
Nature-Based Interventions Targeting Elderly People’s Health and Well-Being: An Evidence Map

 , , ,
, , ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Coding and Critical Evaluation
2.7. Evidence Map
3. Results
3.1. Characterization of the Platform Used to Analyze the Literature Search
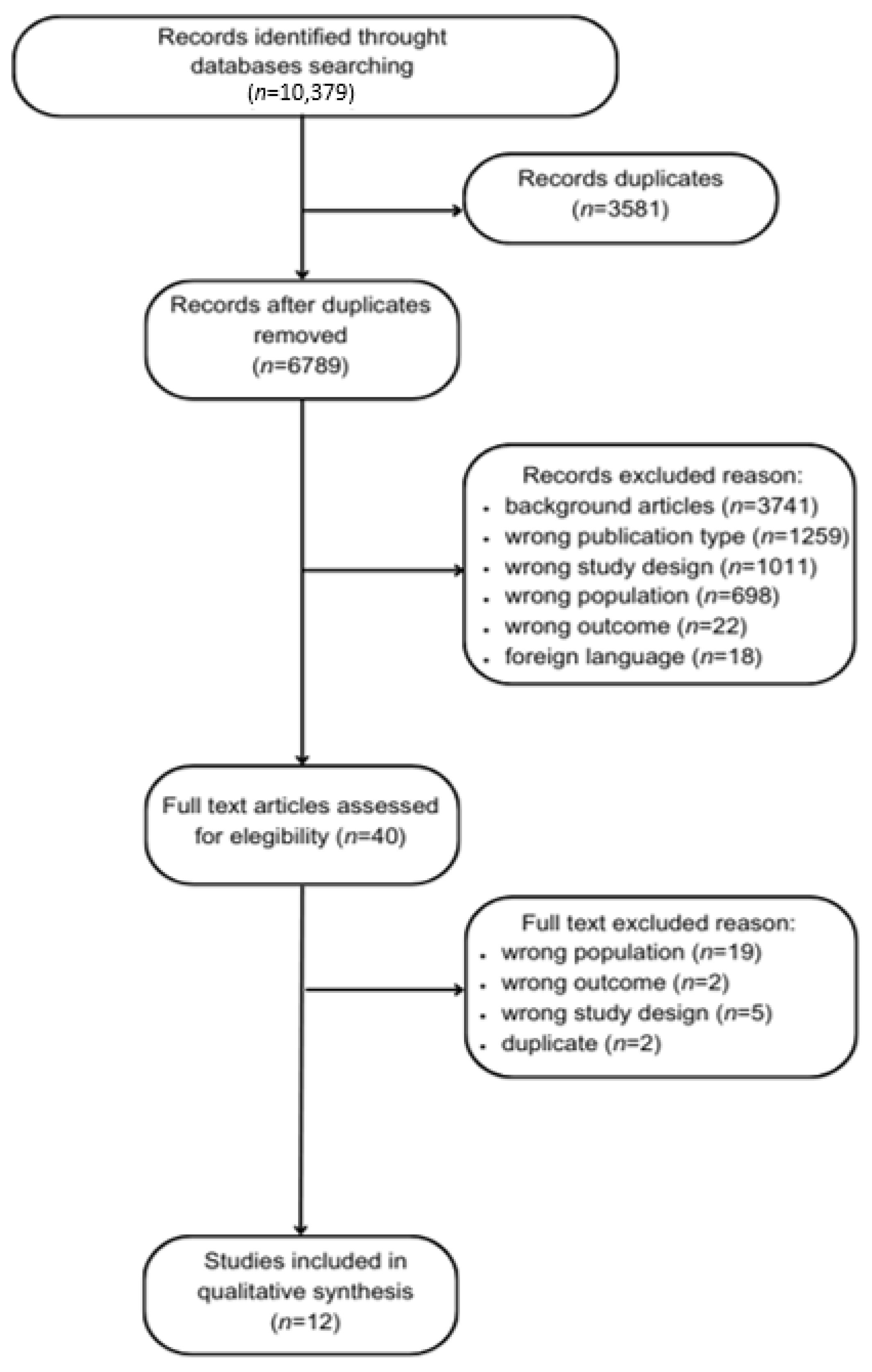
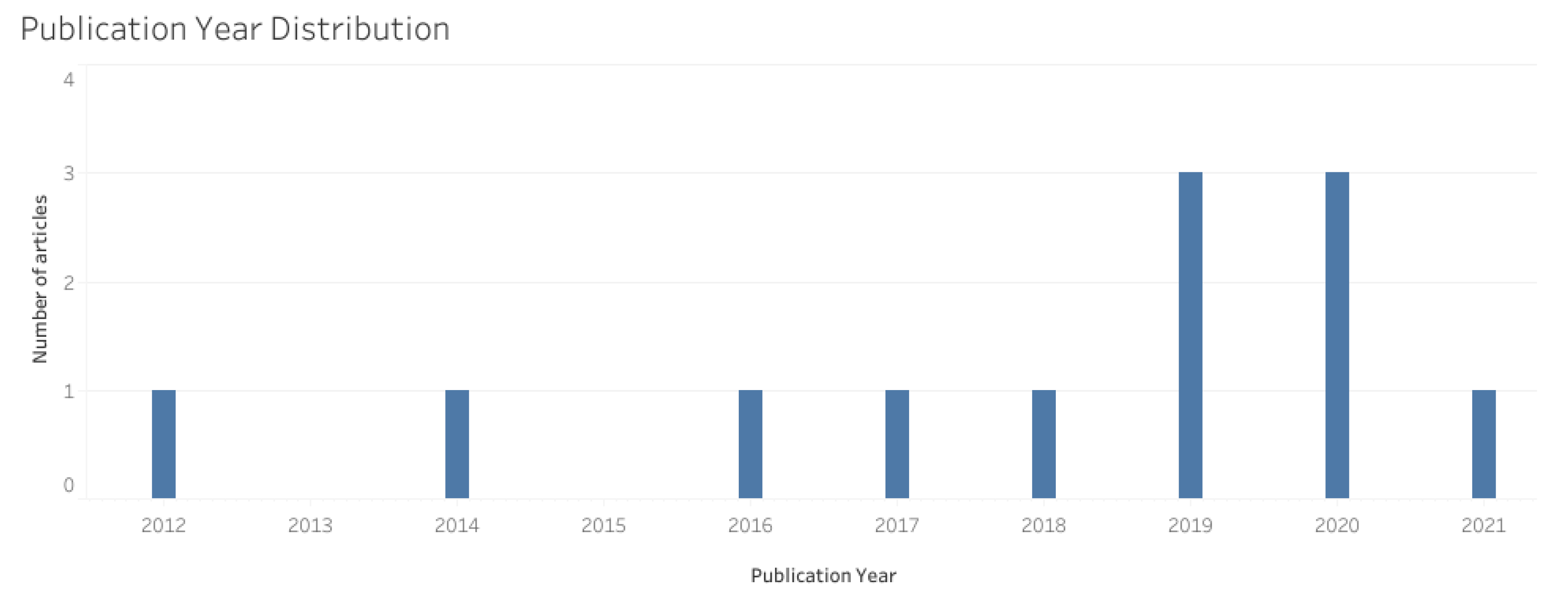
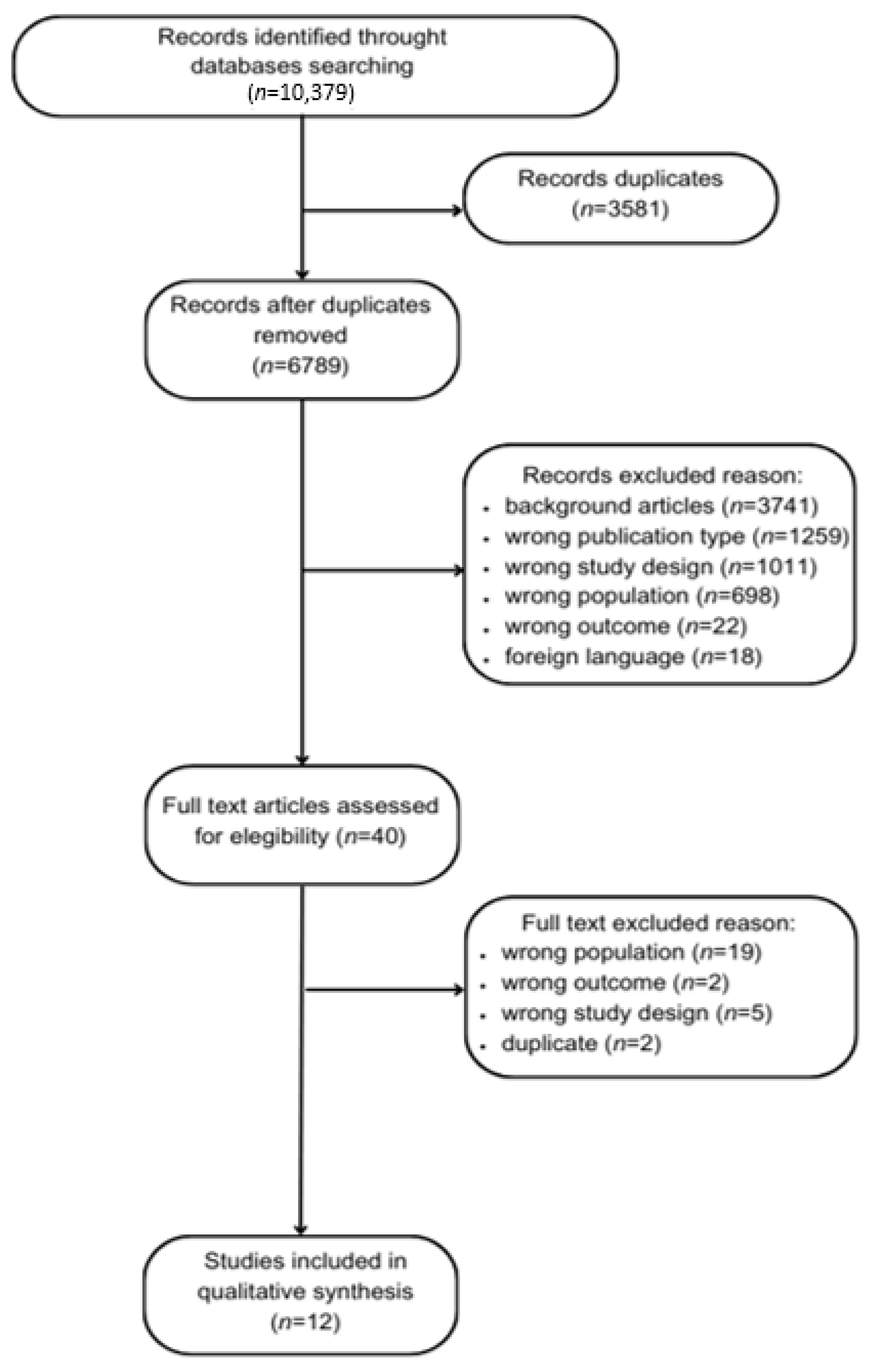
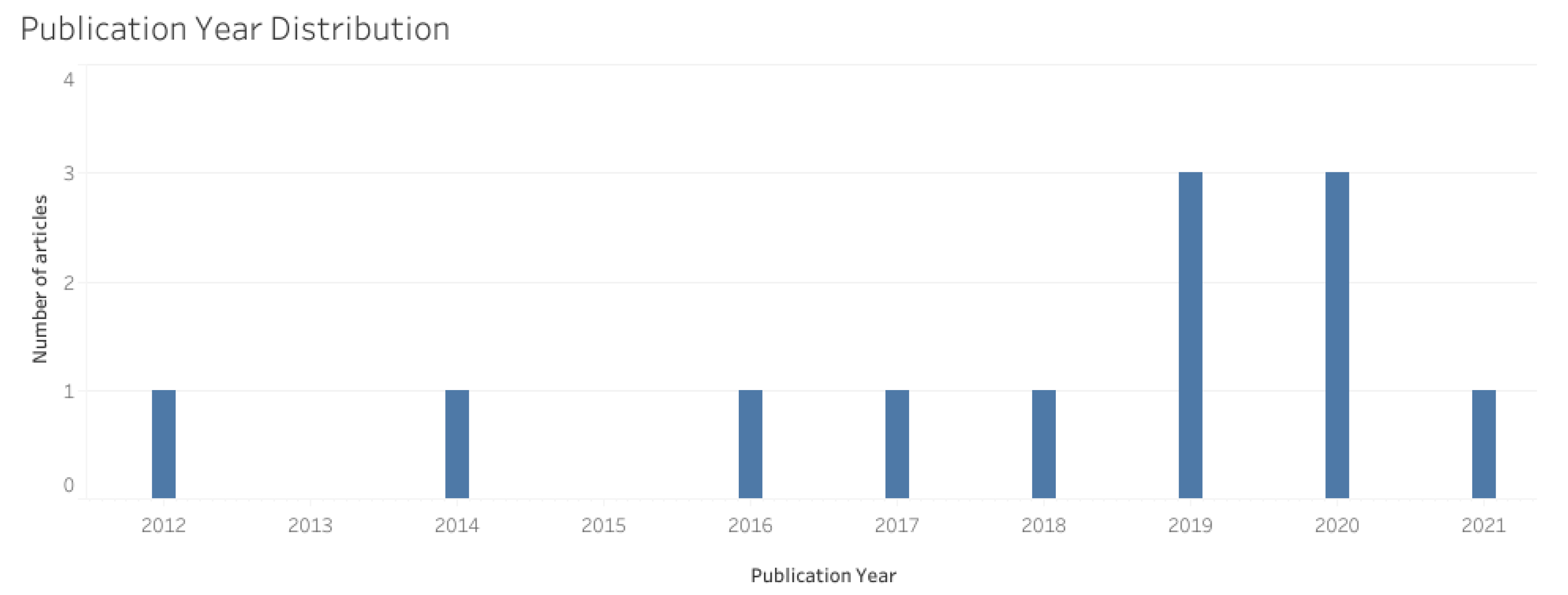
3.2. Selected Studies
3.3. Characteristics of the Studies
3.3.1. Population
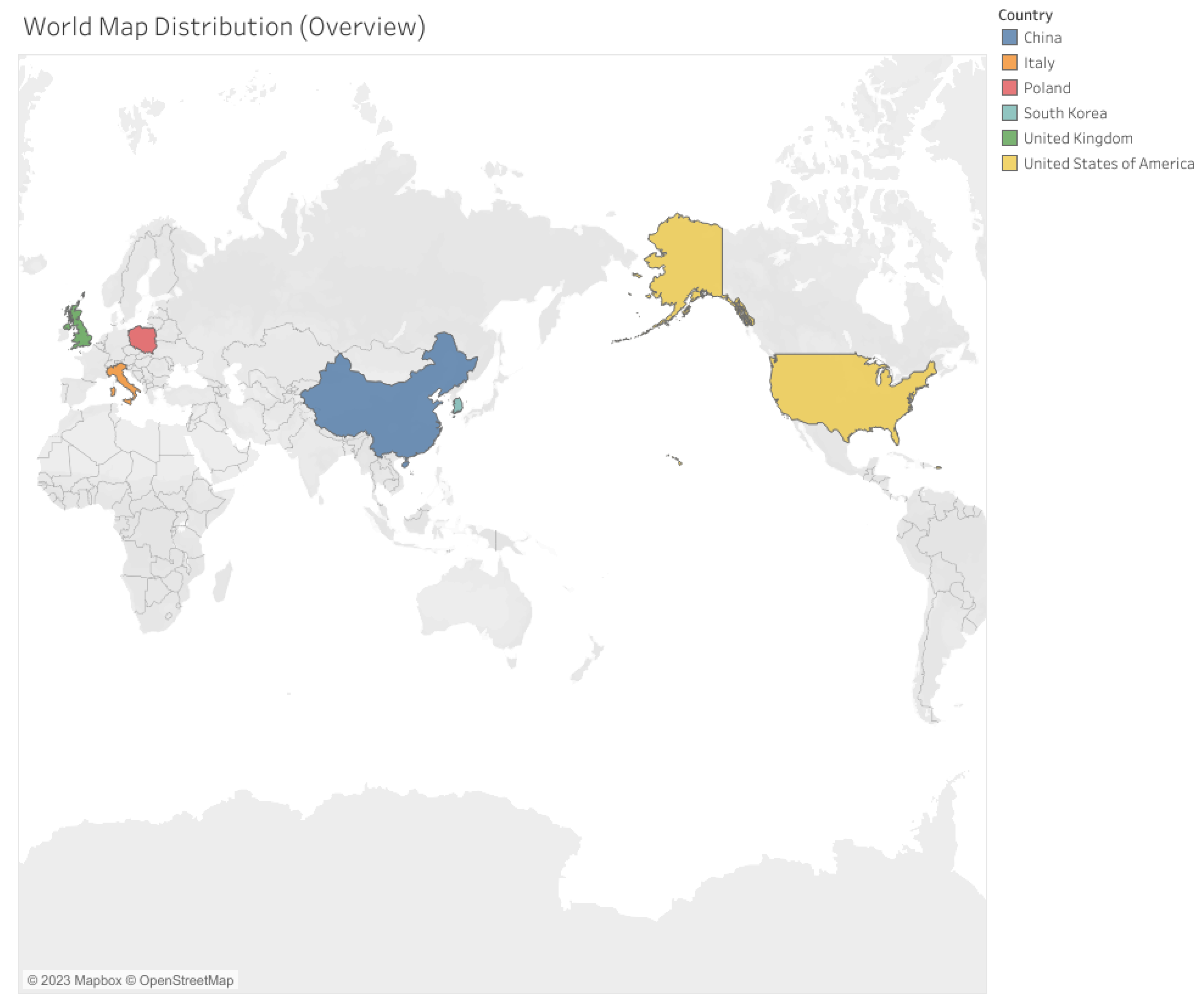
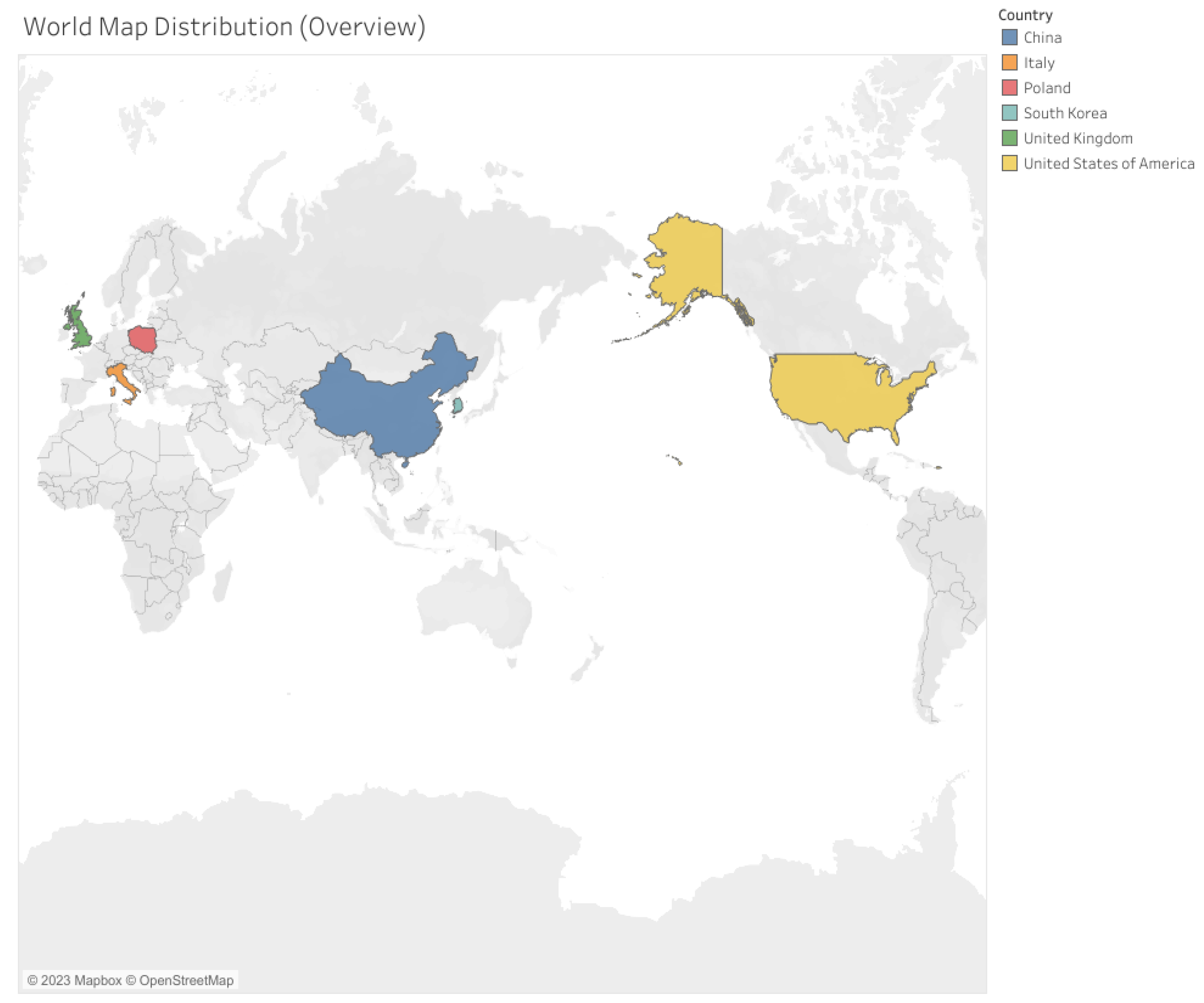
3.3.2. Countries of the Studies
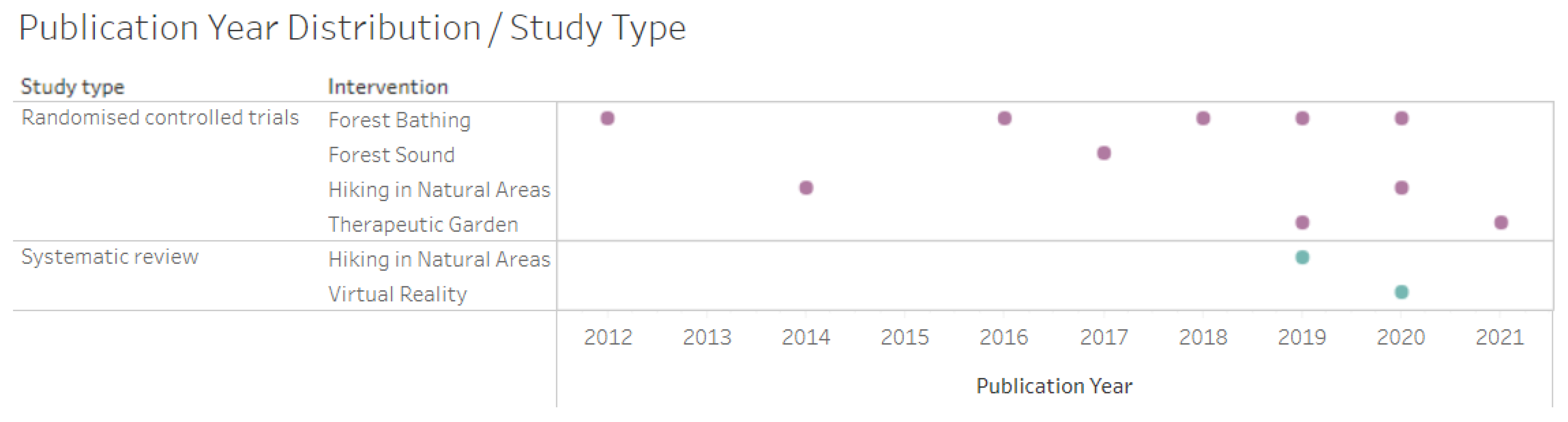
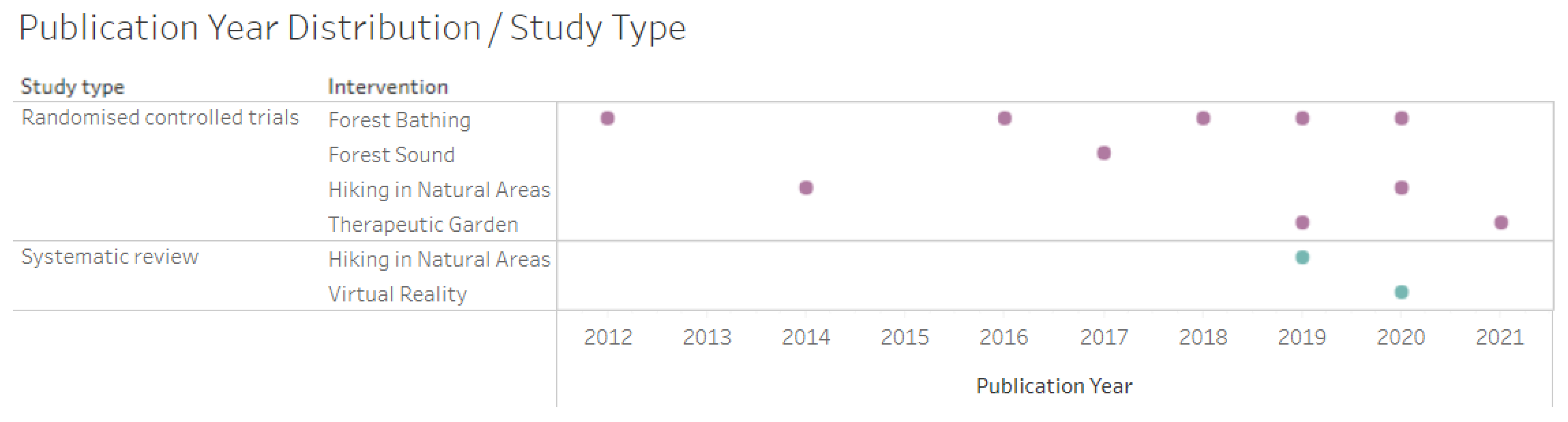
3.3.3. Study Design and Quality
