich, S.; Riggs, N.R.; Legget, K.T.; et al. Mindfulness-Based Group Intervention in Adolescents At-Risk for Excess Weight Gain: A Randomized Controlled Pilot Study. Appetite 2019, 140, 213–222. [Google Scholar] [CrossRef]
- Goffnet, J.; Leichty, J.M.; Kidder, E. Interventions to Reduce Shame: A Systematic Review. J. Behav. Cogn. Ther. 2020, 30, 141–160. [Google Scholar] [CrossRef]
- Fosse, N.E.; Haas, S.A. Validity and Stability of Self-Reported Health Among Adolescents in A Longitudinal, Nationally Representative Survey. Pediatrics 2009, 123, e496–e501. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Identity | Number (Total N = 20) | Percentage (%) |
|---|---|---|
| Gender | ||
| Female/Woman | 7 | 35 |
| Male/Man | 9 | 45 |
| Non-Binary | 3 | 15 |
| Transgender | 1 | 5 |
| Sexual Orientation | ||
| Lesbian | 7 | 35 |
| Gay | 8 | 40 |
| Bisexual | 3 | 15 |
| Asexual | 1 | 5 |
| Demisexual | 1 | 5 |
| Race | ||
| Black | 12 | 6 |
| Asian | 1 | 5 |
| Native Hawaiian | 1 | 5 |
| White | 6 | 3 |
| Ethnicity | ||
| Hispanic | 5 | 2 |
| Non-Hispanic | 14 | 7 |
| No Response | 1 | 5 |
| Age | ||
| 14 | 1 | 5 |
| 16 | 9 | 45 |
| 17 | 7 | 35 |
| 18 | 3 | 15 |
| Themes | Sub-Themes | Example Responses: |
|---|---|---|
| Acceptability | Facilitator Characteristics | “Looking forward to meeting every week thanks to the moderators we had”. |
| “It was all good and the moderators were the best”. | ||
| Platform | “Discord for sure”. | |
| “Discord is perfect” | ||
| Mindful Practice | “These [activities] helped a lot always looking forward”. | |
| “Gratitude practice helps you be more thankful and it was a boost to my self- esteem”. | ||
| Camera Usage | “Trying to stay anonymous” | |
| “I’m an introvert I don’t like being seen”. | ||
| Implementation | Activity Changes | “Some visuals would be nice” |
| “Maybe some written instructions”. | ||
| Participant Engagement | “Good contents and activities will always bring anyone back. It’ll keep us coming for more”. | |
| “Sometimes I get carried away by other stuff like a date night or friends’ night out”. | ||
| Group Connection | “[The groups were] too small and sometimes we lacked proper communication”. | |
| “More introductions and maybe got to know each other a bit more I would be more willing to show my face”. | ||
| Practicality | Timing | “The time is a little late”. |
| “I want to stay longer”. | ||
| Demand | Peer Recruitment | “[I will] play by my friends”. |
| “[My friend] moved out of Colorado, she would have loved to join”. |
| Variable | Baseline | Post-Intervention | Mdiff | Cohen’s d | 95% CI | ||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| Depression | 8.67 | 7.24 | 5.11 | 4.89 | −3.56 | −0.82 | (−1.34, −0.27) |
| Anxiety | 7.59 | 5.30 | 4.82 | 5.98 | −2.76 | −0.65 | (−1.17, −0.12) |
| Mindfulness | 3.40 | 1.20 | 3.78 | 1.31 | 0.38 | 0.23 | (−0.25, 0.71) |
| Sleep Disturbance | 10.59 | 2.06 | 9.53 | 3.56 | −1.06 | −0.33 | (−0.81, 0.17) |
| Non-Intuitive Eating | 16.39 | 5.71 | 13.33 | 4.93 | −3.06 | −0.47 | (−0.03, 0.95) |
| Physical Activity | 4.56 | 1.79 | 5.17 | 1.69 | 0.61 | 0.56 | (0.05, 1.05) |
| Physical Stress | 19.39 | 6.07 | 17.61 | 6.03 | −1.78 | −0.35 | (−0.82, 0.14) |
| Internalized Shame | 18.18 | 6.70 | 19.00 | 8.46 | 0.82 | 0.11 | (−0.37, 0.58) |
| Community Connectedness | 18.33 | 3.03 | 19.44 | 2.77 | 1.11 | 0.36 | (−0.12, 0.83) |
| Positive Identity: Self-Awareness | 19.00 | 5.20 | 21.72 | 3.46 | 2.72 | 0.53 | (0.03, 1.02) |
| Positive Identity: Authenticity | 19.76 | 4.80 | 20.71 | 3.12 | 0.95 | 0.17 | (−0.31, 0.65) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klimo, K.D.; Wilson, J.W.; Farewell, C.; Grose, R.G.; Puma, J.E.; Brittain, D.; Shomaker, L.B.; Quirk, K. A Pilot and Feasibility Study on a Mindfulness-Based Intervention Adapted for LGBTQ+ Adolescents. Int. J. Environ. Res. Public Health 2024, 21, 1364. https://doi.org/10.3390/ijerph21101364
Klimo KD, Wilson JW, Farewell C, Grose RG, Puma JE, Brittain D, Shomaker LB, Quirk K. A Pilot and Feasibility Study on a Mindfulness-Based Intervention Adapted for LGBTQ+ Adolescents. International Journal of Environmental Research and Public Health. 2024; 21(10):1364. https://doi.org/10.3390/ijerph21101364
Chicago/Turabian StyleKlimo, Kasey D., Jessica Walls Wilson, Charlotte Farewell, Rose Grace Grose, Jini E. Puma, Danielle Brittain, Lauren B. Shomaker, and Kelley Quirk. 2024. "A Pilot and Feasibility Study on a Mindfulness-Based Intervention Adapted for LGBTQ+ Adolescents" International Journal of Environmental Research and Public Health 21, no. 10: 1364. https://doi.org/10.3390/ijerph21101364
APA StyleKlimo, K. D., Wilson, J. W., Farewell, C., Grose, R. G., Puma, J. E., Brittain, D., Shomaker, L. B., & Quirk, K. (2024). A Pilot and Feasibility Study on a Mindfulness-Based Intervention Adapted for LGBTQ+ Adolescents. International Journal of Environmental Research and Public Health, 21(10), 1364. https://doi.org/10.3390/ijerph21101364