3.3.4. Interventions Carried out per Study
3.3.5. Outcomes and Effects of Study
3.3.6. Evidence Map
- Physical Aspects: Cardiovascular and Pulmonary: covered by the outcomes of blood pressure reduction; heart rate reduction; heart variation reduction; vasoconstriction reduction; decreased levels of brain natriuretic peptide (BNP); improved levels of cardiovascular bioindicators (endothelin I, renin, angiotensin; Angiotensin II, angiotensin II receptor I and II); and improved lung function.
- Physical Aspects: Neuro-immuno-endocrinological: covered by the outcomes of decreased inflammatory response; salivary cortisol reduction; decreased levels of granzyme B and perforin; reduction in oxidative stress; healing improvement; bioimpedance improvement; reduction in agitation and mental confusion; reduction in cognitive decline; improved sleep pattern; improvement in neuropsychiatric indicators; and improved autonomy for activities of daily life.
- Mental/Behavioral Aspects: covered by the outcomes of depression reduction; anxiety reduction; stress reduction; tension reduction; improvement in negative emotions; increased feeling of happiness; improved quality of life; increased feeling of pleasure; increased sense of well-being; reduced feeling of fatigue; improved empathy levels.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dardengo, C.F.R.; Mafra, S.C.T. Os conceitos de velhice e envelhecimento ao longo do tempo: Contradição ou adaptação? Rev. Ciências Humanas 2019, 18, S1. [Google Scholar]
- Eurostat. Ageing Europe—2021 Interactive Edition. Available online: https://ec.europa.eu/eurostat/en/web/products-interactive-publications/-/ks-08-21-259 (accessed on 17 March 2022).
- Instituto Nacional de Estatística (INE). Estatística Demográfica. 2020. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_publicacoes&PUBLICACOESpub_boui=442993507&PUBLICACOESmodo=2 (accessed on 17 March 2022).
- Ministério da Saúde. Plano Nacional de Saúde 2021–2030. Saúde Sustentável: De tod@s Para Tod@s. 2022. Available online: https://www.sns.gov.pt/noticias/2022/04/08/plano-nacional-de-saude-2021-2030-2/ (accessed on 10 August 2022).
- Crelier, C. Expectativa de Vida Dos Brasileiros Aumenta Para 76, 3 Anos em 2018. Agência Instituto Brasileiro de Geografia e Estatística Notícias. Available online: https://agenciadenoticias.ibge.gov.br/agencia-noticias/2012-agencia-de-noticias/noticias/26103-expectativa-de-vida-dos-brasileiros-aumenta-para-76-3-anos-em-2018 (accessed on 9 February 2021).
- Veras, R. Envelhecimento populacional contemporâneo: Demandas, desafios e inovações. Rev. Saúde Pública 2009, 43, 548–554. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; WHO: Geneva, Switzerland, 2008; Available online: https://www.who.int/publications/i/item/WHO-IER-CSDH-08.1 (accessed on 22 September 2023).
- Brasil. Ministério da Justiça. Lei nº 10.741 de 01 de Outubro de 2003. Dispõe Sobre o Estatuto do Idoso e dá Outras Providências. Brasília. 2003. Available online: https://www.planalto.gov.br/ccivil_03/leis/2003/l10.741.htm (accessed on 10 August 2022).
- World Health Organization (WHO). Global Strategy and Action Plan on Ageing and Health (2016–2020); A framework for coordinated global action by the World Health Organization, Member States, and Partners across the Sustainable Development Goals; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Suzman, R.; Beard, J.R.; Boerma, T.; Chatterji, S. Health in an ageing world—What do we know? Lancet 2015, 385, 484–486. [Google Scholar] [CrossRef] [PubMed]
- Tavares, R.E.; de Jesus, M.C.P.; Machado, D.R.; Braga, V.A.S.; Tocantins, F.R.; Merighi, M.A.B. Envelhecimento saudável na perspectiva de idosos: Uma revisão integrativa. Rev. Bras. Geriatr. Gerontol. 2017, 20, 889–900. [Google Scholar]
- Antonelli, M.; Barbieri, G.; Donelli, D. Effects of forest bathing (shinrin-yoku) on levels of cortisol as a stress biomarker: A systematic review and meta-analysis. Int. J. Biometeorol. 2019, 63, 1117–1134. [Google Scholar] [CrossRef]
- Stigsdotter, U.K.; Corazon, S.S.; Sidenius, U.; Kristiansen, J.; Grahnc, P. It is not all bad for the grey city—A crossover study on physiological and psychological restoration in a forest and an urban environment. Health Place 2017, 46, 145–154. [Google Scholar] [CrossRef]
- Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.S.; Suzuki, S. Blood pressure-lowering effect of Shinrin-yoku (Forest bathing): A systematic review and meta-analysis. BMC Complement. Altern. Med. 2017, 17, 409. [Google Scholar] [CrossRef]
- Djernis, D.; Lerstrup, I.; Poulsen, D.; Stigsdotter, U.; Dahlgaard, J.; O’Toole, M. A Systematic Review and Meta-Analysis of Nature-Based Mindfulness: Effects of Moving Mindfulness Training into an Outdoor Natural Setting. Int. J. Environ. Res. Public Health 2019, 16, 3202. [Google Scholar] [CrossRef]
- McCormick, R. Does Access to Green Space Impact the Mental Well-being of Children: A Systematic Review. J. Pediatr. Nurs. 2017, 37, 3–7. [Google Scholar] [CrossRef]
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and well-being benefits of spending time in forests: Systematic review. Environ. Health Prev. Med. 2017, 22, 71. [Google Scholar] [CrossRef]
- Mao, G.X.; Cao, Y.B.; Lan, X.G.; He, Z.H.; Chen, Z.M.; Wang, Y.Z.; Hu, X.L.; Lv, Y.D.; Wang, G.F.; Yan, J. Therapeutic effect of forest bathing on human hypertension in the elderly. J. Cardiol. 2012, 60, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Buckley, R. Nature tourism and mental health: Parks, happiness, and causation. Sustain. Tour. 2020, 28, 1409–1424. [Google Scholar] [CrossRef]
- Europarc Federation. Case Study—Active Senior Tourism, c2021. Case Study. Available online: https://www.europarc.org/case-studies/active-senior-tourism/ (accessed on 18 November 2021).
- Lee, I.; Choi, H.; Bang, K.S.; Kim, S.; Song, M.; Lee, B. Effects of forest therapy on depressive symptoms among adults: A systematic review. Int. J. Environ. Res. Public Health 2016, 13, 321. [Google Scholar] [CrossRef]
- Rejeh, N.; Heravi-Karimooi, M.; Tadrisi, S.D.; Jahani, A.; Vaismoradi, M.; Jordan, S. The impact of listening to pleasant natural sounds on anxiety and physiologic parameters in patients undergoing coronary angiography: A pragmatic quasi-randomized-controlled trial. Complement. Ther. Clin. Pract. 2016, 25, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Wichrowski, M.J.; Corcoran, J.R.; Haas, F.; Sweeney, G.; Mcgee, A. Effects of Biophilic Nature Imagery on Indexes of Satisfaction in Medically Complex Physical Rehabilitation Patients: An Exploratory Study. Health Environ. Res. Des. 2021, 14, 288–304. [Google Scholar] [CrossRef] [PubMed]
- Marselle, M.R.; Irvine, K.N.; Lorenzo-Arribas, A.; Warber, S.L. Does perceived restorativeness mediate the effects of perceived biodiversity and perceived naturalness on emotional wellbeing following group walks in nature? J. Environ. Psychol. 2016, 46, 217–232. [Google Scholar] [CrossRef]
- Miake-Lye, I.M.; Hempel, S.; Shanman, R.; Shekelle, P.G. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Syst. Rev. 2016, 5, 28. [Google Scholar] [CrossRef]
- McKinnon, M.C.; Cheng, S.H.; Garside, R.; Masuda, Y.J.; Miller, D.C. Sustainability: Map the evidence. Nature 2015, 528, 185–187. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Reis, A.; Geus, J.L.; Wambier, L.; Schroeder, M.; Loguercio, A.D. Compliance of Randomized Clinical Trials in Noncarious Cervical Lesions with the CONSORT Statement: A Systematic Review of Methodology. Oper. Dent. 2018, 43, 129–151. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. A declaração PRISMA 2020: Diretriz atualizada para relatar revisões sistemáticas. Epidemiol. Serv. Saúde 2022, 31, e2022107. [Google Scholar] [CrossRef]
- Tableau Software. Tableau Desktop [Software de Visualização de Dados]; Versão 2022Tableau Software: Seattle, WA, USA, 2022. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Lee, D.C. Cardiac and pulmonary benefits of forest walking versus city walking in elderly women: A randomised, controlled, open-label trial. Eur. J. Integr. Med. 2014, 6, 5–11. [Google Scholar] [CrossRef]
- Szczepańska-Gieracha, J.; Cieślik, B.; Serweta, A.; Klajs, K. Virtual Therapeutic Garden: A Promising Method Supporting the Treatment of Depressive Symptoms in Late-Life: A Randomized Pilot Study. J. Clin. Med. 2021, 10, 1942. [Google Scholar] [CrossRef]
- Yeo, N.L.; Elliott, L.R.; Bethel, A.; White, M.P.; Dean, S.G.; Garside, R. Indoor Nature Interventions for Health and Wellbeing of Older Adults in Residential Settings: A Systematic Review. Gerontologist 2020, 60, 184–199. [Google Scholar] [CrossRef]
- Roe, J.; Mondschein, A.; Neale, C.; Barnes, L.; Boukhechba, M.; Lopez, S. The Urban Built Environment, Walking and Mental Health Outcomes Among Older Adults: A Pilot Study. Front. Public Health 2020, 8, 575946. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Ye, B.; Lv, X.; Mao, G.; Wang, S.; Chen, Z.; Wang, G. Adjunctive Therapeutic Effects of Cinnamomum Camphora Forest Environment on Elderly Patients with Hypertension. Int. J. Gerontol. 2020, 14, 327–331. [Google Scholar]
- Pedrinolla, A.; Tamburin, S.; Brasioli, A.; Sollima, A.; Fonte, C.; Muti, E.; Smania, N.; Schena, F.; Venturelli, M. An Indoor Therapeutic Garden for Behavioral Symptoms in Alzheimer’s Disease: A Randomized Controlled Trial. J. Alzheimers Dis. 2019, 71, 813–823. [Google Scholar] [CrossRef]
- Fraser, M.; Polson, R.; Munoz, S.A.; MacRury, S. Psychological effects of outdoor activity in type 2 diabetes: A review. Health Promot. Int. 2020, 35, 841–851. [Google Scholar] [CrossRef]
- Jia, B.B.; Yang, Z.X.; Mao, G.X.; Lyu, Y.D.; Wen, X.L.; Xu, W.H.; Lyu, X.L.; Cao, Y.B.; Wang, G.F. Health Effect of Forest Bathing Trip on Elderly Patients with Chronic Obstructive Pulmonary Disease. Biomed. Environ. Sci. 2016, 29, 212–218. [Google Scholar]
- Mao, G.X.; Cao, Y.B.; Yan, Y.A.N.G.; Chen, Z.M.; Dong, J.H.; Chen, S.S.; Qing, W.U.; Lyu, X.L.; Jia, B.B.; Yan, J.; et al. Additive Benefits of Twice Forest Bathing Trips in Elderly Patients with Chronic Heart Failure. Biomed. Environ. Sci. 2018, 31, 159–162. [Google Scholar] [PubMed]
- Mao, G.; Cao, Y.; Wang, B.; Wang, S.; Chen, Z.; Wang, J.; Xing, W.; Ren, X.; Lv, X.; Dong, J.; et al. The Salutary Influence of Forest Bathing on Elderly Patients with Chronic Heart Failure. Int. J. Environ. Res. Public Health 2017, 14, 368. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.; Ku, B.; Kim, S.G.; Khil, T.; Lim, Y.; Shin, M.; Jeon, S.; Kim, J.; Kang, B.; Shin, J.; et al. Traditional Korean Medicine-Based Forest Therapy Programs Providing Electrophysiological Benefits for Elderly Individuals. Int. J. Environ. Res. Public Health 2019, 16, 4325. [Google Scholar] [CrossRef]
- White, M.P.; Alcock, I.; Grellier, J.; Wheeler, B.W.; Hartig, T.; Warber, S.L.; Bone, A.; Depledge, M.H.; Fleming, L.E. Spending at least 120 minutes a week in nature is associated with good health and wellbeing. Sci. Rep. 2019, 9, 7730. [Google Scholar] [CrossRef] [PubMed]
- Richardson, M.; Passmore, H.A.; Lumber, R.; Thomas, R.; Hunt, A. Moments, not minutes: The nature-wellbeing relationship. Int. J. Wellbeing 2021, 11, 8–33. [Google Scholar] [CrossRef]
- Pálsdóttir, A.M.; Stigmar, K.S.; Norrving, B.; Petersson, I.F.; Åström, M.; Pessah-Rasmussen, H. The nature stroke study; NASTRU: A randomized controlled trial of nature-based post-stroke fatigue rehabilitation. J. Rehabil. Med. 2020, 52, 1–7. [Google Scholar]
- Li, Q. Effects of forest environment (Shinrin-yoku/Forest bathing) on health promotion and disease prevention—The Establishment of “Forest Medicine”. Environ. Health Prev. Med. 2022, 27, 43. [Google Scholar] [CrossRef]
- Meuleman, B.; Rudrauf, D. Induction and Profiling of Strong Multi-Componential Emotions in Virtual Reality. IEEE Trans. Affect. Comput. 2021, 12, 189–202. [Google Scholar] [CrossRef]
- Mastandrea, S.; Fagioli, S.; Biasi, V. Art and Psychological Well-Being: Linking the Brain to the Aesthetic Emotion. Front. Psychol. 2019, 10, 739. [Google Scholar] [CrossRef]
- Chatterjee, A.; Vartanian, O. Neuroscience of aesthetics. Ann. N. Y. Acad. Sci. 2016, 1369, 172–194. [Google Scholar] [CrossRef]
- Catissi, G.; de Oliveira, L.B.; da Silva Victor, E.; Savieto, R.M.; Borba, G.B.; Hingst-Zaher, E.; Lima, L.M.; Bomfim, S.B.; Leão, E.R. Nature Photographs as Complementary Care in Chemotherapy: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2023, 20, 6555. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Decade of Healthy Ageing—Baseline Report; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240017900 (accessed on 5 February 2021).
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; De Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T.; et al. Nature and mental health: An ecosystem service perspective. Sci. Adv. 2019, 5, eaax0903. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Jorgensen, A.; Sun, Q.; Corcoran, A.; Alfaro-Simmonds, M.J. Negotiating Complexity: Challenges to Implementing Community-Led Nature-Based Solutions in England Pre- and Post-COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 14906. [Google Scholar] [CrossRef] [PubMed]
- Leatherdale, S.T. Natural experiment methodology for research: A review of how different methods can support real-world research. Int. J. Soc. Res. Methodol. 2019, 22, 19–35. [Google Scholar] [CrossRef]
- Pearson, A.L.; Pfeiffer, K.A.; Buxton, R.T.; Horton, T.H.; Gardiner, J.; Asana, V. Four recommendations to tackle the complex reality of transdisciplinary, natural experiment research. Front. Public Health 2023, 11, 1240231. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N° | Author/Year | Study Type/ Sample Size | Interventions |
|---|---|---|---|
| 1 | Lee & Lee, 2014 [32] | RCT 70 participants | Both groups walked 1 h in the park or city and after 30 min had blood drawn. Assessed: arterial stiffness, pulmonary function, blood pressure, plus lifestyle questionnaire including smoking, alcohol consumption, and exercise. Collection pre- and post-intervention. |
| 2 | Mao et al., 2012 [18] | RCT 24 participants | Randomized into urban vs. forest. For 7 days, subjects walked a predetermined route at a calm pace for about 1.5 h, with 20 min rest. After lunch, they walked another predetermined route as well. Blood pressure, pathological factors related to cardiovascular diseases, inflammatory cytokines interleukin-6, tumor necrosis factor α, and Profile of Mood States (POMS) were assessed. |
| 3 | Szczepańska-Gieracha et al., 2021 [33] | RCT 25 participants | Control received the standard treatment (40 min general physical training and 20 min health promotion education and psychoeducation two times per week). Virtual reality (VR) group received the same treatment + VR therapy. The therapy cycle consisted of eight VR sessions of 20 min, 2× a week, for four weeks. Used Geriatric Depression Scale (GDS-30), Perception of Stress Questionnaire (PSQ), and Anxiety and Depression Scale (HADS). |
| 4 | Yeo et al., 2020 [34] | Systematic review 930 participants | Interventions of an “active” nature (intentional, direct, tactile interaction with real forms of nature or VR) vs. interventions of a “passive” nature (observation of forms of real nature, such as indoor plants) or simulated nature (nature videos). Assessment by self-reported scales, researcher observations, participant tests and tasks (e.g., to assess cognition), and direct objective measures (physiological outcomes such as pulse rate). |
| 5 | Roe et al., 2020 [35] | RCT 11 participants | Participants were randomly allocated to one of two groups, each of five to six participants. Group 1 walked the “gray” urban route on Day 1, followed by the “green” urban route on Day 2, and Group 2 vice versa, with a one-day break period between walks. Assessed Mood Adjective Check List; subjective well-being; cognitive function—reaction time; cognitive function—memory retrieval; physiological measures; real-time stress, captured with smart watch. |
| 6 | Wu et al., 2020 [36] | RCT 31 participants | The intervention group was exposed to forest bathing (C. camphora) vs. control in urban sites. Assessed C-reactive protein, at day 1 and 3, blood pressure measurements, O2 saturation, and heart rate before and after intervention, every day, in addition to mood state assessment. |
| 7 | Pedrinolla et al., 2019 [37] | RCT 163 participants | All patients participated in the intervention, lasting 2 h each, 5× per week for six months (120 sessions, 240 h of exposure), either in an indoor therapeutic garden (intervention group) or standard care environment (control group). Assessment by Neuropsychiatric Inventory Scale; Mini Mental State Examination; Actiheart device; Barthel Index; and Salivary cortisol. |
| 8 | Fraser et al., 2020 [38] | Systematic review 231 participants | Any form of physical activity performed in an outdoor exercise setting. Psychological assessment for depression, anxiety, quality of life, stress, general well-being. |
| 9 | Jia et al., 2016 [39] | RCT 18 participants | One group was sent to the forest (forest bath) vs. urban area (control), with no other details about the intervention. Assessed lung chemokine; surfactant protein D; interleukin-6, -8, and -1β; interferon-γ; tumor necrosis factor α; C-reactive protein; and proportion of T, NK, and POMS lymphocyte subsets. |
| 10 | Mao et al., 2018 [40] | RCT 20 participants | Randomized into urban vs. forest. After four weeks, the patients who had experienced the first forest bathing trip were recruited again, and 20 of them were enrolled for the second experiment. These 20 CHF patients were randomly categorized into two groups consisting of 10 patients in each. Collected pre- and post each experiment, fasting. Assessed: brain natriuretic peptide, interleukin-6, and tumor necrosis factor α. |
| 11 | Mao et al., 2017 [41] | RCT 33 participants | Preintervention: fasting blood draw + physical examination. Preintervention collection + POMS questionnaire. Allocated into urban vs. forest group. Subjects walked outdoors 2× per day during the experimental period, and each time, they walked along a predetermined flat path in each area at an unhurried pace for about 1.5 h. They were then asked to complete the POMS test for a second time. |
| 12 | Yi et al., 2019 [42] | RCT 88 participants | 1°: Walking Program (WP) (active walking in the forest). 2°: Breathing Program (BP) (guided breathing meditation). 3°: Control group (no intervention or activities in the forest). The first two groups were conducted in urban forests. The WP consisted of 30 min of preparatory activities, 50 min of walking in the forest, 20 min of muscle training with elastic band, and 20 min of closing activities. Participants taped red Yongquan beans on both feet so that they could be stimulated by acupressure during the walk. The AP consisted of 30 min preparatory session, 30 min guided breathing meditation, 20 min slow forest walk, 20 min muscle training with elastic band, and 20 min closing activities. |
| N° | Author/Year | Outcomes and Effects |
|---|---|---|
| 1 | Lee & Lee, 2014 [32] |
|
| 2 | Mao et al., 2012 [18] |
|
| 3 | Szczepańska-Gieracha et al., 2021 [33] |
|
| 4 | Yeo et al., 2020 [34] |
|
| 5 | Roe et al., 2020 [35] |
|
| 6 | Wu et al., 2020 [36] |
|
| 7 | Pedrinolla et al., 2019 [37] |
|
| 8 | Fraser et al., 2020 [38] |
|
| 9 | Jia et al., 2016 [39] |
|
| 10 | Mao et al., 2018 [40] |
|
| 11 | Mao et al., 2017 [41] |
|
| 12 | Yi et al., 2019 [42] |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catissi, G.; Gouveia, G.; Savieto, R.M.; Silva, C.P.R.; de Almeida, R.S.; Borba, G.B.; Rosario, K.A.; Leão, E.R. Nature-Based Interventions Targeting Elderly People’s Health and Well-Being: An Evidence Map. Int. J. Environ. Res. Public Health 2024, 21, 112. https://doi.org/10.3390/ijerph21010112
Catissi G, Gouveia G, Savieto RM, Silva CPR, de Almeida RS, Borba GB, Rosario KA, Leão ER. Nature-Based Interventions Targeting Elderly People’s Health and Well-Being: An Evidence Map. International Journal of Environmental Research and Public Health. 2024; 21(1):112. https://doi.org/10.3390/ijerph21010112
Chicago/Turabian StyleCatissi, Giulia, Gabriela Gouveia, Roberta Maria Savieto, Cristiane Pavanello Rodrigues Silva, Raquel Simões de Almeida, Gustavo Benvenutti Borba, Kaue Alves Rosario, and Eliseth Ribeiro Leão. 2024. "Nature-Based Interventions Targeting Elderly People’s Health and Well-Being: An Evidence Map" International Journal of Environmental Research and Public Health 21, no. 1: 112. https://doi.org/10.3390/ijerph21010112
APA StyleCatissi, G., Gouveia, G., Savieto, R. M., Silva, C. P. R., de Almeida, R. S., Borba, G. B., Rosario, K. A., & Leão, E. R. (2024). Nature-Based Interventions Targeting Elderly People’s Health and Well-Being: An Evidence Map. International Journal of Environmental Research and Public Health, 21(1), 112. https://doi.org/10.3390/ijerph21010112